
Abstract
Background
Patients with a left (LHS) or right hemispheric stroke (RHS) differ in terms of clinical symptoms due to lateralization of specific cortical functions. Studies on functional outcome after stroke and endovascular thrombectomy (EVT) comparing both hemispheres showed conflicting results so far. The impact of stroke laterality on patient-reported health-related quality of life (HRQoL) after EVT has not yet been adequately addressed and still remains unclear.
Methods
Consecutive stroke thrombectomy patients, derived from a multi-center, prospective registry (German Stroke Registry) between June 2015 and December 2019, were included in this study. At 90 days, outcome after EVT was assessed by the modified Rankin scale (mRS) and HRQoL using the European QoL-five dimensions questionnaire utility-index (EQ-5D-I; higher values indicate better HRQoL) in patients with LHS and RHS. Adjusted regression analysis was applied to evaluate the influence of stroke laterality on outcome after EVT.
Results
In total, 5683 patients were analyzed. Of these, 2953 patients (52.8%) had LHS and 2637 (47.2%) RHS. LHS patients had a higher baseline NIHSS (16 vs. 13, p < 0.001) and a higher ASPECTS (9 vs. 8, p < 0.001) compared to RHS patients. Among survivors, patients with LHS less frequently had a self-reported affected mobility (p = 0.037), suffered less often from pain (p = 0.04) and anxiety/depression (p = 0.032) three months after EVT. After adjusting for confounders (age, sex, baseline NIHSS), LHS was associated with a better HRQoL (ß coefficient 0.04, CI 95% 0.017–0.063; p = 0.001), and better functional outcome assessed by lower values on the mRS (ß coefficient − 0.109, CI 95% − 0.217–0.000; p = 0.049).
Conclusions
Ninety days after EVT, LHS patients have a better functional outcome and HRQoL. Patients with RHS should be actively assessed and treated for pain, anxiety and depression to improve their HRQoL after EVT.
Similar content being viewed by others

Introduction
Endovascular thrombectomy (EVT) has become standard of care for anterior circulation stroke in patients with large vessel occlusion irrespective of stroke lateralization. Strokes affecting the left and right hemisphere, however, are different with regards to acute clinical symptoms and outcome. Lateralization of specific cortical functions, e.g., language or spatial perception, results in important clinical differences between the hemispheres. In line with this, previous studies have demonstrated that patients with right hemispheric stroke (RHS) are less frequently recognized as having a stroke, present later to hospital, are less likely to receive intravenous thrombolysis therapy (IVT) and show a worse functional recovery compared to patients suffering from left hemispheric stroke (LHS) 1,2,3].
Moreover, imaging studies revealed that RHS may comprise a substantial and similar infarct size compared to LHS, while having a lower National Institutes of health Stroke Scale Score (NIHSS), thus, indicating that the NIHSS is biased towards LHS and presumably underpowered for assessing the clinical severity of RHS adequately 4,5,6].
However, studies on functional outcome, commonly assessed by the modified Rankin Scale (mRS), comparing RHS and LHS have provided conflicting evidence so far 7,8,9]. To our knowledge, the impact of hemispheric lateralization on quality of life in stroke patients after EVT has not yet been adequately addressed.
Thus, the objective of our study was to determine whether (a) outcome of stroke patients after EVT, assessed by the modified Rankin Scale (mRS) and self-reported HRQoL, differ between LHS and RHS patients and (b) stroke laterality has an influence on these outcome parameters after EVT in a large, representative, multi-center patient cohort of clinical practice.
Methods
Patients and data collection
In this study, patients from the German Stroke Registry-Endovascular Treatment (GSR-ET; ClinicalTrials.gov, Identifier: NCT03356392), enrolled between June 2015 and December 2019, were analyzed. The GSR-ET is an ongoing prospective, multicenter registry which comprises both university and community hospitals in Germany. This registry includes data from consecutive acute ischemic stroke patients with proximal large vessel occlusion of the anterior and posterior circulation treated with EVT. The study design and major findings have already been reported elsewhere [10, 11].
The decision for EVT was made at the physicians ‘decretion, interdisciplinary between a vascular neurologist and an interventional neuroradiologist. The neuroradiologists performed the interventions in accordance with the institutional guidelines. Ninety days after stroke thrombectomy, functional outcome and HRQoL were assessed by a standardized telephone interview or face-to-face visit by a well-trained investigator, who was blinded to patients’ variables.
The study was approved by all responsible ethics committees of the participating sites. The patients themselves or their proxies gave written informed consent. Consent was waived if patients died before consent could be obtained or lacked the capacity to give consent and no proxy was available.
Health-related quality of life assessment
The three level European QoL-five dimensions (EQ-5D-3L) questionnaire, as an established instrument to assess quality of life, was applied to evaluate the self-reported HRQoL in this patient cohort. A detailed description is provided elsewhere [12]. Briefly, the EQ-5D-3L comprises the five health domains mobility, selfcare, usual activities, pain/discomfort and anxiety/depression. Patients may choose one of the three different response options for each of these five dimensions: no complaints, some complaints or extreme complaints. In total, 243 (35) health states, and thus, 243 different indices can be calculated to evaluate the HRQoL [13]. Previously, this EQ-5D utility index (EQ-5D-I) was established by the time trade off method and is based on the country-specific value set of the UK population for this patient cohort, since a German-specific value set for the EQ-5D questionnaire is still unavailable and both countries are commonly assumed to be comparable [13]. As per instrument validation, a zero score is assigned to patients who died. Due to the time trade off method negative index values may also be achieved and are interpreted as situations in which patients might evaluate their health state worse than death. In our patient population, the minimum negative value was -0.594. Higher index values reflect better HRQoL, with the value “1” as the best health status. The patients themselves, their proxies or health care providers, if patients lacked capacity to respond, provided the EQ-5D information.
Statistical analysis
Continuous variables are reported as median and interquartile range (IQR) or mean ± standard deviation (SD). Categorical variables are provided as proportions. Between group comparisons (LHS vs. RHS) for continuous variables were performed by Mann–Whitney-U-tests, for catagorical variables by chi-square or Fisher’s Exact tests. Of note, one part of the present study population has already been analyzed in terms of HRQoL after stroke thrombectomy, and the results were published recently [12].
Multivariate linear and binary logistic regression analyses assessed the influence of stroke laterality on outcome with the mRS and the EQ-5D-I, and with mortality (dichotomized to mRS 6 vs. 1–5) at 90 days as dependent variables. The analyses were adjusted by important clinical baseline variables: age, sex and NIHSS on admission. The resulting ß coefficients and odds ratios (OR) with 95% confidence intervals (CI) and p values are reported. P values < 0.05 were considered statistically significant. The statistical analysis was performed using SPSS (Version 25.0; IBM, Armonk, New York).
Results
Patient cohort
In total, n = 6634 patients were enrolled in the registry during the study period (Fig. 1). Data on infarct location were available in n = 6456 patients, with n = 5683 (88%) subjects suffering from anterior circulation infarcts. In n = 93 (1.6%) data on stroke laterality were missing, leaving n = 5590 patients for this analysis. Of these, n = 2953 patients (52.8%) had LHS, and n = 2637 (47.2%) patients had RHS (Table 1). Patients with LHS had a higher stroke severity on admission assessed by the NIHSS (16 vs. 13, p < 0.001) and a higher Alberta Stroke Program Early CT Score (ASPECTS) (9 vs. 8, p < 0.001) compared to patients with RHS. The time elapsed from symptom onset to groin puncture and recanalization were shorter in LHS patients (189.5 vs. 200 min, p = 0.004 and 236 vs. 248 min, p = 0.012, respectively) than in RHS subjects. LHS patients less frequently had any intracranial hemorrhage (ICH) 24 h after intervention (11.1 vs. 13.2%, p = 0.008).

Flowchart of patients included in this subanalysis of the GSR-ET. In total, n = 6634 patients were enrolled in the GSR-ET between June 2015 and December 2019. After excluding subjects with missing data n = 5590 patients were included in the present study, whereas 53% of these had a LHS and 47% a RHS
Functional outcome assessed by the mRS
The distribution of the mRS scores at 90 days of both LHS and RHS patients is displayed on Fig. 2. The rate of functional independence (mRS 0–2) and death or dependency (mRS 5–6) did not differ between both patient subgroups. In unadjusted analysis, LHS patients had 3.3% higher mortality rate 90 days after stroke thrombectomy than RHS patients (30.2 vs. 26.9%, p = 0.008). After adjusting for confounding variables, hemispheric lateralization showed no association with mortality at 90 days anymore (OR 1.011, CI 95% 0.876–1.167; p = 0.879).

The distribution of the mRS scores at 90 days according to the affected hemisphere. The rate of functional independence (mRS 0–2) and death or dependency (mRS 5–6) showed no difference between LHS and RHS patients. In unadjusted analysis, a 3.3% higher mortality rate was found in LHS compared to RHS patients 90 days after stroke thrombectomy (30.2 vs. 26.9%, p = 0.008)
In adjusted analyses, LHS was associated with a better functional outcome (ß coefficient -0.109, CI 95% − 0.217–0.000; p = 0.049) (Fig. 3A).

Forrest plot showing the impact of stroke laterality on outcome assessed by the mRS (A) and by the EQ-5D-I B 90 days after EVT. After adjusting for the confounding variables (age, sex and baseline NIHSS), LHS was associated with a better functional outcome (ß coefficient − 0.109, CI 95% − 0.217–0.000; p = 0.049) (Fig. 3A) and strongly associated with a better HRQoL (ß coefficient 0.04, CI 95% 0.017–0.063; p = 0.001) (Fig. 3B)
Health-related quality of life assessed by EQ-5D-I
In adjusted analyses, LHS was associated with a better HRQoL (ß coefficient 0.04, CI 95% 0.017–0.063; p = 0.001) (Fig. 3B).
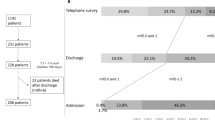
Patients with LHS less frequently had a self-reported affected mobility (p = 0.037), suffered less often from pain (p = 0.04) and anxiety/depression (p = 0.032) three months after stroke thrombectomy compared to RHS subjects. The patient responses in terms of the dimensions selfcare (p = 0.219) and usual activities (p = 0.914) did not differ between the hemispheres (Fig. 4).

Health-related quality of life 90 days after EVT between patients with LHS and RHS. The distribution of the EQ-5D 3L results in LHS compared to RHS patients is displayed. Patients with LHS had less often mobility constraints (p = 0.037), suffered less frequently from pain (p = 0.04) and anxiety/depression (p = 0.032) 90 days after EVT compared to RHS subjects. The patient responses in the dimensions selfcare (p = 0.219) and usual activities (p = 0.914) showed no differences between both hemispheres. GSR-ET, German Stroke Registry-Endovascular Treatment; LHS, Left hemispheric stroke; RHS, Right hemispheric stroke; mRS, modified Rankin Scale; EQ-5D-I, European Quality of Life-five dimensions questionnaire utility-index; EVT, endovascular treatment; NIHSS, National Institutes of Health Stroke Scale
Discussion
In the present study, which included stroke thrombectomy patients from a large, prospective, multi-center and industry-independent registry, we provide real world data on the impact of stroke laterality on functional outcome and HRQoL, and detailed information about different health dimensions after EVT in patients with LHS compared to RHS.
In this study cohort of clinical practice, we found an effect of hemispheric lateralization on functional outcome assessed by mRS. In addition, we observed a highly significant effect of stroke laterality on HRQoL.
Most of the trials on stroke and thrombectomy assessed functional outcome by the mRS which mainly reflects the physical disability of a patient. Previous studies already demonstrated that the impact of stroke laterality on functional outcome after stroke and thrombectomy is still inconclusive [7,8,9]. In line with this, the association of hemispheric lateralization only showed a ß coefficient of − 0.109 (CI 95% − 0.217–0.000; p = 0.049) in our patient cohort.
However, previous studies on stroke and thrombectomy have suggested to assess outcome and effectiveness of medical treatment by additional scales beside the mRS, such as patient self-reported outcomes. In particular, HRQoL is a valuable complementary outcome measure to evaluate outcome after stroke and EVT, as already applied and stated by several studies [12, 14, 15]. The European Stroke Organization has also prioritized the use of patient-reported outcomes in research studies to develop specific targets in stroke rehabilitation and facilitate the recovery process [16].
One possible explanation for the better HRQoL in LHS patients is that recovery might be protracted in RHS patients due to non-dominant hemisphere symptoms such as depression, apathy and amotivation [3, 7]. Furthermore, LHS patients tend to remain longer in rehabilitation [17] which may also account for the better HRQoL in this subgroup of patients. A lower rehabilitation potential of RHS patients due to neglect has also been discussed [18, 19].
In fact, in our study population RHS patients more frequently suffered from pain/discomfort and anxiety/depression, and perceived higher mobility constraints than LHS patients at 90 days. Thus, RHS patients might be scored well on available functional assessment scores while still being extremely disabled by these factors. Thus, our findings provide valuable additional data for targeted rehabilitation therapies after EVT, in particular for patients with RHS. In consequence, our results suggest that patients with RHS should be actively assessed and treated for pain, anxiety and depression beside physical disability after EVT to improve their quality of life.
In line with our results, a previous study found a significant association of depression with stroke lesions of the right hemisphere [3]. Furthermore, since in LHS patients speech disabilities are in the foreground, they might perceive mobility impairments less than RHS subjects. Moreover, patients with RHS suffer more frequently from the pusher-syndrome (lateropulsion) after stroke [20] which might also account for a worse perception of mobility. Interestingly, imaging studies revealed an increased activation of the right-sided insula in the presence of neuropathic pain [21, 22], indicating a strong association of right hemispheric lesions with the perception of pain, consistent with our findings.
In between-group comparisons, we discovered a higher baseline NIHSS in LHS patients compared to RHS patients. Thus, we confirmed previous findings, as several studies found similar results after stroke and thrombectomy [7,8,9, 23]. The difference in the NIHSS between the hemispheres might be explained by a structural inherent bias of the NIHSS itself. In particular, the NIHSS is biased towards LHS, as the NIHSS gives more weight to language, attributable to left hemispheric lesions, than to hemispatial neglect, a hallmark of RHS [6].
Notably, patients with RHS were shown to have a comparable infarct volume as LHS [4] despite scoring less on the NIHSS. This indicates that the NIHSS systematically underestimates stroke severity in RHS patients [4]. The different weighting in scoring the NIHSS for both hemispheres may impact on treatment decision that rely on NIHSS tresholds. In fact, RHS patients were shown to receive less frequently IVT than LHS subjects [7]. It was suggested that a combination of late diagnosis, delayed admission to hospital and the use of stroke severity scales biased towards the left hemisphere may have induced this imbalance of treatment [18, 19]. However, we did not find different IVT rates between the hemispheres in our patient cohort of clinical practice.
The differences in clinical symptoms depending on the side of lesion may, indeed, affect awareness and recognition of stroke. Since sudden speech disturbances are more apparent than perceptual deficits, RHS patients are more likely to be later diagnosed as a stroke, and, in consequence, present later to hospital [1]. This is in line with our findings showing longer workflow times in RHS patients of our study cohort. Interestingly, the ASPECT score was found to be lower in RHS patients, potentially explained by the deferred admission [1]. Correspondingly, the higher rate of any ICH 24 h after intervention in RHS patients might be attributed to the higher extent of early ischemic changes on brain imaging in RHS patients on admission.
There are some factors that may limit our findings. Our study provides a short-term follow up period of three months after stroke thrombectomy for HRQoL measurements. Long-term assessments may provide additional clues about HRQoL. Furthermore, in cases who lacked capability the questionnaire was completed by proxies. This might reduce the validity of the responses, since over- or underestimation of QoL might occur. However, we believe that this limitation did not significantly confound our findings, since agreement between caregivers and patient self-reports have been demonstrated to be reasonable [24].
Conclusions
This study represents real world experience and provides data from a full spectrum of patients with acute ischemic stroke treated with EVT over a broad range of stroke severity. Stroke laterality had an influence on functional outcome assessed by the mRS, and showed a clear impact on HRQoL 90 days after EVT. Our findings reinforce that assessment of HRQoL as a complimentary outcome measure is of paramount importance, since it enables an identification of non-motor determinants affecting HRQoL, such as pain, anxiety and depression. In particular, in patients with RHS rehabilitation needs for these factors should not be underestimated, but rather actively assessed and specifically targeted in rehabilitation therapies to improve their quality of life.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- LHS:
-
Left hemispheric stroke
- RHS:
-
Right hemispheric stroke
- HRQoL:
-
Health-related quality of life
- GSR-ET:
-
German Stroke Registry-Endovascular Treatment
- EQ-5D-I:
-
European quality of life-five dimension questionnaire utility index
- EQ-5D-3L:
-
Three level European quality of life-five dimensions questionnaire
References
Foerch, C., Misselwitz, B., Sitzer, M., Berger, K., Steinmetz, H., & Neumann-Haefelin, T. (2005). Difference in recognition of right and left hemispheric stroke. Lancet, 366, 392–393.
Di Legge, S., Fang, J., Saposnik, G., & Hachinski, V. (2005). The impact of lesion side on acute stroke treatment. Neurology, 65, 81–86.
MacHale, S. M., O’Rourke, S. J., Wardlaw, J. M., & Dennis, M. S. (1998). Depression and its relation to lesion location after stroke. Journal of Neurology, Neurosurgery and Psychiatry, 64, 371–374.
Fink, J. N., Selim, M. H., Kumar, S., et al. (2002). Is the association of National Institutes of Health Stroke Scale scores and acute magnetic resonance imaging stroke volume equal for patients with right-and left-hemisphere ischemic stroke? Stroke, 33, 954–958.
Woo, D., Broderick, J. P., Kothari, R. U., et al. (1999). Does the National Institutes of Health Stroke Scale favor left hemisphere strokes? NINDS t-PA stroke study group. Stroke, 30, 2355–2359.
Lyden, P., Claesson, L., Havstad, S., Ashwood, T., & Lu, M. (2004). Factor analysis of the National Institutes of Health Stroke Scale in patients with large strokes. Archives of Neurology, 61, 1677–1680.
Di Legge, S., Saposnik, G., Nilanont, Y., & Hachinski, V. (2006). Neglecting the difference: Does right or left matter in stroke outcome after thrombolysis? Stroke, 37, 2066–2069.
Fink, J. N., Frampton, C. M., Lyden, P., & Lees, K. R. (2008). Does hemispheric lateralization influence functional and cardiovascular outcomes after stroke?: An analysis of placebo-treated patients from prospective acute stroke trials. Stroke, 39, 3335–3340.
Almekhlafi, M. A., Hill, M. D., Roos, Y. M., et al. (2019). Stroke laterality did not modify outcomes in the HERMES meta-analysis of individual patient data of 7 trials. Stroke, 50, 2118–2124.
Alegiani, A. C., Dorn, F., Herzberg, M., et al. (2019). Systematic evaluation of stroke thrombectomy in clinical practice: The German Stroke Registry Endovascular Treatment. International Journal of Stroke, 14, 372–380.
Wollenweber, F. A., Tiedt, S., Alegiani, A., et al. (2019). Functional outcome following stroke thrombectomy in clinical practice. Stroke, 50, 2500–2506.
Deb-Chatterji, M., Konnopka, A., Flottmann, F., et al. (2020). Patient-reported, health-related, quality of life after stroke thrombectomy in clinical practice. Neurology, 95, e1724–e1732.
Dolan, P. (1997). Modeling valuations for EuroQol health states. Medical Care, 35, 1095–1108.
Dávalos, A., Cobo, E., Molina, C. A., et al. (2017). Safety and efficacy of thrombectomy in acute ischaemic stroke (REVASCAT): 1-year follow-up of a randomised open-label trial. Lancet Neurology, 16, 369–376.
McCarthy, D. J., Diaz, A., Sheinberg, D. L., et al. (2019). Long-term outcomes of mechanical thrombectomy for stroke: A meta-analysis. Scientific World Journal, 2019, 7403104.
Norrving, B., Barrick, J., Davalos, A., et al. (2018). Action plan for stroke in Europe 2018–2030. European Stroke Journal, 3, 309–336.
Wade, D. T., Hewer, R. L., & Wood, V. A. (1984). Stroke: Influence of patient’s sex and side of weakness on outcome. Archives of Physical Medicine and Rehabilitation, 65, 513–516.
Aszalós, Z., Barsi, P., Vitrai, J., & Nagy, Z. (2002). Lateralization as a factor in the prognosis of middle cerebral artery territorial infarct. European Neurology, 48, 141–145.
Ween, J. E., Alexander, M. P., D’Esposito, M., & Roberts, M. (1996). Factors predictive of stroke outcome in a rehabilitation setting. Neurology, 47, 388–392.
Pérennou, D. A., Mazibrada, G., Chauvineau, V., et al. (2008). Lateropulsion, pushing and verticality perception in hemisphere stroke: A causal relationship? Brain, 131, 2401–2413.
Wang, N., Zhang, Y. H., Wang, J. Y., & Luo, F. (2021). Current understanding of the involvement of the insular cortex in neuropathic pain: a narrative review. Int J Mol Sci, 22, 2648.
Friebel, U., Eickhoff, S. B., & Lotze, M. (2011). Coordinate-based meta-analysis of experimentally induced and chronic persistent neuropathic pain. NeuroImage, 58, 1070–1080.
Hedna, V. S., Bodhit, A. N., Ansari, S., et al. (2013). Hemispheric differences in ischemic stroke: Is left-hemisphere stroke more common? Journal of Clinical Neurology, 9, 97–102.
Kozlowski, A. J., Singh, R., Victorson, D., et al. (2015). Agreement between responses from community-dwelling persons with stroke and their proxies on the NIH Neurological Quality of Life (Neuro-QoL) Short forms. Archives of Physical Medicine and Rehabilitation, 96, 1986-1992.e1914.
Acknowledgements
GSR-ET Steering Committee Investigators: Universitätsklinikum Hamburg-Eppendorf: Prof. Dr. C. Gerloff, Prof. Dr. J. Fiehler, Prof. Dr. G. Thomalla, Dr. med. A. Alegiani; Klinikum rechts der Isar: Dr. Boeckh-Behrens, Dr. Silke Wunderlich; Universitätsklinik Tübingen: Prof. Dr. Ulrike Ernemann, Dr. Sven Poli; Charité–Campus Benjamin Franklin und Campus Charité Mitte, Berlin: Dr. Eberhard Siebert, Prof. Dr. Christian H. Nolte; Charité—Campus Virchow Klinikum, Berlin: Dr. Sarah Zweynert, Dr. Georg Bohner; Sana Klinikum Offenbach: Dr. med. Alexander Ludolph, Dr. med. Karl-Heinz Henn; Uniklinik Frankfurt/ Main: Dr. med. Jan Hendrik Schäfer, Dr. Fee Keil; Asklepios Klinik Altona: Prof. Dr. Joachim Röther, Prof. Dr. Bernd Eckert; Klinikum Altenburger Land: Prof. Dr. Jörg Berrouschot, Dr. Albrecht Bormann; Uniklinik Bonn: Dr. med. Franziska Dorn, Prof. Dr. Gabor Petzold; Klinikum Lüneburg: Dr. Christoffer Kraemer, Dr. med Hannes Leischner; Uniklinik München (LMU): Dr. med. Christoph Trumm, Dr. Dr. Steffen Tiedt, Dr. Lars Kellert; Klinikum Osnabrück: Dr. Martina Petersen, Prof. Dr. Florian Stögbauer; Bezirkskrankenhaus Günzburg: Dr. med. Michael Braun, Prof. Dr. Gerhard F. Hamann; Universitätsmedizin Mainz: Prof. Dr. Klaus Gröschel, Dr. Timo Uphaus; Uniklinik RWTH Aachen: Dr. med. Arno Reich, Prof. Dr. med. Omid Nikoubashman; Johannes Wesling Klinikum Minden: Prof. Dr. med. Peter Schellinger, Prof. Dr. med. Jan Borggrefe; Klinikum Nordstadt: Dr. med. Jörg Hattingen; Universitätsmedizin Göttingen: Prof. Dr. med. Jan Liman, Dr. med. Marielle Ernst.
Funding
This study received no industrial, governmental or institutional funding.
Author information
Authors and Affiliations
Consortia
Contributions
MDC: Substantial contributions to the conception and design of the work. Acquisition, analysis and interpretation of data. Drafting the work and revising it critically for important intellectual content. JF, CG: Analysis and interpretation of data. Revising the work critically for important intellectual content. FF, LM, CB: Acquisition of data. Revising the work critically for important intellectual content. GT: Substantial contributions to the conception and design of the work. Analysis and interpretation of data. Drafting the work and revising it critically for important intellectual content. All authors read and approved the final version of the manuscript to be published and have agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by all responsible ethics committees of the participating sites. Written informed consent was obtained from the patient or their proxies. Consent was waived if patients died before consent could be obtained or lacked the capacity to give consent and no proxy was available.
Consent for publication
Not applicable.
Competing interests
CB: The author declares that he has no competing interest. FF: received personal fees from Eppdata GmbH outside the submitted work. LM: received compensation as a speaker for Balt Prime outside the submitted work. MDC has received research grants from the Werner Otto Stiftung outside the submitted work. JF receives research support from the German Ministry of Science and Education (BMBF), German Ministry of Economy and Innovation (BMWi), German Research Foundation (DFG), European Union (EU), Hamburgische Investitions- und Förderbank (IFB), Medtronic, Microvention, Stryker; and serves as a consultant for Acandis, Cerenovus, Medtronic, Microvention, Penumbra, Phenox, and Stryker. CG serves on scientific advisory boards for Bayer Vital, Boehringer Ingelheim, Acticor Biotech, Amgen, and Prediction Biosciences; has received funding for travel and/or speaker/ consulting honoraria from Bayer Vital, Boehringer Ingelheim, Sanofi Aventis, Amgen, EBS Technologies, GlaxoSmithKline, Lundbeck, Pfizer, Silk Road Medical, and UCB, and Abbott; serves on editorial boards for INFO Neurologie & Psychiatrie and Aktuelle Neurologie and as editor of textbook Therapie und Verlauf neurologischer Erkrankungen; has received grants to supporting employees/ scientists of his clinic from Merz Pharmaceuticals, Allergan, Novartis, and NeuroConn; and receives research support from Deutsche Forschungsgesellschaft, the European Union, Wegener Foundation, Schilling Foundation, and Werner-Otto- Foundation. GT has received personal fees as consultant or lecturer from Acandis, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb/Pfizer, Daichi Sankyo, Stryker, and research grants from Bayer, Federal Ministry for Economic Affairs and Energy (BMWi), Corona-Foundation, German Research Foundation (DFG), Else Kröner-Fresenius Foundation, European Union (Horizon 2020), German Innovation Fund.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Deb-Chatterji, M., Flottmann, F., Meyer, L. et al. Side matters: differences in functional outcome and quality of life after thrombectomy in left and right hemispheric stroke. Neurol. Res. Pract. 4, 58 (2022). https://doi.org/10.1186/s42466-022-00223-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42466-022-00223-7