
Abstract
Background
Considering the close link between polycystic ovary syndrome (PCOS) and metabolic syndrome considerable research has been devoted to studying the pattern of fat distribution in PCOS.
Objectives
The study aims to assess the usefulness of dual-energy X-ray absorptiometry (DEXA) based regional fat distribution indices as a predictor of the development of PCOS.
Methods
This case–control study recruited diagnosed cases of PCOS using Rotterdam Criteria (cases n = 86) and healthy age-matched controls (n = 90). DEXA was performed in both groups for assessment of total and regional body fat distribution after undergoing ultrasonography (USG) and baseline/biochemical evaluation.
Results
The study revealed a significant difference between cases and controls in trunk fat percentage (40.2% ± 9.1% vs 26.5% ± 9.1%; p < 0.001), android fat percentage (42.4% ± 41%vs 27.8% ± 1.51%; p < 0.001), total fat percentage (43.8% ± 8% vs28.5% ± 1.6%; p < 0.001), fat mass/ht2 (fat mass index) (8.82 ± 3% vs 4.8 ± 1.7%; p < 0.001), android/gynoid ratio (1.05 ± 0.1 vs 0.7 ± 0.2; p < 0.001), and trunk/limb fat mass ratio (1.06 ± 0.3 vs 0.69 ± 0.3; p 0.001). Multivariate analysis revealed a significant relation of trunk fat mass with android % fat, gynoid fat mass, and android-gynoid ratio.
Conclusions
The study demonstrates that there is a central pattern of fat distribution in patients with PCOS while the overall fat might not be increased which is well analyzed by DEXA. Hence, we suggest its use in the initial diagnostic workup and follow-up of PCOS patients for their body fat distribution and content.
Similar content being viewed by others
Background
It is estimated that 6 to 20% of women in the reproductive age group have polycystic ovarian syndrome (PCOS), characterized by oligo/anovulation, hyperandrogenism, and/or polycystic ovaries with the majority of them having hyperinsulinemia and insulin resistance [1]. Increased insulin stimulates ovarian androgen production and decreases hepatic production of sex-hormone binding globulin (SHBG), and thus free testosterone is increased [2]. Different study populations of PCOS have varying prevalence of overweight/obesity [3]. Pattern of fat distribution alters the metabolic risk in PCOS including the propensity to develop type-ii diabetes [4]. Central obesity is ubiquitous in PCOS irrespective of differences in weight and is known to decrease levels of adiponectin and increase secretion of other adipokines and inflammatory markers [5]. Whole-body dual-energy X-ray absorptiometry (DEXA) scans are a proven method to estimate total, abdominal, and extremity fat mass [6]. Some studies have found increased trunk fat in patients with PCOS compared to controls and fat mass-based indices could be superior to the measurement of body mass index (BMI) or waist circumference as a predictor of metabolic risk in PCOS [7].
The aim of the present study was to compare the usefulness of regional fat mass DEXA indices as a predictor of the development of PCOS.
Objectives
To assess body fat distribution in patients with PCOS using dual-energy X-ray absorptiometry and determine the predictability of various fat indices in diagnosing the cases.
Methods
The case–control study was conducted in the Department of Radiodiagnosis and Imaging, Government Medical College Srinagar, India from July 2019 up to July 2022. The cases were referred from the Department of Dermatology and Department of Gynecology, Sher-i-Kashmir Institute of Medical Sciences, Srinagar. It enrolled 94 cases of PCOS (age > 18 years) and 90 age-matched controls. The Rotterdam 2003 criteria [8] were used to diagnose PCOS in which two out of three criteria must be present:
-
1. Oligomenorrhea (menstrual cycle length of more than 35 days but less than 90 days) or anovulation (absence of menstrual cycle for more than 90 days).
-
2. Hyperandrogenism (clinical/biochemical): modified Ferriman Gallwey score [9] ≥ 8 or total testosterone of > 0.48 ng/ml.
-
3. Sonographically polycystic ovaries: ≥ 12 follicles (2–9 mm) in each ovary or volume of > 10 cc.
Exclusion criteria
Patients with clinical or biochemical evidence of other endocrine disorders, e.g., Cushing syndrome, hyperprolactinemia, congenital adrenal hyperplasia, ovarian or adrenal tumors associated with hyperandrogenism. Patients who had a history of drug intake in the previous 6 months that could alter metabolism were also excluded. Out of the 94 recruited patients, 8 were excluded based on the presence of other endocrine abnormalities or intake of medicine in the previous 6 months.
Selection of controls
Ninety age-matched healthy female volunteers who had no clinical/sonographic/biochemical evidence of PCOS were taken as controls. Prior permission was obtained from the ethical committee before conducting the study. All subjects and controls were informed about the details of the study.
Clinical information
A detailed history was taken and a physical examination was done for the presence of signs and symptoms of hyperandrogenism, i.e., hirsutism, acne, androgenetic alopecia, and acanthosis nigricans and menstrual irregularities (oligomenorrhea/amenorrhea). Prior to the referral, the referring physicians from the departments of dermatology and gynecology would advise the patients to practice the barrier method, specifically the use of condoms by their partners to prevent conception in the cases and on the day of DEXA scan, a rapid hCG Card test would be performed. Both the use of the barrier method of contraception and rapid hCG card test were included in the consent protocol to include only those cases who agreed to the protocol. The hCG card test results were then checked by the investigators and DEXA scans were done on patients with a negative pregnancy hCG card test. None of the cases or controls in our study cohort were pregnant at the time of the scan.
A hirsutism assessment was done based on mFGS and a score ≥ 8 (out of 36) was considered clinical hirsutism.
Baseline and biochemical investigations
Fasting blood samples were collected between 8 and 10 am in the follicular phase, on the 2nd or 3rd day of the menstrual cycle (or during the progestin-induced cycle), and tested for LH, FSH, PRL, testosterone, 17alpha hydroxyprogesterone using electrochemiluminescence immunoassay of pooled samples. Metabolic evaluation included total cholesterol, high-density lipoproteins (HDL), low-density lipoproteins (LDL), and triglycerides.
Ultrasonography
USG was performed on the same day as blood tests (day 2–3) either by transvaginal ultrasound (TVS) probe (frequency 9–12 Hz) in married or transabdominal ultrasound (TAS) with curvilinear probe (frequency 3–5 Hz) in unmarried cases.
DEXA
Dual-energy X-ray absorptiometry technique was performed using the Hologic Discovery USA machine within seven days of blood tests and USG. The patients were required to be overnight fasting and without any metal accessories. The percentage of total body fat was calculated by the ratio of total fat mass/total body mass. The body fat composition was assessed for the limbs, trunk, android, and gynoid regions along with total body fat percentage, fat mass/height2, android/gynoid ratio, and trunk/limb fat mass ratio.
The raw data was transferred to the Hologic QDR station. NHANES calibration was used as the default setting in APEX Version 2.0 of the Hologic QDR workstation, based on research studies comparing DXA results in the NHANES pilot study to other body composition measurement systems, principally deuterium dilution and hydrostatic weighing [10]. The “NHANES BCA” adjustment to the classic calibration was implemented via a multiplicative reduction in lean mass as recommended by Schoeller et al., with the practical implication that leaner subjects (individuals with more lean mass) will see a greater increase in % body fat than subjects with less lean mass.
Statistical analysis
Statistical analysis was performed in SPSS Statistics for Windows (Version 25.0. Armonk, NY: IBM Corp.). The study population was divided into two groups: (1) PCOS patients, and (2) controls.
Continuous variables were presented as means ± standard deviation (SD) or median with interquartile range where appropriate. Means were compared between the two groups using t-tests where appropriate. Categorical variables were expressed as counts and percentages of the total. Data across the two groups was compared using one-way ANOVA for multiple comparisons. Multivariate analysis was done using the MANOVA test. The correlation between continuous and categorical parameters was assessed using univariate regression analysis. Significance was set at p < 0.05.
Results
Table 1 shows the demographic, anthropometric, and DEXA indices of patients with and without PCOS. The majority of cases (both PCOS and controls) were in the age group of 25–29 years (47%).
Data across the two groups was compared using one-way ANOVA for multiple comparisons.
The table reveals statistically significant differences in some DEXA indices between PCOS patients and controls in the following:
-
1. Arms fat mass, arms fat %
-
2. Trunk fat mass and fat %
-
3. Android fat mass, android total mass.
-
4. Android-gynoid ratio.
-
5. Fat mass index.
-
6. Total body % fat.
-
7. Trunk/limb fat mass ratio.
There was preferential fat distribution in a trunk in females with PCOS as compared to controls (58.5% vs 49.3% of total fat mass; p value < 0.0001).
Pair-wise correlation between various DEXA/anthropometric indices by Pearson correlation coefficient analysis was done. The results are shown in Fig. 1a–f.

a Pair-wise correlation between arm fat mass and leg fat mass. The first graph above shows the log-likelihood function of the difference between the arm fat mass and leg fat mass. The second shows a uniform prior distribution which suggests no prior belief. The third graph shows the plot of the posterior distribution of 0.8. b Pair-wise correlation between trunk fat mass and android fat mass. The first graph above shows the log-likelihood function of the difference between the trunk fat mass and Android fat mass. The second shows a uniform prior distribution, this suggests no prior belief. The third graph shows the plot of the posterior distribution of 0.8. c Pair-wise correlation between trunk fat mass and fat mass/height2. The first graph above shows the log-likelihood function of the difference between the trunk fat mass and fat mass/height2. The second shows a uniform prior distribution, this suggests no prior belief. The third graph shows the plot of the posterior distribution of 0.8. d Pair-wise correlation between trunk fat mass and android-gynoid ratio. The first graph above shows the log-likelihood function of the difference between the trunk fat mass and the android/gynoid ratio. The second shows a uniform prior distribution which suggests no prior belief. The third graph shows the plot of the posterior distribution of 0.8. e Pair wise correlation between android fat mass and fat mass/height2 ratio. The first graph above shows the log-likelihood function of the difference between the Android fat mass and fat mass/ht2. The second one shows a uniform prior distribution—this suggests no prior belief. The third graph shows the plot of the posterior distribution of 0.9. f Pair wise correlation between android fat mass and android-gynoid ratio. The first graph above shows the log-likelihood function of the difference between the Android fat mass and android/gynoid ratio. The second shows a uniform prior distribution—this suggests no prior belief. The third graph shows the plot of the posterior distribution of 0.8
There was a significant correlation between arms fat mass and leg fat mass; trunk fat mass and android fat mass; trunk fat mass and fat mass/ht2; trunk fat mass and android-gynoid ratio; android fat mass and fat mass/ht2; android fat mass and android-gynoid ratio.
Multivariate analysis
To determine as to which DEXA indices were interdependent, a multivariate analysis (MANOVA test) was done, which revealed that there was a significant relation between trunk fat mass and (1) android % fat, (2) gynoid fat mass, (3) android-gynoid ratio, (4) fat mass/ht2. There was no statistically significant relation between trunk fat mass to arm or leg fat mass Table 2.
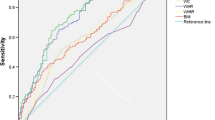
An area under the curve (ROC curve) of android fat % to predict the presence or absence of PCOS is shown in Fig. 2. There was a high ARC value (0.937). Coordinates of the curve revealed that the use of android fat mass %age of > 36.6% has 96.6% sensitivity and 85.2% specificity for independently diagnosing PCOS.

ROC curve for predictability of PCOS by android fat%
An area under the curve (ROC curve) of the android/gynoid ratio to independently predict the presence or absence of PCOS is shown in Fig. 3. There was a high ARC value (0.893). The coordinates of the curve revealed that the use of the android/gynoid ratio for independently diagnosing PCOS with an android/gynoid ratio of > 0.89 has 100% sensitivity and 85.2% specificity.

ROC curve for predictability of PCOS by android/gynoid ratio
Discussion
Our study used DEXA scans to examine the body composition of patients with PCOS in comparison with a control group of healthy patients.
The BMI of our cases and controls were comparable. This is important as most of the prior work done in PCOS patients has been skewed towards choosing patients with increased BMI. Using anthropometric indices like waist circumference, and waist-hip ratio can only serve as a surrogate for fat distribution [11]. The use of DEXA to determine body fat composition and distribution is accurate and less time-consuming as compared to other imaging modalities like MRI [12]. Besides, the DEXA scan is more reproducible and cheaper.
Previous studies have proven by using dual-energy X-ray absorptiometry that women with PCOS have a high prevalence of central fat accumulation compared to BMI-matched control [13].
Arms fat mass, arms fat %, trunk fat mass and fat %, android fat mass, android total mass, android-gynoid ratio, fat mass index, total body % fat, and trunk/limb fat mass ratio were found to be raised in our cases as compared to controls.
In our study, there was preferential fat distribution in the trunk in females with PCOS as compared to controls (58.5% vs 49.3% of total fat mass; p value < 0.0001), a finding that has been seen in other studies as well [14]. Fat mass index (FMI; kg/m2] = fat mass (kg)/height (m)2, android-gynoid ratio, and total body fat %age were found to be raised in our cases. Previous studies have proven that these DEXA-derived fat indices are significantly raised in PCOS cases and correlate with anthropometric indices [15]. Valuation of these fat indices has been reproduced in previous studies as well [16].
In our multivariate analysis, we found that there was a significant relation between trunk fat mass and (1) android % fat, (2) gynoid fat mass, (3) android-gynoid ratio, (4) fat mass/ht2.
We analyzed the ROC curve of these significant variables to define the cut-off for independently predicting PCOS phenotype in our cohort. Such an attempt has also been made in prior studies [15]. Defining cut-offs might help in evaluating and following these patients. The android-gynoid ratio was a strong predictor of PCOS diagnosis in our cohort (ARC of 0.89). Aziz M et al. found that the android-gynoid ratio is a strong predictor of cardiovascular risk in PCOS cases [17].
Using DEXA to measure adipose tissue has some disadvantages (no difference between types of adipose tissues, at low levels of visceral fat it can be underestimated while at high levels it can overestimate fat percentage) [18, 19].
In conclusion, DEXA-derived adipose tissue parameters can be used to determine cut-offs in diagnosing PCOS with reasonable success and should be widely used in basic patient assessment. It can help to delineate PCOS patients who need diet and lifestyle modification. However, more studies on the accuracy and cut-offs of DEXA-derived measures in different ethnic and age groups of PCOS women are still needed.
Summary
The present case–control study illustrates a few important points:
-
1.In PCOS patients, there was increased deposition of fat around the trunk and upper limbs in the android pattern with an increased android-gynoid ratio as compared to controls.
-
2.Trunk fat percentage and android-gynoid ratio can independently predict the presence or absence of PCOS with high sensitivity and specificity with predictable cut-offs.
-
3.Though the mean BMI of PCOS cases was more than controls it was statistically insignificant.
In conclusion, the study demonstrates that there is a central pattern of fat distribution in patients with PCOS while the overall fat might not be increased which is well analyzed by DEXA. DEXA is a feasible, affordable, reliable, and safe modality (radiation exposure is the same as that of natural background levels of radiation). Hence, we suggest its use in the initial diagnostic workup and follow-up of PCOS patients for their body fat distribution and content.
Study limitations
The study may have had a few limitations the sample size was not adequate to notice differences between obese and lean PCOS patients.
-
1.
The sample size was not large enough to determine age-wise trends in each subgroup.
-
2.
Referral bias of physicians to refer obese PCOS patients more than lean PCOS patients may have skewed the results.
Availability of data and materials
Not applicable.
Abbreviations
- PCOS:
-
Polycystic ovary syndrome
- DEXA:
-
Dual-energy X-ray absorptiometry
- BMI:
-
Body mass index
References
Witchel SF, Oberfield SE, Peña AS (2019) Polycystic ovary syndrome: pathophysiology, presentation, and treatment with emphasis on adolescent girls. Journal of the Endocrine Society 3(8):1545–1573. https://doi.org/10.1210/js.2019-0007
Baptiste CG, Battista MC, Trottier A, Baillargeon JP (2010) Insulin and hyperandrogenism in women with polycystic ovary syndrome. J Steroid Biochem Mol Biol 122(1–3):42–52. https://doi.org/10.1016/j.jsbmb.2009.12.01
Lim SS, Davies MJ, Norman RJ, Moran LJ (2012) Moran, Overweight, obesity and central obesity in women with polycystic ovary syndrome: a systematic review and meta-analysis. Human Reprod Update. 18(6):618–637. https://doi.org/10.1093/humupd/dms030
Forslund M, Landin-Wilhelmsen K, Trimpou P, Schmidt J, Brännström M, Dahlgren E (2020) Type 2 diabetes mellitus in women with polycystic ovary syndrome during a 24-year period: importance of obesity and abdominal fat distribution. Human reproduction open 2020(1):hoz042. https://doi.org/10.1093/hropen/hoz04
Lin K, Sun X, Wang X, Wang H, Chen X (2021) Circulating adipokine levels in nonobese women with polycystic ovary syndrome and in nonobese control women: a systematic review and meta-analysis. Front Endocrinol 11:537809. https://doi.org/10.3389/fendo.2020.53780
Glickman SG, Marn CS, Supiano MA, Dengel DR (2004) Validity and reliability of dual-energy X-ray absorptiometry for the assessment of abdominal adiposity. J Appl Physiol (1985). 97(2):509–14. https://doi.org/10.1152/japplphysiol.01234.2003. (Epub 2004 Apr 9. PMID: 15075304.)
Zhu S, Li Z, Hu C, Sun F, Wang C, Yuan H, Li Y (2021) Imaging-based body fat distribution in polycystic ovary syndrome: a systematic review and meta-analysis. Front Endocrinol 12:697223. https://doi.org/10.3389/fendo.2021.69722
Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group (2004) Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 81(1):19–25. https://doi.org/10.1016/j.fertnstert.2003.10.004. (PMID: 14711538)
Aswini R, Jayapalan S (2017) Modified Ferriman-Gallwey Score in hirsutism and its association with metabolic syndrome. International journal of trichology 9(1):7–13. https://doi.org/10.4103/ijt.ijt_93_1
Schoeller et al (2005) QDR 4500A dual-energy X-ray absoptiometer underestimates fat mass in comparison with criterion methods in adults. Am J Clin Nutr 81:1018–1025
De Silva K, Demmer RT, Jönsson D, Mousa A, Teede H, Forbes A et al (2022) Causality of anthropometric markers associated with polycystic ovarian syndrome: Findings of a Mendelian randomization study. PLoS ONE 17(6):e0269191. https://doi.org/10.1371/journal.pone.0269191
Frossing S, Nylander MC, Chabanova E (2018) Quantification of visceral adipose tissue in polycystic ovary syndrome: dual-energy X-ray absorptiometry versus magnetic resonance imaging. Acta Radiol. 59(1):13–17. https://doi.org/10.1177/0284185117711475
Douchi T, Ijuin H, Nakamura S, Oki T, Yamamoto S, Nagata Y (1995) Body fat distribution in women with polycystic ovary syndrome. Obstet Gynecol 86:516–519
Alyan II, El-Dein OS, Melika ASM (2018) Validity of dual-energy X-ray absorptiometry scan in evaluation of trunk fat in non-obese patients with polycystic ovary syndrome. J Med Sci Res 1:86–89
Kałużna M, Czlapka-Matyasik M, Bykowska-Derda A (2021) Indirect predictors of visceral adipose tissue in women with polycystic ovary syndrome: A Comparison of Methods. Nutrients. 13(8):2494. https://doi.org/10.3390/nu13082494
Mokhort T, Savchenko A (2014) Valuation of fat tissue distribution in young women with polycystic ovarian syndrome. Endocrine Abstracts 35:656. https://doi.org/10.1530/endoabs.35.P656
Aziz M, Sidelmann JJ, Faber J, Wissing MLM, Naver KV, Mikkelsen AL et al (2015) Polycystic ovarysyndrome: cardiovascular risk factors according to specific phenotypes. Acta ObstetGynecol Scand. 94:1082–1089
Rotterdam E-A-S (2003) consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004(81):19–25
Ching YK, Chin YS, Appukutty, Gan WY, Ramanchadran V, Chan YM (2018) Prevalence of metabolic syndrome and its associated factors among vegetarians in Malaysia. Int J Environ Res Public Health 15:2031
Acknowledgements
No special acknowledgements from any of the authors.
Funding
The authors did not have any grant/support for the research.
Author information
Authors and Affiliations
Contributions
Study concept and design: S.B., and M.J.; analysis and interpretation of data: S.B., and M.R.; drafting of the manuscript: M.R., S.B., and M.J.; critical revision of the manuscript for important intellectual content: S.B., S.Q., and F.A.; statistical analysis: S.B. and M.R. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved under the ethical approval code of 126/GMC/IEC/ICMR. Informed consent was taken from all research participants and was properly obtained as noted in ethics committee stipulations.
Consent for publication
The consent for publication was properly obtained from all authors.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Birjees, S., Jehangir, M., Rasool, M.V. et al. Pattern of body fat distribution in patients of PCOS using DEXA-based indices. Middle East Fertil Soc J 29, 14 (2024). https://doi.org/10.1186/s43043-024-00175-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43043-024-00175-9