
Abstract
Background
Well-being includes the physical, social, and emotional dimensions of a person’s state. University students experience increased levels of psychological and academic distress, mostly affecting their mental well-being. This study employed a descriptive, correlational, cross-sectional design to assess the level of mental well-being among health sciences students at three health science colleges at King Saud University in Riyadh, Saudi Arabia. Convenience total sampling was used to select 339 female undergraduate students from the three faculties. A questionnaire consisting of two parts—a sociodemographic datasheet and the Arabic version of the Warwick–Edinburgh Mental Well-being Scale (WEMWBS) without modifications to assess individuals’ mental well-being—was distributed, with data collection lasting for one month (February 2019).
Results
Participants had an average level of mental well-being, with the highest recorded among students from the College of Pharmacy and the lowest recorded among the students from the College of Nursing. The study findings revealed no significant correlations or differences in the mental well-being of the questionnaire respondents according to sociodemographic variables.
Conclusions
It is important to assess the mental well-being of students to detect any possible mental illnesses or disturbances and address any issues so as to support their academic achievement.
Similar content being viewed by others


Background
Positive mental health was declared by the World Health Organization in its 2018 Summary Report to be the “foundation for well-being and effective functioning for both the individual and the community,” while mental well-being (MWB) was defined as “a state which allows individuals to realize their abilities, cope with the normal stresses of life, work productively and fruitfully, and make a contribution to their community” [1]. More broadly, well-being includes the physical, social, and emotional dimensions of a person’s state; a healthy state of well-being exists when the basic needs of individuals are met, they have a sense of purpose, and they are able to achieve important personal goals and socialize in society. As such, mental health is not just the absence of mental disorders [1].
However, a knowledge deficit concerning MWB exists in the community, with many individuals unable to identify symptoms of common disorders affecting MWB, such as depression, while those with these conditions often fail to receive and comply with treatment strategies endorsed by professionals [2]. As cited by Thai and Nguyen [3], there are approximately 450 million people worldwide living with mental disorders that firstly arose during adolescence and young adulthood. In addition, at least 350 million people total are living with depression worldwide [1]. According to the National Institute of Mental Health [4], an estimated 20.1% of 18- to 25-year-old worldwide are experiencing mental health issues; thus, poor MWB among college students has grown into a significant public health issue. A study by the Healthy Minds Institute revealed that 17% of undergraduate students screened positive for depression, including 9% with major depression, while 10% had an anxiety disorder [5].
Indicators of poor MWB are exemplified by data from the National College Health Assessment, where one in six undergraduate students reported within the last 6 months that they “felt so depressed [that] it was difficult to function,” one in five in the last 6 months “felt overwhelming anxiety,” and one in 15 had “seriously considered suicide in the past year” [6]. Supporting these data, current research indicates that more than half of college and university counseling center directors reported that the severity of student mental health concerns on their campus had increased from 2015 to 2016 [7]. University students often experience increased levels of psychological and academic distress and further encounter stressors resulting from family instability and dysfunction, substance misuse, and psychological disorders that can result from not completing their chosen academic programs or courses [8,9,10]. Thus, students’ overall physical and MWB, including their academic performance, may be impacted by their elevated levels of stress [11].
There is also a robust and intensifying base of evidence specifying that university students are at very high risk for mental disorders and psychological distress and that the prevalence and severity of mental difficulties are rising among student populations [12]. Health professional students in particular face challenges to their mental health and well-being, including elements of psychological distress such as depression, anxiety, and burnout [13, 14]. These conditions are related to participation in health professional courses that are demanding in terms of competition for specific career pathways, long contact hours and course lengths, knowledge retention requirements, and the frequently confronting circumstances associated with service provision. As peer influence is crucial to identity formation and decision-making in emerging adulthood, perceptions of peer beliefs and the experience of social pressures are integral to the decision to seek help within this culture.
In Saudi Arabia, very little research had been carried out to date that has focused on the nature of MWB among university students. Therefore, this research study was designed to assess the level of MWB among health sciences students at King Saud University in Riyadh, Saudi Arabia, and to identify significant differences in their well-being based on selected demographic characteristics.
Aim of the study
The present study, which aimed to assess the MWB among health sciences students at King Saud University, sought specifically to accomplish the following research objectives:
-
1.
Identify the personal characteristics of health sciences students who participated in this study
-
2.
Assess the level of MWB of the studied participants.
-
3.
Identify the correlation between the level of MWB and demographic characteristics among health sciences students
Research questions
-
1.
What are the demographic characteristics of health sciences students?
-
2.
What is the level of MWB of health sciences students?
-
3.
Is there a correlation between the demographic characteristics and the level of MWB among health sciences students?
Methods
Research design
This study used a descriptive, correlational, cross-sectional design to identify the demographic characteristics of health sciences students and explore the nature of their MWB. It also assessed whether there were significant differences in the levels of MWB of health sciences students when grouped according to certain demographic characteristics.
Research setting
This study involved students from the College of Nursing, College of Pharmacy, and College of Medicine at King Saud University. The reason for choosing the participants from these specialties was that, for all of these three specialties, students take an advanced-level mental health course as part of their undergraduate curriculum. King Saud University was chosen as the site for this study because it is the largest governmental university in the Kingdom of Saudi Arabia that supports and facilitates the conduct of research work.
Sampling
Convenience sampling (total in specific) was performed in the current study to promote wider participation of health sciences students as defined by the inclusion and exclusion criteria. Due to the cultural sensitivity of the Saudi universities, the researcher preferred implementing the current research in the female campus of the three health science colleges at King Saud University for her convenience and the easy access to students.
Eligible participants were those who met the following criteria:
-
1.
Officially registered for the 2018 to 2019 academic year during the conduct of this study
-
2.
Female health sciences students from the College of Nursing, College of Pharmacy, and College of Medicine at King Saud University, who had already passed the preparatory year in their health sciences program. Females only were included for the convenience and accessibility of the researcher.
-
3.
Available at the time the data were collected
-
4.
Were willing volunteers to participate in this study
The total number of eligible students who met the inclusion criteria was 400; however, 339 surveys were finally processed, representing a response rate of 85%. As the total number of female students at the three colleges was only 400, the researcher preferred studying all accessible students utilizing convenience sampling “total sampling” to give the best reflection and representation of the current population.
Study tool
The questionnaire for the current study is composed of two parts: a demographic profile and an MWB survey. The first part of the questionnaire assessed the demographic characteristics of female students who willingly consented and participated in this study, including their age, marital status, college in which they were registered, academic level, and place of residence. Meanwhile, to assess the MWB of the participants, the Warwick–Edinburgh MWB Scale (WEMWBS) was used [15]. This scale was developed by an expert panel who drew on recent academic literature and qualitative research with a focus on undergraduate students and following psychometric testing of an existing scale. The scale consists of 14 positively worded items designed to assess a respondent’s MWB over the last two weeks. The questionnaire was completed using a 5-point Likert scale (1–5 points) corresponding to the following response categories: none of the time, rarely, some of the time, often, and all of the time.
No modifications were made after pilot testing of the present study; hence, only its reliability was tested. For reliability testing, the WEMWBS survey was deployed among 40 male respondents from the same colleges (representing 10% of the sample size) in an Arabic version developed by Zayed in Oman in 2018 [16]. A content validity assessment of the scale was carried out by three experts in psychology and psychiatric health nursing. Furthermore, reliability tests confirmed a Cronbach’s alpha value of 0.870, which indicated good internal consistency. These findings imply that the WEMWBS was an acceptable means for data collection in this study.
Data collection
After obtaining ethical approval, the pilot study was conducted to test the feasibility and applicability of the research project, while the empirical investigation and actual work study were conducted after the pilot results were analyzed. The study participants were recruited after reviewing all students registered for the academic year. The questionnaire was administered to study participants by hand during the working days of the mental health course and all copies were retrieved by the study investigator after the participants finished their responses. The duration time for data collection was one month (February 2019). The participants were gathered in groups in a classroom before the questionnaire was distributed to them by the study investigator and were provided with a pencil for answering the survey. Filling out the questionnaire took approximately 10 to 15 min for each participant.
Ethical considerations
Ethical approval was obtained from the directorate of the College of Medicine, College of Pharmacy, and College of Nursing and the institutional review board at King Saud University. An authorization letter from the committee was issued to permit the investigator to perform the pilot and main study. The investigator assured the informed consent, confidentiality, and privacy of the study participants. All of the study participants who were approached and who voluntarily agreed to participate by answering the questionnaire were informed of the nature and purpose of the study before being included. The participants were told that they could withdraw their participation in the study at any time and for any reason. Furthermore, the investigator also explained the conduct of the study verbally to the eligible participants. They were informed that their responses would remain confidential and their identities would not be revealed in research reports or in the publication of findings. It was emphasized that their refusal to participate would not influence or terminate their academic participation at King Saud University. Official permission from the corresponding authors for the use of WEMWBS scale was obtained via email.
Data analysis
All analyses were performed using the Statistical Package for the Social Sciences version 23 software program (IBM Corporation, Armonk, NY, USA) [17]. Descriptive statistics were used to analyze the data of all study variables. Percentages were calculated to determine the demographic characteristics of the health sciences students. Weighted mean values were calculated to measure the levels of MWB of the participants. An analysis of variance was used to compare the levels of MWB of the participants when they were grouped according to their demographic profile. The significance level was set at a probability value of 0.05.
Results
The results of the current study are represented in three tables. In total, 339 university students from the three colleges at King Saud University participated, including 135 from the College of Nursing, 117 from the College of Pharmacy, and 87 from the College of Medicine.
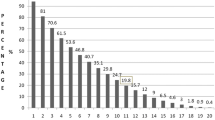
In terms of the age of the participants, as shown in Table 1, the majority of the participants from the three colleges were aged between 16 and 20 years old (n = 185; 58.54%), while 129 (40.82%) were aged between 21 and 25 years old, and 25 (7.91%) were aged between 26 and 30 years old. Considering the marital status of the participants, most were single (n = 307; 97.15%), 28 (8.86%) were married, and 4 (1.27%) were widowed. Regarding the academic level of the participants, nearly half (145, 45.89%) of the participants were in level 4, more than one-quarter (n = 84; 26.58%) were in level 3, 67 (21.20%) were in level 6, and 43 (13.61%) were in level 5. Most of the participants (n = 318; 93.80%) from the three colleges lived inside Riyadh, while a few (n = 21; 6.20%) lived outside Riyadh. Among those participants who lived inside Riyadh, nearly half lived in the northern part of Riyadh (n = 150; 44.2%), while the remaining participants lived in the eastern part (n = 81; 23.90%), southern part (n = 49; 14.50%), and western part (n = 38; 11.20%), respectively. Among those university students who resided outside Riyadh, 14 (4.10%) university students from the 3 colleges lived in the western part, 4 (1.20%) lived in the eastern part, 2 (0.60%) lived in the northern part, and just 1 (0.30%) lived in the southern part of Saudi Arabia.
As presented in Table 2, the MWB of the participants indicated that the highest scored indicator was item 11 [mean = 3.95 points, standard deviation (SD) = 1.03 points], which revealed that participants were often able to make up their own minds about things. The other MWB indicators with high scores, in descending order, were items 13 (mean = 3.74 points, SD = 1.02 points), 12 (mean = 3.69 points, SD = 1.07), 2 (mean = 3.59 points, SD = 1.09 points), 4 (mean = 3.35 points, SD = 1.14 points), 1 (mean = 3.56 points, SD = 1.09 points), and 10 (mean = 3.55 points, SD = 1.09 points), respectively. On the other hand, the MWB indicators with low scores were items 14, 8, 6, 9, 5, 7, and 3, respectively (mean < 3.5 points); the lowest scored indicator (item 3) correlated with the participants sometimes feeling relaxed.
Participants generally had an average level of MWB, with the highest values recorded for the students from the College of Pharmacy (mean = 3.49 points, SD = 1.08 points) and the lowest values recorded for the students from the College of Nursing (mean = 3.30 points, SD = 1.06 points), with no significant difference between them.
Regarding the correlation between and within demographic variables and MWB among health sciences university students (Table 3), the statistical results showed that there were no significant associations between and within the age groups of health sciences university students and their MWB (F = 0.088; p = 0.916). In terms of the marital status of the participants, the statistical results showed that there were no significant associations between and within the marital status groups of health sciences university students and their MWB (F = 2.343; p = 0.098).
With regard to the college of the participants, the statistical results showed that there were no significant associations between and within the college groups of health sciences university students and their MWB (F = 2.233; p = 0.109). Similarly, considering the academic level of the participants, the statistical results showed that there were no significant associations between and within the academic level groups of health sciences university students and their MWB (F = 0.481; p = 0.696).
Moreover, the statistical results also showed that there were no significant associations between and within the residence groups of health sciences university students and their MWB (F = 0.103; p = 0.749). Further, for those participants residing inside Riyadh, the statistical results showed that there were no significant associations between and within the health sciences university students’ residence groups and their MWB (F = 0.924; p = 0.450). In similar fashion, for those living outside Riyadh, the statistical results showed that there were no significant associations between and within the health sciences university students’ residence groups and their MWB (F = 0.736; p = 0.568).
Discussion
The discussion of the current study was based on its findings guided by the research objectives. Mental health among young people is of acute concern and a global issue nowadays [18]. Moreover, studies have shown that university students exhibit a great deal of vulnerability in relation to suffering mental health disorders [19,20,21].
While family affluence, sex, and age have been shown to impact young people’s MWB [1], our results showed that the majority of participants were registered in their second year of school (level 4), which is different from other studies that surveyed participants who were mostly in their first year at university [22,23,24]. The current study is similar to other studies in terms of demographics in that the majority of participants were female aged 15 to 21 years old and living in an urban area [22, 24,25,26]. Additionally, it is comparable to other studies performed in Portugal [27] and Saudi Arabia [28] in that the majority of the participants attending college and university were single.
With regard to the MWB among health sciences university students, it was found that the highest scored indicator was item 11, which reflected that participants were often able to make up their own minds about things. Seemingly in contrast, as cited by Tennant et al. [29], distinct bodies of research are less obvious in the literature relating to poor mental health, where items measuring effects like feeling happy or sad are often combined with items measuring psychological functioning such as playing a useful part in things and making decisions, which suggests that poor mental health at least is accepted as involving limitations in MWB. Meanwhile, the lowest scored indicator in the present research was item 3, which revealed that participants rarely felt relaxed. The study of Thai and Nguyen [3] noted that the ability to relax and meditation was the highest scored intervention related to mental health for depression among public health and sociology undergraduate students in Hanoi, Vietnam, while using alcohol and smoking were their least frequent interventions.
Similarly, the association between participants’ demographic characteristics such as their age, marital status, college, academic level, and residence and their MWB revealed no significant results. The findings of the study related to the above-mentioned variables are contrary to those of another study wherein significant differences were observed between age groups in that people aged 16 to 24 years old showed higher scores of MWB than did other age groups, while MWB scores were significantly higher among men than among women [29]. Although not considered in the current study, a similar study also found that individuals with previous mental disorders experienced significantly lower levels of well-being than did those with no previous mental disorders [24]. Overall, the results of the current study regarding the relationship between participants’ demographic characteristics and their level of MWB suggest that the MWB of female health sciences university students was not affected by any of their demographic characteristics.
Conclusion
The present study contends that increasing international interest in the concept of MWB and its contribution to all aspects of human life is evident. The study findings indicated that the majority of participants were aged between 16 and 20 years old, almost all were single, many were in level 4 of their education, and most lived in the northern part of the Riyadh region. The participants overall boasted an average level of MWB, with the highest found among students from the College of Pharmacy and the lowest found among students from the College of Nursing.
The level of MWB among the participants revealed that the highest scored indicator was item 11, which reflected that they were often able to make up their own minds about things, while the lowest scored indicator was item 3, which revealed that the participants rarely felt relaxed. Regarding the association between participants’ demographic characteristics and their MWB, the findings revealed no significant correlations or differences in the MWB of the participants according to certain sociodemographic variables.
Implications of the study
The findings of the current study have some implications for both faculty and administrators at health science colleges. It is important to assess the MWB of students when accepting them at the university level to detect any possible mental illnesses or disturbances and work to treat and mitigate them in the earliest stages, thus setting up students for success in their academic journey. University administrators and faculty must work together to plan and revise the policies and guidelines for the admission criteria of accepting high school students or students from the preparatory year to the university.
While transitioning from high school to college or university, health sciences university students need to strengthen their MWB in order to be able to overcome the challenges brought about by the demanding workload at the university level of education. The assessment of the MWB of students can help university administrators in developing programs geared toward improving their MWB while continuing their studies and in anticipation of the successful completion of their chosen program.
University faculty members should be offered courses focusing on mental health so they can recognize indicators of mental problems among students and possibly prevent worsening of these conditions by referring the student to the psychiatric guidance clinic. Moreover, it is recommended that faculty members work to increase the coverage of mental health subjects in courses geared toward students in the preparatory year to prepare them to face challenges during the rest of their academic journey.
Limitations
There is a lack of an ability to generalize the findings of the current study as it focused and included only female health sciences students. Also, self-reporting is a unique source of data collection that increases the potential for bias as the investigator is unable to ensure that the students who participated reported all information honestly. In future research, drawing from a larger sample size of both sexes and from different universities and colleges, investing in a longitudinal design, and using random sampling are key tactics that may allow better study generalizability.
Availability of data and materials
The data supporting the findings in this study are confidentially available from the corresponding author upon reasonable request.
Abbreviations
- MWB:
-
Mental well-being
- WEMWBS:
-
Warwick–Edinburgh Mental Well-being Scale
References
World Health Organization (2018) Mental health: strengthening our response (Fact Sheet). https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response.
Jorm AF (2015) Why we need the concept of “mental health literacy”. Health Commun 30(12):1166–1168
Thai QCN, Nguyen TH (2018) Mental health literacy: knowledge of depression among undergraduate students in Hanoi, Vietnam. Int J Mental Health Syst 12(1):19
National Institute of Mental Health (2017) Any mental illness (AMI) among US adults. US Department of Health and Human Services Bethesda (MD). https://www.nimh.nih.gov/health/statistics/mental-illness.shtml.
Hunt J, Eisenberg D (2010) Mental health problems and help-seeking behavior among college students. J Adolesc Health 46(1):3–10
American College Health Association (2017) National College Health Assessment II-Undergraduate Student Reference Group Data Report Fall 2016. Available at: https://wwwachaorg/documents/ncha/NCHA-II_FALL_2016_UNDERGRADUATE_REFERENCE_GROUP_EXECUTIVE_SUMMARYpdf Updated March, 2018 29:1-19
Reetz DR, Bershad C, LeViness P, Whitlock M (2016) The association for university and college counseling center directors annual survey. 2015 AUCCCD Survey, Reporting period: September 1, 2015 through August 31, 2016. AUCCCD:1–118
Stallman HM (2010) Psychological distress in university students: a comparison with general population data. Aust Psychol 45(4):249–257
Andrew S, Salamonson Y, Weaver R, Smith A, O’Reilly R, Taylor C (2008) Hate the course or hate to go: semester differences in first year nursing attrition. Nurse Educ Today 28(7):865–872
Kitzrow MA (2003) The mental health needs of today's college students: challenges and recommendations. J Stud Aff Res Pract 41(1):167–181
Stoeber J, Rambow A (2007) Perfectionism in adolescent school students: Relations with motivation, achievement, and well-being. Pers Individ Diff 42(7):1379–1389
Baik C, Larcombe W, Brooker A, Wyn J, Allen L, Brett M, James R (2016) A framework for promoting student mental wellbeing in universities. Enhancing Student Wellbeing
Shapiro SL, Shapiro DE, Schwartz GE (2000) Stress management in medical education: a review of the literature. Acad Med 75(7):748–759
Balogun JA, Titiloye V, Balogun A, Oyeyemi A, Katz J (2002) Prevalence and determinants of burnout among physical and occupational therapists. J Allied Health 31(3):131–139
Taggart F, Stewart-Brown S, Parkinson J (2016) Warwick-Edinburgh mental well-being scale (WEMWBS). User Guide (Version 2) Edinburgh: NHS Health Scotland, Warwick Medical School, University of Warwick
Zayed K (2018) Warwick-Edinburgh Mental Well-being Scale (WEMWBS) in Arabic Language. Warwick Medical School. https://warwick.ac.uk/fac/sci/med/research/platform/wemwbs/using/translations/.
IBM Corp (2015) IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp. Released 2015.
Byrne S, Swords L, Nixon E (2015) Mental health literacy and help-giving responses in Irish adolescents. J Adolesc Res 30(4):477–500
Storrie K, Ahern K, Tuckett A (2010) A systematic review: students with mental health problems—a growing problem. Int J Nurs Pract 16(1):1–6
Universities UK Student mental wellbeing in higher education: good practice guide. In: London: MWBHE/Universities UK/Standing Conference of Principals, 2015.
Royal College of Psychiatrists (2011) Mental health of students in higher education, College Report CR166 September 2011. Royal College of Psychiatrists
O’Connor M, Casey L (2015) The Mental Health Literacy Scale (MHLS): A new scale-based measure of mental health literacy. Psychiatry Res 229(1-2):511–516
Kutcher S, Wei Y, Morgan C (2016) Mental health literacy in post-secondary students. Health Educ J 75(6):689–697
Gorczynski P, Sims-Schouten W, Hill D, Wilson JC (2017) Examining mental health literacy, help seeking behaviours, and mental health outcomes in UK university students. The Journal of Mental Health Training, Education and Practice
McCann T, Lu S, Berryman C (2009) Mental health literacy of Australian Bachelor of Nursing students: a longitudinal study. J Psychiatric Mental Health Nurs 16(1):61–67
Reavley NJ, McCann TV, Jorm AF (2012) Mental health literacy in higher education students. Early Interv Psychiatry 6(1):45–52
Dias P, Campos L, Almeida H, Palha F (2018) Mental health literacy in young adults: Adaptation and psychometric properties of the mental health literacy questionnaire. Int J Environ Res Public Health 15(7):1318
Mahfouz MS et al. (2016) Mental health literacy among undergraduate students of a Saudi tertiary institution: a cross-sectional study. Mental illness
Tennant R et al (2007) The Warwick-Edinburgh mental well-being scale (WEMWBS): development and UK validation. Health Qual Life Outcomes 5(1):63
Acknowledgements
The researcher would like to thank the students who participated in this study and King Saud University for facilitating the conduct of the study in the Health Science Specialty Colleges. Acknowledgment is to the Middle East Current Psychiatry Journal for their publishing support.
Funding
None.
Author information
Authors and Affiliations
Contributions
EA conceived and designed the study, did the data collection and statistical analyses, editing, and submission of the manuscript. The author read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Written informed consent was obtained from all participants and the study was approved by the institutional review board at King Saud University (ethical approval no. E-18-3617, received 30 January 2019).
Consent for publication
Not applicable.
Competing interests
The investigator declares that no conflicts of interest exist concerning the research work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alshehri, E.A.R. Mental well-being among health science specialty female students in Riyadh, Saudi Arabia. Middle East Curr Psychiatry 28, 15 (2021). https://doi.org/10.1186/s43045-021-00096-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43045-021-00096-7