
Abstract
Background
Functional somatic syndromes (FSSs), defined as chronic physical symptoms with no identifiable organic cause, may impact results after hip and knee arthroplasty. The purpose of this study was to perform a systematic review assessing the relationship between FSSs and clinical outcomes after primary total hip arthroplasty (THA), total knee arthroplasty (TKA), and unicompartmental knee arthroplasty (UKA).
Methods
The PubMed and Web of Science databases were queried from January 1955 through December 2021 for studies investigating the impact of at least one FSS (fibromyalgia, irritable bowel syndrome (IBS), chronic headaches, and chronic low back pain) on outcomes after primary THA/TKA/UKA. Outcomes of interest included patient-reported outcome measures (PROMs), postoperative opioid use, complications, revisions, and costs of care.
Results
There were twenty-eight studies, including 768,909 patients, of which 378,384 had an FSS. Five studies reported preoperative PROMs prior to THA/TKA, all of which showed worse PROMs among patients with at least 1 FSS diagnosis. Thirteen studies reported postoperative PROMs after THA/TKA, all of which demonstrated worse PROMs among patients with at least 1 FSS diagnosis. Patients with FSS diagnoses were more likely to continue using opioids at 3, 6, and 12 months following TKA, THA, and UKA. Medical and surgical complications, as well as revision rates, were higher among patients with FSSs.
Conclusion
Patients with FSSs have inferior PROMs and are at increased risk for prolonged postoperative opioid use, medical and surgical complications, and revision after hip and knee arthroplasty. Improved understanding of the factors influencing the success of hip and knee arthroplasty is critical. Future studies should address the biopsychosocial determinants of health that can impact outcomes after total joint arthroplasty.
Similar content being viewed by others


Introduction
The volume of total joint arthroplasty (TJA) procedures performed in the USA continues to rise on an annual basis [1, 2]. Projections indicate that total hip arthroplasty (THA) and total knee arthroplasty (TKA) volume will increase up to 145% and 147%, respectively, over the next decade [2]. Between 1.9 and 2.6 million TJA procedures are expected to be performed in the year 2030 [2]. Total joint arthroplasty consistently improves patient quality of life with excellent overall results and low complication rates [3,4,5,6,7,8]. Despite their generally high rates of success, up to 7% and 20% of patients remain dissatisfied following THA and TKA, respectively [9, 10]. Various patient-specific factors, including social and demographic characteristics, medical comorbidities, and mental health disorders, have been shown to influence outcomes following TJA [11,12,13,14,15].
Functional somatic syndromes (FSS) have been defined as “several related syndromes that are characterized more by symptoms, suffering, and disability than by disease-specific, demonstrable abnormalities of structure or function” [16]. Examples of FSSs include fibromyalgia, irritable bowel syndrome, chronic headaches, chronic fatigue syndrome, and chronic low-back pain [16,17,18,19,20,21]. Given the interrelatedness of these conditions with high rates of co-occurrence and overlap in definitions, prior authors have argued that FSSs should be considered as a single condition rather than multiple disorders [21]. FSSs have received increasing attention within the medical communities as they can result in significant disability, psychological distress in patients, and disproportionate use of health care resources [21,22,23,24]. FSSs have been associated with poor outcomes and higher hospitalization costs following shoulder arthroplasty [25]. However, the relationship between FSSs and outcomes following total joint arthroplasty is not clear and has not been systematically reviewed.
With an increased emphasis on patient-reported outcomes, an enhanced understanding of the factors influencing success following TJA is imperative. The primary purpose of this systematic review was to assess the relationship between functional somatic syndromes and patient-reported outcome measures (PROMs) after primary hip and knee arthroplasty. Secondary outcomes included postoperative opioid consumption, postoperative complications, revision or re-operation, and costs of care.
Materials and methods
This systematic review was conducted and reported in adherence to the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement.
Search strategy
Relevant randomized control trials (RCTs) and retrospective or prospective cohort studies that examined the relationship between at least one FSS and orthopedic clinical outcomes following hip and/or knee arthroplasty were acquired through a comprehensive electronic literature search in two databases (PubMed and Web of Science) from January 1955 to December 2021.
The search strategy was: (“fibromyalgia” OR “functional somatic syndrome” OR “irritable bowel syndrome” OR “chronic headaches” OR “chronic migraines” OR “chronic low back pain”) AND (“hip arthro*” OR “knee arthro*” OR “hip replacement” OR “knee replacement”).
Selection of studies
Two authors (K.M., R.M.) independently screened and assessed the titles, abstracts, and full text of retrieved literature for their eligibility of inclusion and excluded any irrelevant studies and/or duplicates. The two authors also searched the reference lists of identified studies for potential inclusion. Any discrepancies regarding the inclusion and/or exclusion of a given study were to be resolved by discussion among the two authors (K.M., R.M.) and the corresponding author (M.J.S.); however, no discrepancies occurred during the selection process.
Inclusion and exclusion criteria
For this systematic review, articles were included if they (1) were written in English language; (2) involved subjects who underwent primary hip or knee arthroplasty (TKA, UKA, or THA); (3) compared outcomes of patients with pre-treatment diagnosis of at least one of four well-recognized FSSs (fibromyalgia, irritable bowel syndrome, chronic headaches, low back pain) to patients without a pre-treatment diagnosis of any of the aforementioned FSSs. All other studies were excluded if they did not include patients who underwent primary hip or knee arthroplasty, did not include patients with the aforementioned FSSs, and did not compare outcomes of patients with at least one of the included FSSs to patients without a pre-treatment diagnosis were excluded.
Types of outcome measures
The primary outcome measures of this systematic review were baseline and postoperative patient-reported outcome measures of pain and function. Secondary outcome measures included postoperative opioid consumption, postoperative complication rates, revision or reoperation, and costs of care.
Data extraction
Data pertaining to patient demographics (age, sample size, gender), type of procedure, follow-up, loss to follow-up, PROMs, postoperative opioid use, complication rates, revision rates, and hospitalization costs were recorded.
Quality assessment
Evaluation of risk of bias was performed using the Methodological Index for Non-Randomized Studies (MINORS) criteria. The MINORS criteria is a validated tool that contains 12 items, each scoring from 0–2. The maximum score for non-comparative studies is 16 and the maximum score for comparative studies is 24.
Results
Study identification
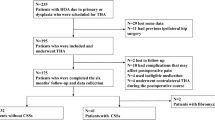
The search identified a total of 517 studies, of which 28 met the inclusion criteria. 12 of these studies were identified through citation searching. A PRISMA flow diagram is shown in Fig. 1.

PRISMA flow diagram depicting study selection for systematic review
Study characteristics
There were 17 retrospective cohort studies [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42], 10 prospective cohort studies [43,44,45,46,47,48,49,50,51,52], and 1 case–control study [53]. The included studies had a mean MINORS score of 16.9 out of 24 for comparative studies and 10 out of 16 for the 1 non-comparative study. Sixteen studies were conducted in the USA, with the remainder conducted in UK, Scotland, Spain, Australia, Canada, and Denmark. Sample sizes ranged from 75 to 305,510 subjects. Eighteen studies were level III evidence and 10 studies were level II evidence. A summary of study characteristics is presented in Table 1.
Study findings
The total number of subjects was 768,909 (Table 2). Twenty studies assessed chronic low back pain, 16 studies assessed fibromyalgia, and 5 assessed chronic migraines/tension headaches. Medical records (14) and American College of Rheumatology (ACR) criteria (2) were used to assess for fibromyalgia. Medical records (12), self-report/questionnaires (7), and a combination of self-report/questionnaires and medical records (1) were used to determine the presence of low back pain. Medical records (5) were used to determine the presence of chronic migraines/tension headaches. Nineteen studies involved outcomes after primary TKA, 5 studies involved outcomes after primary THA, and 3 involved both TKA and THA. One study reported outcomes following unicompartmental knee arthroplasty (UKA). Minimum follow-up lasted for 6 weeks and maximum follow-up for 7 years. Using the 15 studies that reported mean age, the weighted mean age of patients was 62.5 years. 67.7% (n = 520,421) of the subjects were female.
Patient-reported outcome measures
Four studies (n = 2,999) reported baseline PROMs before TKA. All four studies reported no significant difference in preoperative scores when comparing patients with at least one FSS to controls. One study (n = 251) reported baseline PROMs before THA and found that patients with at least one FSS had lower preoperative PROMs as compared to controls.
Thirteen studies (n = 8,478) reported postoperative PROMs (Table 3). PROMs reported included 36-item Short Form Health Survey (SF-36), 12-item Short Form Survey (SF-12), Oxford Knee Scores (OKS), American Knee Society Scores (AKSS), Oxford Hip Score (OHS), Western Ontario and McMaster Universities Score (WOMAC), Visual Analogue Scale (VAS), Forgotten Joint Score-12 (FJS-12), Knee Injury and Osteoarthritis Outcome Score (KOOS), Numeric Rating Scale (NRS), pain, and satisfaction.
Overall, SF-36 Physical Functioning Scores (PFS), SF-12 scores, OKS, AKSS, WOMAC, satisfaction, and NRS for pain were all worse among patients undergoing TKA with at least one FSS in comparison to controls. Two studies reported SF-36 scores following TKA and found that patients with at least one FSS had worse Physical Functioning Scores (PFS) than patients without at least one FSS. Three studies examined SF-12 scores after TKA and reported that patients with at least one FSS had worse scores than controls. Oxford Knee Scores and American Knee Society Scores following TKA were each reported by two studies. In comparison to controls, patients with at least one FSS demonstrated worse outcome measures with both of these scoring systems. Following TKA, patients with at least one FSS showed worse WOMAC scores compared to controls in 4 studies. One study reported KOOS following TKA and found that patients with an FSS diagnosis had worse outcomes. In terms of postoperative satisfaction, 3 studies reported that patients with an FSS diagnosis were significantly less satisfied than controls. In terms of postoperative pain metrics, one study demonstrated that patients with at least one FSS had worse NRS for pain than patients without FSS following TKA.
SF-36 physical functioning scores, SF-12 scores, WOMAC, OHS, and FJS-12 scores were reported following THA. Loth et al. (2017) found that patients with at least one FSS had worse SF-12, OHS, and FJS-12 scores following THA compared to controls [29]. Quintana et al. (2009) reported that patients with an FSS diagnosis had worse SF-36 PFS and WOMAC scores following THA than controls [50].
Opioid use
Eleven studies (n = 348,047) reported postoperative opioid use following TJA. (Fig. 2) Several studies reported postoperative opioid use at many time points. However, we chose representative time points to summarize in Fig. 2. All 11 studies concluded that patients with at least one FSS are at risk for higher opioid use postoperatively. Higher patient ACR fibromyalgia score was associated with greater inpatient opioid consumption following THA and TKA in one study. Patients with FSS diagnoses were more likely to continue using opioids at 3, 6, and 12 months after TKA, THA, and UKA. Chronic back pain and migraine headaches were also shown to be significant risk factors for new chronic opioid use following THA.

Visual representation of post-operative opioid use following total joint arthroplasty among patients with functional somatic syndromes
Complications
Four studies (n = 412,494) reported postoperative complications (Table 4). Moore et al. (2019) showed that patients with fibromyalgia were 1.95 times more likely to develop any medical complication after TKA than controls (OR = 1.95, 95% CI: 1.86–2.04) [31]. In terms of reoperation, patients with fibromyalgia were significantly more likely to undergo lysis of adhesions for arthrofibrosis within one year after TKA in one study. In the same study, patients with fibromyalgia were more likely to undergo revision TKA within 2 years of index TKA than controls. D’Appuzo et al. (2012) reported an overall revision rate of 6% among patients with fibromyalgia who underwent primary TKA with a mean follow-up of 7 years [40]. Sodhi et al. (2019) showed that patients with fibromyalgia had significantly increased odds of surgical complications following TKA, including bearing wear, periprosthetic osteolysis, mechanical loosening, infection, dislocation, and revision of tibial insert [34].
Costs
One study (n = 305,510) reported surgical and medical costs among patients who underwent TKA. While patients with fibromyalgia had lower readmission costs than patients without, they incurred greater management costs for medical and surgical complications following total knee arthroplasty in comparison to patients without fibromyalgia, thus resulting in net losses.
Discussion
Functional somatic syndromes (FSS) are a group of interrelated conditions characterized by the presence of chronic symptoms that cannot be attributed to a known somatic disease or disorder [16, 17]. FSSs are common and have been reported to account for as high as 35% of primary care visits [54, 55]. The etiology of FSSs is not clear; however, they are considered to arise via a complex interaction among biological and psychosocial factors [16, 56]. Common examples of FSSs are fibromyalgia, irritable bowel syndrome, chronic headaches, chronic fatigue syndrome, and chronic low back pain [16,17,18,19,20,21]. However, prior authors have proposed that FSSs be considered collectively as “variants of a common biopsychosocial process”, given their high rates of co-occurrence and overlap of symptoms [16,17,18,19,20,21]. Moreover, there is evidence to support that FSSs should be considered on a continuum, as patients with more functional symptoms demonstrate increasing disease severity states [29, 57, 58]. Prior studies have reported the role of individual conditions and isolated functional symptoms in outcomes following total joint arthroplasty [36, 53]. However, the relationship between FSS as a single entity and results following TJA has not been studied, highlighting the importance of our systematic review.
The primary focus of this systematic review was to determine the relationship between FSSs and patient-reported outcome measures following primary hip and knee arthroplasty. Overall, our results showed that the presence of at least one FSS is associated with worse PROMs among patients undergoing hip or knee arthroplasty. Scores for SF-36 or its abbreviated version (SF-12) were reported by 6 studies for patients after TKA and by 2 studies after THA [29, 36, 43, 45, 46, 50, 53]. All of these studies reported worse scores among patients with an FSS diagnosis in comparison to controls. These metrics are typically utilized to assess a patient’s quality of life and comprised of eight health domains, including limitations in physical and social activities, bodily pain, mental health, fatigue, and general health perceptions [59]. The prevalence of psychological disorders such as depression and anxiety is much higher in patients with FSS than in the general population, which certainly could lead to lower scores on the overall SF-36 and SF-12 metrics [17]. However, Ayers et al. (2013) and Bican et al. (2011) specifically reported SF-36 Physical Functioning Scores (PFS) following TKA and demonstrated worse results among patients with at least one FSS [43, 53]. Quintana et al. (2009) showed similar results for THA [50]. In terms of PROMs specific to the hip and knee, OHS, OKS, AKSS, KOOS, and WOMAC were all included in various studies [29, 36, 45,46,47,48, 50, 52]. Patients with FSS performed worse on each of these metrics in comparison to controls, even when preoperative scores were not significantly different. The relationship between FSS and PROMs has been previously studied in the orthopedic literature with reference to shoulder arthroplasty. Moverman et al. (2021) found that at least one FSS was associated with both worse 2-year postoperative American Shoulder and Elbow Surgeons Shoulder (ASES) and Single Assessment Numerical Evaluation (SANE) scores [25]. Furthermore, this study demonstrated that each additional functional disorder was associated with a stepwise decline in these PROMs. In light of FSS as a continuum, future prospective studies are needed to investigate the impact of an increasing number of functional disorders on outcomes following total hip and knee arthroplasty.
In addition to PROMs, we systematically reviewed the impact of FSSs on postoperative opioid consumption following hip and knee arthroplasty. Increased inpatient opioid consumption has been shown to be strongly associated with an increased risk of chronic postoperative opioid use following TJA [60]. Brummett et al. (2013) reported that higher patient scores on the American College of Rheumatology (ACR) criteria for fibromyalgia were independently associated with increased inpatient postoperative opioid consumption following THA and TKA [44]. FSS diagnoses appear to increase the risk of prolonged postoperative opioid use up to 1 year after TJA. Bedard et al. (2017) found that both fibromyalgia and chronic back pain significantly increased the risk of continued opioid use at 6 and 12 months following total hip arthroplasty [26]. Similar results were reported following total knee and unicompartmental knee arthroplasty [27, 35]. Multiple additional studies supported these findings, with fibromyalgia, chronic back pain, and chronic headaches increasing the risk of opioid prescription refills and protracted opioid use following TJA [28, 32, 37, 41, 49, 51]. Preoperative opioid use has been shown to increase the risk of chronic postoperative opioid use following hip and knee arthroplasty [49, 60,61,62,63,64,65]. A study by Agger et al. (2018) reported that prescription opioids are used by 26% of patients with multiple functional somatic syndromes at baseline [66]. However, FSSs might also increase the risk of new persistent opioid use after TJA among patients who were not previously opioid users [42]. Given the ongoing opioid epidemic within the USA, an improved recognition of the risk factors for prolonged opioid use following TJA is crucial. Preoperative patient education and counseling regarding postoperative pain control expectations among patients with FSSs undergoing TJA is critical. Furthermore, detailed multimodal pain control plans (potentially including regional anesthesia and non-opioid analgesics) should be formulated for these patients.
Medical complications following total joint arthroplasty increase patient morbidity and can lead to higher episode-of-care costs [67]. Moore et al. (2019) performed a retrospective review of the PearlDiver database and found that, compared to propensity score matched controls, patients with fibromyalgia had increased odds of developing any medical complication after TKA [30]. Our systematic review also demonstrates that FSSs are a risk factor for surgical complications and revision following primary hip and knee arthroplasty. In an analysis of both the Humana and Medicare databases, Cregar et al. (2021) showed that fibromyalgia was associated with an increased risk of undergoing lysis of adhesions for arthrofibrosis within 1 year of primary TKA as well as revision TKA within 2 years [39]. D’Appuzo et al. (2012) reported an overall revision rate of 6% among patients with fibromyalgia who underwent primary TKA with a mean follow-up of 7 years [40]. This is consistent with previously published registry data reporting overall 10-year TKA revision rates between 4.9 and 7.8% [68]. However, Sodhi et al. (2019) found that patients with fibromyalgia had a significantly increased risk of surgical complications following TKA such as bearing wear, periprosthetic osteolysis, mechanical loosening, infection, dislocation, and tibial insert revision [34].
Functional somatic syndromes are associated with high healthcare utilization rates and total annual healthcare costs [69,70,71,72,73]. Patients with FSSs have been shown to incur higher hospitalization costs following shoulder arthroplasty [25]. In a retrospective database study by Moore et al. (2019), patients with fibromyalgia incurred greater management costs for medical and surgical complications following total knee arthroplasty in comparison to patients without fibromyalgia [31]. Within bundled payment reimbursement models, healthcare providers are responsible for all costs incurred during an episode of care. Given the evidence that FSSs can increase episode-of-care costs, perhaps adjusted target prices are needed for these patients when undergoing total hip and knee arthroplasty.
Inferior outcomes following TJA among patients with FSSs may be circumvented by managing these conditions preoperatively. Literature has shown that using a biopsychosocial, patient-involving approach is an effective management strategy [74]. In addition, FSSs can be managed using a multi-modal approach, including diagnosis explanation, guided self-help, cognitive behavioral therapy, and specialist referral [75].
We recognize limitations to our analysis. Due to the nature of systematic reviews, studies investigating outcomes after hip and knee arthroplasty among patients with FSSs that satisfy our inclusion criteria could have been omitted. However, our search was performed systematically using two separate databases. Furthermore, concern for publication bias exists with any systematic review. In addition, the majority of included studies were cohort studies which are prone to selection bias, confounding factors, and information bias. Further, based on the MINORS criteria, the included studies were not of high quality. We chose to include four of the most well-recognized functional somatic syndromes in our search, but did not search for other more obscure FSSs such as chronic fatigue syndrome or multiple chemical sensitivity. These four FSSs were selected based on the substantial literature regarding these conditions. However, other search terms may have captured additional studies in our review. In addition, follow-up time of the included studies ranged from 6 weeks to 7 years, with most studies having a follow-up time of 1 year or less. Thus, further studies should focus on the outcomes of patients with FSSs following joint arthroplasty after mid- or long-term follow-up.
Conclusion
In conclusion, the present systematic review demonstrates that patients with FSSs have inferior PROMs and are at increased risk for prolonged postoperative opioid use, medical and surgical complications, and revision after hip and knee arthroplasty. Future studies should address the biopsychosocial determinants of health that can impact outcomes after total joint arthroplasty.
Availability of data and materials
The data analyzed is available in the publications referenced studies.
Abbreviations
- TJA:
-
Total joint arthroplasty
- THA:
-
Total hip arthroplasty
- TKA:
-
Total knee arthroplasty
- FSSs:
-
Functional somatic syndromes
- PROMs:
-
Patient-reported outcome measures
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RCTs:
-
Randomized controlled trials
- MINORS:
-
Methodological Index for Non-Randomized Studies
- ACR:
-
American College of Rheumatology
- UKA:
-
Unicompartmental knee arthroplasty
- SF-36:
-
36-Item Short Form Health Survey
- SF-12:
-
12-Item Short Form Survey
- OKS:
-
Oxford Knee Scores,
- AKSS:
-
American Knee Society Scores
- OHS:
-
Oxford Hip Score
- WOMAC:
-
Western Ontario and McMaster Universities score
- VAS:
-
Visual analogue scale
- FJS-12:
-
Forgotten Joint Score-12
- KOOS:
-
Knee Injury and Osteoarthritis Outcome Score
- NRS:
-
Numeric Rating Scale
- PFS:
-
Physical Functioning Scores
- ASES:
-
American Shoulder and Elbow Surgeons Shoulder
- SANE:
-
Single Assessment Numerical Evaluation
References
Maradit Kremers H, Larson DR, Crowson CS, Kremers WK, Washington RE, Steiner CA, et al. Prevalence of Total Hip and Knee Replacement in the United States. J Bone Joint Surg Am Vol. 2015;97(17):1386–97.
Sloan M, Premkumar A, Sheth NP. Projected volume of primary total joint arthroplasty in the U.S., 2014 to 2030. J Bone Joint Surg. 2018;100(17):1455–60.
Wiklund I, Romanus B. A comparison of quality of life before and after arthroplasty in patients who had arthrosis of the hip joint. J Bone Joint Surg. 1991;73(5):765–9.
Dailiana ZH, Papakostidou I, Varitimidis S, Liaropoulos L, Zintzaras E, Karachalios T, et al. Patient-reported quality of life after primary major joint arthroplasty: a prospective comparison of hip and knee arthroplasty. BMC Musculoskelet Disord. 2015;16(1):366.
Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007;370(9597):1508–19.
Evans JT, Walker RW, Evans JP, Blom AW, Sayers A, Whitehouse MR. How long does a knee replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. The Lancet. 2019;393(10172):655–63.
Evans JT, Evans JP, Walker RW, Blom AW, Whitehouse MR, Sayers A. How long does a hip replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. The Lancet. 2019;393(10172):647–54.
Carr AJ, Robertsson O, Graves S, Price AJ, Arden NK, Judge A, et al. Knee replacement. Lancet. 2012;379(9823):1331–40.
Scott CEH, Howie CR, MacDonald D, Biant LC. Predicting dissatisfaction following total knee replacement: a Prospective Study of 1217 Patients. J Bone Joint Surg Br. 2010;92-B(9):1253–8.
Anakwe RE, Jenkins PJ, Moran M. Predicting dissatisfaction after total hip arthroplasty: a study of 850 patients. J Arthroplasty. 2011;26(2):209–13.
Barrack RL, Ruh EL, Chen J, Lombardi AV, Berend KR, Parvizi J, et al. Impact of socioeconomic factors on outcome of total knee arthroplasty. Clin Orthop Relat Res. 2014;472(1):86–97.
D’Apuzzo MR, Novicoff WM, Browne JA. The John Insall award: morbid obesity independently impacts complications, mortality, and resource use after TKA. Clin Orthop Relat Res. 2015;473(1):57–63.
Xu J, Twiggs J, Parker D, Negus J. The association between anxiety, depression, and locus of control with patient outcomes following total knee arthroplasty. J Arthroplasty. 2020;35(3):720–4.
Blackburn J, Qureshi A, Amirfeyz R, Bannister G. Does preoperative anxiety and depression predict satisfaction after total knee replacement? Knee. 2012;19(5):522–4.
Pan X, Wang J, Lin Z, Dai W, Shi Z. Depression and anxiety are risk factors for postoperative pain-related symptoms and complications in patients undergoing primary total knee arthroplasty in the United States. J Arthroplasty. 2019;34(10):2337–46.
Barsky AJ. Functional somatic syndromes. Ann Intern Med. 1999;130(11):910.
Donnachie E, Schneider A, Enck P. Comorbidities of patients with functional somatic syndromes before, during and after first diagnosis: a population-based study using Bavarian routine data. Sci Rep. 2020;10(1):9810.
Kanaan RAA, Lepine JP, Wessely SC. The association or otherwise of the functional somatic syndromes. Psychosom Med. 2007;69(9):855–9.
Mayou R, Farmer A. ABC of psychological medicine: functional somatic symptoms and syndromes. BMJ. 2002;325(7358):265–8.
Polatin PB, Kinnedy RK, Gatchel RJ, Lillo E, Mayer TG. Psychiatric illness and chronic low-back pain: the mind and the spine—which goes first? Spine. 1993;18(1):66–71.
Wessely S, Nimnuan C, Sharpe M. Functional somatic syndromes: one or many? Lancet. 1999;354(9182):936–9.
Berger A, Dukes E, Martin S, Edelsberg J, Oster G. Characteristics and healthcare costs of patients with fibromyalgia syndrome: characteristics and costs of patients with fibromyalgia. Int J Clin Pract. 2007;61(9):1498–508.
Lee AD, Spiegel BM, Hays RD, Melmed GY, Bolus R, Khanna D, et al. Gastrointestinal symptom severity in irritable bowel syndrome, inflammatory bowel disease and the general population. Neurogastroenterol Motil. 2017;29(5):e13003.
Tack J, Stanghellini V, Mearin F, Yiannakou Y, Layer P, et al. Economic burden of moderate to severe irritable bowel syndrome with constipation in six European countries. BMC Gastroenterol. 2019;19(1):69.
Moverman MA, Puzzitiello RN, Pagani NR, Moon AS, Hart PA, Kirsch JM, et al. Functional somatic syndromes are associated with suboptimal outcomes and high cost after shoulder arthroplasty. J Shoulder Elbow Surg. 2022;31(1):48–55.
Bedard NA, Pugely AJ, Dowdle SB, Duchman KR, Glass NA, Callaghan JJ. Opioid use following total hip arthroplasty: trends and risk factors for prolonged use. J Arthroplasty. 2017;32(12):3675–9.
Bedard NA, Pugely AJ, Westermann RW, Duchman KR, Glass NA, Callaghan JJ. Opioid use after total knee arthroplasty: trends and risk factors for prolonged use. J Arthroplasty. 2017;32(8):2390–4.
Kim SC, Choudhry N, Franklin JM, Bykov K, Eikermann M, Lii J, et al. Patterns and predictors of persistent opioid use following hip or knee arthroplasty. Osteoarthritis Cartilage. 2017;25(9):1399–406.
Loth FL, Giesinger JM, Giesinger K, MacDonald DJ, Simpson AHRW, Howie CR, et al. Impact of comorbidities on outcome after total hip arthroplasty. J Arthroplasty. 2017;32(9):2755–61.
Moore T, Sodhi N, Kalsi A, Vakharia RM, Ehiorobo JO, Anis HK, et al. A nationwide comparative analysis of medical complications in fibromyalgia patients following total knee arthroplasty. Ann Transl Med. 2019;7(4):64.
Moore T, Sodhi N, Cohen-Levy WB, Ehiorobo J, Kalsi A, Anis HK, et al. Surgical and medical costs for fibromyalgia patients undergoing total knee arthroplasty. J Knee Surg. 2019;32(11):1069–74.
Namba RS, Singh A, Paxton EW, Inacio MCS. Patient factors associated with prolonged postoperative opioid use after total knee arthroplasty. J Arthroplasty. 2018;33(8):2449–54.
Skrejborg P, Petersen KK, Kold S, Kappel A, Pedersen C, Østgaard SE, et al. Presurgical comorbidities as risk factors for chronic postsurgical pain following total knee replacement. Clin J Pain. 2019;35(7):577–82.
Sodhi N, Moore T, Vakharia RM, Leung P, Seyler TM, Roche MW, et al. Fibromyalgia increases the risk of surgical complications following total knee arthroplasty: a nationwide database study. J Arthroplasty. 2019;34(9):1953–6.
Bedard NA, DeMik DE, Dowdle SB, Callaghan JJ. Trends and risk factors for prolonged opioid use after unicompartmental knee arthroplasty. Bone Joint J. 2018;100-B(1 Supple A):62–7.
Boyle JK, Anthony IC, Jones BG, Wheelwright EF, Blyth MJG. Influence of low back pain on total knee arthroplasty outcome. Knee. 2014;21(2):410–4.
Cancienne JM, Patel KJ, Browne JA, Werner BC. Narcotic use and total knee arthroplasty. J Arthroplasty. 2018;33(1):113–8.
Clement ND, Bardgett M, Weir D, Holland J, Deehan DJ. Increased symptoms of stiffness 1 year after total knee arthroplasty are associated with a worse functional outcome and lower rate of patient satisfaction. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1196–203.
Cregar WM, Khazi ZM, Lu Y, Forsythe B, Gerlinger TL. Lysis of adhesion for arthrofibrosis after total knee arthroplasty is associated with increased risk of subsequent revision total knee arthroplasty. J Arthroplasty. 2021;36(1):339-344.e1.
D’Apuzzo MR, Cabanela ME, Trousdale RT, Sierra RJ. Primary total knee arthroplasty in patients with fibromyalgia. Orthopedics. 2012;35(2):e175-178.
Hansen CA, Inacio MCS, Pratt NL, Roughead EE, Graves SE. Chronic use of opioids before and after total knee arthroplasty: a retrospective cohort study. J Arthroplasty. 2017;32(3):811-817.e1.
Inacio MCS, Hansen C, Pratt NL, Graves SE, Roughead EE. Risk factors for persistent and new chronic opioid use in patients undergoing total hip arthroplasty: a retrospective cohort study. BMJ Open. 2016;6(4):e010664.
Ayers DC, Li W, Oatis C, Rosal MC, Franklin PD. Patient-reported outcomes after total knee replacement vary on the basis of preoperative coexisting disease in the lumbar spine and other nonoperatively treated joints: the need for a musculoskeletal comorbidity index. J Bone Joint Surg Am. 2013;95(20):1833–7.
Brummett CM, Janda AM, Schueller CM, Tsodikov A, Morris M, Williams DA, et al. Survey criteria for fibromyalgia independently predict increased postoperative opioid consumption after lower-extremity joint arthroplasty: a prospective, observational cohort study. Anesthesiology. 2013;119(6):1434–43.
Clement ND, MacDonald D, Simpson AHRW, Burnett R. Total knee replacement in patients with concomitant back pain results in a worse functional outcome and a lower rate of satisfaction. Bone Joint J. 2013;95-B(12):1632–9.
Collados-Maestre I, Lizaur-Utrilla A, Martinez-Mendez D, Marco-Gomez L, Lopez-Prats FA. Concomitant low back pain impairs outcomes after primary total knee arthroplasty in patients over 65 years: a prospective, matched cohort study. Arch Orthop Trauma Surg. 2016;136(12):1767–71.
Escobar A, Quintana JM, Bilbao A, Azkárate J, Güenaga JI, Arenaza JC, et al. Effect of patient characteristics on reported outcomes after total knee replacement. Rheumatology (Oxford). 2007;46(1):112–9.
Mehta SP, Perruccio AV, Palaganas M, Davis AM. Do women have poorer outcomes following total knee replacement? Osteoarthritis Cartilage. 2015;23(9):1476–82.
Prentice HA, Inacio MCS, Singh A, Namba RS, Paxton EW. Preoperative risk factors for opioid utilization after total hip arthroplasty. J Bone Joint Surg Am. 2019;101(18):1670–8.
Quintana JM, Escobar A, Aguirre U, Lafuente I, Arenaza JC. Predictors of health-related quality-of-life change after total hip arthroplasty. Clin Orthop Relat Res. 2009;467(11):2886–94.
Sheth DS, Ho N, Pio JR, Zill P, Tovar S, Namba RS. Prolonged opioid use after primary total knee and total hip arthroplasty: prospective evaluation of risk factors and psychological profile for depression, pain catastrophizing, and aberrant drug-related behavior. J Arthroplasty. 2020;35(12):3535–44.
Sullivan M, Tanzer M, Stanish W, Fallaha M, Keefe FJ, Simmonds M, et al. Psychological determinants of problematic outcomes following total knee arthroplasty. Pain. 2009;143(1–2):123–9.
Bican O, Jacovides C, Pulido L, Saunders C, Parvizi J. Total knee arthroplasty in patients with fibromyalgia. J Knee Surg. 2011;24(4):265–71.
Peveler R, Kilkenny L, Kinmonth AL. Medically unexplained physical symptoms in primary care: a comparison of selfreport screening questionnaires and clinical opinion. J Psychosom Res. 1997;42(3):245–52.
Arnold IA, de Waal MWM, Eekhof JAH, Assendelft WJJ, Spinhoven P, van Hemert AM. Medically unexplained physical symptoms in primary care: a controlled study on the effectiveness of cognitive-behavioral treatment by the family physician. Psychosomatics. 2009;50(5):515–24.
Potts SG, Bass CM. Psychological morbidity in patients with chest pain and normal or near-normal coronary arteries: a long-term follow-up study. Psychol Med. 1995;25(2):339–47.
Brummett CM, Urquhart AG, Hassett AL, Tsodikov A, Hallstrom BR, Wood NI, et al. Characteristics of fibromyalgia independently predict poorer long-term analgesic outcomes following total knee and hip arthroplasty. Arthritis Rheumatol. 2015;67(5):1386–94.
Gierk B, Kohlmann S, Kroenke K, Spangenberg L, Zenger M, Brähler E, et al. The somatic symptom scale-8 (SSS-8): a brief measure of somatic symptom burden. JAMA Intern Med. 2014;174(3):399–407.
Wee CC, Davis RB, Hamel MB. Comparing the SF-12 and SF-36 health status questionnaires in patients with and without obesity. Health Qual Life Outcomes. 2008;6(1):11.
Ruddell JH, Reid DBC, Shah KN, Shapiro BH, Akelman E, Cohen EM, et al. Larger initial opioid prescriptions following total joint arthroplasty are associated with greater risk of prolonged use. J Bone Joint Surg. 2021;103(2):106–14.
Politzer CS, Kildow BJ, Goltz DE, Green CL, Bolognesi MP, Seyler TM. Trends in opioid utilization before and after total knee arthroplasty. J Arthroplasty. 2018;33(7):S147-S153.e1.
Pryymachenko Y, Wilson RA, Abbott JH, Dowsey MM, Choong PFM. Risk factors for chronic opioid use following hip and knee arthroplasty: evidence from New Zealand population data. J Arthroplasty. 2020;35(11):3099-3107.e14.
Kaidi AC, Lakra A, Jennings EL, Neuwirth AL, Geller JA, Shah RP, et al. Opioid prescription consumption patterns after total joint arthroplasty in chronic opioid users versus opioid naive patients. JAAOS Glob Res Rev. 2020;4(6):e20.00066-11.
Cook DJ, Kaskovich SW, Pirkle SC, Mica MAC, Shi LL, Lee MJ. Benchmarks of duration and magnitude of opioid consumption after total hip and knee arthroplasty: a database analysis of 69,368 patients. J Arthroplasty. 2019;34(4):638-644.e1.
Namba RS, Inacio MCS, Pratt NL, Graves SE, Roughead EE, Paxton EW. Persistent opioid use following total knee arthroplasty: a signal for close surveillance. J Arthroplasty. 2018;33(2):331–6.
Agger JL, Fink PK, Gormsen LK, Jensen JS, Schröder A. The use of prescription medication in 239 patients with multiple functional somatic syndromes. Gen Hosp Psychiatry. 2018;51:96–105.
Pulido L, Parvizi J, Macgibeny M, Sharkey PF, Purtill JJ, Rothman RH, et al. In hospital complications after total joint arthroplasty. J Arthroplasty. 2008;23(6):139–45.
Pabinger C, Berghold A, Boehler N, Labek G. Revision rates after knee replacement. Cumulative results from worldwide clinical studies versus joint registers. Osteoarthritis Cartilage. 2013;21(2):263–8.
Sicras-Mainar A, Rejas J, Navarro R, Blanca M, Morcillo A, Larios R, et al. Treating patients with fibromyalgia in primary care settings under routine medical practice: a claim database cost and burden of illness study. Arthritis Res Ther. 2009;11(2):R54.
Hiller W, Fichter MM, Rief W. A controlled treatment study of somatoform disorders including analysis of healthcare utilization and cost-effectiveness. J Psychosom Res. 2003;54(4):369–80.
Reid S, Wessely S, Crayford T, Hotopf M. Frequent attenders with medically unexplained symptoms: service use and costs in secondary care. Br J Psychiatry. 2002;180(3):248–53.
Saunders NR, Gandhi S, Chen S, Vigod S, Fung K, De Souza C, et al. Health care use and costs of children, adolescents, and young adults with somatic symptom and related disorders. JAMA Netw Open. 2020;3(7):e2011295.
Wortman MSH, Lokkerbol J, van der Wouden JC, Visser B, van der Horst HE, olde Hartman TC. Cost-effectiveness of interventions for medically unexplained symptoms: a systematic review. Lhachimi SK, editor. PLoS ONE. 2018;13(10):e0205278.
Henningsen P, Zipfel S, Sattel H, Creed F. Management of functional somatic syndromes and bodily distress. Psychother Psychosom. 2018;87(1):12–31.
Husain M, Chalder T. Medically unexplained symptoms: assessment and management. Clin Med (Lond). 2021;21(1):13–8.
Acknowledgements
Not applicable.
Funding
No funds were received in support of this work.
Author information
Authors and Affiliations
Contributions
R.M. performed data collection, interpreted data, and drafted the manuscript, and provided revisions to the manuscript. K.M. performed data collection, interpreted data, drafted the manuscript, and provided revisions to the manuscript. N.R.P. conceived the ideas of the manuscript, interpreted data, drafted the manuscript, and provided revisions to the manuscript. M.A.M. conceived the ideas of the manuscript and provided revisions to the manuscript. R.N.P. conceived the ideas of the manuscript and provided revisions to the manuscript. M.E.M. provided revisions to the manuscript. M.J.S. conceived the ideas of the manuscript and provided revisions to the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors declare no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Masood, R., Mandalia, K., Pagani, N.R. et al. Functional somatic syndromes are associated with inferior outcomes and increased complications after hip and knee arthroplasty: a systematic review. Arthroplasty 6, 2 (2024). https://doi.org/10.1186/s42836-023-00223-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42836-023-00223-1