
Abstract
Background
Suicide has become a major threat to achieving Sustainable Development Goals three and four, especially for school-going adolescents worldwide. As part of efforts to prevent suicide, population-based studies regarding the prevalence and variables that predict suicidal behaviours are required to inform decisions. Despite this realisation, Samoa lacks empirical data on suicidal behaviours among adolescents. We conducted a secondary analysis of the 2017 Global School-based Student Health Survey to examine the prevalence of suicidal behaviours (idea, plan, and attempt) of school-going adolescents in Samoa.
Results
The prevalence of suicidal ideation, plan, and attempt was 24.1%, 23.8%, and 21.8%, respectively. Also, we found that having understanding parents was an important protective factor against all three suicidal behaviours among Samoan in-school adolescents. Suicidal ideation was predicted by cigarette smoking, having someone who smokes in adolescents’ presence, bullying, loneliness, and worrying about things they could not study. Also, cigarette smoking, bullying, having multiple sexual partners, and worrying increased the risk of having suicidal plans. Again, adolescents’ suicidal attempt was predicted by adolescent truancy, alcohol use, cigarette smoking, being bullied, having close friends, loneliness, and worry.
Conclusions
Rather than focusing on the school setting alone, suicide prevention interventions in Samoa should foster interdisciplinary collaborations to help reduce suicide.
Similar content being viewed by others


Introduction
Suicide accounts for over 700,000 global deaths, almost 80% in low- and middle-income countries [48]. Among suicide cases recorded annually, adolescent suicide consistently increases over time [2]. This rate is particularly of concern for adolescents due to the vast years of potential life lost. Among people aged 15 to 29 years, suicide ranks as the fourth most common cause of death [48]. Suicidal behaviours usually involve suicidal ideation, planning, and attempt. Adolescent suicide has been identified as a serious public health problem in all economies. In 2020, suicide was the cause of 45,979 fatalities in the USA [7].
Recent statistics indicate suicide was the second-leading cause of death in 2020 for people aged 10 to 24 [3]. In 2017, there were over 1000 suicides among young people aged 15 to 19 in the European Union, with boys making up most of these deaths. Despite the comparatively low absolute number of adolescent suicides, this age group’s leading cause of death is suicide [24]. Adolescents in low-income and middle-income nations, particularly in Africa and the Western Pacific, and girls aged 15 to 17 are more likely to have suicidal behaviours [44]. In countries like Mozambique, the prevalence of suicidal behaviours was as follows; ideation (17.7%), plan (19.6%), and attempt (18.5%) [38]. The prevalence of suicidal behaviours was also high in Ghana, with a prevalence of ideation (18.2%), plan (22.5%), and attempt (22.2%) [26].
According to data from the 2016 State of the World Children (SOWC), adolescents in Samoa make up 22% of the total population, which is a much larger percentage than the 13% regional average for East Asia and the Pacific [45]. For the past 20 years, suicide-specific death among Samoans has consistently exceeded the world average. While the world average of suicidal deaths as of 2019 was 9.49 per 100,000 people, that of Samoa was 12.6 per 100,000, with marked gender differences of 6.7 per 100,000 for females against 18 per 100,000 for males (World Bank, 2022). Adolescents in Samoa have particularly been identified as a high-risk group for suicidal behaviours, with the most recent data showing that the suicide rate among adolescents aged 15–19 is 18.13 suicides per 100,000, also with sex variations of 22.13 per 100,000 for males and 13.17 per 100,000 for females. Additionally, the 15–24 years age group were the second highest contributor to suicidal deaths in Samoa.
Similarly, earlier studies have identified specific predictors associated with an increased risk of suicidal behaviours in low- and middle-income countries. These predictors included food insecurity, bullying, loneliness, anxiety, cigarette smoking, and alcohol use [21]. This finding is consistent with existing studies but for gender disparities in predictors. For example, a survey from 90 countries indicates that being bullied continued to be a key problem for girls,however, having no friends, being bullied, and being physically injured remained significant predictors of suicide attempts in boys [6]. Hunger and bullying were significant predictors for ideation and attempt, respectively, while the physical attack was associated with suicidal ideation, plan and attempt [38].
Progress towards achieving Sustainable Development Goal (SDG) 3.4.2 of reducing the suicide mortality rate requires that the issue of suicide is tackled. In Samoa, the previous studies on the prevalence of suicide behaviours among school-going adolescents are alarmingly high [44]. Many researchers [6, 9, 18, 22] have relied on the Global School-based Student Health Survey (GSHS) to understand the suicidal behaviours of adolescents. The findings of previous studies [1, 21] are based on older versions of the GSHS and may not reflect current happenings. This study aims to investigate the occurrence and associated factors of suicidal behaviours among school-going adolescents in Samoa using the most current version of the GSHS data.
Conceptual framework of adolescent suicide
We conceptualised adolescent suicidal behaviours to be made up of suicidal ideation, plan, and attempt. Our conceptual framework is based on the risk and protective factors model [12] and literature on correlates of adolescent suicidal behaviours [4, 13, 26, 36,37,38]. This framework proposes that within a specific population, there are factors that can either decrease (protective factors) or increase (risk factors) the likelihood of an adolescent exhibiting any suicidal behaviour [4, 13, 18, 26, 27, 36,37,38]. These explanatory variables included adolescent sociodemographic characteristics such as sex, age, and grade. Also, the other factors include personal like adolescent truancy at school and hunger, drugs and substance use, and psychosocial characteristics of adolescents in Samoa.
In our study, the sex of the participants and their parental characteristics were conceptualised as protective factors. We also considered personal factors like truancy and hunger, drugs and substance use, and other psychosocial factors like bullying and loneliness as risk factors. These correlates have often provided mixed findings in similar studies in settings like Bangladesh [22], Brunei Darussalam [40], Ghana [26], Guatemala [29, 30], Indonesia [22], Indonesia [35], Iran [50], Mozambique [38], and Tonga [32].
Method
Design
Using 2017 GSHS data, we examined suicide and its correlates among school-aged adolescents in Samoa. The WHO repository contains these secondary open data. A self-administered questionnaire was used in the GSHS to obtain data on young people’s physical, social, and mental health habits. The GSHS was developed with WHO, Samoa’s Ministry of Health (MoH), and the Centres for Disease Control and Prevention (CDC). A cross-sectional study methodology was used to collect data from WHO member countries interested in reducing teen suicide. In Samoa, data was collected from school-aged teenagers aged 13 to 17.
Sampling
In the 2017 Samoa GSHS, a two-stage cluster sample design was used to obtain data representing all students between 13 and 17 years. Schools in Samoa were chosen with a probability proportionate to enrollment size in the first stage. Classes were randomly selected in the second round, and all students in those classes could participate. The overall response rate was 59%, with 94% from the institution and 63% from the students.
Variables
The outcome variables in this study were “Suicide ideation, plan, and attempt” among the students. The study measured each of the suicide behaviours during the past 12 months (suicide ideation, suicide plan, and suicide attempt) with a single self-report item or question. The responses to these questions were categorised as “yes” (1) or “no” (0).
We also classified the explanatory variables as sociodemographic (sex, age, and grade), personal (school truancy, hunger), drugs and substance use (adolescent use of amphetamine, marijuana smoking, alcohol), and psychosocial (physical attacks, and bullying victimisation). Except for sociodemographic (sex: 1 = male, 0 = female; age: 1 = 12–14, 0 = 15–17; and grade: 0 = grades 1–3, 1 = grades 4–6), all other explanatory variables were categorised as “yes” (1) or “no” (0).
Data analysis
We employed the sample weighting technique at the school, student, and also for sex within grade levels to prevent bias on various nonresponse tendencies and make the findings a reflection of school-going teenagers in Samoa. We assessed the final model’s goodness of fit, and the results indicated no evidence of a lack of fit with our model’s capacity to predict suicidal behaviours. We also performed bivariate analysis using Pearson chi-square to measure the relationships between variables. The covariates that showed a significant correlation (p0.05) were then incorporated into a binomial logistic regression model. The results of the study were provided with the corresponding adjusted odds ratio (AOR) at a 95% confidence interval (CI) (p0.05).
Results
Background characteristics of adolescents in Samoa
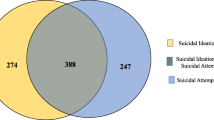
The prevalence of suicide behaviours in Samoa was 24.1% ideation, 23.8% plan and 21.8% attempt (see Fig. 1). Significantly, truant participants experienced suicidal ideation (9.9%), plan (1.0%), and attempted suicide (10.3%). Also, amphetamine use significantly influenced suicidal ideation (2.3%), plan (2.6%), and attempt (3.1%). Marijuana use, alcohol consumption and cigarette smoking were significantly associated with suicide ideation (3.2%, 4.9%, and 5.1%), plan (3.6%, 5.1%, and 5.4%), and attempt (3.7%, 5.6%, and 5.2%), respectively. Moreover, participants who got drunk after consuming too much alcohol reported suicidal ideation (4.0%), plan (4.3%), and attempted suicide (4.0%). Also, participants who were physically attacked, engaged in a physical fight, seriously injured, and those who were bullied significantly experienced suicidal ideation (6.4%, 1.3%, 13.8% and 11.9%), plan (6.1%, 12.0%, 12.5%, and 11.7%), and attempted suicide (6.4%, 11.5%, 12.8% and 11.6%) respectively. Adolescents who mostly felt lonely, people smoked in their presence, and those who worried about what they could not study significantly experienced suicidal ideation (4.0%, 18.5%, 2.7%), plan (3.7%, 17.8%, 4.3%) and suicide attempt (4.2%, 16.6%, 4.4%) respectively. Also, participants who had multiple sexual partners and those with understanding parents significantly had suicidal ideation (3.6%, 4.6%), plan (3.9%, 5.1%), and attempt (3.9%, 4.5%), respectively. Further, participants whose parents checked on whether they had done their assignment and those whose parents knew what they do with their free time significantly experienced suicidal thoughts (10.3%, 6.4%), plan (10.6%, 6.4%), and attempted suicide (9.3%, 5.2%) respectively. However, participants who did not have close friends and those who had parents/guardians who use any form of tobacco significantly influenced only suicide plans (3.0%, 8.0%) and attempts (3.1%, 7.6%), respectively (see Table 1).

Prevalence of suicide behaviours (suicide thoughts, plan, and attempt) among school-going adolescents in Samoa
Bivariate analysis
Table 2 shows the chi-square analysis of the relationship between outcome and explanatory variables. Personal factor like truancy was significantly associated with suicidal ideation (p < 0.006), plan (p < 0.002), and attempt (p < 0.001). Also, using drugs or substances significantly predicted suicide behaviours. For instance, amphetamines use was significantly associated with suicide ideation (p < 0.004), suicide plan (p < 0.001) and suicide attempt (p < 0.001). Also, marijuana use was significantly associated with suicide ideation (p < 0.001), plan (p < 0.001), and attempt (p < 0.001). Further alcohol use was significantly associated with suicide ideation (p < 0.001), plan (p < 0.001), and attempt (p < 0.001). Also, smoking cigarettes was significantly associated with suicide ideation (p < 0.001), plan (p < 0.001), and attempt (p < 0.001). Again, related psychosocial factors were significantly associated with suicidal behaviours. For instance, experiencing a physical attack was significantly associated with suicide ideation (p < 0.001), suicide plan (p < 0.001), and attempt (p < 0.001). Also, the physical fight was associated with suicide ideation (p < 0.001), plan (p < 0.001), and attempt (p < 0.001). Experiencing serious injuries and bully were significantly associated with suicide ideation (p < 0.000, p < 0.001), plan (p < 0.002, p < 0.001), and attempt (p < 0.001, p < 0.001), respectively.
Furthermore, loneliness and worrying about things an adolescent could not study were significantly associated with suicide ideation (p < 0.001, p < 0.001), plan (p < 0.001, p < 0.001), and attempt (p < 0.001, p < 0.001), respectively. Further, having multiple sexual partners and people smoking in an adolescent’s presence were significantly associated with suicide ideation (p < 0.001, p < 0.000), plan (p < 0.000, p < 0.002), and attempt (p < 0.000, p < 0.003) respectively. Again, having parents/guardians who check if adolescents have done their homework and having an understanding of parents were significantly associated with suicide ideation (p < 0.002, p < 0.001), plan (p < 0.030, p < 0.004), and attempt (p < 0.004, p < 0.005) respectively. Also, having parents/guardians who knew what children do in their free time was significantly associated with suicide ideation (p < 0.010), plan (p < 0.019), and attempt (p < 0.000). Again, having close friends (p < 0.003, p < 0.001) and parental/guardian use of tobacco (p < 0.011, p < 0.002) were significantly associated with only suicidal plans and attempts, respectively (see Table 1).
Multivariate analysis
Table 2 shows the logistic regression for predictors of suicide behaviours (ideation, plan, and attempt. Adjusting for the results, compared to non-truant participants, truant participants were more likely to attempt suicide (AOR = 1.34, 95%CI = 1.038–1.736). Also, participants who use alcohol are more likely to attempt than those who do not use alcohol (AOR = 1.34, 95%CI = 1.038–1.736). Again, compared to those who do not smoke cigarettes, those who smoke cigarettes were more likely to have suicidal thoughts (AOR = 1.83, 95%CI = 1.281–2.602), plan (AOR = 2.12, 95%CI = 1.494–3.020), and attempt (AOR = 1.74, 95%CI = 1.205–2.506). Also, bullied victims were more likely to have suicidal ideation (AOR = 1.66, 95%CI = 1.298–2.111), plan (AOR = 1.75, 95%CI = 1.369–2.236), and attempt (AOR = 1.91, 95%CI = 1.476–2.467) than those who were not bullied.
Compared to those who do not have understanding parents, those with understanding parents were less likely to have suicide ideas (AOR = 0.58, 95%CI = 0.429–0.782), plan (AOR = 0.70, 95%CI = 0.520–0.934), and attempt suicide (AOR = . 68, 95%CI = 0.495–0.929). Having multiple partners predicted only suicide plans (AOR = 1.51, 95%CI = 1.016–2.243), while not having close friends predicted only suicide attempts (AOR = 1.75, 95%CI = 1.186–2.582). Loneliness increased the odds of having suicide ideas (AOR = 1.60, 95%CI = 1.125–2.286) and suicide attempts (AOR = 1.88, 95%CI = 1.303–2.720). Also, worry about things participants could not study increased the odds of experiencing suicidal thoughts (AOR = 1.95, 95%CI = 1.375–2.754), plan (AOR = 1.91, 95%CI = 1.190–2.409), and attempt (AOR = 1.89, 95%CI = 0.311–2.723) (see Table 2).
Discussion
Given the public health significance of suicide prevention among adolescents to meet SDGs 3 and 4, our study examined the prevalence and factors that predict suicidal behaviours among school-going adolescents in Samoa using data set from the 2017 GSHS. Among this population, the prevalence of suicidal ideation, plan, and attempt was 24.1%, 23.8%, and 21.8%, respectively. The prevalence of suicidal ideation among Samoan adolescents is relatively higher compared to GSHS findings of studies from countries such as Ghana [26], Iran [50], and Indonesia [35]. Also, the prevalence of suicidal plan among this study’s population is higher compared with evidence from Bangladesh and Indonesia [22], Mozambique [38], and Brunei Darussalam [40]. Again, the prevalence of suicidal attempts among our study population is higher than those reported in Saint Vincent and the Grenadines (SVATG) [37], Tonga [32] and Guatemala [29, 30]. Interestingly, these studies conducted in WHO member countries also utilised data sets from GSHS, which provided a neutral ground for comparing prevalence rates. The relatively higher prevalence of suicidal behaviours among adolescents in Samoa signifies the problematic nature of suicide among the population. Suicide prevention interventions should be prioritised in Samoan schools to help combat this canker among school-going adolescents.
Aside from measuring the prevalence of suicidal behaviours among Samoan in-school adolescents, our results observed that understanding parents was the only significant protective factor conceptualised in our study. Similar to our study finding, parents who are considerate, understanding, and supportive of adolescents have been reported to be an important protective factor against suicidal behaviours in several studies [23, 36]. This finding implies that parents have a major role to play in reducing suicide risk among adolescents. Since adolescence is a period of transitioning into adulthood, parental support and guidance expressed through understanding adolescents’ problems and needs will help adolescents appreciate life’s beauty and disengage from suicidal risk behaviours.
After adjusting for other predictor variables, we found that adolescents who were truant in school were at higher risk of attempting suicide. This finding corroborates evidence from SVATG [37], Nepal [27], Tonga [32], and five Southeast Asian countries (Indonesia, Laos, Philippines, Thailand, and Timor-Leste) [31], which predicted a strong association between truancy and adolescents’ suicidal behaviours. From our perspective, the link between truancy and suicidal attempt can be explained on the basis that most adolescents who are truant from school may fall victim to externalising behaviours (substance use, physical attack, bullying, and fight victimisation) and high internalising behaviours [29, 30] which may predispose them to suicidal attempt. Rather than focusing on the school setting alone, truancy prevention interventions in Samoa should foster interdisciplinary collaboration between stakeholders and policymakers.
Among our study population, the use of alcohol was found as a significant risk factor for a suicidal attempt. Also, smoking cigarettes increases the odds of ideating, planning, and attempting suicide. Again, having people who smoke in adolescents’ presence increases their risk of ideating suicide. The predictive link between substance use (alcohol use and cigarette smoking) and suicidal behaviours has been substantiated by the findings of several studies [8, 10, 19, 39]. Given that alcohol is a sedative and stimulant [14], we suggested that alcohol use might impair adolescents’ decision-making, driving their impulsivity toward suicide. Schools in Samoa need to pay particular attention to substance-use risk assessment interventions to identify students at risk of substance use and those already using them to inform policies and interventions for suicide prevention.
We also found that school-going adolescents in Samoa who were bullied were highly predisposed to ideating, planning, and attempting suicide than their peers who were not bully-victimised. Findings of several previous studies have validated the predictive association between bullying of any form and the suicidal behaviours of adolescents [15, 17, 41, 49]. Adolescents who do not have well-adaptive mechanisms against the psychosocially devastating consequences of bullying, suicide ideation, plan, or attempt may be seen as an option. This finding may partly explain this observed outcome among adolescents in Samoa. Multi-collaborative efforts between Samoan school administrations, policymakers, parents and teachers will significantly prevent bullying among school-going adolescents on- and off-campus.
In line with previous studies which found multiple sexual relationships as a significant risk factor for suicidal behaviours [33, 43], our study found that having multiple sexual partners increased Samoan school-going adolescents’ odds for suicidal plans. This finding can be explained from the perspective of intimate partner violence mainly occurring among adolescents, possibly predisposing them to suicidal behaviours. Adolescents in Samoa must be educated on the risks and negative consequences of practising multiple sexual relationships.
Contrary to our study findings which found having close friends as a predictive factor of suicidal attempts among school-going adolescents in Samoa, Seidu et al. [38] found having close friends as a protective factor. The study findings of Campisi et al. [6],and Pengpid and Peltzer [31] also contradict ours, as they reported having no close friends instead increased the risk of suicide. However, our study finding corroborates Oppong Asante et al. [26] and Sarfo et al. [37]. Close friends significantly influence their negative or positive peers. In the case of school-going adolescents in Samoa, it could be that their close friends might have been engaged in suicide risk behaviours or may be ideating, planning or attempting suicide, which increased their vulnerability to suicidal behaviours. Parents and teachers in Samoa should develop a keen interest in school-going adolescents’ friendships and help them make meaningful choices regarding the company they keep.
The psychosocial state of being lonely increased the possibility of ideating and planning suicide among our study population. Our finding is supported by some previous studies [11, 28]. Similarly, our study confirmed the results of previous studies in which the state of worrying was a significant predictor of suicidal behaviours [20, 37].
Conclusion
Using data from the 2017 GSHS, the study discovered that suicide conduct was highly common among Samoan school-aged teenagers. We found that teenagers with understanding parents protected against suicide activity in the research population after controlling for other characteristics linked with suicidal behaviour (idea, plan, and attempt). Furthermore, multiple risk variables predicted the chance of some or all suicidal behaviours among the individuals in our study. Cigarette smoking, having someone who smokes in the company of teenagers, bullying, loneliness, and worrying about topics an adolescent could not study, for example, all predicted suicidal thoughts. Cigarette smoking, bullying, having several sexual partners, and worrying all raised the likelihood of suicide ideation. In contrast, suicidal attempts were predicted by truancy, alcohol use, cigarette smoking, bullying, having close friends, loneliness, and worrying about things an adolescent could not study.
If this incidence of suicidal conduct continues, Samoa may be unable to ensure healthy lives for these school-age teens by 2030, create opportunities for lifelong learning, or provide inclusive and equitable quality education. Government, school administration, parents, and other stakeholders must adopt policies and programmes to assist and influence teens’ conduct at school and home. Samoa would also benefit from proactive initiatives to minimise the prevalence of suicidal behaviour in order to reach several SDG objectives, specifically SDGs 3.5 and 4.1. Students must have access to services to assist with their psychosocial and mental health needs.
Strengths and limitation
Our study examines adolescent suicide behaviours in Samoa using a national dataset that covers all in-school adolescents. Since our sample is very representative, we can learn more about the factors that make it more likely for these Samoan adolescents to engage in suicidal behaviours. Notwithstanding these strengths, our study is limited in several aspects. As a secondary data study, we were restricted to using only explanatory variables included in the WHO’s GSHS questionnaire.
Furthermore, because the GSHS is a cross-sectional database, we could not account for causal relationships between the various risk variables and suicidal conduct. Again, utilising a single dichotomised question to evaluate mental health categories such as suicidal behaviour, concern, loneliness, and parental traits may not capture all elements of the variables. A question style like this may not effectively offer a meaningful estimate of all essential clinical symptoms for diagnostic reasons. Despite these limitations, our study provides important findings that would inform research, policy, and adolescent-focused interventions in Samoa. These constraints must also govern the interpretation and application of our study’s findings.
Implications for research and intervention
We measured the prevalence and correlates of suicidal behaviours among adolescents in the island country of Samoa. We wanted to look for protective characteristics and risk factors that make people more prone to suicide. This section highlighted a few prospective research initiatives and tactics for preventing suicide behaviours. First, school administrators and teachers in Samoa must obtain suicide literacy training on recognising early warning signals among their adolescent students. Training school staff to act as gatekeepers is a major concern for effective school-based suicide prevention programmes [34]. This will increase their competence and confidence in identifying early warning signs, assessing the risk of suicide, and linking these troubled adolescents to school-based resources [42, 46]. This intervention would include appointing some school staff members as mental health points of contact or contact points and training them on the essential skills for recognising learners who are vulnerable to suicide [26].
The relevance of the family and social connections in suicidality is reflected in the fact that parental-associated risk variables were strongly related to suicidal behaviours among students in the current study. As a result, the family’s role in preventing youth suicide might be contradictory depending on whether it is protective or risky [16]. In the past decade, it has been discovered that connection offers a conceptual framework for pursuing a public health prevention agenda in the area of teenage suicide behaviours, where parents’ awareness of adolescents in distress requesting help and encouraging them to seek care becomes crucial. According to Whitlock et al. [47], an important prevention goal is community-based initiatives that educate parents about adolescent distress and how to relate to and assist their children [25]. Again, parenting practices have a major impact on teenage suicide behaviour; hence, community-based programs should educate parents on how their parenting practices affect adolescent suicidal behaviour.
Initiatives to prevent suicidal behaviour should focus heavily on adolescents’ use of drugs and other substances. The use of amphetamine, marijuana, tobacco, alcohol, cigarettes and other drugs has been associated with various suicide behaviours. Additionally, researchers have found a connection between student drug and substance use and subpar academic results [5]. Eliminating student substance use would improve both academic performance and aggressiveness levels. According to Botvin and Griffin [5], the educational system or environment could not be disregarded in efforts to prevent teenage drug and alcohol use. By providing chances for skill development in areas like music, athletics, and other activities that stimulate teenagers’ interests and act as an alternative to drug use. More significantly, teachers should give children the tools to increase their self-esteem and confidence to resist peer pressure and media messages.
Availability of data and materials
We used data from the GSHS database. WHO and the CDC support this open data, which is freely available at: https://extranet.who.int/ncdsmicrodata/index.php/catalog/773/study-description.
Abbreviations
- AOR:
-
Adjusted odds ratio
- CDC:
-
Centers for Disease Control and Prevention
- CI:
-
Confidence interval
- GSHS:
-
Global School-based Student Health Survey
- MoE:
-
Ministry of Education
- MoH:
-
Ministry of Health
- SVATG:
-
Saint Vincent and the Grenadines
- SDG:
-
Sustainable Development Goal
- WHO:
-
World Health Organization
References
Abio A, Owusu PN, Posti JP, Bärnighausen T, Shaikh MA, Shankar V, Lowery Wilson M (2022) Cross-national examination of adolescent suicidal behavior: a pooled and multi-level analysis of 193,484 students from 53 LMIC countries. Soc Psychiatry Psychiatr Epidemiol 57(8):1603–1613. https://doi.org/10.1007/s00127-022-02287-x
Abraham ZK, Sher L (2019) Adolescent suicide as a global public health issue. Int J Adolesc Med Health 31(4):20170036. https://doi.org/10.1515/ijamh-2017-0036
America’s Health Rankings. (2022). Retrieved from https://www.americashealthrankings.org/explore/health-of-women-and-children/measure/teen_suicide/state/ALL
Ati NA, Paraswati MD, Windarwati HD (2021) What are the risk factors and protective factors of suicidal behaviour in adolescents? A systematic review. J Child Adolesc Psychiatr Nurs 34(1):7–18
Botvin GJ, Griffin KW (2003) Drug abuse prevention curricula in schools. In: Sloboda Z, Bukoski WJ (eds) Handbook of drug abuse prevention: Theory, science, and practice. Kluwer Academic/Plenum Publishers, New York, pp 45–74
Campisi SC, Carducci B, Akseer N, Zasowski C, Szatmari P, Bhutta ZA (2020) Suicidal behaviours among adolescents from 90 countries: a pooled analysis of the global school-based student health survey. BMC Public Health 20(1):1–11. https://doi.org/10.1186/s12889-020-09209-z
Centers for Disease Control and Prevention. (2020). Suicide: Facts at a Glance. https://www.cdc.gov/suicide/facts/index.html
Conner KR, Bagge CL (2019) Suicidal behavior: links between alcohol use disorder and acute use of alcohol. Alcohol Res 40(1):e1–e4. https://doi.org/10.35946/ARCR.V40.1.02
Dema T, Tripathy JP, Thinley S, Rani M, Dhendup T, Laxmeshwar C, Tenzin K, Gurung MS, Tshering T, Subba DK, Penjore T, Lhazeen K (2019) Suicidal ideation and attempt among school going adolescents in Bhutan – a secondary analysis of a global school-based student health survey in Bhutan 2016. BMC Public Health 19(1):1605. https://doi.org/10.1186/s12889-019-7791-0
Esang M, Ahmed S. (2018). A closer look at substance use and suicide. Https://Doi.Org/https://doi.org/10.1176/Appi.Ajp-Rj.2018.130603, 13(6), 6–8. https://doi.org/10.1176/APPI.AJP-RJ.2018.130603
Gomboc V, Krohne N, Lavrič M, Podlogar T, Poštuvan V, ZadravecŠedivy N, De Leo D (2021) Emotional and social loneliness as predictors of suicidal ideation in different age groups. Commun Mental Health J 58(2):311–320. https://doi.org/10.1007/S10597-021-00823-8
Hawkins JD, Catalano RF, Miller JY (1992) Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psycholog Bull 112(1):64–105. https://doi.org/10.1037/0033-2909.112.1.64
Huang HW, Wang RH (2019) Roles of protective factors and risk factors in suicidal ideation among adolescents in Taiwan. Public Health Nurs 36(2):155–163
Hendler RA, Ramchandani VA, Gilman J, Hommer DW (2013) Stimulant and sedative effects of alcohol. Curr Top Behav Neurosci 13:489–509. https://doi.org/10.1007/7854_2011_135
Holt MK, Vivolo-Kantor AM, Polanin JR, Holland KM, DeGue S, Matjasko JL, Reid G (2015) Bullying and suicidal ideation and behaviors: a meta-analysis. Pediatrics 135(2):e496–e509. https://doi.org/10.1542/PEDS.2014-1864
Hooven C (2013) Parents-CARE: a suicide prevention program for parents of at-risk youth. J Child Adolesc Psychiatr Nurs 26(1):85–95
John A, Glendenning AC, Marchant A, Montgomery P, Stewart A, Wood S, Hawton K. (2018). Self-harm, suicidal behaviours, and cyberbullying in children and young people: systematic review. J Med Internet Res 2018;20(4):E129. Https://Www.Jmir.Org/2018/4/E129, 20(4), e9044. 10.2196/JMIR.9044.
Khan M, Ali M, Rahman M, Islam M, Karim M, Hasan M, Jesmin SS (2020) Suicidal behaviour among school-going adolescents in Bangladesh: findings of the global school-based student health survey. Soc Psychiatry Psychiatr Epidemiol 55(11):1491–1502
Kim SH, Jeong SH, Park EC, Jang SI (2021) Association of cigarette type initially smoked with suicidal behaviors among adolescents in Korea from 2015 to 2018. JAMA Netw Open 4(4):e218803–e218803. https://doi.org/10.1001/JAMANETWORKOPEN.2021.8803
Law KC, Tucker RP. (2018). Repetitive negative thinking and suicide: a burgeoning literature with need for further exploration - ScienceDirect. Retrieved September 21, 2022, from https://www.sciencedirect.com/science/article/pii/S2352250X17301689
Liu X, Huang Y, Liu Y (2018) Prevalence, distribution, and associated factors of suicide attempts in young adolescents: school-based data from 40 low-income and middle-income countries. PLOS ONE 13(12):e0207823. https://doi.org/10.1371/journal.pone.0207823
Marthoenis M, Yasir Arafat SM (2022) Rate and associated factors of suicidal behavior among adolescents in Bangladesh and Indonesia: global school-based student health survey data analysis. Scientifica 2022(2022):8625345. https://doi.org/10.1155/2022/8625345
McKinnon B, Gariépy G, Sentenac M, Elgar FJ (2016) Adolescent suicidal behaviours in 32 low- and middle-income countries. Bull World Health Organ 94(5):340-350F. https://doi.org/10.2471/blt.15.163295
OECD (2019). Education at a Glance 2019: OECD indicators. Paris, France: OECD Publishing. Retrieved from https://www.oecd-ilibrary.org/sites/c98d92af-en/index.html?itemId=/content/component/c98d92af-en
Omer H, Dolberger DI (2015) Helping parents cope with suicide threats: an approach based on nonviolent resistance. Fam Process 54(3):559–575
Oppong Asante K, Kugbey N, Osafo J, Quarshie ENB, Sarfo JO (2017) The prevalence and correlates of suicidal behaviours (ideation, plan and attempt) among adolescents in senior high schools in Ghana. SSM - Population Health 3(May):427–434. https://doi.org/10.1016/j.ssmph.2017.05.005
Pandey AR, Bista B, Ram Dhungana R, Aryal KK, Chalise B, Dhimal M (2019) Factors associated with suicidal ideation and suicidal attempts among adolescent students in Nepal: Findings from Global School-based Students Health Survey. PLOS ONE 14(4):e0210383. https://doi.org/10.1371/JOURNAL.PONE.0210383
Park C, Majeed A, Gill H, Tamura J, Ho RC, Mansur RB, McIntyre RS (2020) The effect of loneliness on distinct health outcomes: a comprehensive review and meta-analysis. Psychiatr Res 294:113514. https://doi.org/10.1016/J.PSYCHRES.2020.113514
Pengpid S, Peltzer K (2019) Prevalence and correlates of past 12-month suicide attempt among in-school adolescents in Guatemala. Psychol Res Behav Manag 12:523. https://doi.org/10.2147/PRBM.S212648
Pengpid S, Peltzer K (2019) Prevalence of truancy in a national sample of school going adolescents in Laos is associated with potential risk and protective factors. Child Youth Serv Rev 107:104521. https://doi.org/10.1016/J.CHILDYOUTH.2019.104521
Pengpid S, Peltzer K (2020) Suicide attempt and associated factors among adolescents in five southeast Asian countries in 2015. Crisis 41(4):296–303. https://doi.org/10.1027/0227-5910/A000642
Pengpid S, Peltzer K (2021) Past 12-month history of single and multiple suicide attempts among a national sample of school-going adolescents in Tonga. Asia Pac Psychiatry 13(3):e12425. https://doi.org/10.1111/APPY.12425
Pengpid S, Peltzer K (2022) Factors associated with single and multiple suicide attempts in adolescents attending school in Argentina: national cross-sectional survey in 2018. BJPsych Open 8(4):e128. https://doi.org/10.1192/BJO.2022.524
Pompili M, Innamorati M, Girardi P, Tatarelli R, Lester D (2011) Evidence-based interventions for preventing suicide in youths. In: Pompili M, Tatarelli R (eds) evidence based practice in suicidology: A source book. Hogrefe, Gottingen, pp 173–209
Putra IG. N. E., Karin, P. A. E. S., & Ariastuti, N. L. P. (2021). Suicidal ideation and suicide attempt among Indonesian adolescent students. International Journal of Adolescent Medicine and Health, 33(5). https://doi.org/10.1515/IJAMH-2019-0035/MACHINEREADABLECITATION/RIS
Quarshie ENB, Onyeaka HK, Oppong Asante K (2020) Suicidal behaviours among adolescents in Liberia. BMC Psychiatry 20(1):1–12. https://doi.org/10.1186/S12888-020-02985-3/TABLES/3
Sarfo JO, Obeng P, Debrah TP, Gbordzoe NI, Fosu AK (2022) Suicidal behaviours (ideation, plan and attempt) among school-going adolescents: a study of prevalence, predisposing, and protective factors in Saint Vincent and the grenadines. Dialogues in Health 1:100077. https://doi.org/10.1016/J.DIALOG.2022.100077
Seidu AA, Amu H, Dadzie LK, Amoah A, Ahinkorah BO, Ameyaw EK, Kissah-Korsah K (2020) Suicidal behaviours among in-school adolescents in mozambique: cross-sectional evidence of the prevalence and predictors using the global school-based health survey data. PLoS ONE 15:1–13. https://doi.org/10.1371/journal.pone.0236448
Sellers CM, Diaz-Valdes Iriarte A, Wyman Battalen A, O’Brien KHMM (2019) Alcohol and marijuana use as daily predictors of suicide ideation and attempts among adolescents prior to psychiatric hospitalisation. Psychiatry Res 273:672–677. https://doi.org/10.1016/J.PSYCHRES.2019.02.006
Shahedifar N, Shaikh MA, Oporia F, Wilson ML (2020) Global School-based student health survey reveals correlates of suicidal behaviors in Brunei Darussalam: a nationwide cross-sectional study. J Injury Viol Res 12(3 Suppl 1):15. https://doi.org/10.5249/JIVR.V12I3.1371
Shayo FK, Lawala PS (2019) Does bullying predict suicidal behaviors among in-school adolescents? A cross-sectional finding from Tanzania as an example of a low-income country. BMC Psychiatry 19(1):1–6. https://doi.org/10.1186/S12888-019-2402-2/TABLES/3
Silverman MM, Berman AL (2014) Suicide risk assessment and risk formulation part I: A focus on suicide ideation in assessing suicide risk. Suicide Life Threat Behav 44(4):420–431
Smith L, Jackson SE, Vancampfort D, Jacob L, Firth J, Grabovac I, Koyanagi A (2020) Sexual behavior and suicide attempts among adolescents aged 12–15 years from 38 countries: a global perspective. Psychiatry Res 287:112564. https://doi.org/10.1016/J.PSYCHRES.2019.112564
Uddin R, Burton NW, Maple M, Khan SR, Khan A (2019) Suicidal ideation, suicide planning, and suicide attempts among adolescents in 59 low-income and middle-income countries: a population-based study. Lancet Child Adolescent Health 3(4):223–233. https://doi.org/10.1016/S2352-4642(18)30403-6
United Nations Children’s Fund (2017). Situation Analysis of Children in Samoa. Retrieved from https://www.unicef.org/pacificislands/media/1206/file/Situation-Analysis-of-Children-Samoa.pdf
Walsh E, Hooven C, Kronick B (2013) School-wide staff and faculty training in suicide risk awareness: successes and challenges. J Child Adolesc Psychiatr Nurs 26(1):53–61
Whitlock J, Wyman PA, Moore SR (2014) Connectedness and suicide prevention in adolescents: pathways and implications. Suicide Life Threat Behav 44(3):246–272
World Health Organization. (2019). Suicide in the world: Global Health Estimates. Geneva: World Health Organization. Retrieved from https://apps.who.int/iris/bitstream/handle/10665/326948/WHO-MSD-MER-19.3-eng.pdf
Yang T, Guo L, Hong F, Wang Z, Yu Y, Lu C (2020) Association between bullying and suicidal behavior among chinese adolescents: an analysis of gender differences. Psychol Res Behav Manag 13:89. https://doi.org/10.2147/PRBM.S228007
Ziaei R, Viitasara E, Soares J, Sadeghi-Bazarghani H, Dastgiri S, Zeinalzadeh AH, Mohammadi R (2017) Suicidal ideation and its correlates among high school students in Iran: a cross-sectional study. BMC Psychiatry 17(1):1–7. https://doi.org/10.1186/S12888-017-1298-Y/TABLES/2
Acknowledgements
We thank the WHO, CDC, and the Samoan MoH for making the data available. We sincerely thank the Centre for Behaviour and Wellness Advocacy, Ghana, for their expert review and writing support.
Funding
None.
Author information
Authors and Affiliations
Contributions
Conceptualisation: JOS, methodology, data curation, data analysis: JOS and PO; writing—original draft preparation, writing: JOS, NIG, DA, TPD, COBO, and PO; writing—review and editing: all authors; writing—supervision: JOS. All authors read and agreed to the final version of the manuscript for publication.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study received the necessary authorisation from Samoa’s MoH and the Ministry of Education (MoE) Institutional Review Board before the researchers commenced the data collection. The study strictly adhered to the ethical policies set by Samoa’s MoH and MoE. Entry permission protocols were followed to obtain authorisation from the MoH, and the heads of the individual schools included in the study. Informed consent, parental consent, and child assent were obtained from teenagers under the age of 18 using both verbal and written agreements. The data can be accessed at the WHO website: https://extranet.who.int/ncdsmicrodata/index.php/catalog/773/study-description.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sarfo, J.O., Gbordzoe, N.I., Attigah, D. et al. Suicidal behaviours among school-going adolescents in samoa: a secondary analysis of prevalence, protective, and risk factors. Middle East Curr Psychiatry 30, 68 (2023). https://doi.org/10.1186/s43045-023-00343-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-023-00343-z