
Abstract
Background
Child sexual abuse has deep and profound effects on personality and growth of children so that it is recognized as one of the major health issues in different countries. A psychological interventions program with a robot was designed and its effects on children sexual care was examined.
Results
The results showed that experts confirmed and supported 85% of the total content of the program and the sessions, and the program was effective in improving sexual cares in the subjects (p < 0.01).
Conclusion
The program to protect children against sexual abuse through empowering them by the skills to protect themselves, recognize good and bad physical touches, and find a trustable adult can be considered as a therapeutic method by consultants, psychologists, and authorities.
Similar content being viewed by others

Background
Children constitute a major part of the world population, so that they are about 50% of the total population in the developing countries [1]. Children and teenagers are important parts of any healthy society and deserver extensive mental health care to ensure their mental and physical health. Through this, children can assume their social responsibility and role in adulthood. Having the right knowledge and insight into the different physical and mental aspects of this age group and necessity to work hard to provide a decent physical and mental conditions for their emotional, intellectual, and physical growth are beyond any question [2].
Child sexual abuse is one of the most prevalent and complicated psychosocial issues in society. It has undeniable effects on child’s mental health. This social issue affects and harms thousands of children in the world. The growing trend of such crimes risks the future of hundreds of children. Doubtlessly, no event like sexual abuse can destroy the future of children. Unfortunately, the extent of the crime is growing all around the world [3]. There is no detailed statistics of child abuse in Iran and the figures announced by some of the media are nowhere close to the reality. The religious culture in Iranian society makes many victims of this crime not to publicly ask for help as way to protect the family’s pride. This is more common in the cases that girls are the victims. Child abuse does not usually happen in public and families that experience such crime usually prefer to hide it and this prevents supervision and prevention by the law [4, 5]. Evidences have shown that the risk factors of sexual abuse against children are bullying, sexual abuse by individuals with homosexual traits, childbearing methods of parents, poverty, alcohol abusive use, inequality as a social norm, lack of empowerment of girls and women, ruling power of men, and laws and policies that promote gender inequality [6]. Therefore, experts’ role to prevent such crimes is more important than ever. Assessing and providing psychotherapy and consultation services to prevent such crimes are more efficient and economic than providing treatments after the crime. Such measures also decrease the level of damage and disorders caused to the victims [4]. Children older that three years have the capability to learn about some of sexual and protective matters. Therefore, it is possible to increase personal safety skills and self-knowledge in these children [7]. Through education and psychological intervention (e.g. behavioral, cognitive, cognitive-behavioral, supportive treatments, interpersonal psychological interactions, mentality and the like) children can learn interpersonal communication and problem-solving skills. They can also learn coping skills to deal with their [8]. Implementing these interventions using robots and game playing can be more efficient as playing are better ways to attract children’s attention. Robots are very useful for therapeutic purposes so that their natural attraction makes them an efficient motivational tool for educational purposes [9].
Therefore, educating and informing children is one of the ways to control child abuse. Many countries with successful experience in controlling child abuse have relied on educational and informing measures for children and families [10].
The public bodies in charge of controlling and preventing social damages including child abuse and violence in Iran are Welfare Organization, Municipalities, and Police. In absence of a centralized command center, these organizations have failed to fulfill their responsibility in this regard.
Educating children and parents is one of the ways to fight social damages like child sexual abuse. Sexual care educations using smart robots and other interesting ways of providing education to children seems like an efficient way to attenuate the risk of sexual abuse in the society. A psychological interventions program was developed and implemented using a robot and the effects on sexual care in children were assessed.
Method
In this study, the researcher uses a qualitative method to develop a program or educational package of robot-based psychological interventions. Then, using the quantitative method, he manipulates the independent variable to check its effect on the dependent variables.
A) Qualitative method
The study was carried out as a qualitative work (codification of the program or educational package of psychological interventions with a smart robot) following Delphi’s approach.
Psychological interventions program with a robot
Step 1: theoretical background and literature review
The psychological interventions program using a smart robot is one of the ways of providing care to children against sexual abuse. The program was designed based on the literature review results.
The available literature including articles and books were used to assess educational needs of children for prevention of sexual abuse. In addition, available curriculums or similar programs, if any, and available studies on the subject were found and used to determine the factors in education. In addition, strength and weakness point of the available programs with robots were examined. At first, the drawbacks of psychological intervention programs with robots in education and prevention of sexual abuse in children and pertinent cares were determined and used for further planning. In other words, determining the educational needs in terms of emotional (attitude), cognitive (knowledge), and skill needs was the first step for educational programming and the first factor to ensure efficiency and optimization. By taking this step in the right way, a more objective basis for programming can be achieved. There are different ways to determine educational needs and each has its advantages and limitations that make each one a better choice in different settings.
Step 2: examining the syllabus of educational programs
The content of the psychological interventions program with a smart robot for children sexual care was designed and represented as a 11-session course (Table 1).
Step 3: designing and codifying the program content
To design and interventional program using Delphi method, five experts in clinical and educational psychology were selected to examine the educational content (Table 1). Based on their opinions and analyzing the feedbacks, a pilot design of the intervention program was developed. It is notable that in addition to modifying the content, the number sessions decreased to 10. Afterwards, the final version of the program was designed based on the experts’ opinion (Annex 1).
Step 4: revising and finalizing the program
Based on the experts’ opinions, sessions nos. 3 and 4 were combined and more applied items and instances were added to the educational assignments. Based on these three last steps, the program was finalized and confirmed by experts. Therefore, the program was finalized with 10 sessions. To review the program and its comprehensiveness, a booklet was developed to be provided to the parents of subjects at the final session.
To examine construct validity of the interventional program, the theoretical foundations were examined in detail and based on the strong theoretical background, construct validity of the tool was supported. The authors and experts who helped us in the design of program supported face validity of the program. To design the program, the authors visited five experts of clinical and educational psychology and their feedbacks and opinions were used to finalized the program. All changes in the program were reported to the experts until finalizing the program. In other words, content validity of the program was supported by the experts.
B) Quantitative method
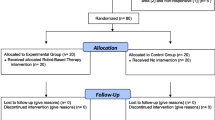
The study was carried out as a quasi-experimental work with pretest, posttest, and follow-up design and control and experiment groups. The follow-up test was conducted three months after the posttest stage. The study population consisted of all children at age range 8–12 (elementary school) in Ghaenat City, Iran in 2019. The sample group was comprised of 80 children at 8–12 years old range who were selected through cluster random sampling. The participants were allocated to two control groups (boys and girls each with 20 participants) and two experiment groups (boys and girls each with 20 participants). The inclusion criteria were desire to participate, age range 8–12 years, no acute mental and physical disease (based on interviewing and health checklist of students), and informed consent by the parents. The exclusion criteria were missing one of the educational sessions, using specific medicines, participation in similar educational intervention at the same time, and reluctance to participate. There were no dropouts from the study and all the participants were retained for the follow-up and data analyses of results.
Data gathering was done using an endogenized questionnaire of knowledge and awareness of sexual abuse [11]. The questionnaire contains 33 items and its reliability has been reported equal to 0.65 and 0.74 by Jacqueline et al. and Gangos et al. respectively [12, 13]. The tool was validated for Iranian society by Tahan et al. [14].
The questionnaire is designed to measure information and learning performance of children about the key beliefs of sexual abuse. The tool is designed in a way that respondents can understand the questions without any background.
The Iranian version of the tool has 38 items with two-point Likert’s scale (0 = yes, 1 = no). the minimum and maximum scores of the tool are 0 and 21 respectively. The higher the score the higher the respondent awareness of the concept of sexual abuse. The questionnaire is suitable for children at age range 8–12 years. The tool has two sub-scales of good touch (eight items) and bad touch (30 items). Psychometric data collected from the 80 participants in this study was examined and validity and reliability of the tool were tested using K-R20 test.
Implementation
After securing required permissions and an ethical code from the Research Department, Islamic Azad University of Birjand-Iran the authors visited the study site to establish friendly relationships with the officials of Ghaenat-based elementary schools. The school principals were briefed about the objective and importance of the study. Then the parents and teachers (based on interview and health checklist) were invited to attend a briefing session to discuss the importance of the study. The parents of children signed an informed letter of consent and they were insured that their and their children’s personal information and name will remain confidential and their participations entails no cost and damage to the participants. Then, 80 students were selected randomly and allocated to control and experiment groups. At first, the questionnaire was filled out for the participants in the both groups (pretest). The experiment groups, then, received 10 sessions of group therapy (45 min, twice a week) where psychological interventions (using a robot) were implemented. The first session was held at Payam Salamt Clinic. Each session would be started by giving an introduction to the topic of the day and the robot would start the education. Powerpoint slides, movies, and so on were used in the course and after education the students would be motivated and encouraged for better learning. The session would be completed by answering probable questions and removing ambiguities. The sessions would be started by checking the home assignment of the previous session. The participants were required to complete their home assignment if any. Immediately and three months after the intervention the both groups filled out the questionnaire (posttest and follow-up respectively). Since the intervention was free of charge and in clinic under supervision of the authors, all the questionnaires were completed. In observance of ethical codes, the control group received the same educations after the study. A summary of the sessions content is listed in Table 2. It is notable that the study was registered under the code IR.IAU.BOJNOURD.REC.1398.004 in the Ethics Committee of the Islamic Azad University and International Registry of Clinical Trial (ISRCTN17186302).
Data analyses were done using descriptive statistics (frequency, percentage, mean, and standard deviation) and inferential statistics (ANCOVA and ANOVA with repeated measures) (P ≤ 0.05). The data included pretest, posttest, and follow-up data and SPSS (v.25) was used for data analysis.
Findings
Question statements 1: how to design and validate a psychological intervention program with a robot?
To validate the interventions program, triple reciprocal interactions and triangulation method were used. The assessment was done by psychologist experts. To validate using triangulation method, the authors provided the content of session along with detailed explanations and a four-item questionnaire to each expert.
The selected experts expressed their opinions based on a questionnaire for the content of each session. The statements of the questionnaire were designed based on Likert’s ten-point score. The results are listed in Table 3. After summarizing and analyzing the data, the intervention program was validated. To determine reliability of the program, criteria depended reliability tests were used through agreement percentage method.
As listed in Table 4, the mean score of consistency of experts’ opinion about each session is higher than 8. In addition, total mean score of consistency about the total content is 8.46 out of 10. That is, the consistency among experts about the content of each session and all sessions is equal to 85%. This indicates a high reliability of the intervention program. To examine content validity in a quantitative way, content validity ratio (CVR) and content validity index (CVI) were used. Lawshe method was used to obtain CVR of the content [15]. To this end, the items of program were examined using three alternatives including “essential,” “useful,” and “not essential.” The panel members judged every pieces of the content in terms of its necessity. The validity of the tool was obtained as follows:
VCR = content validity ratio
Ne = number of experts that found the session and educational content essential
N = total number of experts
To measure content validity index, Waltz and Bausell was used [16]. The CVI of each item (I-CVI) and total CVI (S-CVI) were obtained [17]. The results supported comprehensiveness of judgements about validity and feasibility of implementation of the final program. To calculate this index, three measure of specificity, simplicity, and clarity were examined for each item of the program using Likert’s four-point score. To measure CVI of each measure, the following formula was used [18]. The S-CVI for each item of the program included total mean scores of the triple measures for that item.
The items with score > 0.79, were evaluated as acceptable. The items with 0.70 < score < 0.79 needed improvement and items with score < 0.70 were unacceptable and eliminated [19]. The mean CVI was used to examine total mean CVI (S-CVI/Ave) [17].
Validity coefficients for the 10 sessions are listed in Table 5. In addition, total content coefficient of the sessions was equal to 80%. Since, the closer the validity coefficient to 1, the higher the validity, validity of the intervention program is supported.
Question statement 2: Does psychological interventions program with a robot affect sexual cares in children?
To answer this question, univariable ANCOVA was used and before that the presumptions like normal distribution of the dependent variable, consistency of variances, and consistency of regression line slope were checked.
As listed in Table 6, the KS and Shapiro Wilk tests support normal distribution of all the elements of the study (p value < 0.05). Therefore, the first presumption is supported. with p value > 0.05, consistency of the variance of the groups is supported. Therefore, the presumption is supported. The f value of the interaction in pretest group is not significant (p = 0.34); therefore, regression line slope of sexual care for the experiment and control groups is identical and the presumption of consistency of regression line slope is supported.
As listed in Table 7, F1.75 = 24.80 indicates that the effect of independent variable is significant (p = 0.00 < 0.01). In other words, there is a significant difference between the mean score of sexual care in posttest stage between the experiment and control groups.
Because of the independent variable (psychological interventions with a robot), the dependent variable (sexual care in children) to measure the effect of interventional programs in pretest, posttest, and follow-up stages on the two groups (experiment and control), frequent measures ANCOVA was used. The results supported the effect of intervention.
As listed in Table 8, the significant effect in a specific stage indicates that the mean scores of children sexual care in pretest and follow-up stages in the experiment and control groups were significantly difference. In other words, posttest and follow-up scores were significantly different between the two groups (p < 0.01). In addition, there was a significant difference between the two groups throughout the study in terms of sexual care. That is, by removing the effect of pretest stage, the increase in sexual care in children in the two groups is notable. Therefore, the psychological interventions with a robot Was effective in improvement of children sexual care (p < 0.01).
Discussion and conclusion
A psychological interventions program with a smart robot for child sexual care was designed and assessed. Child abuse is a social damage and one of the first priorities of social hygiene and health in many countries. Many children become victims of war, sexual abuse, family violence, and human organs trafficking in the world every year. Child abuse (physical, emotional, sexual, and negligence) is not accepted in any society and it is a crime in many countries with heavy punishments [3, 20]. Children older than three years can learn about sexual matters and pertinent cares. Therefore, they can improve their personal safety skills and knowledge about safe relationships [7]. Through educational and consultation process using psychological interventions (behavioral, cognitive, cognitive-behavioral, supportive treatment, interpersonal psychological interaction, mentality, and so on) children can learn communicational skills, interpersonal problem solving, and coping skills to deal with challenges [8]. Education is the most serious and influential way of preventing child sexual abuse. It is emphasized that children and teenagers who have learned these skills in early ages can employ such skills efficiently in their lives.
In examining the first research question based on “design and validate psychological intervention program with a robot” the findings showed that the proposed program can be sued as one of the methods to prevent sexual abuse in children. The program was designed based on literature review [3, 5, 13, 21,22,23,24,25]. After implementing the opinions of psychology experts and modifications, the program was finalized. The key point of this finding is that to determine reliability of the program, criteria depended reliability tests were used through agreement percentage method. The agreement percentage in experts about the final content and total sessions was equal to 85%. The purpose of prevention program was to save children from sexual abuse by self-protection educations and teaching them how to recognize good and bad touches or how to find a trustable adult to seek help. As to the limitations of the study, paucity of similar studies in Iran about the intervention program is notable. As the results showed, future works can focus on skill learning with the help of robots and pilot education design.
In examining the second research question that “does psychological interventions program with a robot affect sexual care in children?” The results showed that the mean score of sexual cares in posttest stage in the experiment group increased compared to pretest stage (p = 0.00 < 0.01; F1.75 = 24.80); while the change in the control group was not significant. Therefore, the program affected the sexual care performance of children. This finding is consistent with Nevena et al., Shamsuddin, Kozima et al., and Robins who showed that robots helped treatment performance in children [26,27,28,29]. Langevin, Czerwinski, Martin, Ladapo et al., and Jin showed that through timely and efficient sexual education to children, the negative effects of child sexual abuse can be avoided [22, 23, 30,31,32]. Ahmadi and Jaberzadeh showed that using proper and timely sexual education, it is possible to improve knowledge of individuals about sexual matters [3, 33]. Khanjari et al. reported that awareness, attitude, and performance of parents affected prevention of sexual misbehaviors in children [34]. Meinck et al., Abeid et al., Citak et al., Gangos et al. showed that educations to prevent child sexual abuse was possible and such measures increased child’s knowledge about preventing and coping skills in the case of any risk of abuse [13, 21, 35, 36]. These results are consistent with our findings except for the fact that the present study examined the effect of psychological interventions using a robot on children sexual care and other studies have focused on specific element or variable separately. There has been no study on all the variables and their interaction so far, and this is a distinguishing feature of the present work.
In general, children have a limited knowledge about their safety and prevention of sexual abuse. Without efficient education, they are not able to tell abusive behaviors from normal behaviors. Studies have shown that increasing one’s knowledge about sexual abuse is the best way to improve self-protection skills [37]. According to UNESCO, the primary goal of sexual education to children is to equip children and teenagers with the knowledge and skills so that they can learn specific values to make reasonable choices about their social and sexual interactions [38]. Despite the alarming statistics of child sexual abuse and children’s need for education in this field, not all parents are ready to talk to their children about such potential risks. Those parents who may talk to their children about sexual abuse tend to have a higher education level or be engaged with the issue more than others (e.g., those who know more about the victims of child sexual abuse or the victims). Personal safety educations to children are as important as education about road traffic or safety. When this education is coordinated with other aspects of growth and cogitation level, it becomes integrated to other aspects of safety and protection [5]. Statistics show that children with more extensive knowledge about sexual topics like good and bad touches, know the name of their sexual organs, and the like are at a lower risk of sexual abuse [20, 39]. Gangos et al. showed in their study that sexual care education affected physical and mental health in children [13]. Wilen et al. reported that psychological interventions helped underaged victims of sexual abuse [40]. To elaborate on this finding, children tend to be less interested in direct education, while combining psychological interventions and playing with a smart robot adds to the attraction of education. In addition, the robot can act as a role model for children. Robots add to the attraction and purposefulness of creativity development in children, which adds to the efficiency of education as children will find the education as an entertainment. Children love playing and eagerly follow the education that is integrated into a game. Psychological interventions program using a smart robot for sexual care education improved mental picturing in children and the depth of learning in them. The intervention emphasized on active participation of children in education based on enabling children to control behavioral change in them and accept their responsibility for their choices [3]. In addition, the interventions alter children’s feelings and attitudes about good and bad touches. The program was a framework for children to express part of their emotions, thoughts, and feelings. Demonstration of narrations about sexual matters, sexual cares, and familiarity with sexual organs enabled children to deal with such issues with more awareness and find creative solutions for them. They could also learn from the experiences shared with them in the course to protect themselves against sexual hazards and control their situation [13]. Therefore, sexual care education not only helps children with their reaction, but also affects their assessment of emotions when experiencing a threatening situation. The program also tried to make the children understand that like physical growth, sexual aspect of their life has its own stages and each stage requires a specific behavior and education. The children also learned about the necessity of preventing sexual abuse [24]. In fact, children tend to have no knowledge about sexual issues and how to deal with individuals who have ill will towards them. In addition, social and religious boundaries are obstacles to proper educations in this field to children. In many cases, children become victims of sexual abuse only because they do not know how to avoid the risks or how to deal with such issues. Such experiences may lead to acute disorders in adulthood and disrupts physical and mental health of children [3]. The program is a new way deal with such challenges. Children can learn the efficient resistance style from the robot and learn about the ways to fight sexual abuse and the risks using the demonstrations in the course. Therefore, the program positively affected sexual cares performance in children.
Availability of data and materials
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
References
Narimani M, Soleymani E, Abolghasemi A (2012) A comparison of internal and external dimensions of thinking styles in blind and sighted students. J Sch Psychol 1(1):108–118
Malek M, Hasanzadeh R, Tirgari A (2013) Effectiveness of group play therapy and cognitive behavioral techniques in reducing behavioral problems in children with reading disorder. J Learn Disabil 2(4):140–153. https://doi.org/10.22098/jld-2-4-92-5-8
Tahan M (2023) Robot-based psychological intervention program for the prevention of child sexual abuse: an overview. Neuropsychopharmacol Hung 25(1):18–25
Forsberg L, Douglas T (2017) Anti-libidinal interventions in sex offenders: medical or correctional? Med Law Rev 24(4):453–473. https://doi.org/10.1093/medlaw/fww003
Yousefzadeh E (2012) Effectiveness of self-protection components training on increasing knowledge and Prevention skills of sexual harassment in preschool girl children. Iran, Master Thesis, Allameh Tabataba'i University
Higa D, Hoppe MJ, Lindhorst T et al (2014) Negative and positive factors associated with the well-being of lesbian, gay, bisexual, transgender, queer, and questioning (LGBTQ) youth. Youth Soc 46(5):663–687. https://doi.org/10.1353/etc.2007.0016
Dautenhahn K (2007) Socially intelligent robots: dimensions of human-robot interaction. Philos Trans R Soc Lond B Biol Sci 362(1480):679–704. https://doi.org/10.1098/rstb.2006.2004
Churchill R, Moore TH, Caldwell D et al (2010) Cognitive behavioural therapies versus other psychological therapies for depression. Cochrane Database Syst Rev 9:CD008698. https://doi.org/10.1002/14651858.CD008698
Baxter P, Ashurst E, Read R, Kennedy J & Belpaeme T (2017) Robot education peers in a situated primary school study: Personalization promotes child learning. PLOS One 12(5). https://doi.org/10.1371/journal.pone.0178126.
Mushrafian Dehkordi L (2017) Child abuse, causes and types with reference to the rights of the child and the important role of the family in its occurrence. No-Andish Sabz Publications, Tehran
Tutty LM (1995) The revised Children’s Knowledge of Abuse Questionnaire: development of a measure of children’s understanding of sexual abuse prevention concepts. Soc Work Res 19(2):112–120. https://doi.org/10.1093/swr/19.2.112
Jacqueline L, Holloway & Mary L, Pulido (2018) Sexual abuse prevention concept knowledge: low income children are learning but still lagging. J Child Sex Abuse 27(6): 642-662. https://doi.org/10.1080/10538712.2018.1496506
Gangos CJ, Nega C, Apergi FS (2018) Adaptation and psychometric evaluation of the Children’s Knowledge of Abuse Questionnaire (CKAQ-RIII) in Greek Elementary School Children. Journal homepage 4:2–18. https://doi.org/10.1080/10538712.2018.1538175
Tahan M (2019) Artificial Intelligence applications and psychology: an overview. Neuropsychopharmacol Hung 21(3):119–126
Lawshe CH (1975) A qualitative approach to content validity. Pers Psychol 28(4):563–575. https://doi.org/10.1111/j.1744-6570.1975.tb01393.x
Waltz CF, Bausell BR (1981) Nursing research: design statistics and computer analysis. Davis FA, New York
Zamanzadeh V, Ghahramanian A, Rassouli M, Abbaszadeh A, Alavi-Majd H, Nikanfar AR (2015) Design and implementation content validity study: development of an instrument for measuring patient-centered communication. J Caring Sc 4(2):165–178. https://doi.org/10.15171/jcs.2015.017
Katherine MD, Christine AG (2000) Child sexual abuse prevention programs: a meta-analysis. J Clin Child Psychol 29(2):257–265. https://doi.org/10.1207/S15374424jccp2902_11
Hajizadeh E, Asghari M (2018) Statistical methods and analyzes with a view to research methods in biological and health sciences. Academic Jahad Publishing Organization, Tehran
Tahan M, Afrooz GA, Bolhari J (2021) The effectiveness of smart robot psychological intervention program on good sexual care for elementary school children. Shenakht J Psychol Psychiatry 7(6):53–65. https://doi.org/10.52547/shenakht.7.6.53
Citak Tunc G, Gorak G, Ozyazicioglu N, Ak B, Ozlem I, Pinar V (2018) Preventing child sexual abuse: body safety training for young children in Turkey. J Child Sex Abus 27(4):347–364. https://doi.org/10.1080/10538712.2018.1477001
Czerwinski F, Finne E, Alfes J, Kolip P (2018) Effectiveness of a school-based intervention to prevent child sexual abuse-Evaluation of the German IGEL program. Child Abuse Negl 86:109–122. https://doi.org/10.1016/j.chiabu.2018.08.023
Jin Y, Chen J, Jiang Y (2017) Evaluation of a sexual abuse prevention education program for school-age children in China: a comparison of teachers and parents as instructors. Health Educ Res 32(4):364–373. https://doi.org/10.1093/her/cyx047
Najari F (2018) Designing and developing a sex education program for preschool children. Master Thesis, Scientific Training Center, Applied Welfare and Social Security of South Khorasan Province
Ghazizadeh S (2015) Effectiveness of trauma-focused cognitive behavioral therapy on cognitive emotion regulation strategies and improvement of post-traumatic stress disorder symptoms in sexually abused children: a single case study. Iran, Master thesis of Ferdowsi University of Mashhad
Nevena A, Vesna K, Ana T, Liljana B, Adrijan B (2017) Robot - assisted therapy for autistic children. Concord, Southeast Con., https://doi.org/10.1109/SECON.2017.7925401
Shamsuddin S, Yussof H, Ismail LI, Mohamed S, Hanapiah FA, Zahari NI (2012) Initial response in HRI-A case study on evaluation of child with Autism Spectrum Disorders interacting with a humanoid robot NAO. Procedia Engineering 41:1448–1455. https://doi.org/10.1016/j.proeng.2012.07.334
Kozima H, Michalowski MP, Nakagawa C (2009) Keepon. Int J of Soc Robotics 1:3–18. https://doi.org/10.1007/s12369-008-0009-8
Robins K, Dautenhahn R, Te Boekhorst B (2005) Robotic assistants in therapy and education of children with autism: can a small humanoid robot help encourage social interaction skills? Univ Access Inf Soc 4:105–120. https://doi.org/10.1007/s10209-005-0116-3
Langevin R, Cossette L, Hebert M (2016) Emotion regulation in sexual abuse preschoolers. Child Psychiatry Hum Dev 47(1):1–12. https://doi.org/10.1007/s10578-015-0538-y
Martin KA (2014) Making sense of children’s sexual behavior in child care: analysis of adult responses in special investigation reports. Child Abuse Negl 38:1636–1646. https://doi.org/10.1016/j.chiabu.2014.07.002
Ladapo JA, Elliott MN, Bogart LM, Kanouse DE, Vestal KD, Klein DJ, Ratner JA, Schuster MA (2012) Cost of talking parents, healthy teens: a worksite-based intervention to promote parente adolescent sexual health communication. J Adolesc Health 53:595–601. https://doi.org/10.1016/j.jadohealth.2012.11.015
Ahmadi T (2011) Assessing the needs of the sex education curriculum from the point of view of middle school teachers of an educational district of Shiraz from 1990-1991. Iran, Master’s Thesis, Curriculum Planning, Islamic Azad University of Marvdasht
Khanjari S, Bastani F, Kamalinahad R, Hosseini A (2014) Prevention of child sexual abuse: parents’ knowledge, attitudes and practices. IJN 27(89):12–20. https://doi.org/10.29252/ijn.27.89.12
Meinck F, Cluver LD, Boyes ME, Mhlongo EL (2015) Risk and protective factors for physical and sexual abuse of children and adolescents in Africa: a review and implications for practice. Trauma Violence Abuse 16(1):81–107. https://doi.org/10.1177/1524838014523336
Abeid M, Muganyizi P, Olsson P. et al (2014) Community perceptions of rape and child sexual abuse: a qualitative study in rural Tanzania. BMC Int Health Hum Rights 14(23). https://doi.org/10.1186/1472-698X-14-23
Kolahi Heshmat F (2017) Examining and comparing the level of sexual vulnerability of female and adolescent male students in north and south of Tehran. Master's thesis. Iran, Allameh Tabataba'i University
Unesco (2018) International technical guidance on sexuality education. Unesco: Paris. Online at: http://data.unaids.org/pub/ExternalDocument/2009/20091210_international_guidance_sexuality_education_vol_2_en.pdf
Kenny MC, Capri V, Thakkar-Kolar R, Runyon MK (2008) Child sexual abuse: from prevention to self-protection. Child Abuse Rev 17:36–54. https://doi.org/10.1002/car.1012
Wilen JS, Littell JH, Salanti G (2017) Psychosocial interventions for adults who were sexually abused as children. Cochrane Database Syst Rev 2017(1):CD010099. https://doi.org/10.1002/14651858.CD010099.pub2
Acknowledgements
Further we would also like to express our thankful, gratitude to all the research participants, who participated in this study.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
MT designed the study and conducted the literature searches, wrote the first draft of the manuscript. MT, GA, and JB assisted in the methodology and planning of the clinical trial. GA and JB revised the draft of the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
To adhere to ethical considerations, In the present study, the parents who were interested in participation in the study were asked to sign a written letter of consent for their child’s participation in the study. The participants were ensured that their personal and private information will remain confidential and that the study is in compliance with religious and cultural code. It is notable that the current research was approved by the ethics committee of the Islamic Azad University with the code if IR.IAU.BOJNOURD.REC.1398.004 and this study registered in International Clinical Trial Registry Platform by number ISRCTN17186302.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tahan, M., Afrooz, G. & Bolhari, J. Designing, assessing, and effectiveness a psychological interventions program with a robot for children sexual care. Middle East Curr Psychiatry 30, 73 (2023). https://doi.org/10.1186/s43045-023-00347-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-023-00347-9