
Abstract
Background
Traditional Chinese food has been believed to be closely associated with affecting salubrious health outcomes, enhancing longevity, and interoperating with traditional Chinese medicine. Over the past several decades, traditional Chinese food has been going through significant evolution and qualitative transition of nontraditional eating behaviors. This food transition and eating pattern transformation are propelled by China’s vast population size, rapid socioeconomic development, lifestyle changes, and global influence. Inevitably, these dietary shifts are having a considerable impact not only on public health in China but also globally.
Purpose
The purpose of the present study is to examine the socioeconomic and health effects of the shift from consuming traditional Chinese food into increasingly consuming Western-style processed foods, fast foods, saturated fats, snacks, sugary beverages, and eating out more often than the traditional home cooking. This study also investigates the prevalence, health effects, and sociodemographic implications of food transition and adopting Western-style eating patterns.
Methods
Cross-sectional analysis of primary data collected from 1292 adult male and female participants was performed. Participants responded to a cross-sectional self-administered paper-and-pencil-based food history and beverage intake questionnaire. Chi-square analyses were employed to analyze data obtained from the nonparametric variables, whereas t tests were performed to analyze data obtained from the parametric variables.
Results
There were significant differences in snack food shopping distributions between gender and marital status factors. Females were more likely to purchase more snacks than males, whereas singles were more likely to purchase more snacks than married. Pooled data suggest that 79.67% of the respondents consumed fast food with wide-ranging frequencies. There were significant differences between water and all other typical drinks, as water recorded the highest consumption rate by 65.31%. There were significant differences between the three meal-eating locations, as 48.45% of the respondents were more likely to consume most of their daily meals at home, whereas, combined, 51.55% were more likely to consume most of their daily meals out-of-home. Baking food scored 77.94% compared with all other food preparation methods. Overall healthy eating behaviors results indicated that 49.67% of the respondents consumed a healthy diet most of the time, whereas combined, 50.33% either consumed a healthy diet sometimes or not at all.
Conclusions
Traditional Chinese eating practices have been transitioning into nontraditional eating behaviors that may be associated with a multitude of chronic non-communicable diseases and high mortality rates. As these rates have been projected to continue rising, there is a need to focus on introducing public health promotion policies, including health education and lifestyle-enhancing initiatives aimed at promoting nutritive balance and adopting healthier eating behaviors. These policies can be tailored to support the most affected groups among the lower- and middle-income Chinese, as well as similar populations in developing countries.
Similar content being viewed by others

Introduction
Over nearly 5000 years and more than thirteen imperial dynasties, traditional Chinese food has evolved from a rudimentary style in a primitive society to sophisticated gastronomic art and science in contemporary society. Traditional food is a quintessential symbol of Chinese culture and identity, and it occupies a unique status that far exceeds its economic and nutritional values. Traditional Chinese food can be dated back to 770–476 BC when the Chinese began to consume foods obtained from home-cultivated milled cereal grains such as rice, whole wheat, and barley. Regardless of its duration and food styles, traditional food and eating habits of any culture are invariably susceptible to eventually evolve beyond their time and geographical space. Food made from milled grains, especially wheat and barley in northern China was a staple ingredient in meeting the dietary needs of people by making various types of noodles, dumplings, stuffed buns, and pastry. Conversely, rice was the staple ingredient in making rice-based foods to meet the dietary needs of Chinese living in the southern regions of the country. As a sign of an early natural dietary evolution, the northern-cultivated wheat and barley found their way down to the south, whereas rice and rice-based food products proliferated from the south up to the north, and eventually burgeoned throughout the rest of the country making a significant contribution to the shaping of the Chinese dietary culture and longstanding eating traditions. The traditional Chinese food culture is no exception as it faces the unavoidable challenges of natural evolution and social changes. For some cultures, these challenges might also present unexplored opportunities for innovation, growth, and positive changes. One of the most influential factors in the transition of traditional food is the massive contemporary urbanization of the vast Chinese rural territories. The steady influx of rural migrants into urban cities seeking better employment opportunities had a significant influence on the evolution of traditional dietary behaviors during the 1980s and 1990s. This rapid dietary evolution led to the emergence of a raft of new diseases related to the adoption of novel dietary behaviors. Several researchers identified urbanization as a major driving force in the expansion of an emerging pandemic of food transition associated with chronic non-communicable diseases (NCDs) among urban city inhabitants. Research findings showed that within 10 years (1994–2004), the production of cooking oil increased by nearly 50%, which was chiefly driven by low prices and rising in the average household income of low- and middle-class Chines. According to these research findings, this transition from a traditional rural-style diet to a more urban-adapted diet may contribute to higher risks of diet-related NCDs [1,2,3,4,5,6,7,8].
As a nutrition transition model, the term “nutrition transition” was conceived by [9] in 1993. The term describes the model as an alteration in food intake and energy expenditure, which is measured by the number of calories spent daily based on the Total Daily Energy Expenditure (TDEE) equation. According to this model, nutrition transition typically follows demographic, socioeconomic, and epidemiological changes. Particularly, the term is employed to describe food consumption transition patterns in developing countries through shifting from consuming traditional indigenous diets that are high in whole grains, vegetables, fruits, and dietary fiber to increasingly consume Western-style diets that are high in simple sugars, saturated fat, processed carbohydrates, and animal-based foods. Recent research by [10] identified significant environmental and climate impacts on dietary changes across food systems over the last 10 years. These impacts include under-nutrition, household food insecurity, child malnutrition, environmental health, issues, and inadequate access to healthcare services. Therefore, the existing nutrition transition phenomenon necessitates a socio-anthropological examination of the current food supply chain. Especially, reexamining the environmental and health impact of the high consumption of animal-sourced foods. The India and France model of de-animalization of food sources advocates for considering finding an alternative approach to food and nutrition transitions [11]. These environmental and food security impacts on the global food systems are consistent with the nutrition transition models proposed by [9,10,11]. Rapid environmental and food transition impacts are commonly occurring in countries that are going through significant economic and sociodemographic developments. Although impacted differently by nutrition and food transition, among these affected countries are China, Brazil, and India.
Research by [12] suggested that there is a need to learn more about the influences of the interaction of nutrition transition, dietary behavior, and demographic changes on the development of lifestyle-related conditions in China, where the dietary patterns differ greatly from those of the Western populations. According to [9], the dynamic shifts in increased caloric intake from poor diets coupled with physical inactivity patterns lead to higher rates of lifestyle-related NCDs. As one of the countries impacted by the effects of nutrition transition, whereas China has made significant progress in managing food insecurity and nutrition transition as defined by [9], it is still facing many challenges in connection with diet-related NCDs because of the demographic, economic, and epidemiological changes it has been experiencing during the last several decades. Several studies examined the effects of the intersection of the factors of social and economic transformation with the shifts in dietary patterns and nutritional status in China, particularly in urban environments [13, 14]. Research by [15] reported high rates of prevalence of diseases among the ethnic minority groups in rural areas in China [15]. attributed several contributing factors chiefly among them are indigenous social customs, cultural-specific traditions, variations in food consumption, healthcare access disparities, level of education, and genetic backgrounds. Moreover, [15] suggested that the ethnic backdrop and socioeconomic status of the rural ethnic groups represent the major contributing factors to the health disparity between the Chinese ethnic minority groups and the Chinese Han ethnic majority group. Consistent with the findings by [15, 16] found that rural disparity in healthcare among minority Chinese who had less access to healthcare facilities and visited physicians considerably fewer times than those minority Chinese living in urban settings. These findings indicated that there is a need to further examine the effects of nutrition transition as described by [9] in China in the under-researched and under-served minority ethnic populations. A study by [17] suggested that food functions not only as a source of nutrition for humans, but also contributes in different ways to people’s daily life, their beliefs, and socioeconomic needs. Further, [9] argued that there is a relationship between food and human health, as the nutrients that people obtain from different food sources, their eating behaviors, and food choices may directly affect the nutrient intake and its health implications for people. Food choices and eating behavior are not only associated with negative health outcomes, but can also be influenced by cultural, socioeconomic, and geographical factors such as the various effects of migration from rural to urban settings. Understanding the interplay of these factors can be conducive to preventing diet-related diseases and improving the health and longevity of people, which has been one of the goals of the traditional Chinese diet.
The historical evolution of Chinese food reveals that since the inception of the Zhou eating protocol system during the Zhou Dynasty (1047 BC–256 BC), the Chinese eating behavior was regarded as a “social ritual.” This ancient eating etiquette was one of the expected customary social characteristics of the ancient Chinese food culture that originated as a form of religious rites by offering food and fruits to deities, departed ancestors, and ghosts. Relatedly, Confucius (551–479 BCE), a Chinese philosopher and teacher who was recognized for establishing a dietetic culture by developing proper culinary techniques and special eating etiquettes. Although they are becoming nearly extinct, his teachings regarding food preparation methods and eating mannerisms are still considered an essential constituent of Chinese traditional food culture [18]. However, like many ancient cultural phenomena, over time, the Chinese food culture is no longer able to circumvent the eventual transmutation [2]. With the inevitable socioeconomic and cultural evolutions, traditional food cultures must adapt to the new challenges of the emergence of the contemporary food culture to satisfy the demands of the modern lifestyle of the consumers they cater to [19]. The processed food, fast food, and soft beverage industries are increasingly targeting the growing young adult populations in the lucrative Asian markets with ultra-processed food advertisements [20].
One of the instrumental factors that facilitated nutrition transition and changes in traditional dietary habits over time was that the Chinese people are not stringently nationalistic to the extent of totally resisting imported foreign food ingredients. Throughout Chinese food history, foreign foods have found their way to China in a myriad of ways and were readily accepted to be amalgamated within the native Chinese food culture. Moreover, traditional Chinese food is prodigiously diverse and is a presentation of a mélange of extraterritorially imported and regional food cultures. Whereas it is locally originated and produced, traditional Chinese food has long been influenced and characterized by several factors, including the enormous diversity of food sources, diversity of physical and human geographies, distinct socio-ethnic food traditions, and faith-based food traditions [18]. For millennia, employing food as a modality of “food therapy” or “medical diet therapy” in the field of traditional medicine to preserve health and improve lifespan, which is believed to be achieved by maintaining a balance between the “Yin” or “receptive” and the “Yang” or “active” through the proper combination of nutrition and medicine. This has been an important function of the Chinese traditional food culture that made it more enduring throughout the centuries [21,22,23]. During prehistoric times, goat, sheep, and wheat were brought to China from Western and Central Asia, whereas various fruits and vegetables found their way to China during the Han Dynasty (206 BC-220 AD) and Tang Dynasty (618–906 AD). Further, sweet potatoes and peanuts were transported by mariners during the Ming Dynasty (1368–1644 AD). Through the overland Silk Road trade routes (Fig. 1), pomegranates, lima bean, watermelon, muskmelon, carrot, fennel, grapes, celery, and other spices came to China through Central Asia into the Xinjiang Uygur territories in western China. These foreign food imports were fully assimilated into traditional Chinese foods [1, 24]. Similarly, through the overland and maritime trade routes (Fig. 1), exotic animals and foods were transported into China, which enriched the diversity of Chinese gastronomies. Only a few of them maintained their foreign provenance. Coriander, onions, peas, and sesame seeds were also imported from Bactria, an ancient region in Central Asia. Whereas cucumber entered China from Western Asia during the Han Dynasty [25, 26]. Red hot chili peppers, an indispensable spice ingredient that transformed the contemporary Chinese culinary culture and can be found ubiquitously across the celebrated regional cuisines, were incipiently introduced to China by the Portuguese sailors through voyaging the Indian Ocean and South China seashores in the 1570s (Fig. 2) [27]. During the Tang Dynasty, almonds, figs, sugar beets, spinach, and lettuce were transported into China by traders and migrants from the Middle East, Western, and Central Asia, particularly from Turkey, Iran, and North Africa. As an earlier indication of the adaptation to foreign food ingredients, during the Han Dynasty, Chinese chefs accepted foreign cooking styles and modified indigenous milled wheat and barley flour to make the first noodles and cakes. Similarly, early Chinese cooks were willing to adapt to and learn from other ethnic food cultures and modify them to appeal to Chinese palates (Table 1).

The Ancient overland Silk Road (depicted in red lines) and maritime Silkroad (depicted in blue lines) trade routes map. Source: Ancient History Encyclopedia, retrieved from https://www.ancient.eu/image/8327/map-of-the-silk-road-routes/, March 2018

Red hot chili peppers that transformed the contemporary Chinese culinary culture were incipiently introduced to China by the Portuguese sailors in the 1570s. Reprinted from Tomas Castelazo, retrieved from www.tomascastelazo.com / Wikimedia Commons. Created: January 15, 2012
In addition to red hot chili peppers, two of the most omnipresent ingredients in traditional Chinese food are ginger and garlic. They are essential cooking spices featured in most of the cuisine recipes throughout China. However, neither of the tangy-flavored ginger nor the pungent-flavored garlic plants is native to China. Both plants were integral ingredients of the diet of several ancient food cultures. Garlic can be traced back to 3200 BC in ancient Egypt, where the workers who built the pyramids were provided with a steady diet of garlic to stimulate them to summon up enough stamina to continue enduring constructing the Great Pyramid of Cheops, which took 20 years to build. In the Roman Empire, garlic was used to feed the gladiators ahead of their fighting contests. Furthermore, historic evidence showed that ceremonial banquets in the Medieval era provided raw garlic, which was employed as a prophylactic against the plague. There is a long-held belief in Chinese food culture that garlic and ginger contribute to a myriad of therapeutic benefits to cure ailments ranging from the common cold, respiration, and leprosy to treating gastrointestinal disorders and parasitic infestation. This herbal medicinal belief might explain the importance and ubiquity of garlic and ginger as essential ingredients in both the Chinese culinary culture and nontraditional medicine practice [28, 29]. Ultimately, this adaptability and intercultural food exchange approach has shaped and facilitated the evolution of the contemporary Chinese culinary culture and led to adopting nontraditional eating patterns such as consuming Western-style fast foods, as the present study aims to examine [30, 31].
Over the past few decades, modern lifestyle changes coupled with diminishing leisure time and physical activity have propelled the transition from traditional Chinese full-service food in restaurants to more convenient fast-food eateries. One of the most notable shifts in Chinese consumer eating behavior is the prevalence of Western-style fast-food restaurants throughout China. Market research reported that consuming fast food has been increasingly growing among the Chinese, especially the younger generations. Fast-food consumption has been linked to high rates of NCDs caused by increased caloric intake, saturated fat, trans-fats, sugar-sweetened beverages, and sodium [32]. Due to the lack of a scholarly consensus on the precise definition of fast food, in this study, it is broadly described as the kind of processed food that is readily prepared and served promptly upon request to customers in restaurants or snack kiosks to be eaten as a quick meal on the restaurant’s premises or carried away. Fast-food restaurants are also referred to as “quick-service restaurants,” where customers order food and beverage items and, in most instances, customers pay before eating. Foods provided by fast-food restaurants include both Chinese and Western-style fast foods. In China, Western fast-food restaurants are predominantly from the USA, including trademarks such as McDonald’s, Burger King, Kentucky Fried Chicken (KFC), and Pizza Hut. Since its introduction to the Chinese market in the 1980s, the fast-food business in China has been enjoying an annual growth rate of nearly 15%. According to market research, the number of fast-food Western-style and fast-food Chinese eateries in China is nearly two million and has been exceedingly expanding across the country [33,34,35].
Materials and methods
Diet History Questionnaire development and procedures
Participants in the present study were 1292 Chinese adults aged 18 years and older, including 720 (55.73%) males and 572 (44.27%) females. Participants responded to a modified cross-sectional self-administered paper-and-pencil-based food history and beverage intake questionnaire. Among others, the questionnaire comprised of nontraditional food and beverage consumption, including Western-style fast food, snacks, and beverages. As a survey research methodology, questionnaires are frequently employed to gather predetermined information regarding a population cohort of interest. The study implemented an adapted version of the National Cancer Institute (NCI) Diet History Questionnaire III (DHQ III) for adults 19 years of age or older. DHQ III is based on a compilation of the national dietary intake recall data from the National Health and Nutrition Examination Surveys (NHANES). Several studies suggested that employing a Food Frequency Questionnaire (FFQ) to obtain the frequency and portion size information concerning food and beverage intake over a designated time, ranging from the past 24 h, a month, or a year is an effective instrument for estimating food and beverage intake of a population of interest [36,37,38]. In the present study, the adapted FFQ encompassed 31 closed-ended questions [39, 40] to obtain relevant data from the respondents to determine their food intake behaviors, frequency consumption history, healthy eating habits, sociodemographic data, including age, gender, education level, marital status, and employment status. Respondents were unpaid volunteers randomly selected from nine cities in the Yellow River Central Plains, Northwestern, Midwestern, and Southeastern regions of China.
Study population inclusion and exclusion criteria
Participants were randomly selected from nine Chinese cities. Participants who qualified for inclusion in this study were a cohort of 1292 adult males and females between the ages of 18 years and older, including all ethnic group associations, all levels of education, and all marital status categories. Participants whose ages were outside the study age range of 18 years and older were excluded from participating in the study. Further, the preexisting health conditions, medical history, and current health status of the participants were excluded from this study.
Statistical analysis
In the present study, qualitative cross-sectional data analysis was performed utilizing primary data sources collected from study participants’ responses to a modified version of the DHQ III and FFQ, which was designed to examine the transition in dietary behaviors among Chinese adults. The Statistical Analysis Software (SAS) Package, Version 9.3 was utilized to analyze the obtained data. Chi-square distribution analyses were implemented to analyze data obtained from the nonparametric variables, whereas t tests were performed to analyze data obtained from the parametric variables. Predominantly, the statistical analyses involved calculating p-values and designating any value of a test statistic with a p value of less than an alpha level of 0.05 as statistically significant.
Results
Snack food shopping patterns (SFSP)
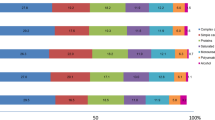
As can be observed in Fig. 3, the snack food shopping pattern (SFSP) results indicate that there were significant differences between the snack shopping patterns. Further, the results show that there were wide-ranging differences in the snack shopping patterns recorded by the respondents where, as nontraditional Chinese food, 34.68% purchased snacks once per week, whereas 25.62% purchased snacks once per month. All-encompassing, the compressed snack shopping data indicate that 46.4% purchased snacks fewer than three times per week, whereas 41.28% purchased snacks three or more times per week. Combined, 87.68% the preponderance of respondents reported purchasing snacks either fewer than three times per week or three or more times per week. Conversely, 12.32% reported never purchasing snacks.

Depicts the probability (%) of snack food shopping frequency reported by respondents. Key: 1 T/day: snack food shopping pattern (SFSP) once/day, 2 T/day: SFSP twice/day, 1 T/week: SFSP once/week, 2 T/week: SFSP twice/week, 3 T/week: SFSP three times/week, 1 T/month: SFSP once/month, 3+T/week: compressed SFSP data for three or more times/week
Demographic factor differences in snack food shopping patterns
Gender (male vs. female) differences in snack food shopping
The results of snack food shopping patterns reported by the male and female respondents are presented in presented Fig. 4. There were significant differences in snack shopping behaviors between male and female respondents. Females reported a higher frequency of snack shopping with a rate of 61.54%, and they were more likely to purchase more snacks than their male counterparts. Juxtaposing, males reported a lower frequency of snack shopping with a rate of 38.46%, and they were more likely to purchase fewer snacks than their female counterparts.

Displays the probability (%) of snack food shopping frequency by gender (male vs. female) and marital status (married vs. single) reported by respondents
Marital status (married vs. single) differences in snack food shopping
The marital status results of snack food shopping patterns reported by the married and single respondents indicated that there were significant differences in snack food shopping behaviors between married and single respondents. Single respondents reported a higher frequency of snack food shopping with a rate of 59.48%, and they were more likely to purchase more snacks than their married counterparts. In comparison, married respondents reported a lower frequency of snack food shopping with a rate of 40.52%, and they were more likely to purchase fewer snacks than their single counterparts.
Fast-food consumption patterns
As presented in Fig. 5, there were significant differences between the results of the fast-food consumption pattern among respondents. The highest consumption rate reported by respondents was consuming fast food once per week by a rate of 28.92%, whereas 15.57% reported consuming fast food once per day, which is closely followed by twice per week with a rate of 14.02%. On the other hand, 20.33% of respondents reported never consuming fast food. As nontraditional Chinese food, combined, these results reveal that 79.67% of the respondents reported consuming fast food with varied frequencies ranging from once per day, once per month, and somewhere in between as stated in Fig. 5.

Denotes the probability (%) of the fast-food consumption pattern reported by
respondents
Typical drink consumption patterns
As can be viewed in Fig. 6, there were significant differences between the typical drink beverage consumption patterns among the respondents. As a leading typically consumed drink beverage by a wide margin, water registered the highest rate of consumption with 65.31%, followed by green tea with 11.16%, milk was the third consumed as a typical drink with 8.32%, whereas other kinds of teas recorded 4.26%, and black tea came in last with 1.42%. Soda consumption, which is not typically a traditional Chinese drink beverage, was reported with a rate of 4.87%. Juice (2.03%) and coffee (1.42%) were far behind among the least consumed typical drink beverages reported by respondents. These results further show that all kinds of tea (green, black, and other types of tea) recorded the second-highest rate of beverage consumption with 16.84% making tea the second most consumed typical beverage reported by respondents. When excluding water, collectively, the non-artificially sugar-sweetened beverages were 29.82%.

Illustrates the probability (%) of consuming typical drinks reported by respondents
Location of eating most of the daily meals patterns (home vs. other locations)
The results of the statistical analysis of the location of eating most of the daily meals (at home, at work/dorm, or out/restaurants) are portrayed in Fig. 7. The findings indicate that there were significant differences between the three locations of eating most of the daily meals. Concerning the eating at home location, 48.45% of the respondents consumed most of their daily meals at home, whereas 29.85% consumed most of their daily meals at work or dormitories, in juxtaposition, 21.7% of respondents indicated that they consumed most of their daily meals out at either street food vending stands or sit-down restaurants. Amalgamated, 51.55% of the respondents were more likely to consume most of their daily meals out of the home at either at work refectory or dormitory cafeterias by a ratio of 29.85% or eating out at street food vending stands or sit-down restaurants by a ratio of 21.7%.

Describes the probability (%) of the location of consuming most meals reported by respondents
Healthy eating behavior patterns: baked vs. fried food and eating healthy vs. unhealthy diets
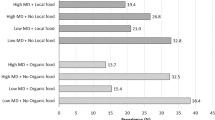
The results obtained from the analysis of healthy eating behavior patterns, including baking vs. frying food and eating healthy vs. unhealthy diets, show there were significant differences between baking vs. frying food, on one hand, eating healthy vs. unhealthy diets on the other hand. The respondents registered baking food by 77.94%, whereas frying food by 22.06%. Regarding consuming a healthy diet most of the time, 49.67% of the respondents indicated that they consumed a healthy diet, juxtaposed, 37.13% consumed a healthy diet sometimes, whereas 13.2% of them did not consume a healthy diet most of the time. Pooled together, 50.33% either consumed a healthy diet sometimes or not at all. As notable healthy eating patterns, the results further reveal that there is statistical proximity between frying food with a rate of 22.06% and not consuming a healthy diet with a rate of 13.2%.
Discussion
The current study presented evidence that the transition of traditional food and eating behaviors can be dated back centuries ago. Throughout Chinese food culture history, gradually, foreign food ingredients have found their way into China through a multitude of ways and were readily accepted to be amalgamated within the traditional Chinese food culture. This food transition and alteration in eating behavior has been associated with the emergence of numerous chronic non-communicable diseases (NCDs) that are caused or exasperated by dietary factors.
One of the stated aims of the present study is to examine the effects of food transition and changes in eating behavior on the prevalence, health outcomes, and sociodemographic implications of food transition and adopting Western-style eating patterns in Chinese adults. A considerable body of research presented evidence-based epidemiological data of the association between chronic NCDs and poor dietary habits, which are associated with nutrition and sociodemographic transition, coupled with adopting an insalubrious lifestyle. In its 2014 Global Status Report on Non-Communicable Diseases, the World Health Organization (WHO) stated that NCDs were responsible for 38 million (68%) of the world’s 56 million deaths in 2012. Predominantly, 82% of the premature mortality rates occur in low- and middle-income countries where there is significant nutrition transition and shift in nutrition and eating behaviors [41]. An estimated 82% of China’s morbidity and mortality burden is attributable to rising NCDs rates, and if not mitigated, this rate is estimated to increase over time [42]. Among other contributing factors to the development and rising rates of NCDs are dietary behavior changes with an emphasis on consumption of animal and trans fatty acids, increased intake of processed foods, decreased dietary fiber intake, coupled with leading a sedentary lifestyle [43,44,45].
The findings of the present study showed that the millennia-old traditional Chinese food patterns have been undergoing significant nutrition and eating behavior transitions. As the study results suggest, this transition has contributed to significant shifts from consuming traditional food into increasingly consuming contemporary Western-style food and beverages as reported by the adult Chinese study participants. According to their responses as a combined study population, the participants reported that they were more likely to consume food and beverages that are consistent with nontraditional Chinese eating behavior patterns, including purchasing snack foods with various time frequencies and consuming Western-style fast food. The results also showed that the participants reported consuming water with a higher rate of 65.31%, juxtaposed with 4.87% consuming nontraditional drinks such as refined sugar-sweeten soda. As suggestions of food transition and shifts in eating behaviors, the results revealed that 51.55% of the participants reported consuming most of their daily meals outside of the home, and combined, 72.35% reported either not eating a healthy diet most of the time, eating healthy diet sometimes, or eating fried food most of the time.
Snacking is one of the key eating behavior indicators of the transition of the traditional eating behaviors that have developed in China in the past 15 years [45]. There is no consistent and specific scholarly definition of “snack food,” and whether eating a “snack” is considered as an extra “small meal” or a “snack.” Therefore, a “snack” in this study’s modified version of the DHQ III and FFQ is self-defined by the study respondents, and it was up to them to make that determination. In China, however, a “snack” is typically an extra eating behavior that occasionally occurs outside of the traditional mealtimes of breakfast, lunch, or dinner [45]. The findings obtained from the current study indicate the consumption of snack foods with various prevalence intervals ranging from three times or more per week to three times or fewer per week. Consistent with these findings, research by [46] reported an increase in the prevalence rates of snacking among young Chinese adults, which was comparable to those rates found in similar findings in a US young adult population. Further, research by [46] expounded that the reason for this prevalence of snack consumption was possibly the result of lower-income levels and differences in the participants’ respective cultural backgrounds. Customarily, consuming regular traditional Chinese meals is favored by Chinese over unplanned snack foods. Western-style snacking in China is not a traditional eating behavior that is typically consumed outside of the preferred normal mealtimes of breakfast, lunch, or dinner [45]. The findings of this study are consistent with this explanation as they reveal the sporadic prevalence of snack shopping reported by the current study’s respondents. Moreover, as the other dietary behaviors are rapidly evolving, snack consumption behavior among the Chinese population is shifting as well. In line with the above-stated findings, several different but cognate studies found similar findings in a US sampled adult population and school-aged children who purchased snacks from school cafeterias. These findings also suggest that snack consumption increased substantially for both females and males, as the snack package sizes increased as well. However, energy-dense snack food consumption did not seem to influence body weight or change percent body fat (BF%) of the students during their adolescent years [47,48,49,50].
Fast-food consumption in China is another evidence of the transition of traditional food and eating behaviors that have been increasingly rising [51]. Multiple factors can be attributed to this upsurge in fast food consumption. Among the factors that stimulated the increased demand for fast food are the convenience and speed of fast-food service, drive-through and take-out amenity, food safety assurance, growing middle-class income, fast-food market deregulation, new food brand tends, global trade liberalization, and relatively affordable prices. A multitude of epidemiological studies presented evidence-based data linked the increased consumption of fast food with increased rates of NCDs, including cardiovascular, disease, obesity, hypertension, and risk of developing type 2 diabetes [33, 35, 51,52,53]. As non-traditional Chinese food, findings from the current study showed that combined, 79.67% of the respondents reported consuming fast food with varied prevalence ranging from once per day, once per month, and somewhere in between (Fig. 5). These findings are compatible with findings found by [53], who posited that nearly 51.9% of the Chinese children often consumed Westernized fast food, and close to 43.6% consumed Chinese fast food over the past three months. In line with the results in the current study, findings from a US-based study showed that nearly 80% of adults in the State of Michigan frequented fast-food restaurants at least once per month, and 28% frequented them regularly more than two times per week. Regular fast-food consumption was found to be higher in younger adults, chiefly males; however, these rates of fast-food consumption were not significantly associated with sociodemographic factors such as the level of education, household income, race, or urbanization [54].
As an essential nutrient, a healthy beverage intake is necessary for maintaining good health throughout the lifespan. In 2015, [55] issued an explicit recommendation to reduce sugar consumption to less than 10% of the total daily energy intake and if possible, below 5% of the total daily energy intake for both adults and children. One of the common sources of simple carbohydrates (sugar) can be found in sugar-sweetened beverages, which have been associated with a multitude of NCDs, including hyperglycinemia, kidney stones, obesity, type 2 diabetes, and the onset of metabolic syndrome. An inadequate intake of plain water is linked to dehydration and increased risks of chronic kidney disease, impairment of physical activity, and disturbance of cognitive functioning [56,57,58,59]. In the current study, the water intake reported by the respondents can be described as a higher intake with 65.31% juxtaposed with all other beverages. Notably, when excluding water, the non-artificially sugar-sweetened beverages combined were the second-highest consumption with 29.82% of the total beverage intake. In comparison, soda consumption accounted for a small proportion of total beverage intake with a rate of 4.87% (Fig. 6). These findings indicate that non-artificially sugar-sweetened beverages can be described as healthy fluid consumption behavior. Previous investigations on fluid intake in China and other countries arrived at similar consistent findings. Research conducted on water and other beverages intake in thirteen countries in three continents, including China [60] were consistent with those in the present study where a high intake of water intake was reported. The relatively high water intake in the present study can be explained by the fact that the study was conducted during the summer months, where people are more likely to consume more water to stay hydrated and cope up with the summer warm weather. This explanation was in line with the high volume of water intake found in some of the thirteen-country studies, where environmental temperatures and seasonal weather variations influenced both the volume and choice of beverages consumed. Inconsistent with these findings, in a cognate study in China, a sizable proportion of the participants did not meet both quantitative and qualitative fluid intake requirements prescribed for urban settings. Only less than 50% of children, 30% of adolescents, and 25% of adults reached the amount of adequate water intake, which might make them more susceptible to underhydration and other adverse health effects [61].
Concerning the location of eating most of the daily meals (home vs. other locations), the findings from the current study showed that nearly less than a half of the participants (48.45%) indicated that they consumed most of their daily meals at home, juxtaposed with slightly over half (51.55%) who indicated that they consumed most of their daily meals at an out-of-home home location (Fig. 7). Regular consumption of meals away from home, particularly at fast-food eateries, has been associated with increased risks of NCDs. In the US, research findings suggested that this trend has been steadily growing since the 1970s [54]. Research findings postulated that regularly eating out of the home may adversely influence healthy eating behaviors, affect food choices, and total daily energy intake balance. Further, regularly eating out of the home may contribute to poor diet quality, overconsumption of food due to larger portion sizes, buffet-style open-ended dining, increased selections of high-calorie-dense foods, availability of foods with a variety of preferred tastes, and increased consumption of foods with high sodium content [62,63,64,65,66]. The findings in the present study were closely consonant with findings from a similar study in Shanghai, China, where the percentage of consuming out-of-home meals was 55.1%, compared with 51.55% in the present study. Similar but different research on the prevalence of dining out of home in China found that the frequency of eating out was relatively higher among college students. In this research, females reported a higher prevalence of eating out than their male counterparts during weekdays. Having an occasion to go out and meet friends was one of the main reasons to eat out by 56.0% [67].
The association between cooking methods and healthy eating behaviors is an important health issue to investigate to better understand if there is a cause-effect relationship between them. The present study examined the respondents’ healthy eating behavior patterns as practiced through baking vs. frying food and overall eating healthy vs. unhealthy diets most of the time. Several studies found that deep frying dark browning food can form acrylamide. Acrylamide is a harmful organic chemical substance that can develop from cooking some foods, especially carbohydrates when utilizing high temperature, including deep-frying, baking, and toasting. Acrylamide may increase the risk of several types of cancer [68]. Avoiding deep frying, heavy crisping, and dark browning by blanching potatoes before frying have been shown to reduce the formation of acrylamide content in some foods [69]. Studies by [70,71,72] found that the acrylamide levels of potato chips prepared by the baking method were lower than the potato chips prepared by the frying method. Findings by [46] provided evidence of profound changes in Chinese dietary behaviors denoted by meal and cooking patterns, as Chines are shifting away from the traditional healthier steaming and boiling of food into the, less healthy, deep-frying of food. Findings from the present study revealed that the respondents baked food with a high rate of 77.94% and fried food with a much lower rate of 22.06%, which can be described as a healthy cooking behavior. The findings further showed that 49.67% of the respondents reported that they consumed a healthy diet most of the time, whereas 37.13% consumed a healthy diet sometimes, and 13.2% did not consume a healthy diet all the time. It is noteworthy to point to the relatively strong association between the findings of frying food as an unhealthy behavior with a rate of 22.06% on one hand and not consuming a healthy diet at all most of the time as an unhealthy behavior with a rate of 13.2% on the other hand. Research by [46], indicated that there is a strong graded association between consuming higher quantities of fried food and the level of education. In related research [73] showed that the incidence of diet-related NCDs was more ubiquitous in developing countries, even when some people enjoy higher socioeconomic status (SES). Conversely, the study asserted the contrary in developed countries where people do not have the same SES. In comparison, in the US, people with higher SES were more likely to have a healthier lifestyle. When compared, Chinese people with higher SES were more likely to be associated with an unhealthy lifestyle. However, research by [74] maintained that the Chinese people with a higher SES are bifurcated into binary groups between healthy and unhealthy lifestyles, whereas those Chinese people with a lower SES are more inclined to have a combination of the two conflicting lifestyles. The results of the present study were nearly in line with those reported by the above-mentioned studies.
Conclusions
One of the strengths of the present study is the sample size (N =1292) and the diversity of the respondents that were randomly sampled from the population at large representing nine cities located in the Yellow River Central Plains, Northwestern, Midwestern, and Southeastern regions of China. Another strength of this study is that it offers an in-depth qualitative analysis of the health implications of the transition of traditional food in the Chinese adult population, especially the association of this food transition with the emergence of nontraditional contemporary eating behaviors that have been linked to a multitude of NCDs. The limitations of the study, including the lack of a scholarly consensus on the precise definition of the term “fast food,” however, in the present study, was broadly defined which may suggest either consuming Western, Chinese, or both fast-food brands. Similarly, the lack of a consistent scholarly definition of the term “snack food,” however, in the present study, was the broadly-defined as an extra “small meal” or a “snack” that is self-defined by the study respondents. Other limitations were that the study did not directly measure or adjust for the extraneous variables, including the respondents’ level of education, total daily energy intake, food portion size, socioeconomic status, average family size, and living in urban or rural settings. Considering these relevant variables may reveal more information and further clarify some of the eating behavior patterns reported in the study findings. Future research would further examine the health implications of these areas of interest.
References
Liu J, Liu J. Chinese food. Cambridge, UK: Cambridge University Press; 2011. Print
Guang RT, et al. Food culture in China: From social-political perspectives. Trames Journal of the Humanities and Social Sciences. 2018;22(4):345–64. https://doi.org/10.3176/tr.2018.4.02.
Baker P, Friel S. Processed foods and the nutrition transition: Evidence from Asia. Obes Rev. 2014;15(7):564–77. https://doi.org/10.1111/obr.12174.
Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21 https://doi.org/10.1111/j.1753-4887.2011.00456.x.
Moran AR. The epidemiologic transition. A theory of the epidemiology of population change. 1971. Bulletin of the World Health Organization, Geneva, Switzerland. 2001;79(2):161–70.
Hawkes C. Uneven dietary development: linking the policies and processes of globalization with the nutrition transition, obesity, and diet-related chronic diseases. Glob Health. 2006;2(1):4. https://doi.org/10.1186/1744-8603-2-4.
He J, Klag MJ, Wu Z, Qian MC, Chen JY, Mo PS, et al. Effect of migration and related environmental changes on serum lipid levels in southwestern Chinese men. Am J Epidemiol. 1996;144(9):839–48. https://doi.org/10.1093/oxfordjournals.aje.a009018.
He J, Tell GS, Tang YC, Mo PS, He GQ. Relation of electrolytes to blood pressure in men: The Yi people study. Hypertension. 1991;17:378 https://doi.org/10.1161/01.HYP.17.3.378.
Popkin BM. Nutritional patterns and transitions. Popul Dev Rev. 1993;19(1):138–57. https://doi.org/10.2307/2938388.
Gill M, Feliciano D, Macdiarmid J, et al. The environmental impact of nutrition transition in three case study countries. Food Sec. 2015;7:493–504 https://doi.org/10.1007/s12571-015-0453-x.
Fourat E, Olivier L. Forms of food transition: Sociocultural factors limiting the diets' animalization in France and India. Sociol Rural. 2017;57(1):41–63. https://doi.org/10.1111/soru.12114.
Du H, Keys T. Diet and health. The China Kadoorie Biobank (CKB) Study of Chronic Disease, 2015; the University of Oxford Publication, Oxford, UK. Available from: https://www.ckbiobank.org/site/Research/Projects#P9.
Popkin BM, Keyou G, Zhai F, Guo X, Ma H, Zohoori N. The nutrition transition in China: a cross-sectional analysis. Eur J Clin Nutr. 1993;47(5):333–46.
Zhai F, Wang H, Du S, et al. Prospective study on nutrition transition in China. Nutr Rev. 2009;67(1):56–61. https://doi.org/10.1111/j.1753-4887.2009.00160.x.
Guan M. Ethnic difference of disease prevalence in rural China: Examples and Explanations. Health. 2015;7(4):449–55. https://doi.org/10.4236/health.2015.74052.
Liu M, Zhang Q, Lu M, Kwon C, Quan H. Rural and urban disparity in health services utilization in China. Med Care. 2007;45(8):767–74. Available from: www.jstor.org/stable/40221504. https://doi.org/10.1097/MLR.0b013e3180618b9a.
Ma G. Food, eating behavior, and culture in Chinese society. J Ethn Food. 2015;2(4):195–9 https://doi.org/10.1016/j.jef.2015.11.004.
Zhang N, Ma G. Nutritional characteristics and health effects of regional cuisines in China. J Ethn Food. 2020;7(7) https://doi.org/10.1186/s42779-020-0045-z.
Leach E. Culture and communication: The logic by which symbols are connected. An introduction to the use of structuralist analysis in social anthropology. Cambridge, UK: Cambridge University Press; 1976. Print
Baker P, Friel S. Food systems transformations, ultra-processed food markets and the nutrition transition in Asia. Glob Health. 2016;12(80) https://doi.org/10.1186/s12992-016-0223-3.
Wu Q, Liang X. Food therapy and medical diet therapy of traditional Chinese medicine. Clinical Nutrition Experimental. 2018;18(1):1–5 https://doi.org/10.1016/j.yclnex.2018.01.001.
Li-te L, Yin L, Saito M. Function of Traditional Foods and Food Culture in China. Japan Agricultural Research Quarterly. 2004;38(4):213–20. https://doi.org/10.6090/jarq.38.213.
Jiang M, Zhang C, Zheng G, Guo H, Li L, Yang J, et al. Traditional Chinese medicine ZHENG in the era of evidence-based medicine: a literature analysis. Evid Based Complement Alternat Med. 2012;2012:409568. https://doi.org/10.1155/2012/409568.
Chang KC. Food in Chinese culture: anthropological and historical perspectives. New Haven, CT: Yale University Press; 1977. Print
Wood F. The Silk Road: Two thousand years in the heart of Asia. 1st ed. Berkeley, CA: University of California Press; 2004. Print
Xinru L. The Silk Road in world history (New Oxford World History). 1st ed. Oxford, UK: Oxford University Press; 2010. Print
Dott BR. The chile pepper in China: A cultural biography. 1st ed. New York City, NY: Columbia University Press; 2020. Print
Bayan L, Koulivand PH, Gorji A. Garlic: a review of potential therapeutic effects. Avicenna J Phytomed. 2014;4(1):1–14 Available from: https://pubmed.ncbi.nlm.nih.gov/25050296/.
Haniadka R, Saldanha E, Sunita V, Palatty PL, Fayad R, Baliga MS. A review of the gastroprotective effects of ginger (Zingiber officinale Roscoe). Food Funct. 2013;4(6):845–55. https://doi.org/10.1039/c3fo30337c.
Yü Y-s. Chinese History and Culture: Sixth Century B.C.E. to Seventeenth Century. Vol. 2. New York City, NY: Columbia University Press; 2016. Print
Simoons FJ. Food in China: A cultural and historical inquiry. 1st ed. Telford, PA: Telford Press; 1990. Print
Wu HW, Sturm R. What's on the menu? A review of the energy and nutritional content of U.S. chain restaurant menus. Public Health Nutr. 2013;16(1):87–96. https://doi.org/10.1017/S136898001200122X.
Wang Y, Mi J, Shan XY, Wang QJ, Ge KY. Is China facing an obesity epidemic and the consequences? The trends in obesity and chronic disease in China. Int J Obes. 2007;31(1):177–88. https://doi.org/10.1038/sj.ijo.0803354.
Zhang X, van der Lans I, Dagevos H. Impacts of fast food and the food retail environment on overweight and obesity in China: A multilevel latent class cluster approach. Public Health Nutr. 2012;15(1):88–96. https://doi.org/10.1017/S1368980011002047.
Bahadoran Z, Mirmiran P, Azizi F. Fast food pattern and cardiometabolic disorders: A review of current studies. Health Promot Perspect. 2016;5(4):231–40. https://doi.org/10.15171/hpp.2015.028.
Lavrakas PJ, editor. Self-Administered Questionnaire: Encyclopedia of Survey Research Methods. Thousand Oaks, CA: Sage Publications, Inc.; 2008. https://doi.org/10.4135/9781412963947.
Thompson FE, Kipnis V, Subar AF, Krebs-Smith SM, Kahle LL, Midthune D, et al. Evaluation of 2 brief instruments and a food-frequency questionnaire to estimate the daily number of servings of fruit and vegetables. Am J Clin Nutr. 2000;71(6):1503–10. https://doi.org/10.1093/ajcn/71.6.1503.
Carrascosa RG, Segovia PG, Monzo JM. Paper and pencil vs online self-administered food frequency questionnaire (FFQ) applied to university population: a pilot study. Nutr Hosp. 2011;26(6):1378–84. https://doi.org/10.1590/S0212-16112011000600027.
Krause N. A comprehensive strategy for developing closed-ended survey items for use in studies of older adults. The Journals of Gerontology: Series B. 2002;57(5):S263–74 DOI: org/10.1093/geronb/57.5.S263.
Davies MB. Doing a successful research project. 2nd ed. London: UK: Palgrave Macmillan (Springer Nature); 2014. Print
WHO. Global status report on-communicable diseases 2014. World Health Organization. Available from: https://apps.who.int/iris/bitstream/handle/10665/148114/9789241564854_eng.pdf.
CDC Global Health - Stories. Addressing non-communicable diseases in China. Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/globalhealth/stories/ncd_china.htm.
Hunter DJ, Reddy KS. Noncommunicable diseases. N Engl J Med. 2013;369(14):1336–43. https://doi.org/10.1056/NEJMra1109345.
Ali MK, Jaacks LM, Kowalski AJ, Siegel KR, Ezzati M. Noncommunicable diseases: Three decades of global data show a mixture of increases and decreases in mortality rates. Health Aff. 2015;34(9):1444–55. https://doi.org/10.1377/hlthaff.2015.0570.
Popkin BM. Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am J Clin Nutr. 2006;84(2):289–98 https://doi.org/10.1093/ajcn/84.2.289.
Wang Z, Zhai F, Du S, Popkin B. Dynamic shifts in Chinese eating behaviors. Asia Pac J Clin Nutr. 2008;17(1):123–30.
Kerver JM, Yang EJ, Obayashi S, Bianchi L, Song WO. Meal and snack patterns are associated with dietary intake of energy and nutrients in U.S. adults. J Am Diet Assoc. 2006;106(1):46–53. https://doi.org/10.1016/j.jada.2005.09.045.
Rolls BJ, Roe LS, Kral TV, Meengs JS, Wall DE. Increasing the portion size of a packaged snack increases energy intake in men and women. Appetite. 2004;42(1):63–9. https://doi.org/10.1016/S0195-6663(03)00117-X.
Wildey MB, Pampalone SZ, Pelletier RL, Zive MM, Elder JP, Sallis JF. Fat and sugar levels are high in snacks purchased from student stores in middle schools. J Am Diet Assoc. 2000;100(3):319–22. https://doi.org/10.1016/S0002-8223(00)00099-7.
Phillips SM, Bandini LG, Naumova EN, Cyr H, Colclough S, Dietz WH, et al. Energy-dense snack food intake in adolescence: Longitudinal relationship to weight and fatness. Obes Res. 2004;12(3):461–72. https://doi.org/10.1038/oby.2004.52.
Wang Y, Wang L, Xue H, Qu W. A review of the growth of the fast-food industry in China and its potential impact on obesity. Int J Environ Res Public Health. 2016;13(11):1112. https://doi.org/10.3390/ijerph13111112.
De Vogli R, Kouvonen A, Gimeno D. The influence of market deregulation on fast food consumption and body mass index: a cross-national time-series analysis. Bull World Health Organ. 2014;92(2):99–107A. https://doi.org/10.2471/BLT.13.120287.
Zhao Y, Wang L, Xue H, Wang H, Wang Y. Fast food consumption and its associations with obesity and hypertension among children: results from the baseline data of the childhood obesity study in China mega-cities. BMC Public Health. 2017;17(1):933. https://doi.org/10.1186/s12889-017-4952-x.
Anderson B, Rafferty AP, Lyon-Callo S, Fussman C, Imes G. Fast-food consumption, and obesity among Michigan adults. Prev Chronic Dis. 2011;8(4):A71.
WHO. Guideline on sugar intake for adults and children. World Health Organization. Available from: http://www.who.int/nutrition/publications/guidelines/sugars_intake/en/.
Suh H, Kavouras SA. Water intake and hydration state in children. Eur J Nutr. 2019;58(2):475–96. https://doi.org/10.1007/s00394-018-1869-9.
Sontrop JM, Dixon SN, Garg AX, Buendia-Jimenez I, Dohein O, Huang SHS, et al. Association between water intake, chronic kidney disease, and cardiovascular disease: a cross-sectional analysis of NHANES data. Am J Nephrol. 2013;37(5):434–42. https://doi.org/10.1159/000350377.
Benefer MD, Corfe BM, Russell JM, Short R, Barker ME. Water intake and post-exercise cognitive performance: An observational study of long-distance walkers and runners. Eur J Nutr. 2013;52(2):617–24. https://doi.org/10.1007/s00394-012-0364-y.
D'anci KE, Vibhakar A, Kanter JH, Mahoney CR, Taylor HA. Voluntary dehydration and cognitive performance in trained college athletes. Percept Mot Skills. 2009;109(1):251–69. https://doi.org/10.2466/PMS.109.1.251-269.
Guelinckx I, Ferreira-Pêgo C, Moreno LA, et al. Intake of water and different beverages in adults across 13 countries. Eur J Nutr. 2015;54(Suppl 2):45–55. https://doi.org/10.1007/s00394-015-0952-8.
Zhang N, Morin C, Guelinckx I, Moreno LA, Kavouras SA, Gandy J, et al. Fluid intake in urban China: results of the 2016 Liq.In 7 national cross-sectional surveys. Eur J Nutr. 2018;57(Suppl 3):77–88. https://doi.org/10.1007/s00394-018-1755-5.
Spiegelman BM, Flier JS. Obesity and the regulation of energy balance. Cell. 2001;104(4):531–43. https://doi.org/10.1016/s0092-8674(01)00240-9.
Ledikwe JH, Ello-Martin JA, Rolls BJ. Portion sizes and the obesity epidemic. J Nutr. 2005;135(4):905–9. https://doi.org/10.1093/jn/135.4.905.
Prentice AM, Jebb SA. Fast foods, energy density, and obesity: a possible mechanistic link. Obes Rev. 2003;4(4):187–94. https://doi.org/10.1046/j.1467-789x.2003.00117.x.
Glanz K, Basil M, Maibach E, Goldberg J, Snyder D. Why Americans eat what they do: taste, nutrition, cost, convenience, and weight control concerns as influences on food consumption. J Am Diet Assoc. 1998;98(10):1118–26. https://doi.org/10.1016/S0002-8223(98)00260-0.
Zang J, Luo B, Wang Y, Zhu Z, Wang Z, He X, et al. Eating out-of-home in adult residents in Shanghai and the nutritional differences among dining places. Nutrients. 2018;10(7):951. https://doi.org/10.3390/nu10070951.
Hu P, Wu T, Zhang F, Zhang Y, Lu L, Zeng H, et al. Association between eating out and socio-demographic factors of university students in Chongqing, China. Int J Environ Res Public Health. 2017;14(11):1322. https://doi.org/10.3390/ijerph14111322.
Virk-Baker MK, Nagy TR, Barnes S, Groopman J. Dietary acrylamide and human cancer: A systematic review of literature. Nutr Cancer. 2014;66(5):774–90. https://doi.org/10.1080/01635581.2014.916323.
Palazoğlu TK, Savran D, Gökmen V. Effect of cooking method (baking compared with frying) on acrylamide level of potato chips. J Food Sci. 2010;75(1):E25–9. https://doi.org/10.1111/j.1750-3841.2009.01389.x.
Skog K, Viklund G, Olsson K, Sjöholm I. Acrylamide in home-prepared roasted potatoes. Mol Nutr Food Res. 2008;52(3):307–12. https://doi.org/10.1002/mnfr.200700240.
Kita A, Bråthen E, Knutsen SH, Wicklund T. Effective ways of decreasing acrylamide content in potato crisps during processing. J Agric Food Chem. 2004;52(23):7011–6. https://doi.org/10.1021/jf049269i.
Mojska H, Gielecińska I, Szponar L. Acrylamide content in heat-treated carbohydrate-rich foods in Poland. Rocz Panstw Zakl Hig. 2007;58(1):345–9.
Kim S, Symons M, Popkin BM. Contrasting socioeconomic profiles related to healthier lifestyles in China and the United States. Am J Epidemiol. 2004;159(2):184–91. https://doi.org/10.1093/aje/kwh006.
Wang F. Status constraint and lifestyle transition: A latent class analysis of health-related lifestyles among different social strata in China. J Chin Sociol. 2019;6(23):1–20 https://doi.org/10.1186/s40711-019-0112-2.
Acknowledgements
I would like to acknowledge the contributions made to this paper and the research leading to it by the Key Research Institute of Yellow River Civilization and Sustainable Development at Henan University, Kaifeng, Henan Province, China, and the National Office of High-End Foreign Experts of the Chinese Ministry of Education, Beijing, China. This work would not have been possible without the inestimable support of the Institute's Director, Dr. Changhong Miao, Professors Ma Zheng, and Shao-wei Ai, as well as their graduate students Yuanyuan Cai, Fengmei Pan, and Huixian Ji for providing their invaluable support in travel, translation, compilation, and systematization of the questionnaire data. I am also grateful to the Institute’s office staff for providing the administrative support that kept this research project on track to its fruition.
Funding
The work leading to the results of this study received funding from the National Bureau of High-End Foreign Experts of the Chinese Ministry of Education, Beijing, China. Individual grant awarded: GDW20154100215.
Author information
Authors and Affiliations
Contributions
The author read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
I declare that there is no conflict of interest. The underwriters of this research had neither influenced nor played any role concerning the development, data analysis, interpretation of the results, or drafting of this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Halawa, A. Analysis of the health effects of the transition of traditional Chinese food on the emergence of nontraditional eating behaviors. J. Ethn. Food 8, 14 (2021). https://doi.org/10.1186/s42779-021-00087-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42779-021-00087-3