
Abstract
Background
The lead of left bundle branch area pacing (LBBAP) inserted into the muscular septum will make the transvenous lead extraction (TLE) of LBBAP more challenging and because in LBBAP ventricular lead (V lead) should be inserted into the part of the septum, damage to the vessel near the lead could occur. The case reports introduced the complications of LBBAP previously introduced, but not being considered in detail.
Case presentation
The two patients (76-year-old man, 90-year-old man) with a complete atrioventricular block (CAVB) undergoing the LBBAP procedure experienced complications related to the procedure. The complications were abrupt dysfunction of V lead and damage to the septal vein in the process of the procedure, respectively. Fortunately, they were discharged without any other complications.
Conclusions
A deliberate approach for the procedure would be needed as well as successful insertion appropriate for the protocol of LBBAP. And long-term follow-up of complications should be needed.
Similar content being viewed by others


Background
Left bundle branch area pacing (LBBAP), which captures the left conduction system and progresses along the Purkinje system, has been introduced as a novel pacing technique. Through prior studies to assess the feasibility and clinical outcomes of LBBAP, the usefulness of LBBAP was identified and the pacing technique was generally used to improve the prognosis [1, 2]. Most studies focused on the criteria of LBBAP and the incidence of complications, such as septal perforation and lead dislodgement. We introduce two complications of LBBAP that have been rarely reported. This would become a significant clinical issue regarding LBBAP lead extraction and insertion.
Case presentation
Case 1
The patient, a 76-year-old man, underwent pacemaker insertion with a CAVB in June.2022. DDD type of pacemaker with LBBAP (Biotronik, Solia S60) was inserted. The baseline rhythm of the patient was RBBB, and pacing rhythm was also RBBB pattern. From the pattern, it can be inferred that the lead was located near the LBB area. At that time, the value of the pacemaker was within the normal range (V lead: sensing threshold–10.9, pacing threshold–1.7 voltage, impedance–507 Ω). (Fig. 1) He was discharged without any incident. However, one month later, the capture threshold of V lead was increased to 7.5 voltage and the unstable status of ventricular capture was identified. The capture threshold did not be normalized even with follow-up, so the revision of the V lead was conducted in January. 2023. In the process of the procedure, we tried to reposition the lead to the right ventricular septal area. However, we failed to unscrew and could not extract the V lead manually. An extraction device was not used because adhesion to the vessel was not suspected. Despite several attempts to remove the existing lead by transvenous lead extraction, the extraction failed. At that time, the tip of the lead was trapped in the ventricular myocardium tightly due to the malfunction of the screw. Therefore, we did not attempt to extract the lead with an extraction device aggressively because of the possibility of myocardial damage. The procedure was completed with the insertion of additional V lead at the apex of the right ventricle (RV) without extraction of V lead previously inserted (Fig. 2).

Initial chest X-ray and ECG after LBBAP procedure. The V lead was positioned at the septal area on the RAO and LAO view of chest X-ray. The RBBB pattern of the rhythm was maintained with V pacing

Failure of V lead extraction. Chest X-ray (RAO view). Atrial lead (white asterisk) was inserted in the right atrial appendage (RAA). The V lead previously inserted for LBBAP was into the part of the septum (blue arrow). Additional V lead for conventional pacing was positioned at the apex
Case 2
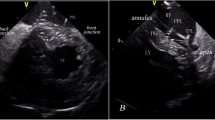
A 90-year-old man diagnosed with CAVB underwent the LBBAP procedure. DDD type of pacemaker with LBBAP (Biotronik, Solia S60) was used. According to the LBBAP protocol, the LBBAP sheath was placed at the RV (right ventricle) septal area, and the screw was inserted into the area, and then a contrast injection was performed to confirm whether the lead was positioned appropriately to the septum or not. However, the septal vein was identified with contrast injection unexpectedly and then coronary sinus drainage was noted (Fig. 3). The repositioning of the lead was decided due to concerns about complications, such as hematoma formation.

Damage of the septal vein. The septal vein was damaged by V lead for LBBAP inserted into the septum (green dotted circle). By infusion of contrast, coronary sinus was identified along the septal vein
Discussion and conclusions
According to the growing population treated with LBBAP, the demand for TLE will be also increased. Even in some cases of conventional lead insertion, TLE is challenging due to fibrosis and stenosis adjacent to the subclavian vein. In case 1, TLE failed even though it has not been long since the V lead was inserted. In this case, the pacing threshold increased unexpectedly without changes in lead impedance and lead insertion site. A significant increase in the LBBAP pacing threshold was reported in 0.7% of patients after 7.1 ± 5.0 months postimplantation [2]. Although there was the case report of successful lead extraction in LBBAP with a simple traction maneuver, the malfunction of the helix and the lead not being separated from the septum made TLE more challenging in some cases [3, 4]. In our case, the cause of the failed extraction of the V lead and the abrupt increase of the pacing threshold would be derived from the malfunction of the helix. However, for an accurate assessment of the case, it is necessary to remove the lead and visually evaluate it. Therefore, it would be needed to further maneuver rather than simple traction and conventional extraction devices.
To accomplish successful V lead insertion for LBBAP based on the cardiac anatomy, a prior study has been focused on describing the localization of the cardiac conduction system [5]. Considering cardiac vein anatomy, blood vessels are distributed in the septum. Because V lead should be inserted into the septum, damage to the vessel adjacent to the lead could occur. Therefore, detailed research on the blood vessel distribution around the conduction system is necessary. In case 2, we repositioned the V lead to another site and no further complication was identified. It is questionable whether minor damage to the septal vein by the lead causes additional complications at long-term follow-up or not.
These two cases are uncommon complications with the LBBAP procedure and the previous study to investigate the cause and solutions of the complications are lacking. We tried to focus on not only successful insertion appropriate for the protocol of LBBAP procedure is important, but also a deliberate approach for the procedure through various complications and long-term follow-up of complications should be needed. The case of failure in V lead extraction which is inserted into the ventricular septum emphasizes the demand for further traction maneuvers rather than conventional methods. Also, a careful approach is required as the process of inserting the V lead into the septum may cause damage to the vein.
Availability of data and materials
Not applicable.
Abbreviations
- LBBAP:
-
Left bundle branch area pacing
- TLE:
-
Transvenous lead extraction
- V lead:
-
Ventricular lead
- CAVB :
-
Complete atrioventricular block
- RV:
-
Right ventricle
References
Huang W, Su L, Wu S, et al. A novel pacing strategy with low and stable output: pacing the left bundle branch immediately beyond the conduction block. Can J Cardiol. 2017;33:1736.e1731-1736.e1733.
Jastrzębski M, Kiełbasa G, Cano O, et al. Left bundle branch area pacing outcomes: the multicentre European MELOS study. Eur Heart J. 2022;43:4161–73.
Sciria CT, Kogan EV, Mandler AG, et al. Low utilization of lead extraction among patients with infective endocarditis and implanted cardiac electronic devices. J Am Coll Cardiol. 2023;81:1714–25.
Wijesuriya N, Elliott MK, Mehta V, et al. Transvenous lead extraction in conduction system pacing. Front Physiol. 2022;13: 993604.
Shinohara G, Morita K, Hoshino M, et al. Three dimensional visualization of human cardiac conduction tissue in whole heart specimens by high-resolution phase-contrast CT ImagiUsing synchrotron radiation. World J Pediatr Congenit Heart Surg. 2016;7:700–5.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
SYP drafting the article and revising it for intellectual content. YC participate in the conception and design, acquisition of data. YSO participate in the conception and design, acquisition of data. SHK revising the article for intellectual content and final approval to be published.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
The case report was prepared underlying publication ethic guideline.
Consent for publication
All authors of the report agree with the publication.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Park, S., Choi, Y., Oh, YS. et al. The unexpected complications of the left bundle branch area pacing (LBBAP) maneuver: a case report. Int J Arrhythm 25, 9 (2024). https://doi.org/10.1186/s42444-024-00113-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42444-024-00113-w