
Abstract
Background
Repetitive transcranial magnetic stimulation showed some evidence for improving symptoms of ADHD along with its relative safety, thus could serve as a treatment strategy or an alternative to stimulant medication. Accordingly, 60 children with ADHD were assessed, and 30 participants were allocated to the rTMS group and received 15 sessions of rTMS over the right dorsolateral prefrontal cortex combined with Atomoxetine 1.2 mg/kg/day. The other 30 participants were allocated to the Sham group and received 15 sessions of sham rTMS and atomoxetine 1.2 mg/kg/day. Clinical assessments of ADHD symptoms and severity were done and compared at 3 points, before treatment, after receiving 15 sessions of rTMS and follow-up 1 month after the last rTMS session, using Conner’s Parent Rating Scale-Revised-Long form, Children’s Global Assessment Scale, and Clinical Global Impression.
Results
The two groups show significant improvement in the T scores of all CPRS subscales, CGI and CGAS. However, the rTMS group had a significantly more improvement than the sham group in inattention, total ADHD severity, CGI, and CGAS after rTMS and continued to the follow-up after 1 month.
Conclusions
rTMS is an efficacious intervention for treating ADHD, and combined rTMS and atomoxetine is superior to atomoxetine alone in improving attention deficit symptoms and total ADHD symptoms severity.
Trial registration
PACTR, PACTR202110558451583. Registered 25 June 2021. Approved 29 October 2021- Retrospectively registered, https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=15968.
Similar content being viewed by others


Background
Attention-deficit hyperactivity disorder (ADHD) is a common neurodevelopmental disorder presented by inattention and/or hyperactivity/impulsivity causing impairment in the child’s academic performance and social functioning [1]. The worldwide ADHD prevalence is estimated to be 7.1% in children and adolescents and 7.2% in the USA [2]; however, the incidence is much higher, reaching 9.4–21.8% in Egypt [3]. Most children with ADHD will have attention problems in adulthood, and many have comorbidities and occupational and social difficulties [2].
Studies of MRI in ADHD have found evidence of brain structural abnormalities in the form of reduction in the gray matter, reduction in cortical thickness and the surface area in the frontal, parietal and temporal areas, and reduction in the basal ganglia and insula as well [4]. These areas are interconnected by functional neurocircuits that regulate attention, thoughts, emotions, and behavior [5]. In addition, fronto-striatal, fronto-cerebellar, and interhemispheric white matter tracts are proven to be affected [6], and dysregulation of these circuits is considered the underlying cause of symptoms of inattention and hyperactivity. The fronto-striatal circuit is known to mediate executive cognitive functions, and its dysregulation causes deficits in sustained attention, organization, planning, working memory, and motor response inhibition. Moreover, dysregulation of the fronto-limbic circuits is associated with symptoms of hyperactivity-impulsivity, delay aversion, aggression, demotivation, and emotional dysregulation. The fronto-cerebellar circuits are associated with motor coordination deficits and problems with the timing and timeliness of behavior [7]. Noteworthy that whole-brain voxel-based morphometry (VBM) and functional MRI (fMRI) studies found evidence of right dorsolateral prefrontal cortex (DLPFC) hypoactivity in ADHD during inhibitory control and attentional tasks [8, 9].
Even while considering psychostimulants as the first-line treatment for ADHD and their adverse effects are typically non-serious and can be transient, they are controversial due to their potential of abuse and that only 50% can tolerate them sufficiently, also their adverse effects, on sleep, nausea/vomiting, abdominal pain, appetite, irritability, headaches, labile mood, and growth suppression [10]. Moreover, a long-term efficacy has not been proven by research [11], and alternative treatments, like behavioral therapies, cognitive training, or dietary interventions, have shown limited efficacy [12].
Repetitive transcranial magnetic stimulation (rTMS) can modulate cortical excitability and brain network activity. TMS can be used diagnostically to study cortical neurophysiology, and the daily use of repetitive TMS can induce long-lasting changes [13]. Accordingly, they are promising therapeutic tool as it can stimulate brain dysregulated neurocircuits that have been implicated in ADHD [6]. Furthermore, they are relatively safe [14], with minimal side effects, cheaper than long-term drug treatments and can induce neuroplasticity [15].
Only a few studies have investigated the role of rTMS on children with ADHD, most of the studies were applied on relatively small samples, used few rTMS sessions, and some studies did not include a sham condition [16]. Most TMS study’s findings also concluded that increasing the excitability of the right DLPFC through high-frequency rTMS can improve ADHD symptoms [17].
Given the high prevalence of ADHD in school-aged children in Egypt, and the absence of sufficient studies on the effect of the combined rTMS and atomoxetine in the treatment of children with ADHD [16], further Sham controlled randomized clinical trials (RCT), applying more numbers of rTMS sessions in a larger sample size in children with ADHD are needed.
Accordingly, the current study is conducted to assess the therapeutic role of rTMS combined with Atomoxetine in children with ADHD and further to assess whether the combined therapy is superior to Atomoxetine alone in treating children with ADHD.
Methods
This study is a double-blind, randomized sham controlled clinical trial and was conducted at the Institute of Psychiatry Ain Shams University, between August 2019 and August 2021, on 60 children with ADHD with ages ranging from 6 to 12 years. The trial protocol was approved by the Research Ethics Committee (REC) at the Ain Shams University Faculty of Medicine (FMASU REC FWA00017585) retrospectively registered, https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=15968.
The sample size was calculated by a statistician using Epi info, setting the type-1 error (α) at 0.05 and power at 80%. Results from a previous study [18], the initial mean was 30 ± 6.86 and dropped to 21 after 10 sessions of rTMS at 10 Hz. Accordingly, the sample size was calculated to be 18 subjects. Gómez et al. [19] showed that the mean of symptoms checklist (SCL) for ADHD from DSM-IV was 18.1 ± 11.63 after a daily session of rTMS, for 5 consecutive days, making a total of 5 rTMS sessions, compared to the initial mean 32.4 ± 14.89. Calculations according to these values produced a sample size of 28 subjects, divided into 14 per group. The number was rounded up to include 30 subjects per group for a total number of 60 subjects.
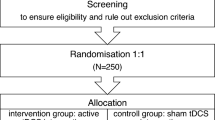
As shown in Fig. 1, a flow diagram showing how the study sample was recruited and handled during the study. Sixty children with ADHD of both sexes and ages ranging between 6 and 12 years old were included in the study. Children with a comorbid diagnosis of autism spectrum disorder, bipolar disorder, obsessive-compulsive disorder, conduct disorder, Tourette disorder or other tic disorders, schizophrenia, schizoaffective disorder, any other psychotic disorder, or other neurological disorders were excluded from the study. Furthermore, participants who have specific contraindications to magnetic stimulation such as any metallic object implanted in the skull (with the exception of oral dental devices), an implanted medication pump or cochlear implant, implanted intra-cardiac lines or pacemaker, also factors that might increase the risk of seizure with TMS such as a history of a seizure disorder, febrile seizures during childhood, known brain lesions, or a history of major head trauma involving loss of consciousness for more than 5 min were excluded from the study.

A flow diagram showing how the study sample was recruited and handled during the study. Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Ann Int Med 2010;152. Epub 24 March [20]
Randomization was conducted and ensured via a computer-based random generation. The sets were generated by the principal investigator. Participants were allocated to the study arms, and they were not aware of which type of rTMS they are going to take, also the outcome assessors were blinded to the allocation of the participants to the study groups and to the type of rTMS used, as allocation of the participants was done without the knowledge of the outcome assessors.
The official sheet of the Okasha Institute of Psychiatry was used for the assessment and interview. This included demographic data, personal and family history, medical history, and mental state examination. All subjects were then assessed using the Structured Clinical Interview for DSM-IV (SCID I) diagnostic tool to diagnose ADHD and to exclude other Axis I diagnoses according to DSM IV classification, which took place in the first interview with the participants before the start of the study. An informed written consent was offered for the parents of the patients participating in the study. The consent contained the name of the study and its aim. It included a detailed description of the procedure, the expected benefits, and the side effects that may result from it. While keeping participants’ identity anonymously, they agreed to use their data for scientific publication. They were informed about their right to withdraw from the study at any time without revealing the reason.
All participants were drug naïve for stimulants and non-stimulants, and all other medications were stopped 2 weeks before the beginning of the study. Atomoxetine was started at 0.5mg/kg/day and was titrated to 1.2 mg/kg/day after 3 days. Thirty participants were allocated to the rTMS group who received 15 sessions of rTMS over the right DLPC, in conjunction with Atomoxetine 1.2 mg/kg/day. The other 30 participants were allocated to the Sham control group who received 15 sessions of sham rTMS and atomoxetine 1.2 mg/kg/day. All participants underwent assessments of the severity of ADHD symptoms done at 3 points, before the beginning of treatment (pre), after receiving 15 sessions of rTMS/Sham rTMS (post), and on follow-up 1 month after treatment (FU), using the Arabic version of revised-conner’s parent rating scale long version, Children’s Global Assessment Scale and Clinical Global Impression. The scores pre, post, and follow-up were compared to evaluate the improvement of clinical symptoms, and the therapeutic effects among the 2 groups were also compared. The primary outcome is defined as an improvement in the severity of ADHD in the rTMS group more than sham group post rTMS. The secondary outcome is defined as the improvement of the severity of ADHD in the rTMS group more than the sham group on follow-up 1 month after that rTMS session.
Magventure R 30 stimulator was used for rTMS. The used coil was a 75-mm figure-eight coil and the stimulation is administered at 10 Hz directed to the right dorsolateral prefrontal cortex, located at the F4 location from the EEG 10-20 system. The pulse intensity was set at 90% of the observed motor threshold, 4 s on-train, 26 s off inter-train interval with 2000 pulses per session for 5 sessions per week, for 15 sessions total (i.e., 30,000 pulses total in treatment course) in the active TMS condition. For the sham rTMS, the coil was tilted over the right dorsolateral pre-frontal cortex without touching the scalp. Participants who received less than 75% of the number of sessions (12 sessions) were considered dropouts.
Clinical assessments
Clinical assessments and follow-ups were done in the outpatient clinics of Okasha Institute of Psychiatry Ain Shams University. In every clinical assessment, parents of the subjects completed the Arabic version of the Conners’ Parent Rating Scale – Revised Long form (CPRS-R-L), Children’s Global Assessment Scale and Clinical Global Impression
Arabic version Conners’ Parent Rating Scale – Revised Long Form
CPRS-R The Long Form contains 80 items and was conducted by parents and is reliable for use with children and adolescents. The form is made of a four-point scale where the parents’ rate how often the child engages in the behaviors from 0 (Never) to 3 Very Often. It can be used to calculate seven subscales, an ADHD Index, three Conners’ Global Indices (CGI), and three DSM-IV Symptom Indices [21, 22].
Children’s Global Assessment Scale (CGAS)
It is a unidimensional assessment of social and psychiatric functioning for children aged 4–16. The CGAS’s score ranges from 1 to 100, with 10-point intervals, that include descriptors of functioning and psychopathology for each interval. The single numerical score representing the severity of disturbance ranges from 1 (most impaired) to 100 (healthiest) [23].
Clinical Global Impression CGI
Clinical Global Impression Scale is designed to assess the effectiveness of a particular treatment: CGI-S assessing Illness Severity and CGI-C assessing Global Improvement or Change. Efficacy Index or Therapeutic Response. CGI—Severity scale (CGI-S): measures illness severity at baseline and after treatment on a scale of seven points. CGI—Improvement scale (CGI-I): measures the improvement in the patient’s condition on treatment from a specific point in time on a scale of 7-point ranging from 1 (very much improved) to 7 (very much worse) [24].
Statistical analysis
The statistical package for Social Science (SPSS 25) was used to review, code, and arrange the data, as well as introduce it to a PC. Data was presented and suitable analysis was done according to the type of data obtained for each parameter. Mixed design ANOVA test was used to assess the statistical significance of the difference between the two-study group means at different times. Mean, standard deviation (± SD), and range for parametric numerical data as the studied groups were normally distributed and were justified after assessment of normality using the Kolmogorov-Smirnov test, while the median and interquartile range (IQR) for non-parametric numerical data. Frequency and percentage of non-numerical data. Student’s T test was used to assess the statistical significance of the difference between the two study group means. Pairwise comparisons were used for comparisons of all possible pairs of group means. Chi-square test was used to examine the relationship between two qualitative variables. P-value: level of significance, P>0.05: nonsignificant (NS) and P< 0.05: significant (S).
Results
Participant characteristics
Table 1 illustrates participant characteristics enrolled in the study. Insignificant differences were found between the characteristics of both study groups on all parameters.
Baseline clinical assessment
Table 2 shows the baseline ADHD symptoms severity in the 2 groups measured using CPRS-R-L, CGAS, and CGI, which revealed the presence of significant problems but with no significant difference between the 2 groups.
Comparative results
Comparison of the reduction in severity in ADHD symptoms and improvement before and after treatment and between the 2 groups by using mixed-design ANOVA tests, revealed that both groups (rTMS combined with atomoxetine and Sham rTMS combined with atomoxetine) had a significantly improved ADHD symptoms from baseline to post rTMS/sham and on follow-up. There was a significant main effect of time on CGI-S, CGI-I, and CGAS as well as on all CPRS sub scores, Oppositional, Cognitive, Hyperactive, Anxious Shy, Psychosomatic, and Social Problems, perfectionism as well as the three Conners’ Global Indices (CGI) and three DSM-IV Symptom Indices.
Regarding CPRS-R:L, the rTMS group showed statistically significant improvement more than the Sham rTMS group in attention deficit symptoms, measured by cognitive subscale, DSM IV inattentive, conner ADHD Index subscales, and total ADHD symptoms severity, measured by ADHD IV Total and Conner’s Global Index, Post rTMS, and on follow-up after 1 month.
Table 3 and Fig. 2 show a statistically significant lower DSM IV inattentive T scores in the rTMS group than in the Sham group, post rTMS, and on follow-up. There is a significant main effect of time on DSM IV TR inattentive score, F = 550.73, P<0.001, a significant main effect of group on DSM IV TR inattentive score, F = 5.72, P<0.001.02 and a significant interaction between time and group as regards their effect on DSM IV TR inattentive score, F = 62.2, P<0.001.

Comparing mean DSM IV inattentive T score between the 2 groups at different times
Table 4 and Fig. 3 show a statistically significant lower DSM IV total T score in the rTMS group than in the Sham group, post rTMS, and on follow-up. It shows the significant main effect of time on DSM IV TR total score, F = 1366.4, P<0.001, the significant main effect of group on DSM IV TR total score, F = 4.86, P<0.001.031, and a significant interaction between time and group as regards their effect on DSM IV TR total score, F = 155.19, P<0.001.

Comparing mean total DSM IV T score between the 2 groups at different times
Table 5 and Fig. 4 show a statistically significant more improvement in the rTMS group than sham post rTMS, but an insignificant difference between the 2 groups on follow-up after 1 month. There is a significant main effect of time on DSM IV TR hyperactive-impulsive score (F = 515.38, P<0.001), a non-significant main effect of group on DSM IV TR hyperactive-impulsive score (F = 3.11, P<0.001.083) and a significant interaction between time and group as regards their effect on DSM IV TR hyperactive impulsive score (F = 46.62, P<0.001).

Comparing mean DSM IV hyperactive impulsive T score between the 2 groups at different times
Regarding the social problem T score, it showed a similar outcome, there was a significant main effect of time on social problems score (F = 303.14, P<0.001), a non-significant main effect of group on social problems score (F = 1.22, P<0.001.275), but there is a significant interaction between time and group as regards their effect on social problems score (F = 32.61, P<0.001).
On the other hand, our results revealed that there is no statistically significant difference between rTMS combined with Atomoxetine and Sham rTMS combined with atomoxetine in oppositional, perfectionism, Anxious Shy, and psychosomatic symptoms.
Table 6 and Fig. 5 represent a statistically significant more improvement in the mean CGAS score in the rTMS group than in the Sham group, post rTMS, and on follow-up. The significant main effect of time on CGAS score was (F = 381.79, P<0.001), the significant main effect of group was (F = 14.45, P<0.001), and the significant interaction between time and group was (F = 41.34, P<0.001).

Comparing mean Children Global Assessment score between the 2 groups at different times
Regarding CGI-Severity score, there is a significant main effect of time on CGI-S (F = 744.32, P = <0.001), a significant main effect of group on CGIS (F = 10.71, P = 0.002), and a significant interaction between time and group as regards their effect on CGI-S (F = 76.91, P = <0.001). There is a statistically significant lower severity score in the rTMS group than the sham group after treatment and on follow-up. Moreover, the rTMS group had a statistically significant more improvement in CGI improv than the sham group, post rTMS, and on follow-up. It showed a significant main effect of time on CGII (F = 12.72, P = 0.001) and group (F = 39.45, P=<0.001) and showed a significant interaction between time and group as regards their effect on CGII (F = 41.21, P = <0.001).
After comparing the 2 studied groups, the effect size post rTMS was P=<0.001, η2 = 0.436 with a power of 1.0; however, this effect size is reduced on follow-up 1 month after last rTMS session to be P=0.021, η2 = 0.088 and power 0.65.
Discussion
The present study revealed that 5 daily sessions/week for 3 weeks of high frequency rTMS over the right DLPFC combined with Atomoxetine is an effective treatment strategy for children with ADHD. Moreover, rTMS combined with atomoxetine is more effective than Atomoxetine alone in improving cognitive symptoms (inattention), total ADHD symptoms severity, and improving the global functioning of children with ADHD.
To date, there are only six studies on the therapeutic effect of rTMS on ADHD that were carried out. Four of the six studies were undertaken on adults and adolescents with ADHD, and only 2 studies were conducted on children [16].
Results of this work are consistent with findings of a study conducted on randomized 60 children with ADHD into either 30 daily 25-min sessions of 10Hz rTMS over right DLPFC, Atomoxetine (1.2mg/kg), or combined treatment over 6 weeks and results showed that rTMS, ATX, or rTMS combined with ATX can effectively alleviate attention deficit, hyperactivity impulse, and oppositional defiance in ADHD children and the combined therapy showed significant advantages in attention deficit and hyperactivity impulse [25].
Cao et al. [17] conducted another study and applied rTMS in children with ADHD to measure the changes in serum miRNA-let-7 level, after being treated by rTMS or atomoxetine, which validated the results of this work. A stimulation protocol similar to our work, but with a higher total number of sessions, was used. Instead of conducting five sessions per week for 3 weeks, this study ranged from 6 weeks. High frequency 10 Hz rTMS was directed to the right DLPFC against sham. The findings of the mentioned study found a statistically significant improvement in attention deficit, hyperactivity/impulsivity, and oppositional defiance symptoms, as measured by the SNAP-IV scale. Sham rTMS failed to show improvement in ADHD children.
The current study findings are also consistent with another open-label tolerability and safety trial in 10 children with ADHD. Despite using different rTMS parameters and without using the sham group showed fewer teacher-rated inattention and parent-rated hyperactivity/impulsivity symptoms 1 week after five daily sessions of 1Hz-rTMS over left DLPFC compared to baseline [19].
Alyagon et al. conducted a randomized sham controlled and active study of 43 young adults with ADHD. The results thereof proved the results of this work. They tested 15 sessions of 18 Hz-rTMS over 3 weeks, with 1-month follow-up and maintenance sessions over the right prefrontal cortex, targeting DLPFC, and inferior frontal cortex (IFC), validated the findings of the present study. Prior to and after the simulation, a short cognitive training session, targeting the right prefrontal cortex. They found improvement of adults’ ADHD symptoms, compared to control groups. The treatment effect size was diminished after 1 month of follow-up [26], and this was in concordance with the results of the present study as the effect size was reduced on follow-up 1 month after the last rTMS session.
Another study proved our results, in which 15 dTMS sessions over 3 weeks to the right PFC, left PFC, and the sham group was conducted. The study found that increased rDLPFC activation was associated with more symptom improvement in the right stimulation group. This study concluded that dTMS is an effective and feasible technique that may improve attention symptoms in adults with ADHD [27].
Also, the results are in concordance with a case study on the effects of repetitive transcranial magnetic stimulation in the treatment of ADHD, of a 22-year-old male diagnosed with ADHD. The protocol applied was 2 weeks of daily rTMS sessions to the right dorsomedial prefrontal cortex (10 Hz, 3000 pulses, 120% motor threshold) to treat attention deficit, hyperactivity, and impulsivity. One and 3 months after, assessments at baseline showed an overall improvement, steadily over this follow-up period [28]. Furthermore, a significant improvement of ADHD symptoms after 4 weeks of treatment was present in Niederhofer’s study that consisted of five sessions per week, in which low frequency rTMS (1 Hz) was used, to stimulate the motor area, using 1200 pulses per session [29].
Moreover, another two sham-controlled, double-blind crossover studies validated the results of this work. In 13 ADHD adults, one session of rTMS delivered at 20Hz directed right DLPFC significantly improved overall ADHD symptoms and inattention compared to the sham group [30]. Weaver et al. also observed a significant reduction and improvement in the ADHD IV scale after delivering 10 sessions of high-frequency rTMS (10 Hz) directed to the right DLPFC [18].
Our results were inconsistent with the results of Paz et al. [31] in their study of deep rTMS on 26 adults with ADHD. Conducting 20 daily sessions of deep TMS using the bilateral H5 coil directed to the prefrontal at high frequency failed to show any significant clinical outcome between active and sham groups. The inconsistency in the results between the 2 studies may be due to the different stimulation protocols, while Paz et al., used bilateral high-frequency deep TMS stimulation to PFC, our study applied high frequency rTMS stimulation to the right dorsolateral prefrontal cortex.
Limitations
This study aimed to explore the possible therapeutic role of repetitive transcranial magnetic stimulation and the effectiveness of combining Atomoxetine and rTMS in children with ADHD. However, this work has several limitations, firstly, the sample size is relatively small, so further studies should be conducted on the larger sample in order to ensure the results; moreover, the study included only unmedicated ADHD without comorbidities which is not representative to the broad spectrum of presentations of ADHD. Secondly, the absence of guidelines for combination therapy including the dose of tests atomoxetine and the stimulation protocol of rTMS. Thirdly, the absence of tests to assess executive functions to validate our results of clinical improvement of inattention, Finally, the follow-up period was relatively short, longer follow-up periods up to 6 months to track the long-term effect of rTMS.
Conclusions
Our results showed that five sessions per week, for 3 weeks (a total of 15 sessions), of high frequency (10 Hz) repetitive transcranial magnetic stimulation directed to the right DLPFC combined with atomoxetine is an efficacious treatment strategy for children with ADHD. Also, the combined treatment is more effective than using Atomoxetine. The optimum combination of treatment protocol and validation of our findings shall be furnished through further research. This study among others proved the clinical effect of rTMS in ADHD giving hope for further clinical trials to be conducted in order to pave the way for the approval of rTMS as a relatively safe tool that improves the symptoms and the global functioning in children with ADHD.
Availability of data and materials
The principal investigator, Mostafa Shohdy, has full access to all data used in the study, and can furnish data upon request. The integrity of the data and the accuracy of its analysis are the responsibility of M. Shohdy.
Abbreviations
- ADHD:
-
Attention deficit hyperactive disorder
- ATX:
-
Atomoxetine
- CGAS:
-
Children’s Global Assessment Scale
- CGI:
-
Clinical Global Impression
- CGI-I:
-
Clinical Global Impression- Improvement
- CGI-S:
-
Clinical Global Impression- Severity
- CPRS-R:L:
-
Conner’s Parent Rating scale Revised Long Version
- DLPFC:
-
Dorsolateral Prefrontal Cortex
- DSM IV:
-
Diagnostic and Statistical Manual of Mental Disorders Version IV
- FU:
-
Follow-up
- IFC:
-
Inferior frontal cortex
- IQR:
-
Interquartile range
- MRI:
-
Magnetic resonance imaging
- NS:
-
Nonsignificant
- RCT:
-
Randomized clinical trials
- rTMS:
-
Repetitive transcranial magnetic stimulation
- SCID:
-
Structured Clinical Interview for DSM IV
- SD:
-
Standard deviation
- VBM:
-
Voxel-based morphometry
References
Association AP (2013) Diagnostic and statistical manual of mental disorders: DSM-5. American Psychiatric Association, Arlington, p 947
Thomas R, Sanders S, Doust J, Beller E, Glasziou P (2015) Prevalence of attentiondeficit/hyperactivity disorder: a systematic review and meta-analysis. Pediatrics 135(4):E994–E1001. https://doi.org/10.1542/peds.2014-3482
Bishry Z, Ramy HA, El-Shahawi HH, El-Sheikh MM, El-Missiry AA, El-Missiry MA (2018) Screening for ADHD in a sample of Egyptian adolescent school students. J Atten Disord 22(1):58–65
Lukito S, Norman L, Carlisi C, Radua J, Hart H, Simonoff E, Rubia K (2020) Comparative meta-analyses of brain structural and functional abnormalities during cognitive control in attention-deficit/hyperactivity disorder and autism spectrum disorder. Psychol Med 50(6):894–919. https://doi.org/10.1017/s0033291720000574
Chen LZ, Hu XY, Ouyang L et al (2016) A systematic review and meta-analysis of tract-based spatial statistics studies regarding attention-deficit/hyperactivity disorder. Neurosci Biobehav Rev 68:838–847. https://doi.org/10.1016/j.neubiorev.2016.07.022
Rubia K (2018) Cognitive neuroscience of attention deficit hyperactivity disorder (ADHD) and its clinical translation. Front Hum Neurosci 12:100. https://doi.org/10.3389/fnhum.2018.00100
Wasserstein J, Stefanatos GA (2016) Re-examining ADHD as corticostriatal disorder: implications for understanding common comorbidities. ADHD Rep 24:1–10
Hart H, Radua J, Nakao T, Mataix-Cols D, Rubia K (2013) Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: exploring task-specific, stimulant medication, and age effects. JAMA Psychiatry 70:185–198. https://doi.org/10.1001/jamapsychiatry.2013.277
Norman LJ, Carlisi C, Lukito S, Hart H, Mataix-Cols D, Radua J, Rubia K (2016) Structural and functional brain abnormalities in attention-deficit/hyperactivity disorder and obsessive-compulsive disorder: a comparative meta-analysis. JAMA Psychiatry 73:815–825. https://doi.org/10.1001/jamapsychiatry.2016.0700
Cortese S, Adamo N, Del Giovane C et al (2018) Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry 5(9):727–738. https://doi.org/10.1016/S2215-0366(18)30269-4
Swanson JM (2019) Debate: are stimulant medications for attention-deficit/hyperactivity disorder effective in the long term? (Against). J Am Acad Child Adolesc Psychiatry 58(10):936–938. https://doi.org/10.1016/j.jaac.2019.07.001
Catala-Lopez F, Hutton B, Nunez-Beltran A et al (2017) The pharmacological and non-pharmacological treatment of attention deficit hyperactivity disorder in children and adolescents: a systematic review with network meta-analyses of randomised trials. PLoS One 12:e0180355
Rubio B, Boes AD, Laganiere S et al (2016) Noninvasive brain stimulation in pediatric ADHD: a review. J Child Neurol 31(6):784–796. https://doi.org/10.1177/0883073815615672
Zewdie E, Ciechanski P, Kuo HC, Giuffre A et al (2020) Safety and tolerability of transcranial magnetic and direct current stimulation in children: prospective single center evidence from 3.5 million stimulations. Brain Stimul 13(3):565–575. https://doi.org/10.1016/j.brs.2019.12.025
Dayan E, Censor N, Buch ER et al (2013) Noninvasive brain stimulation: from physiology to network dynamics and back. Nat Neurosci 16:838–844
Rubia K, Westwood S, Aggensteiner P-M, Brandeis D (2021) Neurotherapeutics for attention deficit/hyperactivity disorder (ADHD): a review. Cells. 10(8):2156. https://doi.org/10.3390/cells10082156
Cao P, Wang L, Cheng Q et al (2019) Changes in serum miRNA-let-7 level in children with attention deficit hyperactivity disorder treated by repetitive transcranial magnetic stimulation or atomoxetine: an exploratory trial. Psychiatry Res 274:189–194. https://doi.org/10.1016/j.psychres.2019.02.037
Weaver L, Rostain AL, Mace W et al (2012) Transcranial magnetic stimulation (TMS) in the treatment of attention-deficit/hyperactivity disorder in adolescents and young adults. J ECT 28(2):98–103
Gómez L, Vidal B, Morales L, Báez M et al (2014) Low frequency repetitive transcranial magnetic stimulation in children with attention deficit/hyperactivity disorder. Preliminary results. Brain Stimul 7(5):760–762. https://doi.org/10.1016/2Fj.brs.2014.06.001
Schulz KF, Altman DG, Moher D et al (2010) CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMC Med 8:18. https://doi.org/10.1186/1741-7015-8-18
Kumar G, Steer R (2003) Factorial validity of the Conners’ Parent Rating Scale – Revised: short form with psychiatric outpatients. J Pers Assess 80:252–259
El-Sheikh M, Sadek A, Omar A, Nahas G (2002) Psychiatric morbidity in first degree relatives of ADHD children. Ain Shams University, Cairo
Shaffer D, Gould MS, Brasic J, Ambrosini P, Fisher P, Bird H, Aluwahlia S (1983) A Children’s Global Assessment Scale (CGAS). Arch Gen Psychiatry 40(11):1228–1231. https://doi.org/10.1001/archpsyc.1983.01790100074010
Guy W (1976) ECDEU Assessment manual for psychopharmacology. US Department of Health, Education, and Welfare Public Health Service Alcohol, Drug Abuse, and Mental Health Administration, Rockville
Cao P, Xing J, Cao Y et al (2018) Clinical effects of repetitive transcranial magnetic stimulation combined with atomoxetine in the treatment of attention-deficit hyperactivity disorder. Neuropsychiatr Dis Treat 14:3231–3240. https://doi.org/10.2147/ndt.s182527
Alyagon U, Shahar H, Hadar A, Barnea-Ygael N, Lazarovits A, Shalev H, Zangen A (2020) Alleviation of ADHD symptoms by non-invasive right prefrontal stimulation is correlated with EEG activity. Neuroimage Clin 26:102206. https://doi.org/10.1016/j.nicl.2020.102206
Bleich-Cohen M, Gurevitch G, Carmi N et al (2021) A functional magnetic resonance imaging investigation of prefrontal cortex deep transcranial magnetic stimulation efficacy in adults with attention deficit/hyperactive disorder: a double blind, randomized clinical trial. NeuroImage 30:102670 https://www.sciencedirect.com/science/article/pii/S2213158221001145
Asimoglou E, Tsakiri A, Gkikas P, Kalimeris S, Karampoutakis G (2021) Effects of repetitive transcranial magnetic stimulation in the treatment of attention-deficit hyperactivity disorser. A case study. Eur Psychiatry 64(S1):S492–S493. https://doi.org/10.1192/j.eurpsy.2021.1317
Niederhofer H (2008) Effectiveness of the repetitive transcranial magnetic stimulation (rTMS) of 1 Hz for attention-deficit hyperactivity disorder (ADHD). Psychiatr Danub 20(1):91–92
Bloch Y, Harel EV, Aviram S, Govezensky J, Ratzoni G, Levkovitz Y (2010) Positive effects of repetitive transcranial magnetic stimulation on attention in ADHD Subjects: a randomized controlled pilot study. World J Biol Psychiatry 11(5):755–758
Paz Y, Friedwald K, Levkovitz Y et al (2018) Randomized sham-controlled study of high-frequency bilateral deep transcranial magnetic stimulation (dTMS) to treat adult attention hyperactive disorder (ADHD): Negative results. World J Biol Psychiatry 19(7):561–566. https://doi.org/10.1080/15622975.2017.1282170
Acknowledgements
The staff of the child psychiatry clinic and EEG and rTMS unit in the Institute of Psychiatry – Ain Shams University Hospitals were cooperative with the research team, and therefore contributed to these findings. The authors would like to voice their sincere gratitude and utmost appreciation.
Funding
This research did not receive any specific grant from funding agencies in any sector. Even though it had no role in any aspect of the study (design, conduct, data collection and management, analysis and interpretation), Okasha Institute of Psychiatry provided rTMS with no operating fees. Any other expenses were borne by the authors.
Author information
Authors and Affiliations
Contributions
NN proposed the research idea and design. GR contributed to developing the research idea, study methodology, and editing of the manuscript. SK helped in developing the study methodology and editing of the manuscript. DA helped in developing the study methodology, revising the data analysis, and helped in the interpretation and editing of the manuscript. HE contributed to the design of the study methodology and editing of the manuscript. The data collection and analysis were conducted by Mostafa Shohdy, who wrote the final manuscript, that was read and approved by all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The trial protocol was approved by the Research Ethics Committee (REC) at the Ain Shams University Faculty of Medicine (FMASU REC FWA00017585).
The legal guardians of the patients participating in the study signed a consent form, after the aim, procedure and expected benefits, possible side effects, as well as the right to abort the participation in the study at any point, without stating reasons, were clearly explained and outlined to them orally and in writing. They also approved the use and publishing of their data, anonymously, for scientific publications.
Competing interests
There is no conflict of interest to the best of the authors’ knowledge.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Nagy, N.A.S., Amin, G.R., Khalil, S.A. et al. The therapeutic role of repetitive transcranial magnetic stimulation in children with attention deficit/hyperactivity disorder in Egypt a randomized sham controlled clinical trial. Middle East Curr Psychiatry 29, 55 (2022). https://doi.org/10.1186/s43045-022-00210-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-022-00210-3