
Abstract
Background
Neonatal septicemia remains one of the main causes of neonatal morbidity and mortality. However, there are challenges hindering the early diagnosis.
Results
nCD64 percent and MFI were not of statistical significance between the confirmed sepsis, clinical sepsis, and control groups (p = 0.453 and 0.149, respectively); meanwhile, the mHLA-DR percent and MFI were both of statistical significance (p = 0.001, 0.0001, respectively) with lower values in the proven sepsis group. Calculating the sepsis index, its value was 74.1% ± 45 SD in the control, 105.5% ± 73 SD probable sepsis group, and 180.6% ± 143 SD in the proven sepsis group; this was of a high statistical significance (p = 0.0001).
Conclusion
HLA-DR expression on monocytes and nCD64/mHLA-DR sepsis index are reliable indices for the early diagnosis of neonatal sepsis. The sepsis index could be feasibly analyzed by automated flow cytometry even in developing countries. In the future, these markers should be widely assessed as their results are rapid, reliable, and of low cost.
Similar content being viewed by others

Background
Sepsis which is caused by a dysregulated host response to an infectious trigger leading to a life-threatening organ dysfunction was declared by the World Health Organization (WHO) on May 2017 as a global health priority that requires resolution for its prevention, diagnosis, and management [1]. Neonatal septicemia, which occurs during the first month of life, remains one of the main causes of neonatal morbidity and mortality despite the better hygiene, the introduction of novel potent antimicrobial agents, and the advances in diagnosis [2].
The early clinical features of infection are often mild, variable, nonspecific, and difficult to recognize. Thus, neonatal sepsis is clinically indistinguishable from other noninfectious conditions such as transient tachypnea of the newborn, meconium aspiration syndrome, respiratory distress syndrome, apnea of prematurity, and acute exacerbation of chronic lung disease [3]. The early diagnosis of sepsis will ensure a prompt treatment, thus reducing organ failure and mortality. However, there are challenges in the early diagnosis, for example, blood culture which is the gold standard test needs time—2 to 4 days—to confirm the diagnosis, and there is a possibility of having a negative result in neonates who were exposed to antibiotics in utero [4, 5]. The assessment of the cytokine profile is considered a good negative indicator; however, it is not widely used as it is expensive, requires a large amount of blood, and need a long interval to retrieve the result [4]. The other biochemical markers used for screening such as procalcitonin (PCT) are not specific and costly [6]. The unnecessary administration of antibiotics in non-septic patients increases the economic burdens and exposes the infants to unnecessary treatment [7]; thus, there is a rising need for a diagnostic indicator for timely sepsis diagnosis [8].
During bacterial infections, the interacting leukocytes increase the expression of cell adhesion molecules; these cell surface antigens are considered promising new markers in the diagnosis of sepsis and can be identified easily by flow cytometry, a technique that robustly progressed [7].
CD64, also called Fc gamma receptor I (FcγRI), is a type of integral membrane glycoprotein. When activated, it increases the neutrophils’ potential for phagocytosis and bacterial killing [9]. It is rapidly upregulated on the neutrophil membrane which has 6-h half-life, making neutrophil CD64 expression a true indication of the current status regarding neonatal sepsis. Thus, its expression should improve the diagnosis of infection by discriminating it from systemic inflammatory response syndrome [10, 11].
HLA-DR is on the surface of monocyte/macrophages, dendritic cells, and B cells and plays a crucial role in adaptive immune response. More than 30 years ago, researchers proved an association between the low level of HLA-DR and the development of sepsis [12]. A decreased expression of mHLA-DR molecules has been associated with immunoparalysis, which is an anti-inflammatory immune response that occurs in sepsis [6].
A new index, first done in 2016, called sepsis index (SI) is used in this study including CD64 (proinflammatory marker) and HLA DR (anti-inflammatory marker) to give a better idea of sepsis. The index is calculated as follows: [6]
The aim of the present study was to evaluate the diagnostic potential of combining neutrophil CD64 and monocytic HL-ADR expression evaluated by flow cytometry as predictors for neonatal sepsis.
Methods
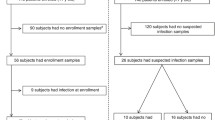
This study included 50 neonates of both sexes who were admitted to the neonatal intensive care unit (NICU) from June 2018 to June 2019 with suspicion of sepsis in the immediate newborn period.
Fifty healthy neonates (attending for elective procedures, e.g., circumcision) were included as the control group. An informed consent was taken from the neonates’ guardians. The study was approved by the institutional committee (I-240416) and was carried out in accordance with the Declaration of Helsinki.
Eligibility criteria
The inclusion criteria are neonates of both sexes included in this study with any suspected case of neonatal sepsis with maternal risk factors for sepsis, e.g., prolonged labor, premature rupture of membrane (PROM) or prolonged PROM >18 h, maternal intrapartum fever, urinary tract infection, and chorioamnionitis, and neonates with sepsis-related clinical signs: temperature instability, apnea, need for supplemental oxygen, bradycardia, tachycardia, hypotension, hypoperfusion, feeding intolerance, and abdominal distension. Initially, the Apgar score was used to indicate the infant’s condition in the first and fifth minutes after birth that includes appearance, heart rate, muscle tone, and respiratory effort.
The exclusion criteria are the administration of antibiotic therapy prior to admission, birth asphyxia, documented necrotizing enterocolitis (NEC), aspiration syndromes, laboratory finding suggestive of inborn error of metabolism, and congenital anomalies including congenital heart disease.
All patients were subjected to an assessment of the presence of maternal risk factor such as fever, prolonged rupture of the membranes and chorioamnionitis, neonatal history including birth weight and gestational age, and signs and symptoms of sepsis including feeding intolerance, temperature instability, apnea, seizures, tachycardia, bradycardia, respiratory distress, abdominal distension and vomits.
Laboratory investigations
The peripheral blood was aseptically withdrawn by venipuncture within the first 24 h of admission prior to the antibiotic therapy. One sample was inoculated into a blood culture bottle. The cultures for aerobic bacteria were incubated at 37 °C for 7 days under aerobic conditions and inspected every morning, and subcultures were performed after 24 h of inoculation, on the 3rd day, and finally on the 7th day. The growth was identified by colony characteristics, gram stain, and standard biochemical tests. A serum sample was collected for the evaluation of C reactive protein (CRP) by nephelometry (Nephstar, Goldsite Diagnostic Inc., China). Complete blood count was performed on Siemens Advia 120 hematology system (Siemens AG, Germany). Flow cytometric assessment was performed within 24 h of sample collection. In brief, 50 μl of blood was stained with CD64 FITC (Beckman Coulter IM1604U) and HLADR PE (Beckman Coulter IM1639) according to the manufacturers. The red blood cells were lysed using an erythrocyte lysing solution (Beckman Coulter Versalyse A09777). Samples were acquired on flow cytometry (FC500 Beckman Coulter, FL, USA) acquiring at least 20,000 events. Gating on neutrophils and monocytes was based on their separation by forward and side scatter. Data was analyzed by the CXP software version 2.2 and recorded as the mean fluorescence intensity (MFI) and percentages. Sepsis index adopts the concept of combining the changes in the expression of pro- and anti-inflammatory markers and was calculated as proposed by Pradhan et al. [6] through the arithmetic division of the MFI value of neutrophil CD64 and the MFI of monocyte HLADR and multiplying the ratio by 100.
Statistical methods
Data was statistically described in terms of median and range or frequencies (number of cases) and percentages when appropriate. Comparison of numerical variables between the study groups was done using the Kruskal-Wallis test with Mann-Whitney as post hoc multiple 2-group comparisons after applying Bonferroni adjustment for multiple comparisons. For comparing categorical data, the chi-square (χ2) test was performed. The exact test was used instead when the expected frequency is less than 5. Receiver operator characteristic (ROC) analysis was used to determine the optimum cutoff value for the studied diagnostic markers in diagnosing sepsis. Two-sided p values less than 0.05 was considered statistically significant. All statistical calculations were done using the computer program IBM Statistical Package for the Social Science (SPSS; IBM Corp, Armonk, NY, USA) release 22 for Microsoft Windows
Results
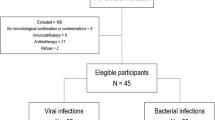
This study included 50 neonates admitted to NICU with suspected sepsis. Based on the results of blood cultures, they were further subdivided into 2 subgroups: proven sepsis with positive culture (n = 23) and probable sepsis with negative culture (n = 27). Healthy neonates (n = 50) served as a control group.
There was no statistical significance between the neonates in the three groups regarding gender, gestational age, and mode of delivery (p = 0.623, 0.367, 0.084, respectively). On the other hand, there was a significant difference between the 3 groups regarding the presence of chorioamnionitis as a risk factor for sepsis (p = 0.006) and also regarding the symptomatology indicating a high risk of sepsis such as apnea (p = 0.0001), feeding intolerance (p = 0.0001), and poor perfusion (p = 0.0001). The demographic characteristics and risk factors of the patients are summarized in Table 1.
Blood culture results were positive in 23 neonates (proven sepsis group), the isolated organisms were Klebsiella Pneumoniae from 14 neonates (60.9%) and Escherichia coli from 6 neonates (26.1%), whereas Methicillin-resistant Staphylococcus aureus (MRSA), Candida Albicans, and Pseudomonas were isolated from one neonate each (4.3%). Neonates with negative blood cultures (n = 27) were considered the probable sepsis group (clinical sepsis).
Regarding the CRP as one of the acute phase reactants widely used, the median level in the control was 3 mg/L, in the probable sepsis group 8 mg/L, and in the proven sepsis group 31 mg/L with a significant statistical difference (p = 0.0001). Meanwhile, regarding total leucocyte count (TLC), there is a statistical difference between control and proven sepsis (p value=0.025), while there is no statistical difference between control and probable sepsis (p value = 0.278), probable and proven sepsis (p value= 0.365), and the three groups together as well (p = 0.082).
As for blood cells surface markers evaluated by the flow cytometry, the nCD64 percent and MFI were not of statistical significance between the 3 groups (p = 0.453 and 0.149, respectively); meanwhile, the mHLA-DR percent and MFI were both of statistical significance (p = 0.001, 0.0001, respectively) with lower values in the proven sepsis group. By calculating the sepsis index, it was 74.1% ± 45 SD in the control, 105.5% ± 73 SD in the probable sepsis group, and 180.6% ± 143 SD in the proven sepsis group. This was of high statistical significance (p = 0.0001). Also, upon comparing the sepsis index in the control group 74.1% ± 45 SD vs all sepsis group (probable and proven) 140.11 ± 116 SD, a high statistical significance (p = 0.0001) was found. All the laboratory data was presented in Table 2.
The ROC analysis was used to determine the best cutoff value of nCD64 MFI, HLA-DR MFI, and sepsis index. Accuracy is represented using the terms sensitivity and specificity. The confidence interval was set to 95%, and the margin error was set to 5%. The CD64 MFI is considered a poor test (p value 0.059 and area under the curve 0.638), while HLA- DR MFI is a good test (p value 0.0001 and area under the curve 0.856) and the sepsis index is also a fair test (p value 0.0001 and area under the curve 0.798) (Fig. 1). A selected cutoff point of 1.960 for HLA-DR MFI was found to have a sensitivity of 73% and specificity 84%, whereas the selected cutoff value for sepsis index was 91% having 65% sensitivity and 80% specificity.

Receiver operating characteristic curves to determine the best cutoff values of the ROC curve to determine the best cutoff values of a nCD64 mean fluorescence intensity (MFI) in differentiating neonates with sepsis from healthy neonates with an area under the curve yielded as 0.638 (p = 0.059), b mHLA-DR mean fluorescence intensity (MFI) in differentiating neonates with sepsis from healthy neonates at cutoff 1.96 area under the curve yielded as 0.856 (p = 0.0001), and c sepsis index in differentiating neonates with sepsis from healthy neonates at cutoff 91% area under the curve yielded as 0.798 (p = 0.0001)
Discussion
Neonatal sepsis has a high mortality rate and remains challenging to health care providers. The early diagnosis of sepsis remains one of the most difficult tasks [13]. Thus, there is a great need to find new indicators for neonatal sepsis to increase the sensitivity and specificity of both diagnosis and monitoring therapy. However, there is no single biomarker available that differentiates between sepsis and systemic inflammatory response syndrome without infection. Each available marker has some advantages and some limitations [10].
Flow cytometry can play a pivotal role in the diagnosis of sepsis. It requires minimal volume of blood and results appear rapidly (< 1 h) [4]. Treatment can be initiated based on the patients’ immune system situation assessed by flow cytometric expression of cell surface markers [10].
In this study, neonates were grouped into three groups: neonates with sepsis (had positive blood culture), neonates with probable sepsis due to the presence of signs of sepsis but with negative blood cultures, and healthy neonates (control group).
This study showed similar male and female predominance. The gestational age had no significant correlation to the occurrence of sepsis. This agrees with the study by Mahmoodpoor et al. [9] and contrasts with other studies like the study by Darmstadt et al. [14] which stated that the majority of cases with early onset sepsis had a gestational age < 30 weeks. These studies explained this via the immaturity of the immune system and hypogammaglobulinemia in premature babies [15].
The most prominent signs of neonatal sepsis in this study were apnea (43.5%), poor perfusion (56.5%), feeding intolerance (34.8%), poor suckling, mottled skin, poor Moro reflex, and lethargy, while the study by Trotman and Bell [16] revealed that the most common presenting clinical features were respiratory distress (32%), poor feeding (23%), vomiting (14%), abdominal distension (14%), lethargy (9%), and irritability (9%).
In our study, the most common organisms isolated in septic patients were Klebsiella (60.9%) and E. coli (26.1%). Similar organisms were reported by Darmstadt et al. [17]; on the other hand, the study by Bizzaro et al. [18] found the most common organisms were Staphylococcus aureus followed by E. coli, Pseudomonas, and Klebsiella. The study by Marchant et al. [19] found that Gram-positive organisms represent 70% of septic cases and Gram-negative organisms 15–20%. Thus, there is a variability of results of infective organisms from NICU to another, between geographical areas and in the same area according to time thus each hospital must adjust their antibiotics accordingly.
CRP is an acute-phase reactant and is widely used for the diagnosis of neonatal sepsis. Consistent with the literature, this study showed a high significant difference between cases and controls in the level of CRP. However, as its concentrations increase slowly at first, the sensitivity is only 60% at the time of sepsis and serial measurements are required to improve the sensitivity, and it is also not specific enough as its concentrations can be elevated in other conditions such as meconium aspiration, tissue necrosis, recent vaccination, and surgery [7, 20].
On utilizing flow cytometry cell surface marker expression, CD64 percent and MFI in neonates with sepsis were statistically insignificant when compared to the control and probable sepsis groups. This agrees with a meta-analysis by Shi et al. [21] that did not find CD64 a sensitive or a specific marker for sepsis. On the contrary, many previous studies showed a rise in the percentage of CD64 in the proven sepsis groups [4, 10, 22]. The present study showed that the ROC curve for CD64 MFI had an area under the curve of 0.46, p = 0.493, making it a non-diagnostic test for neonatal sepsis. On the contrary, other studies such as that done by Elawady et al. [23] found that CD64 had the highest sensitivity (96%) and specificity (100%), with cutoff values of 45.8%. Also, the study by Streimish et al. [22] demonstrated that the sensitivity of CD64 was 78% and the specificity was 59%. The diagnostic efficacy of sensitivity and specificity nCD64 varied from 26 to 97% and 71 to 100%, respectively [24]. Thus, previous reports considered nCD64 a specific but weakly sensitive test for bacterial infection, and therefore, it is better to use it in combination with another more sensitive biological marker [25].
In the present study, mHLA-DR had shown a positive significance with the possibility of occurrence of sepsis. A study by Winkler et al. [26] found a higher number of monocytes, but with lower expression of HLA-DR in peripheral blood of septic patients. Another study by Genel et al. [27] found a lower HLA-DR level in septic neonates and found a prognostic value for it in this group of patients. On the contrary, the study by Ng et al. [3] on neonates with suspected sepsis showed no significant differences in monocyte HLA-DR expression between infected, non-infected, and control groups.
The ROC curve for HLADR MFI showed an area under the curve of 0.856, and a cutoff value of 1.960 was postulated for best sensitivity and specificity (73% sensitivity and 84% specificity). On the other hand, previous studies postulated that a cutoff value for HLA-DR was difficult to find [3].
As diagnosing sepsis is a difficult task, people often use multiple parameters simultaneously; that is why it is best if we use CD 64 and HLA-DR together, and thus, a sepsis index (SI) was created. In our study, SI was found an effective tool for predicting sepsis. The ROC curve showed an area under the curve equal to 0.798 with a cut off value of 91% with corresponding 65% sensitivity and 80% specificity. The mean SI in controls is 74% while in probable sepsis 105% and in proven sepsis is 180%. The pilot study by Chauhan et al. [24] on adults in ICU units indicated that the diagnosis of sepsis is better through the combination of nCD64, mHLA-DR, and sepsis index for better diagnosis of these patients in comparison with all other available modalities. Similarly, the study by Pradhan et al. [6] revealed that sepsis index was significantly higher in infected than non-infected neonates and healthy controls. They hypothesized that to improve the sensitivity of sepsis diagnosis, a combination of parameters should be used, especially if combining nCD64, SI, and positivity of 2 laboratory criteria increased, this will increase the sensitivity to 90.47% on day 1.
Conclusion
HLA-DR expression on monocytes and nCD64/mHLA-DR sepsis index are considered as reliable indices for early diagnosis of neonatal sepsis. They may be helpful for early initiation of treatment and give precious hours to more efficacious interventions, thus improving the outcome in the NICU. The sepsis index could be feasibly analyzed by automated flow cytometry even in developing countries. In the future, these markers should be widely assessed as their results are rapid, reliable, and of low cost.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- ABG:
-
Arterial blood gases
- CRP:
-
C-reactive protein
- CD64:
-
Cluster of differentiation 64
- CSF:
-
Cerebrospinal fluid
- EONS:
-
Early-onset neonatal sepsis
- HLA-DR:
-
Human leucocyte antigen (DR isotope)
- MFI:
-
Mean fluorescence intensity
- LBW:
-
Low birth weight
- LOS:
-
Late-onset sepsis
- NICU:
-
Neonatal intensive care unit
- NEC:
-
Necrotizing enterocolitis
- PROM:
-
Premature rupture of membranes
- RBS:
-
Resting blood sugar
- ROC:
-
Receiver operator characteristic
- SI:
-
Sepsis index
- SIRS:
-
Systemic inflammatory response syndrome
- TLC:
-
Total leukocytic count
- TLR:
-
Toll-like receptors
- TPN:
-
Total parenteral nutrition
- UTI:
-
Urinary tract infection
References
Monneret G, Gossez M, Aghaeepour N et al (2019) How clinical flow cytometry rebooted sepsis immunology. Cytometry A 95(4):431–441
Naher HS, Khamael AB (2013) Neonatal sepsis; the bacterial causes and the risk factors. Int. Res. J. Medical Sci 1(6):19–22
Ng PC, Lam HS (2006) Diagnostic markers for neonatal sepsis. Curr Opin Pediatr 18(2):125–131
Bhandari V, Wang C, Rinder C et al (2008) Hematologic profile of sepsis in neonates: neutrophil CD64 as a diagnostic marker. Pediatrics 121(1):129–134
Sharma A, Thakur A, Bhardwaj C et al (2020) Potential biomarkers for diagnosing neonatal sepsis. Curr Med Res Pract 10(1):12–17
Pradhan R, Jain P, Paria A et al (2016) Ratio of neutrophilic CD64 and monocytic HLA-DR: a novel parameter in diagnosis and prognostication of neonatal sepsis. Cytom Part B Clin Cy 90(3):295–302
Aydin M, Barut S, Akbulut HH et al (2017) Application of flow cytometry in the early diagnosis of neonatal sepsis. Ann Clin Lab Sci 47(2):184–190
Mahmoodpoor A, Paknezhad S, Shadvar K et al (2018) Flow cytometry of CD64, HLA-DR, CD25, and TLRs for diagnosis and prognosis of sepsis in critically ill patients admitted to the intensive care unit: a review article. Anesth Pain Med. 8(6):e83128. https://doi.org/10.5812/aapm.83128
Abd Elkareem RM, Ahmed HM, Meabed MH et al (2020) Diagnostic value of CD64 in early detection of neonatal sepsis. Comp Clin Pathol 29:639–643
Dilli D, Ogˇuz ŞS, Dilmen U et al (2010) Predictive values of neutrophil CD64 expression compared with interleukin-6 and C-reactive protein in early diagnosis of neonatal sepsis. J Clin Lab Anal 24(6):363–370
Vazquez Rodriguez S, Arriaga Pizano LA, Laresgoiti Servitje E et al (2021) Multiparameter flow cytometry analysis of leukocyte markers for diagnosis in preterm neonatal sepsis. J Matern Fetal Neonatal Med. 18;34(14):2323-2333
Cheadle WG, Hershman MJ, Wellhausen SR et al (1991) HLA-DR antigen expression on peripheral blood monocytes correlates with surgical infection. Am J Surg 161(6):639–645
Fleischmann-Struzek C, Goldfarb DM, Schlattmann P et al (2018) The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med. 6(3):223–230
Darmstadt GL, Zaidi AK, Stoll BJ (2011) Neonatal infections: a global perspective. In: Remington J, Klein J, Wilson C, Nizet V, Maldonado Y (eds) Infectious diseases of the fetus and newborn infants, 7th edn. Elsevier, pp 24–51
Haque K (2007) Understanding and Optimizing Outcome in Neonates with Sepsis and Septic Shock. In: Intensive Care Medicine. Yearbook of Intensive Care and Emergency Medicine, vol 2007. Springer, Berlin, Heidelberg, p 55-68. https://doi.org/10.1007/978-3-540-49433-1_6
Trotman H, Bell Y (2006) Neonatal group B streptococcal infection at the University Hospital of the West Indies, Jamaica: a 10-year experience. Ann Trop Paediatr. 26(1):53–57
Darmstadt GL, Batra M, Zaidi AK (2009) Oral antibiotics in the management of serious neonatal bacterial infections in developing country communities. Pediatr Infect Dis J 28(1):S31–SS6
Bizzarro MJ, Raskind C, Baltimore RS et al (2005) Seventy-five years of neonatal sepsis at Yale. Pediatrics 116(3):595–602
Marchant EA, Boyce GK, Sadarangani M et al (2013) Neonatal sepsis due to coagulase-negative staphylococci. Clin Dev Immunol. 2013:586076. https://doi.org/10.1155/2013/586076
Ng P (2004) Diagnostic markers of infection in neonates. Arch Dis Child Fetal Neonatal Ed 89(3):F229–FF35
Shi J, Tang J, Chen D (2016) Meta-analysis of diagnostic accuracy of neutrophil CD64 for neonatal sepsis. Ital J Pediatr. 42(1):57
Streimish I, Bizzarro M, Northrup V et al (2014) Neutrophil CD64 with hematologic criteria for diagnosis of neonatal sepsis. Am J. Perinatol. 31(01):021–030
Elawady S, Botros SK, Sorour AE et al (2014) Neutrophil CD64 as a diagnostic marker of sepsis in neonates. J Investig Med. 62(3):644–649
Chauhan S, Hansa J (2017) Early diagnosis of sepsis through sepsis markers and sepsis index through flow cytometry technology. Asian J Pharm Clin Res. 10:145–148
Gros A, Roussel M, Sauvadet E et al (2012) The sensitivity of neutrophil CD64 expression as a biomarker of bacterial infection is low in critically ill patients. Intensive Care Med. 38(3):445–452
Winkler MS, Rissiek A, Priefler M et al (2017) Human leucocyte antigen (HLA-DR) gene expression is reduced in sepsis and correlates with impaired TNFα response: a diagnostic tool for immunosuppression? PLoS One. 12(8):e0182427
Genel F, Atlihan F, Ozsu E et al (2010) Monocyte HLA-DR expression as predictor of poor outcome in neonates with late onset neonatal sepsis. J Infection. 60(3):224–228
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Conception and study design: RH, SE, and MH. Acquisition of the data: RB. Analysis and interpretation of the data: RH, SE, and RB. Drafting of the manuscript: RB and RH. Revision of the manuscript: RH, SE, MH, and RB. Approval of the final version of the manuscript: RH, SE, MH, and RB. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the institutional committee (research ethics committee, REC) of Cairo university (I-240416) and was carried out in accordance with the Declaration of Helsinki.
A written consent was obtained from all parents of the participants.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alanwary, S., Bakir, R., El Hawary, R. et al. The use of neutrophil CD64 and monocyte HLA-DR sepsis index in the diagnosis of neonatal sepsis. Egypt Pediatric Association Gaz 70, 29 (2022). https://doi.org/10.1186/s43054-022-00120-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-022-00120-3