
Abstract
Background
Despite the high prevalence of communicational differences, anxiety, and sensory processing difficulties in children with autism spectrum disorder (ASD), little is known about the nature of their experiences. Thus, the present study aimed to explore the correlation between communication skills, sensory difficulties, and anxiety in children with ASD. Fifty-three children with ASD (Mage = 8.51, SD = 2.51; males = 42) were recruited. The Persian version of the Short Sensory Profile (SSP), the Children’s Communication Checklist (CCC), and the Spence Children’s Anxiety Scale (SCAS) was used to assess the variables.
Results
The overall sensory score of children with ASD was significantly and positively correlated with most of the communication skills (P < 0.05). The overall sensory score of children with ASD was significantly and negatively correlated with all anxiety subsets of these children (P < 0.05). The social relationships score of children with ASD had a significant and negative correlation with all subsets of anxiety and a significant and positive correlation with all sensory subsets (P < 0.05). The total score of communication was significantly and negatively related to all subsets of anxiety except separation anxiety (P < 0.05).
Conclusions
Sensory processing difficulties in ASD children appear to be significantly associated with communication skills and anxiety acts as a mediator between the two.
Similar content being viewed by others

Background
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by difficulties in social communication as well as restricted and repetitive behaviors, interests, and activities [1]. ASD is one of the most prevalent psychiatric disorders, with an estimated frequency of one in every 68 children [2, 3]. In Iran, the prevalence of ASD is equal to 0.1% (10 per 10 000), with a 2:1 male-to-female ratio. In total, 86% of people with ASD have at least one comorbid condition. Intellectual disability, epilepsy, enuresis, and attention deficit and hyperactivity disorder (ADHD) with prevalence rates of 70.3%, 29.7%, 27%, and 21.62%, respectively, were the most prevalent comorbid conditions in people with ASD [4]. Language comprehension differences, social communication and interaction differences, interactive movements (gestures), nonverbal behaviors, and motor coordination difficulties are all present in ASD [5]. One of the three key areas affected by ASD is communication and language abilities. Many children with ASD are first referred for screening because their parents are concerned about language delays. Furthermore, linguistic milestones (particularly acquiring language abilities by the age of five) are substantially linked to long-term prognosis [6, 7]. However, according to the DSM-5, the ASD category has two basic characteristics: (a) persistent insufficiency in social communication and social interaction observed in various situations and (b) restricted and repetitive behaviors. In addition to these characteristics, it is stressed that specific autistic features appear in early childhood and lead to difficulties in daily life [8]. Language development levels in children with ASD can vary greatly, and while some children do not experience any delays in language development, the pragmatic language does not improve in 25% of cases [9]. Understanding the differences in language development in ASD cases is critical because parents typically perceive failures in language development in children with ASD as a complaint. In addition, the pragmatic of language in the early stages is intimately linked to long term [10]. Atypical patterns of sensory responsiveness (hyporesponsiveness and hyperresponsiveness) are frequent in children with ASD, and they are thought to have cascading effects across other developmental domains [11, 12]. Indeed, sensory response patterns can significantly predict aspects of adaptive behaviors like eating difficulties in ASD children [12, 13].
Sensory processing is the process that organizes sensation from one’s own body and the environment, thus making it possible to use the body effectively in the environment. Hyperresponsiveness is a sensory processing difference involving excessive or unpleasant reactions to sensory inputs [1]. According to Dunn’s approach, hyperresponsiveness represents two types of behavior namely sensitivity to sensations and avoidance of sensations [14]. Sensory difficulties are associated with sleep disorders, poorer levels of social skills and adaptive behaviors, and greater anxiety. In addition, when paired with worry, it predicts an increased degree of gastrointestinal disorders [15, 16]. Previous studies have also indicated that sensory difficulties may have a detrimental influence on children’s psychological well-being. However, little is known about these differences in ASD, indicating that more researches are needed [15]. Sensory difficulties may be linked to problematic behaviors [17]. Few studies have looked at the link between sensory processing impairment, emotion, and behavior differences in children with ASD [18]. For example, Tseng et al. found that in 67 children with ASD aged 48–84 months, sensation avoiding and sensation sensitivity were strongly linked to internalizing and externalizing problematic behaviors [19]. In addition, O’Donnell et al. found that different behaviors such as irritability, lethargy, stereotypic behaviors, hyperactivity/noncompliance, and incorrect speech are more common in preschool children with greater degrees of sensory processing difficulties [20]. Similarly, Dellapiazza et al. [21] found that irritability is linked to avoidance of sensations, whereas hyperactivity/noncompliance is linked to seeking sensations and sensation sensitivity. After adjusting for age and IQ, typical sensory processing also explains a large portion of the variance in different behaviors (from 16 to 39%) [21]. According to the findings, children with ASD who have more sensory processing difficulties are more likely to exhibit different behaviors such as irritability, lethargy, stereotypic behaviors, hyperactivity, and poor speech. Another study showed that in children with ASD, hyporesponsiveness had a significant positive relationship with the severity of socio-communication symptoms [22]. In general, studies have shown that abnormal sensory processing can play an important role in the severity of ASD symptoms as well as in the rate of acquisition of communication skills [11, 22, 23].
Another co-occurring disorder that is linked to both problematic behaviors and sensory difficulties is anxiety. Anxiety disorders are the most commonly diagnosed illnesses in children with ASD, according to a study of concomitant psychiatric features in ASD, with rates of 5–35% generalized anxiety recorded in earlier research [24]. Children with ASD who have more anxiety symptoms also have more sensory difficulties. Differences in sensory responsiveness that are linked to the core and related features of ASD persist in older children and adolescents on the spectrum [11]. There is a significant positive correlation between anxiety and sensory sensitivities in children with ASD [25]. Sensory processing difficulties in ASD children are significantly associated with stereotyped behaviors, and anxiety acts as a mediator between the two [26, 27]. Another study found that anxiety symptoms increased in ASD children, over time while hyperresponsiveness remained constant. Hyperresponsiveness predicts changes in anxiety; however, anxiety cannot predict changes in hyperresponsiveness. In fact, hyperresponsiveness appears earlier than anxiety and predicts the onset of anxiety [28]. Compared to the youth with anxiety and ASD alone, anxiety levels are greater in children and adolescents with ASD who also have a co-occurring behavior difficulty. The youth with ASD exhibits higher levels of anxiety and disruptive behaviors and are more likely to require antipsychotic medication [28, 29]. Although it has been shown that children with ASD may exhibit high rates of anxiety symptoms, a few researches have been done on the correlation between communication skills and anxiety symptoms in children with ASD. Davis et al. showed that both receptive and expressive communication skills play an important role in the development of anxiety symptoms [30]. To date, no research has examined the relationship between anxiety, sensory problems, and all communication skills in children with ASD at the same time.
Given the ample incidences of communication difficulties, anxiety, and sensory difficulties in ASD, further study into the links between communication skills, sensory processing, and anxiety is needed. Changes in the physical and social settings can cause anxiety, which can lead to the onset of maladaptive behaviors in people with ASD. Therefore, this research aims to find out how a child’s communication abilities impact their anxiety level, as well as how the child’s sensory response patterns affect their communication development and anxiety level. Thus, the present study is aimed at exploring the relationships between communication skills, sensory difficulties, and anxiety in children with ASD. The following hypotheses were tested: (1) Sensory characteristics are related to the communication skills of children with ASD. (2) Sensory characteristics are associated with anxiety in children with ASD. (3) Communication skills are associated with anxiety in children with ASD.
Methods
Ethics statement
All procedures in this study were consistent with the guidelines for humans of the National Institute of Health and approved by the Ethical Committee of the Baqiyatallah University of Medical Sciences, Tehran, Iran (IR.BMSU.REC.1399.512).
Participants
Fifty-three children with ASD (42 males/11 females) aged between 6 and 12 years (M = 8.51, SD = 2.51) enrolled in the study. The race of all the participating children was white, and all of them were monolingual Persian speakers and residents of Tehran. All questionnaires were completed by the mothers of these children. The mothers ranged in age from 23 to 45 years (M = 32.7, SD = 5.9). Their education level was as follows: seven had a high school education, 18 had a high school diploma, 20 had a bachelor’s degree, and eight had master’s or doctoral degrees. According to the Diagnostic and Statistical Manual V (DSM-5) criteria, all subjects were diagnosed with ASD by a professional psychiatrist, which was extracted from the participant’s medical records. To confirm this diagnosis, the authors also used the Persian version of the Gilliam Autism Rating Scale-3 (GARS-3) for all participants. All participants in this scale scored above the cutoff point of 54 [31]. The severity of autism was determined based on the DSM-5 categorization. The mild, moderate, and severe ASD are defined as severity level 1, severity level 2, and severity level 3, respectively [32]. All participants of this study had severity level 2 of ASD. Children whose anxiety has not been treated and who have not received any treatment in the past year were included. In addition, participants with visual impairment, hearing loss, epilepsy, and other neurological difficulties such as cerebral palsy were excluded.
Measures
Short Sensory Profile (SSP)
The Short Sensory Profile (SSP) is a shortened version of the Dunn’s Sensory Profile Caregiver Questionnaire [33]. The SSP with 38 items is a standardized assessment instrument for measuring sensory features in children and students in the classroom, school, and preschool settings. The subscales of the SSP are tactile sensitivity, taste/smell sensitivity, movement sensitivity, under-responsive/seeks sensation, auditory filtering, low energy/weak, and visual/auditory sensitivity. In addition to these subscales, four basic patterns of sensory processing are extracted from the SSP. These sub-types are sensation seeking, including the representation of high thresholds and an active self-regulation strategy; sensation avoiding, including low thresholds and an active self-regulation strategy; sensation sensitivity, including low thresholds and a passive self-regulation strategy; and low registration, including representation of high thresholds and a passive self-regulation strategy. This questionnaire can be used for the age range of 3 to 11 years and 11 months. The questionnaire is designed based on Likert’s scale of five points always = 1, often = 2, sometimes = 3, rarely = 4, and never = 5. Cronbach’s alpha for the subscales of the original version of the SSP was reported as 0.74, 0.93, 0.74, 0.74, 0.78, 0.93, and 0.72 [34]. The construct validity of the Persian version of this questionnaire for 384 children and students aged 3 to 12 years was confirmed through confirmatory factor analysis (P < 0.001). In addition, the reliability of the Persian version of the SSP, based on Cronbach’s alpha, for the whole questionnaire was equal to 0.88, and for low registration, sensation seeking, sensation sensitivity, and sensation avoiding were reported as 0.82, 0.88, 0.82, and 0.81 respectively [35]. In this study, the online version of the SSP was used for sampling. Internal reliability of the online version ranges from 0.65 to 0.92 (Cronbach’s alpha for the SSP subscales was 0.71, 0.81, 0.71, 0.70, 0.74, 0.92, and 0.65, respectively). In this study, based on the division of Watson et al. [22], the sum scores of sensory seeking and low registration patterns were considered as the score of hyporesponsiveness, and the sum scores of the patterns of sensation avoiding and sensation sensitivity were considered as the score of hyperresponsiveness. Higher scores indicate normal sensory processing, and lower scores indicate sensory disturbances. The SSP cutoff scores include a score of less than 141 indicating a definite difference and a score between 142 and 154 indicating a possible difference in sensory processing. A score greater than 155 is considered normal performance [36].
The Spence Children’s Anxiety Scale (SCAS)
The Spence Children’s Anxiety Scale (SCAS) is designed to evaluate anxiety in children aged 6 to 12, based on the APA (DSM-IV, 1994) classification system. The scale includes six correlated factors: panic disorder, social phobia, separation anxiety, generalized anxiety, obsessive–compulsive disorder, and fear of physical injury. The scale has 38 questions, and Cronbach’s alpha for the subscales of the original version of the SCAS was reported as 0.82, 0.70, 0.70, 0.60, 0.73, and 0.73, respectively. The construct validity of the Persian version of the SCAS was confirmed using confirmatory factor analysis (P < 0.001). In addition, its reliability based on Cronbach’s alpha for the whole questionnaire was 0.89, and the subscales of the Persian version of the SCAS were reported as 0.82, 0.70, 0.70, 0.60, 0.73, and 0.73, respectively [37]. In this study, the online version of the SCAS was used for sampling. Internal reliability of the online version ranges from 0.55 to 0.83 (Cronbach’s alpha for the SCAS subscales was 0.83, 0.68, 0.66, 0.62, 0.55, and 0.64, respectively.)
Children’s Communication Checklist (CCC)
The Children’s Communication Checklist (CCC) was created to identify the areas of communication disability not effectively assessed by current standardized language assessments [38]. It is normally completed by a parent or other caregiver; however, teachers or other professionals who are familiar with the child might provide helpful information. It takes 5 to 15 min to complete and consists of 70 questions and 9 subscales of (A) speech, (B) syntax, (C) inappropriate initiation, (D) coherence, (E) stereotyped language, (F) use of context, (G) rapport, (H) social relationships, and (I) interests. The Pragmatic Composite Score (PCS) is the sum of the scores of five pragmatic subscales, C to G. Lower scores on this questionnaire indicate more difficulties. Internal reliability for the subscales of the original version of the CCC was reported as 0.86, 0.78, 0.80, 0.86, 0.87, 0.84, 0.87, 0.88, and 0.84, respectively [38]. The checklist has been verified in Iran for children aged 6 to 11 years, with a Cronbach’s coefficient of 0.82 [39]. In this study, the online version of the CCC was used for sampling. Internal reliability of online version ranges from 0.53 to 0.82 (Cronbach’s alpha for the CCC subscales was 0.78, 0.53, 0.77, 0.71, 0.82, 0.57, 0.54, 0.71, and 0.67, respectively).
Procedure
The subjects were selected from three medical centers and two private clinics in Tehran based on the inclusion criteria. First, the examiner (first author) explained the objectives of the present study individually to the parents. To each parent who volunteered, the examiner immediately sent a link to the three questionnaires. While completing these questionnaires, the first author was available to answer any questions from the parents. A written consent was obtained from all participants. All three questionnaires were completed online by parents in the clinic waiting room. Completing all the questionnaires would take about 20 to 25 min. The sampling of this research, which was available as a sample, was done in the winter of 2021. In other words, we only sampled these centers and clinics for 3 months, and during this period, only 53 children met the inclusion criteria.
Data analysis
The data were analyzed using IBM SPSS 16.0 with a two-tailed p = 0.05. Pearson correlation was used to analyze the data to examine the relationship between research variables and research hypotheses.
Results
The mean total score for the SSP was 130.3 (SD = 25.8). Our results showed that 62.3% (n = 33) of the sample scored in the definite difference category and 18.9% (n = 10) in the probable difference category, and 18.9% (n = 10) showed typical performance. The mean total score for the SCAS was 32.9 (SD = 18.4). Also, the mean total score for the CCC was 195.9 (SD = 23.3).
Correlation between the CCC and the SSP
The correlation between sensory characteristics based on short sensory profiles and children’s communication skills based on the CCC in terms of the subsets for children with ASD is shown in Table 1.
Table 1 shows that the overall sensory score of children with ASD is significantly positively correlated with seven out of ten communication subsets (P < 0.05). On the other hand, the total score of communication and the score of pragmatic score in children with ASD have a significant positive relationship with four out of seven subsets of the SSP of these children (P < 0.05). The score of interests in ASD children has a significant positive relationship with five out of seven subsets of the SSP of these children (P < 0.05). Moreover, the score of social relationships of these children had the highest correlation with their overall sensory score (r = 0.62) and had a significant positive relationship with all of the subsets of the SSP (P < 0.05).
Correlation between the SCAS and the SSP
The correlation between sensory characteristics based on the SSP and children’s anxiety based on the SCAS in terms of the subsets for children with ASD is listed in Table 2.
Table 2 shows that the overall sensory score of children with ASD is significantly and negatively correlated with all anxiety subsets of these children (P < 0.05) and has the highest correlation with the overall anxiety score (r = − 0.81). In addition, the score of all SSP subsets except auditory filtering and taste/smell sensitivity in ASD children has a significant and negative relationship with all subsets of anxiety in these children (P < 0.05). Moreover, the overall anxiety score of these children has a significant negative relationship with the score of all subsets of the SSP (P < 0.05). In general, all components of these two questionnaires have a negative relationship with each other, which in most cases, these relationships are significant.
Correlation between the SCAS and the CCC
The correlation between children’s communication skills based on the CCC and children’s anxiety based on the SCAS in terms of subsets for children with ASD is shown in Table 3.
Table 3 indicates that the social relationship score of children with ASD has a significant negative correlation with all subsets of anxiety (P < 0.05) and has the highest correlation with the generalized anxiety disorder score (r = − 0.65). The total score of communication in these children is significantly and negatively related to five out of the six subsets of anxiety (P < 0.05) and has the highest relationship with the score of obsessive–compulsive disorder (r = − 0.56). Interest score has a significant negative correlation with four out of seven subsets of anxiety (P < 0.05) and has the highest correlation with obsessive–compulsive disorder score (r = − 0. 47). On the other hand, the overall anxiety score of these children has a significant negative correlation with six out of ten communication subsets (P < 0.05) and has the most negative correlation with the score of social relationships (r = − 0.60). In general, most of the components of these two questionnaires have a negative relationship with each other, which in some components these relationships are significant.
The correlation between four patterns of sensory processing and subscales of the SCAS and the CCC for children with ASD is shown in Table 4.
Table 4 shows that all patterns of sensory processing of children with ASD are significantly and negatively correlated with all anxiety subsets of these children (P < 0.05). In addition, low registration has a significant positive correlation with all communication skills except speech, syntax, and use of context (P < 0.05). Sensation sensitivity has a significant positive correlation with speech, coherence, social relationships, interests, and PCS (P < 0.05). Sensation avoiding has a significant positive correlation with social relationships and interests (P < 0.05). Sensation Seeking has a significant positive correlation with stereotyped language, use of context, social relationships, interests, and PCS (P < 0.05). Hyporesponsiveness has a significant positive correlation with all communication skills except speech and syntax (P < 0.05). Hyperresponsiveness has a significant positive correlation with only three out of ten subsets of communication skills (P < 0.05).
Discussion
Communicational differences are common in children with ASD; however, the link to sensory processing difficulties and anxiety has not been thoroughly investigated. While researches have revealed some links between communicative skills, sensory difficulties, and anxiety in children with ASD, this is the first study to employ a cross-sectional methodology in Iran. This study contributes to the body of knowledge about children with ASD by looking at the link between these prevalent disorders.
The connection between sensory differences and communication skills
A variety of symptoms, perhaps connected to sensory processing difficulties, are one of the fundamental specific autistic features [1]. The overall sensory score of children with ASD was significantly and positively correlated with most of the communication skills. These findings are in line with Clince et al. [40]. They showed that students with ASD who had higher scores on sensory processing also performed better academically and communicatively [40]. Also, another study showed that ASD children have specific sensory processing patterns, and in these children, there is a significant relationship between sensory processing disorders and communication disorders [41]. The low registration also had a significant positive correlation with most communication skills, which is in line with the results of previous studies [22, 23]. These results show that there is probably a common mechanism underlying communication problems and sensory processing problems in children with autism. In a previous study on ASD children, sensory hyporesponsiveness was associated with poorer communication and social functioning [23]. This is consistent with our results because our results showed that the pattern of sensory hyporesponsiveness had a positive and significant correlation with most of the communication skills (from the CCC), especially the Pragmatic Composite Score (PCS). According to studies, pragmatic problems (from the CCC) are very common in ASD children [42, 43]. In addition, it has recently been proven that the CCC can be used in screening ASD [44, 45]. Therefore, according to our results (Table 4), it can be concluded that the pattern of sensory hyporesponsiveness is more common among ASD children than other patterns. This is in line with the claim by Feldman et al. which reported that hyporesponsiveness is the most common and specific to ASD [11].
Our findings are consistent with the findings of another study that looked at caregiver-reported data of people with ASD and discovered that stereotyped language was linked to sensory processing difficulties [46]. Our findings were similar to Tseng et al. who indicated that there was a link between sensation sensitivity and stereotyped language, as well as sensation avoiding and externalizing activities [19]. Moreover, social relationships had a significant positive correlation with all patterns of sensory processing, which indicated the importance of sensory processing patterns in determining socio-communication skills. Therefore, it can be interpreted that sensory processing patterns play an important role in determining the severity of ASD symptoms, which confirms the results of previous studies [11, 22, 23]. In addition, interests had a significant positive correlation with all patterns of sensory processing, which is consistent with previous research describing the importance of the co-occurrence of sensory processing patterns and different interests in the ASD population [47]. Therefore, it can be concluded that in evaluating and treating the sensory processing pattern of children with autism in the clinical context, attention to social relationships and interests of these children should be a priority for the examiner.
The connection between sensory differences and anxiety
Many studies have been conducted on the relationship between sensory differences and anxiety in children with autism and the co-occurrence of the two [26,27,28, 48, 49]. The results of this study showed that all patterns of sensory processing, as well as most of the sensory subscales of the SSP, had a significant negative correlation with all subsets of anxiety, which is consistent with the results of other studies about the importance of co-occurrence of the sensory processing patterns and types of anxiety in the ASD population. Green et al. showed that sensory processing patterns cause anxiety in these children [28]. Therefore, in assessing and treating anxiety in children with ASD, it is best to first identify and modify the sensory processing pattern of these children.
Individuals with sensory processing impairments showed greater levels of anxiety, which was consistent with our assumptions. In line with other researches [3, 16], this study found that the overall sensory score of children with ASD was significantly and negatively correlated with all anxiety subsets of these children and had the highest correlation with the overall anxiety. This shows that children with ASD who have greater levels of anxiety are more likely to exaggerate their responses to sensory stimuli. Children with ASD who have higher levels of anxiety exhibit more and more different behaviors, such as internalizing, externalizing, and asocial behaviors. Demonstration of different behaviors in the situation of anxiety in ASD has received little attention. Nonetheless, the evidences suggest that clinicians should pay attention to their clients’ comorbid anxiety symptoms, which may be linked to their different behaviors. Further study is needed to confirm this link.
The connection between anxiety and communication skills
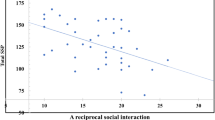
The results indicated that the social relationship score of children with ASD had a significant negative correlation with all subsets of anxiety. That is, by reducing anxiety, even children with ASD establish better social relationships and, on the other hand, by establishing friendly relationships, and increasing these relationships, we can help reduce the anxiety of these children. This is in line with the results of the previous study [50].
According to Green et al. anxiety arises from sensory processing patterns [28]. Therefore, if a child has a sensation avoiding pattern, he/she most likely refuses to participate in daily activities. On the other hand, hyperresponsiveness can prevent ASD children from participating in daily activities. Therefore, it can be interpreted that hyperresponsiveness can negatively affect speech and language learning and communication in general. This is consistent with other studies [26, 51].
Communication skills have different effects on anxiety levels. In some people with ASD, anxiety decreases with an increase in communication deficits, and in some of these children, anxiety increases with increasing communication deficits [50]. Kring et al. suggested that ASD adolescents and adults with co-morbid psychiatric disorders (such as anxiety disorder) are more prone to engage in asocial activities [52]. There may be long-term negative implications of sensory hyporesponsiveness on adaptive outcomes. Children with hyporesponsiveness demonstrate diminished responses to specific sensory input in their environments, including adult and peer attempts for social engagement. Thus, children with high levels of hyporesponsiveness early in life may be especially vulnerable to cascading effects on development over time, perhaps due to reduced opportunities to engage meaningfully and learn from their physical environments and social experiences. Thereby, they fall increasingly further behind their peers [12]. However, to properly address these concerns, more long-term research with larger representative populations is required.
The study looked at the bivariate connections between the three variables of interest. It is crucial to think about how communicational differences affect children with ASD, who also struggle to regulate their responses to sensory inputs and emotions. The findings of this study shed light on the links between sensory processing difficulties, communicational differences, and anxiety in children with ASD. The lack of techniques for dealing with sensory processing difficulties may have an impact on their mental well-being and lead to more severe communicational differences. These three conditions, on the other hand, may have a reciprocal and complicated interaction that requires further research.
There were several limitations to this study. One of the limitations was that children under anxiety treatment were excluded from the study, so the results cannot be generalized to children with anxiety. Second, our participants were volunteers who had access to support resources or service systems; thus, they may not be representative of the overall community of children with ASD. The cross-sectional design was also a limitation. Despite our preliminary results about the links between sensory processing, anxiety, and communicational differences in children with ASD, it is difficult to pinpoint the causative relationship between these factors. To reach more solid results, future research should use alternative forms of sampling and larger sample size. Also, including healthy controls in the study would be of value to know the magnitude of the problem of sensory processing difficulties in ASD and whether sensory processing difficulties in normal children can affect their anxiety level and communication as well.
Conclusions
The study was the first to examine the relationships among communicational differences, sensory processing difficulties, and anxiety in children with ASD. These findings suggest that children with ASD who have communication challenges may also have trouble controlling their sensory input; sensory processing deficits were linked to anxiety in these children. Sensory processing difficulties were indirectly linked to greater communicational differences through elevated levels of anxiety. Sensory processing difficulties in ASD children appear to be significantly associated with communication skills, and anxiety acts as a mediator between the two. Given the specific autistic features, a complete intervention for modifying sensory input modulation, emotional control, and communicational differences may be necessary. Future studies might focus on elucidating the underlying processes and developing an integrated therapy for these three disorders.
Availability of data and materials
Not applicable.
References
Syu YC, Huang PC, Wang TY et al (2020) Relationship among sensory over-responsivity, problem behaviors, and anxiety in emerging adults with autism spectrum disorder. Neuropsychiatr Dis Treat 16:2181–2190
Aghaz A, Salehi F, Taaki F et al (2018) Pattern of phonological awareness skills in children with autism spectrum disorders. Koomesh 20(3):453–457
Dellapiazza F, Vernhet C, Blanc N et al (2018) Links between sensory processing, adaptive behaviours, and attention in children with autism spectrum disorder: a systematic review. Psychiatry Res 270:78–88
Mohammadi MR, Ahmadi N, KhaleghiA, et al. (2019). Prevalence of autism and its comorbidities and the relationship with maternal psychopathology: a national population-based study. Arch Iran Med 22(10)
O’Hearn K, Franconeri S, Wright C et al (2013) The development of individuation in autism. J Exp Psychol Hum Percept Perform 39(2):494–509
DiStefano C, Shih W, Kaiser A et al (2016) Communication growth in minimally verbal children with ASD: the importance of interaction. Autism Res 9(10):1093–1102
Eigsti IM, de Marchena AB, Schuh JM, Kelley E (2011) Language acquisition in autism spectrum disorders: a developmental review. Res Autism Spectr Disord 5(2):681–691
Özyurt G, Eliküçük ÇD (2018) Comparison of language features, autism spectrum symptoms in children diagnosed with autism spectrum disorder, developmental language delay, and healthy controls. Noro psikiyatri arsivi 55(3):205–210
Klinger L, Dawson G, Renner P. (2003). Child psychopathology (pp. pp. 409–454): The Guilford Press New York
Tager-Flusberg H, Paul R, Lord C, et al. (2005). Handbook of autism and pervasive developmental disorders 1:335-364
Feldman JI, Cassidy M, Liu Y et al (2020) Relations between sensory responsiveness and features of autism in children. Brain Sci 10(11):775
Williams KL, Kirby AV, Watson LR et al (2018) Sensory features as predictors of adaptive behaviors: a comparative longitudinal study of children with autism spectrum disorder and other developmental disabilities. Res Development Dis 81:103–112
Shahriyari A, Aghaz A (2020) Prediction of eating problems in children with autism based on resilience and interactive style of mothers. J Res Behavl Sci 18(3):382–392
Dunn W (1997) The impact of sensory processing abilities on the daily lives of young children and their families: a conceptual model. Infan Young children 9:23–35
Ben-Sasson A, Hen L, Fluss R et al (2009) A meta-analysis of sensory modulation symptoms in individuals with autism spectrum disorders. J Autism Devel Dis 39(1):1–11
Mazurek MO, Vasa RA, Kalb LG et al (2013) Anxiety, sensory over-responsivity, and gastrointestinal problems in children with autism spectrum disorders. J Abnorm Child Psychol 41(1):165–176
Nieto C, Lopez B, Gandia H (2017) Relationships between atypical sensory processing patterns, maladaptive behaviour and maternal stress in Spanish children with autism spectrum disorder. J Intellect Disabil Res 61(12):1140–1150
Robertson AE, Simmons DR (2015) The sensory experiences of adults with autism spectrum disorder: a qualitative analysis. Perception 44(5):569–586
Tseng MH, Fu CP, Cermak SA et al (2011) Emotional and behavioral problems in preschool children with autism: relationship with sensory processing dysfunction. Res Autism Spectr Disord 5(4):1441–1450
O’Donnell S, Deitz J, Kartin D et al (2012) Sensory processing, problem behavior, adaptive behavior, and cognition in preschool children with autism spectrum disorders. Am J Occup Ther 66(5):586–594
Dellapiazza F, Michelon C, Oreve MJ et al (2020) The impact of atypical sensory processing on adaptive functioning and maladaptive behaviors in autism spectrum disorder during childhood: results from the ELENA cohort. J Autism Dev Disord 50(6):2142–2152
Watson LR, Patten E, Baranek GT et al (2011) Differential associations between sensory response patterns and language, social, and communication measures in children with autism or other developmental disabilities. J Speech Lang Hear Res 54(6):1562–1576
Lane AE, Young RL, Baker AE, Angley MT (2010) Sensory processing subtypes in autism: association with adaptive behavior. J Autism Dev Disord 40(1):112–122
Skokauskas N, Gallagher L (2010) Psychosis, affective disorders and anxiety in autistic spectrum disorder: prevalence and nosological considerations. Psychopathol 43(1):8–16
Pfeiffer B, Kinnealey M, Reed C, Herzberg G (2005) Sensory modulation and affective disorders in children and adolescents with Asperger’s disorder. Am J Occup Therapy 59(3):335–345
Lane SJ, Reynolds S, Dumenci L (2012) Sensory overresponsivity and anxiety in typically developing children and children with autism and attention deficit hyperactivity disorder: cause or coexistence? Am J Occup Therapy 66(5):595–603
Lidstone J, Uljarević M, Sullivan J et al (2014) Relations among restricted and repetitive behaviors, anxiety and sensory features in children with autism spectrum disorders. Res Autism Spect Dis 8(2):82–92
Green SA, Ben-Sasson A, Soto TW, Carter AS (2012) Anxiety and sensory over-responsivity in toddlers with autism spectrum disorders: bidirectional effects across time. J Autism Developmen Disord 42(6):112–1119
Kennett J (2002) Autism, empathy and moral agency. Philosophical Quarterly 52(208):340–357
Davis TE, Moree BN, Dempsey T et al (2012) The effect of communication deficits on anxiety symptoms in infants and toddlers with autism spectrum disorders. Behav Ther 43(1):142–152
Gorji R, Hassanzadeh S, Ghasemzadeh S, Lavasani MG (2021) Sensitivity, specificity, and accuracy of the Persian version of 3rd edition of the Gilliam Autism Rating Scale (GARS-3): a descriptive study. J Rafsanjan Univ Med Sci. 20(9):1002–1989
Swartz JS, Amos KE, Brindas M et al (2017) Benefits of an individualized perioperative plan for children with autism spectrum disorder. Pediatr Anesth 27(8):856–862
McIntosh DN, Miller LJ, Shyu V, Dunn W (1999) Development and validation of the short sensory profile. Sensory Profile Manual 61:59–73
Williams ZJ, Failla MD, Gotham KO et al (2018) Psychometric evaluation of the short sensory profile in youth with autism spectrum disorder. J Autism Development Dis 48(12):4231–4249
Movallali G, Nesayan A, Asadi GR (2017) Psychometric properties of short sensory profile School Companion. Arc Rehab 18(3):194–201
Leader G, Tuohy E, Chen JL, Mannion A, Gilroy SP (2020) Feeding problems, gastrointestinal symptoms, challenging behavior and sensory issues in children and adolescents with autism spectrum disorder. J Autism Dev Disord 50(4):1401–1410
Mousavi R, Moradi AR, Farzad V et al (2007) Psychometric properties of the Spence children’s anxiety scale with an Iranian sample. Int J Psycho 1(1):17–26
Bishop DV (1998) Development of the Children’s Communication Checklist (CCC): a method for assessing qualitative aspects of communicative impairment in children. J Child Psychol Psychiatry Allied Discip. 39(6):879–891
Kazemi Y, Afsharian E, Mirzaei B et al (2007) Children’s communication checklist: the study of Persian children. Iran J Res Rehab Sci 2(3):1–5
Clince M, Connolly L, Nolan C (2016) Comparing and exploring the sensory processing patterns of higher education students with attention deficit hyperactivity disorder and autism spectrum disorder. Am J Occup Ther 70(2):1–9
Baker AE, Lane A, Angley MT, Young RL (2008) The relationship between sensory processing patterns and behavioural responsiveness in autistic disorder: a pilot study. J Autism Dev Disord 38(5):867–875
Bishop DV, Baird G (2001) Parent and teacher report of pragmatic aspects of communication: use of the Children’s Communication Checklist in a clinical setting. Dev Med Child Neurol 43(12):809–818
Pritzker E. (2020). Pragmatic language and behavioral and emotional functioning-a systematic review: implications for research and interprofessional practice. James Madison University
Deckers A, Muris P, Roelofs J (2020) Screening for autism spectrum disorder with the achenbach system of empirically based assessment scales. J Psychopathol Behav Assess 42(1):25–37
Aghaz A, Kazemi Y, Karbasi-Amel A, Nakhshab M (2022) Diagnostic accuracy of the Children’s Communication Checklist-Persian in identifying children with autism spectrum disorder. Int J Pediatr 10(2):15482–15494
Boyd BA, McBee M, Holtzclaw T et al (2009) Relationships among repetitive behaviors, sensory features, and executive functions in high functioning autism. Res Autism Spectrum Dis 3(4):959–966
Gabriels RL, Agnew JA, Miller LJ et al (2008) Is there a relationship between restricted, repetitive, stereotyped behaviors and interests and abnormal sensory response in children with autism spectrum disorders? Res Autism Spectrum Dis 2(4):660–670
Moore HL, Brice S, Powell L, et al. (2021). The mediating effects of alexithymia, intolerance of uncertainty, and anxiety on the relationship between sensory processing differences and restricted and repetitive behaviours in autistic adults. J Autism Dev Disord 1–13.
Wigham S, Rodgers J, South M et al (2015) The interplay between sensory processing abnormalities, intolerance of uncertainty, anxiety and restricted and repetitive behaviours in autism spectrum disorder. J Autism Dev Disord 45(4):943–952
Davis TE, Moree BN, Dempsey T et al (2011) The relationship between autism spectrum disorders and anxiety: the moderating effect of communication. Res Autism Spectrum Disord 5(1):324–329
Miller LJ, Anzalone ME, Lane SJ et al (2007) Concept evolution in sensory integration: a proposed nosology for diagnosis. Ame J Occupational Ther 61(2):135–140
Kring SR, Greenberg JS, Seltzer MM (2008) Adolescents and adults with autism with and without co-morbid psychiatric disorders: differences in maternal well-being. J Ment Health Res Intellect Disabil 1(2):53–74
Acknowledgements
The study was supported by the Neuroscience Sciences Research Center, Baqiyatallah University of Medical Sciences, Tehran, Iran.
Funding
None.
Author information
Authors and Affiliations
Contributions
HK conceived and designed the analysis, results representation, and discussion. AA, AM, and HD contributed to the data collection. GHM was involved in the supervision of the work and design, aided in the result interpretation, and contributed to the manuscript writing. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All procedures in this study were consistent with the guidelines for humans of the National Institute of Health and approved by the Ethical Committee of the Baqiyatallah University of Medical Sciences, Tehran, Iran (IR.BMSU.REC.1399.512).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Khaledi, H., Aghaz, A., Mohammadi, A. et al. The relationship between communication skills, sensory difficulties, and anxiety in children with autism spectrum disorder. Middle East Curr Psychiatry 29, 69 (2022). https://doi.org/10.1186/s43045-022-00236-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-022-00236-7