
Abstract
Background
Recent studies have questioned the role of implanted cardiac defibrillators (ICDs) in nonischemic cardiomyopathy (NICM). Cardiac resynchronization therapy (CRT) can be delivered by a pacemaker (CRT-P) or an ICD (CRT-D). This meta-analysis assessed the effect of CRT-P versus CRT-D on mortality in patients with NICM.
Methods
Databases were searched for studies reporting the effect of CRT on all-cause mortality in patients with nonischemic cardiomyopathy (Ovid MEDLINE, EMBASE, Scopus, Web of Science, Google Scholar, and EBSCO CINAHL). The primary endpoint was all-cause mortality. The minimum duration of follow-up required for inclusion was one year. The search was not restricted to time or publication status.
Results
The literature search identified 955 candidate studies, 15 studies and 22,763 patients were included. Mean follow-up was 53 months (17–100 months). CRT-D in NICM was associated with lower all-cause mortality (log HR − 0.169, SE 0.055; p = 0.002) compared to CRT-P. Heterogeneity: df = 15 (P 0.03), I2 = 43; test for overall effect: Z = − 3.043 (P = 0.002).
Conclusion
CRT-D in NICM was associated with lower all-cause mortality than CRT-P.
Similar content being viewed by others


Introduction
Heart failure remains a highly prevalent disease worldwide with significant implications on morbidity and mortality as well as healthcare spending. In the USA alone, the incidence of heart failure is estimated to be around 400,000 per year with a prevalence of over 5 million patients and growing [1]. Patients with heart failure with reduced ejection fraction and wide QRS complex qualify for a cardiac resynchronization therapy-defibrillator (CRT-D) [2]. While the role of implantable cardioverter-defibrillator (ICD) implantation has been well established in ischemic cardiomyopathy (ICM), similar studies in nonischemic cardiomyopathy (NICM) have demonstrated conflicting results [3, 4]. There was a trend toward decreased mortality in the ICD arm of the DEFINITE trial which did not reach statistical significance [5]. The SCD-HeFT trial demonstrated a survival benefit with ICD implantation in patients with HFrEF irrespective of etiology compared to standard medical management including amiodarone [6]. In contrast, the DANISH trial did not show an improvement in long-term mortality in patients with NICM and therefore called into question the American Heart Association and American College of Cardiology’s guidelines for prophylactic ICD implantation in this patient subset [2, 3].
Another area of ongoing ambiguity is whether CRT-D is superior to cardiac resynchronization therapy-pacemaker (CRT-P) in patients with NICM. Several studies attempting to address this question have yielded inconsistent results [3, 7,8,9,10]. However, many of these studies were single-center retrospective studies and may have been underpowered. This meta-analysis was conducted to evaluate the effect of CRT-D as compared to CRT-P on mortality in patients with NICM.
Methods
Data search
The systematic review was conducted with a protocol in accordance with the Preferred Reporting of Items for Systematic reviews and Meta-Analyses (PRISMA) statement [11]. An experienced librarian fashioned a search strategy utilized to systematically locate relevant articles. Searches were conducted in October 2021 using the following databases: EMBASE, Ovid Medline, CINAHL, Cochrane Central Register of Controlled Trials, Web of Science: Science Citation Index Expanded, Latin American and Caribbean Health Sciences Literature (LILACS), and Google Scholar.
We used the following Mesh words:
((“Cardiac Resynchronization Therapy”[Mesh] OR “cardiac resynchronization therapy”[All Fields]) AND (“Defibrillators, Implantable”[Mesh] OR “defibrilator”[All Fields] OR “defibrillate”[All Fields] OR “defibrillated”[All Fields] OR “defibrillates”[All Fields] OR “defibrillating”[All Fields] OR “defibrillations”[All Fields] OR “defibrillator s”[All Fields] OR “defibrillators”[MeSH Terms] OR “defibrillators”[All Fields] OR “defibrillator”[All Fields] OR “defibrillation”[All Fields] OR “Electric Countershock”[Mesh] OR ("electric”[All Fields] AND “countershock”[All Fields]) OR “electric countershock”[All Fields])) AND ("nonischaemic”[All Fields] OR “nonischemic”[All Fields] OR “nonischemics”[All Fields]) AND ("cardiomyopathie”[All Fields] OR “cardiomyopathies”[MeSH Terms] OR “cardiomyopathies”[All Fields] OR “cardiomyopathy”[All Fields]).
Citations were uploaded to Rayyan (Rayyan QCRI, Qatar) [12] for combining the citations and removal of duplicates.
Study selection
Two investigators (MA and SS) independently screened the studies at the level of titles and abstracts. Afterward, the references were evaluated for inclusion based on a pre-set inclusion criterion. The pre-specified inclusion criteria were reporting the effect of CRT with or without ICD on all-cause mortality in patients with NICM with EF ≤ 35%. Exclusion criteria were data reporting mortality without comparison between CRT-D and CRT-P, follow-up less than 1 year, review articles, case reports, or publication in languages other than English. Any discrepancy was resolved by a third investigator (FA). The numbers of participants, year of publication, and hazard ratio was collected for included studies. The primary endpoint was all cause mortality.
Statistical analysis
Meta-analysis was performed using Comprehensive Meta-analysis software, version 3 (Biostat, Inc). We used a random-effects model to examine the association between CRT-D and CRT-P and outcomes, which were presented a log hazard ratio (HR) with standard error and Z-value. The extent of heterogeneity was determined by I2 (ranging from 0 to 100%). Statistical significance was considered with a P-value < 0.05, and all tests were 2-sided. Funnel plot of standard error by log HR was created to qualitatively assess publication bias.
Results
Literature search and study selection
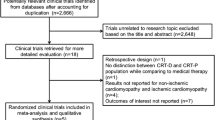
The first stage of literature search identified 955 eligible studies. The process of study inclusion is delineated in detail in Fig. 1. By screening the titles and abstracts, 932 studies were excluded. The remaining 23 articles were reviewed in full text for relevance, and 15 studies were eligible for meta-analysis for the outcomes of CRT-D versus CRT-P in NICM. Abstracts published with detailed information were included for two reasons: Analysis with and without including such data is recommended by the Agency for Healthcare Research and Quality (AHRQ), the Joanna Briggs Institute Reviewer’s Manual, and PRISMA for systematic review protocols (PRISMA-P) [13].

PRISMA flowchart. Flow diagram depicts study selection for inclusion in the meta-analysis according to the PRISMA statement for reporting systematic reviews and meta-analyses
Study, Patient, and Procedural Characteristics
The study population included 22,763 patients for a mean follow-up of 53 months (17–100 months). They were 76% men with a mean age of 73.6 ± 4 years and a mean left ventricular ejection fraction of 27% (range 21–35%). Table 1 summarizes the characteristics of the included studies. The studies included patients that had a CRT device as primary therapy or as an upgrade from a pacemaker. Most of the included studies did not stratify the results based on age, sex, race, or presence of left bundle branch block.
Association between CRT-D versus CRT-P and mortality in patients with NICM
CRT-D was associated with lower all-cause mortality (log HR − 0.169, SE 0.055; p = 0.002) as compared to CRT-P. There was significant heterogeneity: df = 15 (P 0.03), I2 = 43; test for overall effect: Z = − 3.043 (P = 0.002) (Figs. 2, 3).

Forest plot demonstrating impact of CRT-D on long-term (> 1 year) mortality in patients with NICM compared to CRT-P. In patients with NICM and indication for CRT and ICD: CRT-D was associated with lower all-cause mortality (log HR − 0.169, SE 0.055; p = 0.002) compared to CRT-P. Heterogeneity: df = 15 (P 0.03), I2 = 43; Test for overall effect: Z = − 3.043 (P = 0.002)

Funnel plot standard error by log hazard ratio: heterogeneity: df = 15 (P 0.03), I2 = 43 which indicates mild heterogeneity. A risk of bias summary added as a Additional file 1: Table S1
Discussion
The major finding of our study is that CRT-D was associated with lower all-cause mortality than CRT-P in subjects with NICM and EF ≤ 35%. To our knowledge, this meta-analysis is the most comprehensive review of this question to date. The results are consistent with several other recent meta-analyses that also incorporated the data from the DANISH trial, where 58% of patients received CRT [14,15,16]. Our results contradict the most recent meta-analysis, which reported no additional survival benefit with CRT-D in NICM [17]. The included studies did not stratify according to QRS morphology or NYHA class.
We hypothesize that the results differ because our work included the most recent studies on this topic including an updated analysis from the COMPANION trial [17], which reported a survival benefit with CRT-D. Additionally, there may be differences in the benefit of CRT-D over CRT-P based on age. In the DANISH trial, subgroup analysis demonstrated that younger patients (< 68 years old) derived the greatest benefit from prophylactic ICD implantation independent of CRT status [3]. Similar findings were reported by Gras et al. [18], who found that CRT-D only reduced mortality in younger patients (< 75 years old). These observations could be explained by the natural progression of heart failure, as the predominant mode of death may switch from life-threatening arrhythmias to pump failure [18]. Thus, CRT-D may be more beneficial when implanted earlier in the disease course. This is further substantiated by the results of the REVERSE trial, where CRT-D was associated with a reduction in all-cause mortality compared to CRT-P in patients with mild, predominantly NYHA class II heart failure [18, 19].
Several studies have suggested that the mortality benefit of CRT-D is present in the short term but subsequently attenuates over time [7, 8]. In the COMPANION trial, the survival curves for CRT-D and CRT-P merged by 9 months [20]. However, this was not a primary endpoint for the study and the study was underpowered to assess temporal changes in the mortality benefit. The DANISH trial reported similar findings with longer follow-up (67 months vs. 17 months for COMPANION), but was also underpowered for this secondary analysis.
Since NICM is a heterogeneous disease with many different etiologies, it is possible that the inconsistent results of previous studies are also due to differences in the disease subsets, and the geographic location of the study populations could affect the proportion of disease subsets represented. These data could not be extracted from the studies included in this meta-analysis. In addition, the time frame of the studies may affect outcomes. Many guideline directed medical therapies (GDMT) were not approved by regulatory authorities or implemented until recently, and there is wide variability in GDMT adherence and compliance [21]. This information is not reported in the studies that we included in our meta-analysis and may contribute to the heterogeneity that we observed. Re-evaluation of Optimal Re-synchronization Therapy in Patients with Chronic Heart Failure (RESET-CRT) (NCT03494933) is an ongoing multicenter randomized controlled trial that will determine whether CRT-P is non-inferior to CRT-D with respect to all-cause mortality on a background of contemporary GDMT.
The presence of scar on cardiac magnetic resonance imaging (CMR) has emerged as a potent predictor of cardiovascular mortality in NICM. Multiple studies reported an association between the presence of late gadolinium enhancement (LGE) and all-cause mortality, cardiovascular mortality, ventricular tachyarrhythmia, and sudden cardiac death [22]. This information is also not reported in the studies that we included in our meta-analysis, which could contribute to heterogeneity. There are two ongoing prophylactic ICD trials that use LGE as an inclusion criterion: cardiac magnetic resonance GUIDEd management of mild-moderate left ventricular systolic dysfunction (CMR-GUIDE) (NCT01918215) and cardiac magnetic resonance guidance of implantable cardioverter-defibrillator implantation in nonischemic dilated cardiomyopathy (CMR-ICD) (NCT04558723). These studies will also assess CRT response in patients with LGE, since scar burden and location can affect the efficacy of CRT [22].
This meta-analysis is subject to several limitations. The mortality benefit of CRT-D could diminish with longer-term follow-up as a result of favorable LV reverse remodeling with CRT [20] and changes in the predominant mode of death [3]. The landscape of GDMT for NICM has vastly changed over the past decade. As novel therapeutic agents including angiotensin receptor neprilysin inhibitors and sodium-glucose co-transporter 2 inhibitors are introduced with further reduction in all-cause mortality, the risk reduction associated with CRT-D over CRT-P may diminish. In most contemporary studies, medical therapy was limited to angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers, and mineralocorticoid receptor antagonists [4]. Additional adequately powered randomized studies with long-term follow-up and contemporary GDMT are needed to substantiate the clinical benefit of CRT-D over CRT-P in NICM patients.
Conclusion
CRT-D was associated with lower all-cause mortality than CRT-P in subjects with NICM.
Availability of data and materials
Authors can be contacted for any supporting data.
Abbreviations
- ICD:
-
Implantable cardioverter-defibrillator
- ICM:
-
Ischemic cardiomyopathy
- NICM:
-
Nonischemic cardiomyopathy
- CRT-D:
-
Cardiac resynchronization therapy-defibrillator
- CRT-P:
-
Cardiac resynchronization therapy-pacemaker
- PRISMA:
-
Preferred Reporting of Items for Systematic Reviews and Meta-Analyses
References
Saba S, McLaughlin T, He M, Althouse A, Mulukutla S, Hernandez I. Cardiac resynchronization therapy using pacemakers vs defibrillators in patients with nonischemic cardiomyopathy: the United States experience from 2007 to 2014. Hear Rhythm. 2019;16(7):1065–71.
Tracy CM, Epstein AE, Darbar D, DiMarco JP, Dunbar SB, Estes NAM 3rd, et al. 2012 ACCF/AHA/HRS focused update of the 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm. Circulation. 2012;126(14):1784–800.
Køber L, Thune JJ, Nielsen JC, Haarbo J, Videbæk L, Korup E, et al. Defibrillator implantation in patients with nonischemic systolic heart failure. N Engl J Med. 2016;375(13):1221–30.
Bethany D, Chaoqun M, Varosy PD, Kao DP, Saxon LA, Feldman AM, et al. The addition of a defibrillator to resynchronization therapy decreases mortality in patients with nonischemic cardiomyopathy. JACC Hear Fail. 2021;9(6):439–49. https://doi.org/10.1016/j.jchf.2021.02.013.
Kadish A, Dyer A, Daubert JP, Quigg R, Estes NAM, Anderson KP, et al. Prophylactic defibrillator implantation in patients with nonischemic dilated cardiomyopathy. N Engl J Med. 2004;350(21):2151–8.
Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, Boineau R, et al. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure. N Engl J Med. 2005;352(3):225–37.
Looi K-L, Gajendragadkar PR, Khan FZ, Elsik M, Begley DA, Fynn SP, et al. Cardiac resynchronisation therapy: pacemaker versus internal cardioverter-defibrillator in patients with impaired left ventricular function. Heart. 2014;100(10):794–9.
Kutyifa V, Geller L, Bogyi P, Zima E, Aktas MK, Ozcan EE, et al. Effect of cardiac resynchronization therapy with implantable cardioverter defibrillator versus cardiac resynchronization therapy with pacemaker on mortality in heart failure patients: results of a high-volume, single-centre experience. Eur J Heart Fail. 2014;16(12):1323–30.
Reitan C, Chaudhry U, Bakos Z, Brandt J, Wang L, Platonov PG, et al. Long-term results of cardiac resynchronization therapy: a comparison between CRT-pacemakers versus primary prophylactic CRT-defibrillators. Pacing Clin Electrophysiol. 2015;38(6):758–67.
Witt CT, Kronborg MB, Nohr EA, Mortensen PT, Gerdes C, Jensen HK, et al. Adding the implantable cardioverter-defibrillator to cardiac resynchronization therapy is associated with improved long-term survival in ischaemic, but not in non-ischaemic cardiomyopathy. Europace. 2016;18(3):413–9.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. https://doi.org/10.1186/s13643-016-0384-4.
Scherer RW, Saldanha IJ. How should systematic reviewers handle conference abstracts? A view from the trenches. Syst Rev. 2019;8(1):264.
Golwala H, Bajaj NS, Arora G, Arora P. Implantable cardioverter-defibrillator for nonischemic cardiomyopathy: an updated meta-analysis. Circulation. 2017;135:201–3.
Beggs SAS, Jhund PS, Jackson CE, McMurray JJV, Gardner RS. Non-ischaemic cardiomyopathy, sudden death and implantable defibrillators: a review and meta-analysis. Heart. 2018;104(2):144–50.
Luni FK, Singh H, Khan AR, Malik SA, Khawaja O, Riaz H, et al. Mortality effect of ICD in primary prevention of nonischemic cardiomyopathy: a meta-analysis of randomized controlled trials. J Cardiovasc Electrophysiol. 2017;28(5):538–43.
Patel D, Kumar A, Black-Maier E, Morgan RL, Trulock K, Wilner B, et al. Cardiac resynchronization therapy with or without defibrillation in patients with nonischemic cardiomyopathy: a systematic review and meta-analysis. Circ Arrhythm Electrophysiol. 2021;14(6):e008991.
Gras M, Bisson A, Bodin A, Herbert J, Babuty D, Pierre B, et al. Mortality and cardiac resynchronization therapy with or without defibrillation in primary prevention. Europace. 2020;22(8):1224–33.
Linde C, Abraham WT, Gold MR, St John Sutton M, Ghio S, Daubert C; REVERSE (REsynchronization reVErses Remodeling in Systolic left vEntricular dysfunction) Study Group. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008;52(23):1834–43.
Bristow MR, Saxon LA, Boehmer J, Krueger S, Kass DA, De Marco T, et al. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350(21):2140–50.
Bhatt AS. Adherence to evidence-based therapies in heart failure. JACC Hear Fail. 2021;9(12):887–9. https://doi.org/10.1016/j.jchf.2021.07.007.
Alba AC, Gaztañaga J, Foroutan F, Thavendiranathan P, Merlo M, Alonso-Rodriguez D, et al. Prognostic value of late gadolinium enhancement for the prediction of cardiovascular outcomes in dilated cardiomyopathy: an international, multi-institutional study of the MINICOR Group. Circ Cardiovasc Imaging. 2020;13(4):e010105.
Drozd M, Gierula J, Lowry JE, Paton MF, Joy E, Jamil HA, et al. Cardiac resynchronization therapy outcomes in patients with chronic heart failure: cardiac resynchronization therapy with pacemaker versus cardiac resynchronization therapy with defibrillator. J Cardiovasc Med. 2017;18(12):962–7.
Barra S, Boveda S, Providência R, Sadoul N, Duehmke R, Reitan C, et al. Adding defibrillation therapy to cardiac resynchronization on the basis of the myocardial substrate. J Am Coll Cardiol. 2017;69(13):1669–78.
Leyva F, Zegard A, Umar F, Taylor RJ, Acquaye E, Gubran C, et al. Long-term clinical outcomes of cardiac resynchronization therapy with or without defibrillation: impact of the aetiology of cardiomyopathy. Europace. 2018;20(11):1804–12.
Wang Y, Sharbaugh MS, Althouse AD, Mulukutla S, Saba S. Cardiac resynchronization therapy pacemakers versus defibrillators in older non-ischemic cardiomyopathy patients. Indian Pacing Electrophysiol J. 2019;19(1):4–6.
Liang Y, Wang J, Yu Z, Zhang M, Pan L, Nie Y, et al. Comparison between cardiac resynchronization therapy with and without defibrillator on long-term mortality: a propensity score matched analysis. J Cardiol. 2020;75(4):432–8.
Veres DR. Long-term mortality benefit of adding an ICD to CRT in non-ischemic patients. EP Eur. 2021;23(Supplement_3):euab116.465. https://doi.org/10.1093/europace/euab116.465.
Acknowledgements
Not applicable.
Funding
None.
Author information
Authors and Affiliations
Contributions
MA-S contributed to conceptualization; MA-S and MT contributed to data curation and formal analysis; none contributed to funding acquisition; AS, RF, and ER contributed to investigation, writing—review and editing, and supervision; FA contributed to methodology and resources; ER contributed to project administration; MT contributed to software; MA-S and FA contributed to validation and visualization; and MT and FA contributed to roles/writing—original draft.
Corresponding author
Ethics declarations
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors report no relevant conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Risk of bias summary: the risk of bias in the included studies was low for almost all measures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Al-Sadawi, M., Aslam, F., Tao, M. et al. Is CRT-D superior to CRT-P in patients with nonischemic cardiomyopathy?. Int J Arrhythm 24, 3 (2023). https://doi.org/10.1186/s42444-023-00085-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42444-023-00085-3