
Abstract
Background
Total knee arthroplasty (TKA) is one of the most performed orthopedic procedures worldwide. While excellent efficacy has been reported, about 20% of patients are not satisfied with the result. A potential cause is the problematic reproduction of knee kinematics. This systematic review examines gait analysis studies in primary medial pivot (MP) and posterior stabilized (PS) TKAs to investigate the differences between the two prosthesis designs.
Methods
A systematic review was conducted by following PRISMA guidelines. Five databases (PubMed, Medline, Embase, Scopus and the Cochrane Database of Systematic Reviews) were analyzed, and eligible articles were evaluated in terms of the levels of evidence. The methodological quality of the articles was assessed by using the MINORS scoring. This review was registered in PROSPERO.
Results
Nine studies were included. Gait analysis was performed in 197 MP TKA and 192 PS TKA patients. PS TKA cases showed (P < 0.05) a significantly higher peak of knee flexion angle during the swing phase, greater knee flexion angle at toe-off, an increased knee adduction angle, higher knee flexion and extension moment, increased anterior femoral roll during knee flexion and anterior translation on medial and lateral condyle during knee flexion compared to MP TKA. MP TKA showed statistically significant (P < 0.05) higher knee rotational moment and greater tibiofemoral external rotation motion during knee flexion than PS TKA. No statistically significant difference (P > 0.05) was reported regarding gait spatial–temporal parameters. The Forgotten Joint Score (FJS) and Western Ontario and McMaster Universities Comparison in terms of Arthritis Index (WOMAC) score (mean stiffness) showed that MP TKA yielded significantly better results than PS TKA.
Conclusions
This systematic review revealed significant kinematic and kinetic differences between MP and PS TKA at all gait analysis phases. Furthermore, the considerable difference between TKA design and the kinematics of healthy knee were highlighted in this study.
Level of evidence
III.
Similar content being viewed by others


Background
Total knee arthroplasty (TKA) is a reliable and cost-effective surgical procedure for treating symptomatic end-stage knee osteoarthritis [1]. Currently, more than 500,000 TKAs are performed annually in the United States, with a projected increase of 670% by 2030 [2, 3]. De Steiger et al., in their analysis of national registers, have reported an excellent long-term survival of implants, with a revision rate of 5.2% after ten years and a rate of 7.3% after 15 years [4].
Despite the low reoperation rate, approximately 20% of patients remain dissatisfied after TKA, and this percentage has remained unchanged over the past decades despite advances in surgical techniques and implant design [5,6,7]. The failure to reproduce the physiological knee kinematics after TKA is often reported as a major cause of patient dissatisfaction [8, 9]. In recent years, various prosthetic designs have been developed to improve clinical outcomes and patient satisfaction: many of those designs were presented by manufacturers with a special characteristic of reproducing more natural knee kinematics [10, 11]. According to the latest report by the Australian Arthroplasty Registry, implants characterized by lower levels of constraints (cruciate or bicruciate retaining) are currently most frequently used in TKAs. The use of posterior stabilized (PS) designs is decreasing while the use of medial congruent TKAs is steadily increasing worldwide [4].
Insall and Burstein first introduced a PS TKA model to overcome limitations in the range of motion (ROM) and the anterior femoral sliding from knee flexion to extension, typical of total condylar knee implants [12]. The most important feature of the PS TKA design was the post-cam mechanism, providing a constraint to limit the anterior translation of the femur through the tibia (“paradoxical motion”), ensuring femoral rollback with progressive knee flexion [12, 13]. The PS TKA design has the theoretical advantage of allowing for easier balancing of severe coronal deformities, reducing polyethylene wear, and improving maximum flexion compared to total condylar knee prosthesis. Nevertheless, PS TKAs have potential drawbacks, including increased tibial liner wear or breakage, an increase in the rate of postoperative anterior knee pain, and the additional bone resection necessary to accommodate the femoral box [14, 15].
Medial pivot (MP) TKA designs aim to reproduce the natural knee kinematics, where the medial femoral condyle is congruent on the concave medial tibial plateau, acting as a ball and socket mechanism. In contrast, on a flat tibial surface, the lateral femoral condyle shifts anteriorly first and posteriorly later during knee extension and flexion movements [10, 11]. Developed through Freeman and Pisnkerova's kinematic studies [16, 17] and first implanted in 1994, MP designs tend to achieve more physiological knee kinematics, better coronal and sagittal stability, and reduced polyethylene wear [18,19,20,21,22,23].
This systematic review examines comparative gait analysis studies in the primary medial pivot and posterior stabilized TKA to investigate the kinematic and kinetic differences between these two prosthetic designs on (1) the sagittal plane, (2) the coronal plane, (3) in relative tibiofemoral motion, (4) in the spatial–temporal parameters, and finally in the (5) clinical scores.
Materials and methods
This systematic review of the literature was performed in accordance with the Preferred Reporting Items for systematic reviews and meta-analyses (PRISMA) guidelines [20, 24,25,26]. The literature search was conducted by three independent reviewers (G.C., F.B., and F.G.) to search for comparative gait analyses of MP vs. PS TKA studies. In case of discrepancies, a fourth author (LS) was involved to resolve any doubts or disagreements.
Search strategy and study screening
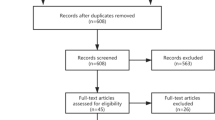
The literature search was conducted in the US National Library of Medicine (PubMed/Medline), Embase, Scopus and the Cochrane Database of Systematic Reviews by using the following MeSH terms without limitation up to August 2022: “medial pivot”, “medial congruent”, “posterior stabilised”, “MP”, “PS”, “kinetic”, “kinematic”, “fluoroscopy”, “gait analysis”, “in vivo”, “knee arthroplasty”. With the above MeSH terms, the initial search produced 433 studies. After removal of duplicates, 297 studies remained for analysis. After title and abstract analysis, the full text of 17 potentially included studies was assessed for eligibility against inclusion and exclusion criteria. Nine studies that directly compared the results of gait analysis of MP vs. PS TKA were included in the final analysis [27,28,29,30,31,32,33,34,35]. Supplementary relevant articles were searched through the reference list of included studies. The PRISMA flow chart to report the study selection is shown in Fig. 1.

Preferred reporting items for systematic review and meta-analysis (PRISMA) flow diagram of studies included in the systematic review
Inclusion and exclusion criteria
Inclusion criteria for the reviewed studies were articles published until September 2022, with full text available, written in English, that reported knee kinematic data in the frontal or sagittal planes or relative tibiofemoral movement or gait parameters, RCTs, prospective and retrospective studies with Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence (LoE) 1 to 4 [36]. Non-comparative studies, non-in vivo studies, editorials, instructional course lectures or abstracts for international meetings were excluded from the search. We also excluded studies with LoE 5 for quality control.
Evaluation of methodological quality
The level of evidence analysis was determined by using the Oxford Centre for Evidence-Based Medicine Levels of Evidence [36]. Additional assessment of the studies’ quality was conducted by three authors (G.C., F.B., and F.G.) according to the Methodological Index for Non-randomised Studies (MINORS) criteria [37]. A fourth author (L.S.) resolved any cases of disagreement. All authors participated equally in the study design, manuscript preparation, and final review. This systematic review was registered on the International Prospective Register of Systematic Reviews (PROSPERO), CRD42022343517, in July 2022 [38].
Data extraction
Two reviewers (G.C. and F.B.) collected data from the selected studies and inserted them into a standard template. Initially, demographic data such as age, relevant surgical information, gait analysis protocol, and a minimum follow-up of the studies were extracted. Then, information regarding the kinematic and kinetic parameters, the tibiofemoral movement, the gait spatial–temporal parameters, and the clinical scores was collected.
Statistical analysis
Statistical analysis was performed by employing R software, version 4.0.5 (2020; R Core Team, Vienna, Austria). Descriptive statistical analysis was conducted for all data extracted from the included studies. Mean values with a measure of variability as standard deviation (SD) or range (minimum–maximum) were calculated for continuous variables. Absolute number and frequency distribution were calculated for categorical variables. Furthermore, when available, the P values of the variable analysis comparisons of the differences included in the various studies were reported.
Results
Study characteristics
Gait analysis was performed in 197 MP TKA (average age, 69.4 ± 3.9 years) and in 192 PS TKA patients (average age, 68.6 ± 4.4). Three studies [23, 26, 27] performed gait analysis also in a control group involving 40 healthy knees (average age, 36.1 ± 5.7). The average study quality based on MINORS criteria was 14.6 ± 2.6. The main demographic characteristics are reported in Table 1.
Kinematic parameters
Six studies reported kinematic data during gait analysis (Table 2) [28, 29, 31,32,33, 35]; two studies [29, 32] reported the peak of knee flexion angle during the swing phase; one of them [32] reported a statistically significantly greater peak in PS TKA compared to MP TKA. Two studies [28, 32] reported knee flexion angle at heel strike with no statistical difference found between the groups. No statistical differences were reported in knee flexion angle at the early stance phase [31], midstance knee flexion angle [28], knee flexion ROM [35], and knee abduction angle [33]. One study reported a significantly reduced knee flexion angle at toe-off in MP compared to PS TKA [32], and another reported a significantly greater knee adduction angle with PS than with MP TKA [28].
Kinetic parameters
Three studies reported kinetic parameters during gait analysis (Table 3) [28, 32, 35]; two studies reported the knee adduction moment [28, 32], and one reported the knee abduction moment [32], but no statistical differences in the two parameters between the two groups were reported. Two studies reported knee flexion moment [28, 32], and in both studies, patients receiving MP TKA showed a statistically significantly higher moment than their counterparts receiving PS TKA. A significantly higher value was reported for PS TKA regarding knee extension moment [28] and for MP TKA regarding knee rotation moment [28]. No statistical differences were reported in the peak internal rotation moment between the two groups [35].
Tibiofemoral movement
Four studies reported the tibiofemoral movement during gait analysis (Table 4) [29, 31, 33, 35]. Three studies [29, 31, 33] reported the anterior femoral roll during knee flexion; one of them [33] reported that PS TKA showed a significantly greater anterior femoral roll than MP TKA. One study reported the posterior translation on the medial condyle during knee flexion [29] with no statistical difference revealed between the two groups. One study reported a statistically significantly greater anterior translation on the medial condyle during knee flexion in the PS TKA group [33]. Two studies [29, 33] reported the anterior translation on lateral condyle during knee flexion, and one study [33] reported a significantly greater anterior translation in the PS TKA group. One study [33] reported the lateral translation on lateral and medial condyle during knee flexion, but no difference between the groups was reported. Three studies [29, 31, 33] reported the tibiofemoral external rotation motion during knee flexion, and only one of them [33] reported a statistically significant increase in the MP TKA group. Lastly, one study [35] reported the overall relative tibiofemoral internal/external rotation during the gait cycle, but no differences were noted between the two groups.
Gait spatial–temporal parameters
Six studies reported gait spatial–temporal parameters (Table 5) [27, 28, 30, 32,33,34]. Five studies [28, 30, 32,33,34] reported the walking speed. Three studies [27, 30, 34] reported the cadence. Three studies [27, 30, 34] reported the step length. One study reported the stride length [32]. Two studies reported the stance time [30, 34]. Lastly, one study reported the base of support [32]. In none of these gait spatial–temporal parameters were stastistically significant differences reported between MP and PS TKA.
Clinical scores
Seven studies reported clinical and functional scores (Table 6) [27, 29,30,31,32, 34, 35]. Three studies [31, 34, 35] utilized the Knee Society Clinical Score (KSCS), and one study [35] among them also analyzed the Knee Functional Score (KFS). Two studies [32, 34] analyzed the Oxford Knee Score (OKS). No statistically significant differences were found between MP and PS TKA patients in terms of these three scores. Two studies [29, 30] utilized the Forgotten Joint Score (FJS), and in one [30] of these studies, a statistically significant difference was noted in favor of the MP TKA. Finally, one study [27] reported the Western Ontario and McMaster Universities Arthritis Index (WOMAC) score, and no statistically significant differences were found in all the subscale results analyzed except for the stiffness, which was found to be significantly higher in MP TKA.
Discussion
This study aimed to comprehensively understand kinetic and kinematic differences between MP and PS TKA designs. Particular attention was paid to tibiofemoral movements, spatio-temporal parameters, and clinical scores between patients treated with MP and those with PS TKA. Several significant differences between the two prosthetic designs were observed in this systematic review.
The analysis of kinematic parameters exhibited a higher knee flexion peak in the swing phase, greater knee flexion at toe-off and an increase in the adduction angle in the PS TKA relarive to MP TKA. The kinetic evaluation revealed that the MP TKA designs had a greater maximum flexion and rotation moment, while the PS TKA presented a higher extension moment than MP TKA. The PS TKA design showed an increased anterior femoral roll and anterior translation on medial and lateral condyle during knee flexion, while the MP TKA showed a greater tibia external rotation than PS TKA. No differences were reported between the two prosthetic designs in spatio-temporal parameters. Finally, the clinical evaluation demonstrated that the MP TKA had a better FJS score and a statistically significant stiffness in terms of the WOMAC score compared to the PS TKA.
Stiff-knee pattern
A typical "stiff knee pattern", characterized by a knee flexion reduction during the initial phase of the swing from toe-off to the peak knee flexion, was observed in both designs. This condition was caused by a compensatory mechanism, known as "quadriceps avoidance", typical of patients with terminal knee osteoarthritis, to limit anterior pain due to quadriceps femoris contraction [39, 40]. Esposito et al. demonstrated that the "stiff-knee pattern" was emphasized in MP TKA compared to PS TKA during peak knee flexion or knee flexion at toe-off: the kinetic results presented in this study supported the kinematic data, having a reduction in maximum knee flexion and extension moment, resulting in clinically lower forces at the patella-trochlear junction [32]. In their electromyographic gait analysis evaluation, the same authors observed that muscle activation time of the rectus femoris, biceps femoris and vastus medialis were significantly lower in the MP TKA compared to both the PS TKA and the control group. Therefore, the PS TKA kinematics during gait was more similar to the physiological non-arthritic knees’ kinematics [32]. Comparable data were also observed by Miura et al. [31], who reported reduced knee flexion in the healthy control group in both MP and PS TKA without finding statistically significant differences between the two prosthetic designs.
Paradoxical anterior femoral roll
The "paradoxical anterior femoral roll" during knee flexion was reported in both MP and PS TKA designs. Several studies have described paradoxical anterior femoral sliding and incorrect tibiofemoral axial rotation during knee flexion in PS TKA in relation to healthy knees [41,42,43]. Compared to other TKA models, MP TKA may limit anterior femoral translation during knee flexion due to the high congruence of the medial compartment [21]. Two of the three studies that analyzed femoral rollback observed that the PS TKA had more statistically significant translation than the MP TKA [29, 33], whereas no difference was reported by Miura et al. in their paper [31]. Contradictory results were reported for the posterior medial condyle translation during knee flexion because. Theoretically, the MP TKA should provide a stable medial compartment, described as a ball and socket, limiting the overall translation. This hypothesis was confirmed by Gray et al. in their article [33]. On the other hand, no difference was observed by Tan et al. [29]. Two studies reported no statistically significant differences in the lateral femoral condyle anterior translation between the two groups [29, 33].
Screw-home mechanism
The "screw-home mechanism" represents one of the most critical factors influencing knee stability during standing. It is characterized by relative tibiofemoral axial rotation during the last 20º–30º of knee extension. All studies included in this systematic review reported that MP, as well as PS TKA designs, failed to reproduce this knee mechanism. The screw-home motion is a complex kinematic phenomenon requiring the integrity of anterior cruciate ligament (ACL). The ACL plays a key role as a stabilizer during the late swing/early stance by promoting external rotation of the tibia relative to the femur. Unfortunately, the ACL is currently sacrificed by many PS and MP TKA designs. Among the three studies [29, 31, 33] which analyzed tibiofemoral external rotation during knee flexion, only Gray et al. [33] described greater external rotation with the MP TKA design when compared to its PS counterpart. At the same time, many other studies covered by the current review reported no statistically significant differences between the two prosthetic designs [29, 31].
Limitations
This paper has multiple limitations. First, various manufacturers' MP and PS TKA designs have been analyzed. The articles included in this systematic review examined five different MP and PS TKA models. In addition, the inclusion of both single-radius and multi-radius TKA may result in kinematic changes of knee. In particular, the radius of condylar curvature has a great impact on reducing pressure in the patellofemoral joint, preventing paradoxical anterior motion, and improving quadriceps efficiency. Second, the number of TKAs included in some studies was small, so the systematic review may be under-powered. Third, all gait analysis studies included in the current review were performed using different cameras, force plates, walking surfaces, walking speed and time after surgery. Finally, various clinical and functional scores were analyzed in the included studies. More homogenous use of the implants, a more standardized gait analysis protocol and clinical and functional evaluation might improve data validity.
Conclusion
This systematic review confirmed that important kinematic and kinetic differences exist between MP and PS TKA designs, but both TKAs kinematics are quite distant from that of a healthy knee. Patients who underwent PS TKA appeared less affected by the stiff-knee pattern. Both prosthetic designs showed an "undesired" paradoxical anterior femoral motion in the early stance phase. This phenomenon was, however, less pronounced in the MP TKA design. Finally, both designs were ultimately unable to reproduce the screw-home mechanism.
Availability of data and materials
The dataset analysed in this study is available from the corresponding author on reasonable request.
References
Kurtz SM, Ong KL, Schmier J, Mowat F, Saleh K, Dybvik E, et al. Future clinical and economic impact of revision total hip and knee arthroplasty. J Bone Joint Surg Am. 2007;89(Suppl 3):144–51. https://doi.org/10.2106/JBJS.G.00587.
Kurtz SM, Ong KL, Lau E, Bozic KJ. Impact of the economic downturn on total joint replacement demand in the United States: updated projections to 2021. J Bone Joint Surg Am. 2014;96(8):624–30. https://doi.org/10.2106/JBJS.M.00285.
Mont MA, Issa K. Updated projections of total joint arthroplasty demands in America. Commentary on an article by Steven M. Kurtz, PhD, et al.: “Impact of the Economic Downturn on Total Joint Replacement Demand in the United States. Updated Projections to 2021.” J Bone Joint Surg Am. 2014;96(8):e68. https://doi.org/10.2106/JBJS.N.00005.
de Steiger RN, Graves SE. Orthopaedic registries: the Australian experience. EFORT Open Rev. 2019;4(6):409–15. https://doi.org/10.1302/2058-5241.4.180071.
Ayers DC, Yousef M, Zheng H, Yang W, Franklin PD. The prevalence and predictors of patient dissatisfaction 5-years following primary total knee arthroplasty. J Arthroplasty. 2022;37(6S):S121–8. https://doi.org/10.1016/j.arth.2022.02.077.
Cacciola G, Mancino F, De Meo F, Bruschetta A, De Martino I, Cavaliere P. Current reconstruction options in periprosthetic fractures around the knee. Geriatr Orthop Surg Rehabil. 2021;12:21514593211023996. https://doi.org/10.1177/21514593211023996.
Capella M, Risitano S, Sabatini L, Faccenda C, Barberis L, Camazzola D, et al. Tibial condylar valgus osteotomy for the treatment of intra-articular varus deformity of the knee. Annals Of Joint, 2022;0. Annals of Joint. 2022 July. https://doi.org/10.21037/aoj-22-19.
Kahlenberg CA, Nwachukwu BU, McLawhorn AS, Cross MB, Cornell CN, Padgett DE. Patient satisfaction after total knee replacement: a systematic review. HSS J. 2018;14(2):192–201. https://doi.org/10.1007/s11420-018-9614-8.
Nakano N, Shoman H, Olavarria F, Matsumoto T, Kuroda R, Khanduja V. Why are patients dissatisfied following a total knee replacement? A systematic review. Int Orthop. 2020;44(10):1971–2007. https://doi.org/10.1007/s00264-020-04607-9.
Cacciola G, Mancino F, De Meo F, Di Matteo V, Sculco PK, Cavaliere P, et al. Mid-term survivorship and clinical outcomes of the medial stabilized systems in primary total knee arthroplasty: a systematic review. J Orthop. 2021;22(24):157–64. https://doi.org/10.1016/j.jor.2021.02.022.
Cacciola G, De Martino I, De Meo F. Does the medial pivot knee improve the clinical and radiographic outcome of total knee arthroplasty? A single centre study on two hundred and ninety seven patients. Int Orthop. 2020;44(2):291–9. https://doi.org/10.1007/s00264-019-04462-3.
Ranawat CS. History of total knee replacement. J South Orthop Assoc. 2002;11(4):218–26 PMID: 12597066.
Insall JN, Lachiewicz PF, Burstein AH. The posterior stabilized condylar prosthesis: a modification of the total condylar design Two to four-year clinical experience. J Bone Joint Surg Am. 1982;64(9):1317–23 PMID: 7142239.
Kolisek FR, McGrath MS, Marker DR, Jessup N, Seyler TM, Mont MA, et al. Posterior-stabilized versus posterior cruciate ligament-retaining total knee arthroplasty. Iowa Orthop J. 2009;29:23–7 PMID: 19742081.
Yacovelli S, Grau LC, Hozack WJ, Courtney PM. Functional outcomes are comparable between posterior stabilized and cruciate-substituting total knee arthroplasty designs at short-term follow-up. J Arthroplasty. 2021;36(3):986–90. https://doi.org/10.1016/j.arth.2020.09.008.
Freeman MA, Pinskerova V. The movement of the knee studied by magnetic resonance imaging. Clin Orthop Relat Res. 2003;410:35–43. https://doi.org/10.1097/01.blo.0000063598.67412.0d.
Freeman MA, Pinskerova V. The movement of the normal tibiofemoral joint. J Biomech. 2005;38(2):197–208. https://doi.org/10.1016/j.jbiomech.2004.02.006.
Sabatini L, Risitano S, Parisi G, Tosto F, Indelli PF, Atzori F, et al. Medial pivot in total knee arthroplasty: literature review and our first experience. Clin Med Insights Arthritis Musculoskelet Disord. 2018;11:1179544117751431. https://doi.org/10.1177/1179544117751431.
Atzori F, Salama W, Sabatini L, Mousa S, Khalefa A. Medial pivot knee in primary total knee arthroplasty. Ann Transl Med. 2016;4(1):6. https://doi.org/10.3978/j.issn.2305-5839.2015.12.20.
Mancino F, Di Matteo V, Mocini F, Cacciola G, Malerba G, Perisano C, et al. Survivorship and clinical outcomes of proximal femoral replacement in non-neoplastic primary and revision total hip arthroplasty: a systematic review. BMC Musculoskelet Disord. 2021;22(Suppl 2):933. https://doi.org/10.1186/s12891-021-04711-w.
Sabatini L, Bosco F, Barberis L, Camazzola D, Bistolfi A, Risitano S, et al. Kinetic sensors for ligament balance and kinematic evaluation in anatomic Bi-cruciate stabilized total knee arthroplasty. Sensors (Basel). 2021;21(16):5427. https://doi.org/10.3390/s21165427.
Bistolfi A, Giustra F, Bosco F, Faccenda C, Viotto M, Sabatini L, et al. Comparable results between crosslinked polyethylene and conventional ultra-high molecular weight polyethylene implanted in total knee arthroplasty: systematic review and meta-analysis of randomised clinical trials. Knee Surg Sports Traumatol Arthrosc. 2022;30(9):3120–30. https://doi.org/10.1007/s00167-022-06879-7.
Bistolfi A, Giustra F, Bosco F, Sabatini L, Aprato A, Bracco P, et al. Ultra-high molecular weight polyethylene (UHMWPE) for hip and knee arthroplasty: the present and the future. J Orthop. 2021;25:98–106. https://doi.org/10.1016/j.jor.2021.04.004.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. https://doi.org/10.1371/journal.pmed.1000100.
Artiaco S, Bosco F, Lusso A, Cioffi LL, Battiston B, Massè A. Flexor tendon pulley injuries: a systematic review of the literature and current treatment options. J Hand Microsurg. 2022. https://doi.org/10.1055/s-0042-1749420.
Via RG, F. Bosco, F. Giustra et al. Acute Rockwood type III ACJ dislocation: Conservative vs surgical approach. A systematic review and meta-analysis of current concepts in literature, Injury, 2022. https://doi.org/10.1016/j.injury.2022.07.050.
Stolarczyk A, Maciąg BM, Mostowy M, Maciąg GJ, Stępiński P, Szymczak J, et al. Comparison of biomechanical gait parameters and patient-reported outcome in patients after total knee arthroplasty with the use of fixed-bearing medial pivot and multi-radius design implants-retrospective matched-cohort study. Arthroplast Today. 2022;14:29–35. https://doi.org/10.1016/j.artd.2021.10.002.
Ghirardelli S, Asay JL, Leonardi EA, Amoroso T, Andriacchi TP, Indelli PF. Kinematic comparison between medially congruent and posterior-stabilized third-generation TKA designs. J Funct Morphol Kinesiol. 2021;6(1):27. https://doi.org/10.3390/jfmk6010027.
Tan J, Zou D, Zhang X, Zheng N, Pan Y, Ling Z, et al. Loss of knee flexion and femoral rollback of the medial-pivot and posterior-stabilized total knee arthroplasty during early-stance of walking in chinese patients. Front Bioeng Biotechnol. 2021;9:675093. https://doi.org/10.3389/fbioe.2021.675093.
Bianchi N, Facchini A, Mondanelli N, Sacchetti F, Ghezzi R, Gesi M, et al. Medial pivot vs posterior stabilized total knee arthroplasty designs: a gait analysis study. Med Glas (Zenica). 2021;18(1):252–9. https://doi.org/10.17392/1312-21.
Miura K, Ohkoshi Y, Ino T, Ukishiro K, Kawakami K, Suzuki S, et al. Kinematics and center of axial rotation during walking after medial pivot type total knee arthroplasty. J Exp Orthop. 2020;7(1):72. https://doi.org/10.1186/s40634-020-00286-y.
Esposito F, Freddolini M, Marcucci M, Latella L, Corvi A. Biomechanical analysis on total knee replacement patients during gait: Medial pivot or posterior stabilized design? Clin Biomech (Bristol, Avon). 2020;78:105068. https://doi.org/10.1016/j.clinbiomech.2020.105068.
Gray HA, Guan S, Young TJ, Dowsey MM, Choong PF, Pandy MG. Comparison of posterior-stabilized, cruciate-retaining, and medial-stabilized knee implant motion during gait. J Orthop Res. 2020;38(8):1753–68. https://doi.org/10.1002/jor.24613.
Benjamin B, Pietrzak JRT, Tahmassebi J, Haddad FS. A functional comparison of medial pivot and condylar knee designs based on patient outcomes and parameters of gait. Bone Joint J. 2018;100-B(1 Supple A):76–82. https://doi.org/10.1302/0301-620X.100B1.BJJ-2017-0605.R1.
Papagiannis GI, Roumpelakis IM, Triantafyllou AI, Makris IN, Babis GC. No differences identified in transverse plane biomechanics between medial pivot and rotating platform total knee implant designs. J Arthroplasty. 2016;31(8):1814–20. https://doi.org/10.1016/j.arth.2016.01.050.
Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg. 2011;128(1):305–10. https://doi.org/10.1097/PRS.0b013e318219c171.
Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712–6. https://doi.org/10.1046/j.1445-2197.2003.02748.x.
Sideri S, Papageorgiou SN, Eliades T. Registration in the international prospective register of systematic reviews (PROSPERO) of systematic review protocols was associated with increased review quality. J Clin Epidemiol. 2018;100:103–10. https://doi.org/10.1016/j.jclinepi.2018.01.003.
Benedetti MG, Catani F, Bilotta TW, Marcacci M, Mariani E, Giannini S. Muscle activation pattern and gait biomechanics after total knee replacement. Clin Biomech. 2003;18(9):871–6. https://doi.org/10.1016/s0268-0033(03)00146-3.
Mandeville D, Osternig LR, Chou LS. The effect of total knee replacement on dynamic support of the body during walking and stair ascent. Clin Biomech. 2007;22(7):787–94. https://doi.org/10.1016/j.clinbiomech.2007.04.002.
Schmidt R, Komistek RD, Blaha JD, Penenberg BL, Maloney WJ. Fluoroscopic analyses of cruciate-retaining and medial pivot knee implants. Clin Orthop Relat Res. 2003;410:139–47. https://doi.org/10.1097/01.blo.0000063565.90853.a4.
Banks SA, Hodge WA. 2003 Hap Paul award paper of the international society for technology in arthroplasty. Design and activity dependence of kinematics in fixed and mobile-bearing knee arthroplasties. J Arthroplasty. 2004;19(7):809–16. https://doi.org/10.1016/j.arth.2004.04.011.
Dimitriou D, Tsai TY, Park KK, Hosseini A, Kwon YM, Rubash HE, et al. Weight-bearing condyle motion of the knee before and after cruciate-retaining TKA: In-vivo surgical transepicondylar axis and geometric center axis analyses. J Biomech. 2016;49(9):1891–8. https://doi.org/10.1016/j.jbiomech.2016.04.033.
Acknowledgements
None.
Funding
No funding has been received for this study.
Author information
Authors and Affiliations
Contributions
S.R., G.C., F.B. and F.G. have contributed substantially to conception and design, data acquisition, analysis, and interpretation. They have been involved in drafting the manuscript and revising it critically for important intellectual content. They agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. F.F. and M.C. have contributed substantially to the data analysis, interpretation, and manuscript drafting. P.F.I. and A.M. have significantly contributed to the conception, analysis and interpretation of data and have been involved in drafting the manuscript. L.S. has made substantial contributions to concept and design. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
All authors have no competing interests for this study to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Risitano, S., Cacciola, G., Capella, M. et al. Comparison between gaits after a medial pivot and posterior stabilized primary total knee arthroplasty: a systematic review of the literature. Arthroplasty 5, 15 (2023). https://doi.org/10.1186/s42836-023-00165-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42836-023-00165-8