
Abstract
Background
Recent studies showed that healthcare disparities exist in use of and outcomes after total joint arthroplasty (TJA). This systematic review was designed to evaluate the currently available evidence regarding the effect socioeconomic factors, like income, insurance type, hospital volume, and geographic location, have on utilization of and outcomes after lower extremity arthroplasty.
Methods
A comprehensive search of the literature was performed by querying the MEDLINE database using keywords such as, but not limited to, “disparities”, “arthroplasty”, “income”, “insurance”, “outcomes”, and “hospital volume” in all possible combinations. Any study written in English and consisting of level of evidence I-IV published over the last 20 years was considered for inclusion. Quantitative and qualitative analyses were performed on the data.
Results
A total of 44 studies that met inclusion and quality criteria were included for analysis. Hospital volume is inversely correlated with complication rate after TJA. Insurance type may not be a surrogate for socioeconomic status and, instead, represent an independent prognosticator for outcomes after TJA. Patients in the lower-income brackets may have poorer access to TJA and higher readmission risk but have equivalent outcomes after TJA compared to patients in higher income brackets. Rural patients have higher utilization of TJA compared to urban patients.
Conclusion
This systematic review shows that insurance type, socioeconomic status, hospital volume, and geographic location can have significant impact on patients’ access to, utilization of, and outcomes after TJA.
Level of evidence
IV.
Similar content being viewed by others


Background
Osteoarthritis of the hip and knee was ranked the 11th highest contributor to global disability in 2010 [1]. Within the United States alone, the demand for primary THA and TKA is estimated to grow by 174% and 673%, respectively, by 2030, with economic downturns having limited impact on this rising demand [2]. However, access to beneficial orthopedic procedures may not be equal across different patient groups. Segal et al. showed that access to spine surgeons was significantly affected by insurance coverage—patients with private insurance were able to obtain an appointment 86.3% of the time without a primary care physician (PCP) referral while Medicaid patients could obtain an appointment 0% of the time without a PCP referral and 55% of the time with a PCP referral [3].
In addition to these observed disparities in access to orthopedic procedures, recent evidence suggests that disparities may persist in outcomes as well. Lansdown et al. showed that patients with Medicaid insurance had significantly lower preoperative and postoperative functional scores and had fewer follow-up visits after shoulder arthroplasty compared to patients with other insurance types [4]. These disparities in healthcare utilization and outcomes after orthopedic procedures call for a better understanding of the underlying causes so that these disparities may be mitigated. The purpose of this systematic review was to evaluate the currently available evidence regarding the effect socioeconomic factors such as income, insurance type, hospital volume, and geographic location have on utilization of and outcomes after lower extremity arthroplasty.
Methods
Search strategy
A search of the literature was performed by querying the MEDLINE database to identify studies that assessed healthcare disparities in patients undergoing THA or TKA. This literature search was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. All possible combinations of the following keywords were used for the search: “healthcare disparities,” “hip,” “knee,” “arthroplasty,” “joint replacement,” “THA,” “TKA,” “insurance”, “hospital volume”, “outcomes”, “social determinants”, “socioeconomic”, “payer type,” “inequities,” “inequality,” “bias,” “utilization rate,” “Medicaid,” “Medicare,” “demographic factors,” and “income.” The literature search was limited to studies published in the last twenty years from February 14, 2001, to February 14, 2021.
Study selection
Studies meeting the following inclusion criteria were selected for the systematic review: (a) Study Level of Evidence was I, II, III, or IV as defined by Centre for Evidence-Based Medicine for therapeutic studies, (b) the study reported on results on topics within the scope of this review and (c) study had all adult participants.
Studies meeting the following exclusion criteria were not included in this review: (a) prior systematic reviews, (b) non-English studies, (c) case reports, expert opinions, or other studies with level V evidence, (d) basic science or biomechanical studies, (e) studies involving non-human subjects, cadavers, or pediatric patients, (f) studies involving revision surgery patients, and (g) studies conducted outside of the United States. The study selection algorithm and search results are provided in Fig. 1.

PRISMA study selection algorithm
Data extraction & analysis
The following details from each article were collected and recorded in Excel: the article title, year of publication, authors, journal published, study design, level of evidence, study question, methods, patient demographics, and pertinent results. These data were independently analyzed and synthesized.
Quality appraisal and risk of bias assessment
The methodological quality of each study was assessed using specific criteria set forth by US Preventive Services Task Force for development of a more evidence-based approach to setting clinical practice guidelines [5]. The specific quality appraisal and risk of bias assessment criteria used to conduct this analysis are listed in the Additional file 1.
Sources of funding
The authors received no funding for this study.
Results
Forty-four studies met the inclusion and quality criteria. The study aims, level of evidence, methodology, and results are listed in alphabetical order of the first author in Table 1A in Additional file 1.
Insurance type
Twenty-five studies assessed the effect of patients’ insurance type on access to and outcomes after TJA.
Insurance type: access/utilization
Five studies assessed insurance type and its effect on access to THA evaluation. Almaguer et al. reported that appointments for THA evaluation were successful 99% of the time with private insurance vs. 72% of the time with Medicaid (P < 0.001) [6]. Average time to appointment was also longer for Medicaid compared to private insurance (26 days vs. 13 days, P = 0.02) [6]. Boylan et al. looked at use of technology assistance in TKA and THA and found that technology was more likely to be used for patients with private insurance (5.9%) compared to Medicare (4.7%, P < 0.001) or Medicaid (2.2%, P < 0.001) [7]. Hanchate et al. assessed the effect of socioeconomic status and insurance coverage on TKA utilization rates and reported that Medicare patients with supplemental insurance, whether it be private (OR 1.27, 95% CI 0.82–1.96) or Medicaid (OR 1.18; 95% CI 0.93–1.49), were more likely to receive a primary TKA than those without it [8]. Among middle-aged patients (age 47–64), the uninsured were much less likely to receive a primary TKA than those with private insurance (OR 0.61, 95% CI 0.40–0.92) [8]. SooHoo et al. reported that Medicaid insurance was an independent predictor of receiving TKA at a low-volume hospital (P < 0.05) [9]. Veltre et al. reported that privately-insured patients tend to undergo total hip replacement at higher-volume hospitals compared to Medicaid-insured or uninsured patients (46.2% vs. 28.7%) [10].
Insurance type: outcomes
There were 19 studies that assessed the relationship between insurance type and outcomes after TJA.
In evaluating mortality and complications, Adelani et al. reported that having Medicaid insurance was associated with higher postoperative mortality (OR 1.97, 95% CI 1.49–2.59) [11]. Browne et al. reported that Medicaid patients had a higher prevalence of postoperative in-hospital infection (OR 1.7, 95% CI 1.3–2.1), wound dehiscence (OR 2.2, 95% CI 1.4–3.4), hematoma or seroma (OR 1.3, 95% CI 1.2–1.4) and longer length of stay but a lower risk of cardiac complications (OR 0.7, 95% CI 0.6–0.9) after TJA [12]. Maman et al. reported that Medicaid patients had greater odds of in-hospital mortality (OR 1.73, 95% CI 1.01–2.95, P < 0.05), any postoperative complications (OR 1.25, 95% CI 1.18–1.33, P < 0.005), extended length of stay (OR 1.09, 95% CI 1.08–1.10, P < 0.005) and higher total charges (OR 1.03, 95% CI 1.02–1.04, P < 0.005) [13]. Menendez et al. reported that Medicaid, but not Medicare or uninsured status was associated with higher odds of in-patient dislocation after THA (OR 1.30, 95% CI 1.02–1.65, P = 0.034) [14]. Plate et al. reported that Medicaid patients had significantly higher ASA scores (P < 0.001) and BMI (P < 0.001), with corresponding increase in procedure duration (P < 0.001), and prolonged LOS (P < 0.001) compared with other insurances, but similar to Medicare patients [15]. Veltre et al. reported that patients with private insurance had fewer medical complications (OR 0.80; P < 0.001) after THA compared to patients with Medicaid, Medicare, or no insurance [10]. Privately-insured patients also had fewer surgical complications and lower mortality after THA compared to other groups [10]. It was also reported that Medicare patients had a higher risk of mortality (relative risk [RR], 1.34; P < 0.001) after TKA compared to privately insured patients [16]. Xu et al. reported that Medicaid payer status was associated with the highest statistically significant adjusted odds of mortality (OR 2.25, 95% CI 1.01–5.01), any complications (OR, 1.26), cardiovascular complications (OR, 1.37), infectious complications (OR, 1.66) when compared with private insurance patients after THA [17].
In assessing readmission, Arroyo et al. reported that patients with Medicare and Medicaid insurance had higher odds of 30-day (OR 1.23, 95% CI 1.17–1.28 and OR 1.58, 95% CI 1.46–1.71 respectively) and 90-day readmission (OR 1.17, 95% CI 1.13–1.20 and OR 1.46, 95% CI 1.38–1.54 respectively) compared to private insurance holders [18]. Oronce et al. reported that, compared to private insurance, Medicare (OR 1.26, 95% CI 1.13–1.43), Medicaid (OR 1.86, 95% CI 1.49–2.32), and uninsured status (OR 1.31, 95% CI 1.01–1.69) were associated with increased 30-day readmission risk after THA [19]. Plate et al. reported that Medicare patients were significantly more likely to return to the ED (OR 3.15, 95% CI 1.88–5.27, P < 0.001) and be readmitted (OR 2.46, 95% CI 1.26–4.81, P = 0.009) compared to private or Medicaid insurance [15]. White et al. found that patients insured by Medicaid (OR 1.23, 95% CI 1.17–1.29) and Medicare (OR 1.58, 95% CI 1.44–1.73) had higher odds of 30-day readmission after THA compared to privately-insured patients [20]. Xu et al. reported that Medicaid payer status was associated with increased odds of 30-day (OR, 1.63) and 90-day readmission (OR, 1.58) after THA [17].
In assessing discharge disposition, Browne et al. reported that Medicaid patients had higher rates of discharge to inpatient facility after TJA (P < 0.01) compared to non-Medicaid insurance holders [12]. Lan et al. also found that non-private insurance holders had higher odds of discharge to an institution after TJA (OR 1.56, 95% CI 1.26–1.94) and having an extended length of stay [21]. Li et al. reported that the rate of discharge to an institution after TJA was 32.5% (95% CI 32.4%–32.7%) for Medicare-only patients, but for dual-eligible patients, the risk was similar, being at 62.3% (95% CI 61.5%–63.0%) for those with full benefits, and 61.5% (95% CI 60.7%–62.3%) for those with partial benefits [22]. Singh et al. reported that Medicare, Medicaid, and other insurance were associated with significantly higher odds of discharge to a rehabilitation facility, with OR of 1.77, 1.40, and 1.14, respectively, compared to private insurance [23]. Weiner et al. reported that Medicaid or uninsured status was associated with increased risk of non-home discharge (P < 0.05) [24]. In contrast, Feng et al. found that Medicaid status had no effect on inpatient facility discharge but was associated with longer length of stay (rate ratio 1.21, 95% CI 1.02–1.43, P = 0.026) [25]. Yayac et al. reported that Medicare Advantage patients were more likely to be discharged to a rehabilitation facility (19% vs. 14%, P < 0.0001) compared to traditional Medicare insurance patients after TJA [26].
In assessing functional outcomes, Halawi et al. reported that, at 1-year follow-up after TJA, Medicaid patients scored lower on PROMs (P < 0.01) even though net gains were comparable between Medicaid, Medicare and private insurance holders [27]. Starring et al. reported that Medicare patients reported significantly less ability to perform activities of daily living (78.6 vs. 63.2, P = 0.001), worse physical function (39.6 vs. 44.9, P = 0.003), and more pain interference (57.9 vs. 52.4, P = 0.018) at day 180 after TKA than commercially-insured patients [28].
Insurance type: preoperative status
Two studies assessed preoperative status of patients with different insurance types prior to TJA. Lavernia et al. reported that patients with private insurance or those who were covered by Medicare had significantly better preoperative Quality of Wellbeing (QWB), SF-36, pain, and WOMAC scores relative to patients with Medicaid or those who were indigent prior to TJA (P < 0.01) [29]. Martin et al. reported that Medicaid patients had significantly worse SF-36 and WOMAC scores across all categories compared with patients with Medicare or private insurance (P < 0.05 for each comparison) [30]. In addition, patients with Medicaid had a higher incidence of current smoking and higher mean BMI and traveled an average of 29 to 30 miles farther for access to care (P < 0.05 for each comparison) [30].
The healthcare disparities among the different insurance holders in terms of TJA utilization rate, surgical outcomes, and preoperative status are summarized in Figs. 2 and 3.

TJA outcomes of Medicaid compared to private/commercial insurance holders

TJA outcomes of Medicare compared to private/commercial insurance holders
Socioeconomic status
Fifteen studies assessed the impact of socioeconomic status (SES) on utilization rates of and outcomes after TJA.
Socioeconomic status: access/utilization
There were 5 studies that assessed the impact of socioeconomic status on access to TJA. Dangelmajer et al. looked at utilization of hemiarthroplasty vs. THA for femoral neck fractures and found that there was no statistically significant difference in rates of THA for patients of different household incomes [31]. Skinner et al. also found little association between income and rates of TKA (OR 0.98, P < 0.05) but the association between TKA and income became stronger after adjusting for hospital referral region—then a 10% increase in income within a region was associated with a 1.9% increase in rate of TKA [32].
However, Hanchate et al. reported that those in the lowest income category (under $10K) had an estimated OR of 0.75 for receiving TKA compared to those in the highest income tier [8]. Similarly, Hawkins et al. reported that patients who lived in lower income areas were 5-10% (P < 0.001) less likely to receive a THA or TKA compared to those who resided in higher income areas [33]. SooHoo et al. reported that patients within the lowest income group were at increased risk of being treated at either a low-volume (relative risk ration [RRR] = 3.19, 95% CI 1.89–5.37, P < 0.001) or intermediate volume (RRR = 1.80, 95% CI 1.09–2.98, P = 0.02) hospital compared to patients within the highest income group [34].
Socioeconomic status: outcomes
There were 10 studies that assessed the impact of socioeconomic status on outcomes after TJA.
In evaluating complication risk, Menendez et al. reported that lower household income ($1–$47,999: OR = 1.22, 95% CI = 1.09–1.36; $48,000–$62,999: OR = 1.16, 95% CI = 1.03–1.31; vs. ≥$63,000) was associated with increased odds of inpatient dislocation after primary THA [14]. However, Singh et al. reported that the lowest income quartile was associated with a lower likelihood of discharge to a rehabilitation/inpatient facility (HR 0.78, 95% CI 0.7– 0.79), hospital stay > 3 days (HR 0.82, 95% CI 0.80–0.83), infection (HR 0.57, 95% CI 0.50–0.65), and transfusion (HR 0.80, 95% CI 0.79–0.82) [23]. These results show that lower income does not negatively impact outcomes after total hip arthroplasty.
In evaluating revision risk, Bass et al. reported that community poverty was not significantly associated with TKA failure or revision [35].
In evaluating readmission risk, Arroyo et al. reported that, when compared to patients in the lowest median income quartile (the first quartile), patients in the higher median income quartiles all had reduced adjusted OR of 30-day and 90-day readmissions after TKA [18]. Oronce et al. also reported that lower socioeconomic status was associated with higher odds of 30-day readmission (OR 1.24, 95% CI 1.10–1.39) after THA [19]. White et al. reported that patients living in areas with higher median household income were less likely to be readmitted after TJA compared to those living in poorer areas (30-day readmission OR = 0.89, P < 0.05 and 90-day readmission OR = 0.91, P < 0.05) [20].
In evaluating discharge disposition, Inneh et al. reported that low and middle socioeconomic status was a significant predictor of discharge to an institution (OR 1.27, 95% CI 1.02–1.57, P = 0.029, and OR 1.26, 95% CI 1.10–1.44, P = 0.001) [36]. In contrast, Weiner et al. reported no significant association between household income and non-home discharge after THA [24].
In evaluating functional outcomes, Goodman et al. reported that higher census tract poverty level was associated with worse WOMAC pain scores at 2 years after TKA (P = 0.001) but this difference in pain scores did not reach minimal clinically important difference (MCID) [37]. Singh et al. reported that lower annual incomes of ≤ US$35, 000 (OR 0.61, 95% CI 0.40–0.94, P = 0.02) and > US$35, 000 to $45,000 (OR 0.68, 95% CI 0.49–0.94, P = 0.02) were associated with moderate to severe pain at 2 years after primary TKA but these differences disappeared by 5 years [38].
The healthcare disparities among the different socioeconomic classes in terms of TJA utilization rates and surgical outcomes are summarized in Fig. 4.

TJA outcomes of lower SES patients compared to higher SES patients
Hospital volume
There were 9 studies that assessed the impact of hospital volume on patient outcomes after TJA.
Anis et al. reported that hospital volume was not found to have a significant association with revision surgery for infection or superficial infection rate when comparing high-volume to medium and low-volume hospitals [39]. In contrast, the remaining studies all showed that hospital volume was inversely correlated with complication rate after arthroplasty. Adelani et al. reported that the complication rate (10.2% in the lowest volume quartile to 6.7% in the highest volume quartile), readmissions (10.5% in the lowest volume quartile to 7.2% in the highest volume quartile), and ED visits (11.4% to 8.0%) after THA decreased as hospital volume increased [40]. Similarly, complications (9.1% in the lowest volume quartile to 6.8% in the highest volume quartile), readmissions (11.4% in the lowest volume quartile to 7.4% in the highest volume quartile), and ED visits (11.4–8.7%) in TKA patients decreased as hospital volume increased [40]. Doro et al. also reported that the highest-volume hospitals had significantly lower risk of mortality (0.16% vs. 0.29%, P < 0.001), discharge to ECF (37% vs. 42%, P < 0.001), and prolonged length of stay (14% vs. 23%, P < 0.001) after primary THA compared to low-volume hospitals [41]. Similarly, Hollenbeck et al. reported that procedure volume (OR 2.116, 95% CI 1.883 to 2.378) and lower patient acuity (OR 2.450, 95% CI 2.429–2.472) were independently associated with better Perfect Inpatient Care Index (PICI) scores for TJA [42]. Koltsov et al. reported that hospitals where less than 54 THA procedures were being performed per year had higher rate of complications (1.5-fold higher) and mortality (4-6-fold higher) after THA compared to hospitals where higher volume of THA procedures were being performed per year [43]. Laucis et al. also showed that very high-volume hospitals (>1000 procedures annually) had the lowest complication rates (2.745 per 100, 95% CI 2.56–2.93), and low-volume hospitals (<100 procedures annually) had the highest complication rates (3.610 per 100, 95% CI 3.58–3.64, P < 0.0001; OR 1.327, 95% CI 1.26–1.40) [44]. Manley et al. reported that TKA patients in the lowest-volume hospitals (1–25 procedures per year) had a higher risk of revision at 5 and 8 years compared with those operated on in highest-volume hospitals (>200 procedures) (OR: 1.57 and 1.52, respectively) [45].
Singh et al. reported that very low volume (≤25 procedures/year), low volume (26–100 procedures/year), and high volume (101–200 procedures/year) hospitals conferred a higher risk of venous thromboembolism (OR 2.0, 95% CI 0.2–16.0 vs. OR 3.4, 95% CI 1.4–8.0 vs. OR 1.1, 95% CI 0.3–3.7, respectively) and 1-year mortality (OR 2.1, 95% CI 1.2–3.6 vs. OR 2.0, 95% CI 1.4–2.9 vs. OR 1.0, 95% CI 0.7–1.5, respectively) than very high-volume (>200 procedures/year) hospitals on patients who underwent primary THA [46]. Similarly, patients who underwent primary TKA at very low-volume hospitals had significantly higher 1-year mortality rate (OR 1.6, 95% CI 1.0–2.4) compared to those who underwent TKA at very-high-volume hospitals [46]. Wilson et al. also found that complication rate after TKA was inversely proportional (P < 0.05) to hospital volume up to a point, i.e., complications decreased with increasing hospital volume but the rates did not differ between high volume (236 to 644 arthroplasties per year) and very high volume (≥645 arthroplasties per year) hospitals [47]. They also reported that mortality rates after TKA were significantly lower (P < 0.05) for hospitals with ≥645 total knee arthroplasties per year compared to those below the threshold [47].
The results of the studies on hospital volume and its impact on arthroplasty outcomes are summarized in Fig. 5.

Hospital volume is inversely correlated with complication rate, readmissions, mortality, and other negative outcomes after TJA
Geographic location
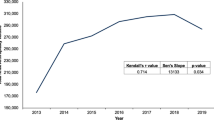
There were 2 studies that assessed the impact of geographic location of the hospital on utilization of TJA. Francis et al. examined utilization rates of TJA in rural vs. urban areas and reported that, compared to urban patients, rural patients were 27% more likely to have THA or TKA (OR 1.27, 95% CI 1.26–1.28) [48]. After adjusting for age, sex, race/ethnicity, median household income, average house value, mean poverty ratio, and state of residence, rural patients were still 14% more likely to have TJA (OR 1.14, 95% CI 1.13–1.16) [48]. Gwam et al. reported that the highest number of TKA procedures were being performed in the Midwest region of the United States (327 procedures per 100,000 in 2014), followed by the Northeast (211), the South (209), and the West (186) [49]. The highest number of primary TKA procedures were being performed in urban, teaching hospitals (45.3%), followed by urban, non-teaching hospitals (42.6%). Rural hospitals had the lowest percentage of primary TKA being performed every year (11.6%) [49].
Discussion
This systematic review reveals several important findings regarding the relationship between insurance type, socioeconomic status, hospital volume, and outcomes in TJA.
The volume of the hospital can significantly affect outcomes after TJA. The results of this review show that hospital volume is correlated with outcomes after TJA—readmissions and ED visits after TJA decreased as hospital volume increased [40,41,42,43,44,45,46,47]. The highest-volume hospitals (>200 arthroplasty procedures annually) have significantly lower rates of mortality, complications, and revisions after primary TJA compared to lower-volume hospitals [40,41,42,43,44,45,46,47].
Another factor shown to affect outcomes after TJA is the patient’s insurance type. The results of this review show that Medicaid and Medicare insurance holders are more likely to have an increased risk of mortality, complications, readmissions, and discharge to institutional care after TJA compared to private/commercial insurance holders [6,7,8, 10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30]. Insurance type may not be a surrogate for socioeconomic status and, instead, represent an independent risk factor for outcomes.
The results of this study show that patients of lower socioeconomic status have less access to healthcare resources and higher readmission risk. Results are inconclusive in determining whether socioeconomic status has an impact on complications, functional outcomes, revisions, or discharge to institutional care after TJA [10, 14, 18,19,20, 23, 24, 31,32,33, 35,36,37,38]. Further studies are needed to delineate the relationship between socioeconomic status and outcomes after TJA.
Geographic location of patients may affect their access to TJA. The results of this review show that rural patients have higher utilization of TJA compared to urban patients, and the highest utilization of TJA is in the Midwest, followed by the South, the Northeast, and the West [48, 49].
This systematic review is subject to certain limitations. One of the weaknesses of this review is the heterogeneity of the data in the included studies. Statistical analysis of continuous variables from different studies was not possible because the included studies utilized different statistical measures (i.e., odds ratio, hazard ratio, relative risk) to report their results. Another limitation of this review is that it included studies with levels of evidence ranging from 1–4. While this ensured that our systematic review was as comprehensive as possible in capturing the effect of all social health determinants on arthroplasty outcomes, this also meant that studies with lower levels of evidence were included, which may weaken the strength of our conclusions.
Nevertheless, this review highlights important relationships between socioeconomic factors and arthroplasty outcomes. The first step in mitigating healthcare inequities is recognizing that disparities exist. Only once this first step is taken can actions items be developed to address the inequities in a patient-centered manner. This review shows that patients with Medicaid insurance, lower income status, and patients being treated at low-volume hospitals, comprise a particularly vulnerable subset. Our study showed that Medicaid holders had less access to orthopedic resources, poorer preoperative functional status, higher mortality and major complication rate, and higher readmission risk, higher rate of discharge to institutional care, and poorer functional outcomes compared to commercial insurance holders after total knee and hip arthroplasty. These findings are similar to the results of a recent study on total shoulder arthroplasty (TSA) outcomes by Singh et al., who showed that Medicaid insurance-holders had poorer outcomes and higher risk of complications compared to commercial insurance-holders after TSA [50]. While our study did not directly explore the reason for the impact of Medicaid insurance status on outcomes after total knee and hip arthroplasty, some possible explanations for this effect have been put forth by prior studies—less access to postoperative healthcare resources, such as physical therapy, reduced choice with respect to choosing providers, poorer preoperative functional status, and higher rates of cigarette use, obesity, and malnutrition among Medicaid insurance-holders [51].
Another key finding of our study is that patients being treated at low-volume hospitals have higher rates of complications, revision, readmission, ED visits, mortality, prolonged length of stay, discharge to institutional care, and poorer functional scores compared to patients treated at high-volume hospitals for total knee and hip arthroplasty. These findings are similar to results by a recent study on TSA outcomes by Singh et al., who showed that patients underwent TSA at low-volume hospital (<15 procedures annually) had higher rate of discharge to institutional care, prolonged hospital stay, postoperative fractures, blood transfusion, and revision compared to those who underwent TSA at higher-volume hospitals (>15 procedures annually) [52]. This relationship between hospital volume and arthroplasty outcomes has been consistently demonstrated across arthroplasty types (hip/knee/shoulder/revision), practice settings, time-periods, and datasets [52]. Some possible explanations that have been put forth for this observed relationship between hospital volume and arthroplasty outcomes include, but are not limited to, streamlined inpatient arthroplasty care, standardized pre-, intra- and postoperative protocols, availability of ancillary staff trained in the specialty care of arthroplasty patients, and better transition of care and discharge planning in higher-volume hospitals [52]. Other possible confounding factors are that patients referred to low-volume hospitals may differ in social support and insurance status compared to those referred to high-volume hospitals. While it creates issues with access to care if all arthroplasty patients were referred only to high-volume hospitals, it is important that patients be made aware of these findings so that they make an informed choice with regards to where they undergo arthroplasty.
Conclusion
This systematic review shows that insurance type, socioeconomic status, hospital volume, and geographic location can have significant impact on patients’ access to, utilization of, and outcomes after TJA.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
References
Cross M, Smith E, Hoy D, et al. The global burden of hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73:1323–30.
Kurtz S, Ong K, Lau E, et al. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg - Ser A. 2007;89:780–5.
Segal DN, Grabel ZJ, Shi WJ, et al. The impact of insurance coverage on access to orthopedic spine care. J Spine Surg. 2018;4:260–3.
Lansdown DA, Ma GC, Aung MS, et al. Do patient outcomes and follow-up completion rates after shoulder arthroplasty differ based on insurance payor? J Shoulder Elbow Surg. 2021;30:65–71.
Harris RP, Helfand M, Woolf SH, et al. Current methods of the U.S. preventive services task force: A review of the process. Am J Prev Med. 2001;20:21–35.
Almaguer AM, Hsu AR, Pearson JM, et al. Do Geographic Region, Medicaid Status, and Academic Affiliation Affect Access to Care Among Medicaid and Privately Insured Total Hip Arthroplasty Patients? J Arthroplasty. 2019;34:2866–71.
Boylan M, Suchman K, Vigdorchik J, et al. Technology-Assisted Hip and Knee Arthroplasties: An Analysis of Utilization Trends. J Arthroplasty. 2018;33:1019–23.
Hanchate AD, Zhang Y, Felson DT, et al. Exploring the determinants of racial and ethnic disparities in total knee arthroplasty: Health insurance, income, and assets. Med Care. 2008;46:481–8.
SooHoo NF, Zingmond DS, Ko CY. Disparities in the utilization of high-volume hospitals for total knee replacement. J Natl Med Assoc. 2008;100:559–64.
Veltre DR, Sing DC, Yi PH, et al. Insurance status affects complication rates after total hip arthroplasty. J Am Acad Orthop Surg. 2019;27:E606–11.
Adelani MA, Archer KR, Song Y, et al. Immediate complications following hip and knee arthroplasty: Does race matter? J Arthroplasty. 2013;28:732–5.
Browne JA, Novicoff WM, D’Apuzzo MR. Medicaid payer status is associated with in-hospital morbidity and resource utilization following primary total joint arthroplasty. J Bone Joint Surg – Am J Bone Joint Surg Vol. 2014;96(1):e180.
Maman SR, Andreae MH, Gaber-Baylis LK, et al. Medicaid insurance status predicts postoperative mortality after total knee arthroplasty in state inpatient databases. J Compar Effect Res. 2019;8:1213–28.
Menendez ME, Ring D, Barnes CL. Inpatient Dislocation After Primary Total Hip Arthroplasty. J Arthroplasty. 2016;31:2889–93.
Plate JF, Ryan SP, Goltz DE, et al. Medicaid Insurance Correlates With Increased Resource Utilization Following Total Hip Arthroplasty. J Arthroplasty. 2019;34:255–9.
Veltre DR, Yi PH, Sing DC, et al. Insurance status affects in-hospital complication rates after total knee arthroplasty. Orthopedics. 2018;41:E340–7.
Xu HF, White RS, Sastow DL, et al. Medicaid insurance as primary payer predicts increased mortality after total hip replacement in the state inpatient databases of California, Florida and New York. J Clin Anesth. 2017;43:24–32.
Arroyo NS, White RS, Gaber-Baylis LK, et al. Racial/Ethnic and Socioeconomic Disparities in Total Knee Arthroplasty 30- and 90-Day Readmissions: A Multi-Payer and Multistate Analysis, 2007-2014. Popul Health Manag. 2019;22:175–85.
Oronce CIA, Shao H, Shi L. Disparities in 30-day readmissions after total hip arthroplasty. Med Care. 2015;53:924–30.
White RS, Sastow DL, Gaber-Baylis LK, et al. Readmission Rates and Diagnoses Following Total Hip Replacement in Relation to Insurance Payer Status, Race and Ethnicity, and Income Status. J Racial Ethn Health Disparities. 2018;5:1202–14.
Lan RH, Kamath AF. Post-acute care disparities in total joint arthroplasty. Arthroplast Today. 2017;3:187–91.
Li Y, Ying M, Cai X, et al. Trends in Postacute Care Use and Outcomes After Hip and Knee Replacements in Dual-Eligible Medicare and Medicaid Beneficiaries, 2013-2016. JAMA Netw Open. 2020;3:e200368.
Singh JA, Cleveland JD. Medicaid or Medicare insurance payer status and household income are associated with outcomes after primary total hip arthroplasty. Clin Rheumatol. 2018;37:2489–96.
Weiner JA, Adhia AH, Feinglass JM, et al. Disparities in Hip Arthroplasty Outcomes: Results of a Statewide Hospital Registry From 2016 to 2018. J Arthroplasty. 2020;35:1776–1783.e1.
Feng JE, Roof MA, Adnan M, et al. Do Patient Point of Entry and Medicaid Status Affect Quality Outcomes Following Total Knee Arthroplasty? J Arthroplasty. 2020;35:1761–5.
Yayac MF, Harrer SL, Janiec DA, et al. Costs and Outcomes of Medicare Advantage and Traditional Medicare Beneficiaries After Total Hip and Knee Arthroplasty. J Am Acad Orthop Surg. 2020;28:e910–6.
Halawi MJ, Cote MP, Savoy L, et al. The Effect of Payer Type on Patient-Reported Outcomes in Total Joint Arthroplasty Is Modulated by Baseline Patient Characteristics. J Arthroplasty. 2019;34:1072–5.
Starring H, Waddell WH, Steward W, et al. Total Knee Arthroplasty Outcomes in Patients with Medicare, Medicare Advantage, and Commercial Insurance. J Knee Surg. 2020;33:919–26.
Lavernia CJ, Lee D, Sierra RJ, et al. Race, ethnicity, insurance coverage, and preoperative status of hip and knee surgical patients. J Arthroplasty. 2004;19:978–85.
Martin CT, Callaghan JJ, Liu SS, et al. Disparity in preoperative patient factors between insurance types in total joint arthroplasty. Orthopedics. 2012;35. Epub ahead of print. https://doi.org/10.3928/01477447-20121120-27.
Dangelmajer S, Yang A, Githens M, et al. Disparities in Total Hip Arthroplasty Versus Hemiarthroplasty in the Management of Geriatric Femoral Neck Fractures. Geriatr Orthop Surg Rehabil. 2017;8:155–60.
Skinner J, Zhou W, Weinstein J. The influence of income and race on total knee arthroplasty in the United States. J Bone Joint Surg - Ser A. 2006;88:2159–66.
Hawkins K, Escoto KH, Ozminkowski RJ, et al. Disparities in major joint replacement surgery among adults with medicare supplement insurance. Popul Health Manag. 2011;14:231–8.
SooHoo NF, Farng E, Zingmond DS. Disparities in the utilization of high-volume hospitals for total hip replacement. J Natl Med Assoc. 2011;103:31–5.
Bass AR, Mehta B, Szymonifka J, et al. Racial Disparities in Total Knee Replacement Failure As Related to Poverty. Arthritis Care Res. 2019;71:1488–94.
Inneh IA, Clair AJ, Slover JD, et al. Disparities in Discharge Destination After Lower Extremity Joint Arthroplasty: Analysis of 7924 Patients in an Urban Setting. J Arthroplasty. 2016;31:2700–4.
Goodman SM, Mandl LA, Parks ML, et al. Disparities in TKA Outcomes: Census Tract Data Show Interactions Between Race and Poverty. Clin Orthop Relat Res. 2016;474:1986–95.
Singh JA, Lewallen DG. Income and patient-reported outcomes (PROs) after primary total knee arthroplasty. BMC Med. 2013;11. Epub ahead of print. https://doi.org/10.1186/1741-7015-11-62.
Anis HK, Mahmood BM, Klika AK, et al. Hospital Volume and Postoperative Infections in Total Knee Arthroplasty. J Arthroplasty. 2020;35:1079–83.
Adelani MA, Keller MR, Barrack RL, et al. The Impact of Hospital Volume on Racial Differences in Complications, Readmissions, and Emergency Department Visits Following Total Joint Arthroplasty. J Arthroplasty. 2018;33:309–315.e20.
Doro C, Dimick J, Wainess R, et al. Hospital Volume and Inpatient Mortality Outcomes of Total Hip Arthroplasty in the United States. J Arthroplasty. 2006;21:10–6.
Hollenbeck B, Hoffman MA, Tromanhauser SG. High-Volume Arthroplasty Centers Demonstrate Higher Composite Quality Scores and Enhanced Value: Perspective on Higher-Volume Hospitals Performing Arthroplasty from 2001 to 2011. J Bone Joint Surg – Am Vol. 2020;102:362–7.
Koltsov JCB, Marx RG, Bachner E, et al. Risk-based hospital and surgeon-volume categories for total hip arthroplasty. J Bone Joint Surg – Am Vol. 2018;100:1203–8.
Laucis NC, Chowdhury M, Dasgupta A, et al. Trend toward high-volume hospitals and the influence on complications in knee and hip arthroplasty. J Bone Joint Surg – Am Vol. 2016;98:707–12.
Manley M, Ong K, Lau E, et al. Total Knee Arthroplasty Survivorship in the United States Medicare Population. Effect of Hospital and Surgeon Procedure Volume. J Arthroplasty. 2009;24:1061–7.
Singh JA, Kwoh CK, Boudreau RM, et al. Hospital volume and surgical outcomes after elective hip/knee arthroplasty: A risk-adjusted analysis of a large regional database. Arthritis Rheum. 2011;63:2531–9.
Wilson S, Marx RG, Pan TJ, et al. Meaningful thresholds for the volume-outcome relationship in total knee arthroplasty. J Bone Joint Surg – Am Vol. 2016;98:1683–90.
Francis ML, Scaife SL, Zahnd WE, et al. Joint replacement surgeries among medicare beneficiaries in rural compared with urban areas. Arthritis Rheum. 2009;60:3554–62.
Gwam C, Rosas S, Sullivan R, et al. The Who, What, and Where of Primary TKAs: An Analysis of HCUP Data from 2009 to 2015. J Knee Surg. 2020;33:378–86.
Singh JA, Cleveland JD. Insurance Payer type and Income are associated with outcomes after total shoulder arthroplasty: Insurance payer, Income and Shoulder Arthroplasty outcomes. J Rheumatol. 2020;47:589.
Lakomkin N, Hutzler L, Bosco JA. The Relationship Between Medicaid Coverage and Outcomes Following Total Knee Arthroplasty: A Systematic Review. JBJS Rev. 2020;8:e0085.
Singh JA, Ramachandran R. Does hospital volume predict outcomes and complications after total shoulder arthroplasty in the US? Arthritis Care Res (Hoboken). 2015;67:885–90.
Acknowledgements
Not applicable.
Ethical committee approval
This systematic review of the literature did not require approval from the Biomedical Institutional Review Board of The Ohio State University.
Funding
None.
Author information
Authors and Affiliations
Contributions
PAM, JAM, and SPV performed the article search and selection and drafted the manuscript. SPV, AIS, CAK, MP, and ML revised the manuscript for important intellectual contents. SPV served as corresponding author and created the figures and tables. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Study performed at the Department of Orthopaedics, The Ohio State University Wexner Medical Center.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alvarez, P.M., McKeon, J.F., Spitzer, A.I. et al. Socioeconomic factors affecting outcomes in total knee and hip arthroplasty: a systematic review on healthcare disparities. Arthroplasty 4, 36 (2022). https://doi.org/10.1186/s42836-022-00137-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42836-022-00137-4