
Abstract
Background
Ozone therapy is highly demarcated in the dental field owing to its efficient antimicrobial action in its gaseous and aqueous forms. One of the most common difficulties accompanied by utilizing dentures is denture stomatitis (DS) which is principally triggered by Candida albicans (C. albicans).
Objectives
Assessing and comparing the impact of ozonated water versus chlorhexidine mouthwash on healing of intra-oral inflammations associated with complete dentures.
Subjects and methods
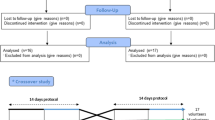
Fifty middle-aged male completely edentulous patients wearing complete dentures were screened for the possibility of having any accompanied DS and/or C. albicans. Patients were randomly distributed into two groups. Group I patients were treated with chlorhexidine mouthwash and oral hygiene measures (OHM); while, Group II patients received ozonated water as a mouthwash and OHM. Evaluation of inflammation, pain grade, and oral Candidiasis count took place for all patients in all visits; from the initial day of treatment and after 7, 14, and 30 days.
Results
The inflammation’s area and severity together with pain grade showed a significant decrease with time when using both chlorhexidine mouthwash and ozonated water. Comparing the use of chlorhexidine mouthwash and ozonated water together showed insignificant differences. Regarding the Candida forming units (CFU) there was a significant decrease in the colonies number over time, but with insignificant difference between the two groups.
Conclusions
Ozonated water showed favorable results in reducing the area and severity of inflammation and pain grade. Ozonated water has an antifungal effect and can be used as an alternative mouth rinse in treating denture stomatitis.
Similar content being viewed by others


Background
Denture sanitary habits that should be tracked to guarantee its cleanliness and avoid oral inflammations particularly during sleeping are demarcated as denture hygiene and its maintenance is one of the major challenges faced by most denture wearers. Accordingly, these geriatric patients especially the disabled ones are experiencing poor oral and denture hygiene together with the incidence of xerostomia, occlusal trauma, and ill-fitting dentures that initiate oral mucosal inflammations, ulcerations, and infections. Dentures’ sides act as a reservoir for gathering plaque by the retained diet beneath dentures. Sequentially creating microbial plaque and cultivating versatile species together with the lack of satisfactory hygienic measures. Hence, denture plaque triggers oral soft tissue hazards and denture stomatitis (DS) is a module; thus, adequate oral and denture hygienisity is obligatory (Sen and Sen 2020; Kumar et al 2016; Sansriti et al 2017; Singh et al 2017; Abhishek et al 2020).
Denture stomatitis is an asymptomatic benign chronic highly prevalent denture-related mucosal lesion (DML) which is further identified as denture-induced or related stomatitis. Despite its superior prevalence, it is rarely noticed for its asymptomatic nature, although mild pain, bleeding, itching, or burning sensations are reported by a few patients in areas affected. Its incidence is multifactorial but Candida albicans (C. albicans) is considered as the DS prime etiological one and the principal pathogen for such inflammation. Furthermore, C. albicans is notable for its supreme ability to adhere to both oral and plastic surfaces and accordingly cope with the mechanical washing salivary effect and colonize successfully. Thus C. albicans is termed as the most opportunistic pathogen among the Candida species (Sharabasy et al. 2022, Preethy and Sabarigirinathan 2022; Nader et al 2023).
Moreover, approaches for oral and denture hygiene are either mechanical or chemical. The mechanical technique has been considered the most suitable hygienic method employed for a long time. Although employing water and a toothbrush is the most common mechanical approach utilized, its limited effect in removing the biofilms’ microbes and encouraging denture plaque formation by influencing its surface are modules for its drawbacks. Even though employing chemical disinfectants and mouthwashes as the chemical approaches succeeded in diminishing the intra-oral biofilm microorganisms, their superior side effects have a deleterious impact on patients, acrylic resin, and prosthesis components. Chlorhexidine is determined as the highly prevalent broad-spectrum antimicrobial agent, causing disruption of cellular membranes. It is thus currently used as a disinfectant agent for cleaning non-living clinical surfaces and catheters. It is biocompatible, being used orally as an antiseptic mouthwash by dental practitioners and the general public to prevent bacterial biofilm and plaque buildup. The latter are potentially causative for dental caries, plaque-induced gingivitis, periodontitis and oral soft tissue disease. Chlorhexidine has an antimicrobial effect on bacteria, viruses and fungi. It is considered as the golden standard method in controlling plaque and has been utilized for a while for its impact in diminishing C. albicans (Orhun and Ahmet 2016; Reham and Neven 2020; Brookes et al 2020; Claudia et al 2023, Kaio et al. 2023).
Ozone (O3) is a natural tri-oxygen molecule presented in the atmosphere as a gas with 1–10 ppm concentration or fabricated by ozone generators. Its high density motivates its downward diminishing from heights and integration with surrounding pollutants, thus being a key member of earth’s self-purifying procedure. Ozone is considered a chief therapeutic agent owing to its efficient disinfection against bacteria, fungi, and viruses including C. albicans in either phase gaseous or aqueous. A multi-dimensional bio-oxidative curative ozone remedy provided out of gas, oil, or water is demarcated as ozone therapy. Ozone therapy via employing ozonated water as a recent advanced hygienic measure has fruitful outcomes in diminishing the biofilm microorganisms with minimal exposure periods and remarkable anti-inflammatory effects (Kumar et al 2014; Orhun and Ahmet 2016; Claudia et al 2023; Mostafa et al 2023).
Even though the plentiful ozone therapy merits its restricted usage in hyperthyroidism, thrombocytopenic, epileptic cases, ozone sensitivity, blood coagulation tendency, alcoholism, and pregnant patients together with induction of faintness, weakness, and allergic skin responses are some of its drawbacks. Considering ozonated water as a potential disinfectant against oral pathogens, it is crucial to compare its effectiveness with the established mouthwashes currently employed in dentistry (Kumar et al 2014; Mostafa et al 2023).
Accordingly, this research aimed to both assess and compare the impact of ozonated water versus chlorhexidine mouthwash on the healing of intra-oral inflammations associated with complete acrylic resin dentures. The null hypothesis was that ozonated water and chlorhexidine mouthwashes have the same impact on the treatment of denture-related stomatitis.
Subjects and methods
Study design
Fifty middle-aged male completely edentulous patients wearing complete dentures visiting the Excellence Medical Centre, National Research Centre, Cairo, Egypt were screened for the possibility of having any accompanied denture stomatitis (DS) and/or Candida albicans (C. albicans). Patients were all randomly distributed into two groups. Group I patients were treated with chlorhexidine mouthwash and oral hygiene measures (OHM); while, Group II patients received ozonated water as a mouthwash and OHM. Evaluation of inflammation, pain grade, and oral Candidiasis count took place for all patients in all visits; initiating from the initial day of treatment and then after 7, 14, and 30 days.
Ethical approval and clinical trial registration
The current research has been applied to the Code of Ethics of the World Medical Association, following the ethics stated in the Declaration of Helsinki in 1975. This research has been permitted by the “Medical Research Ethical Committee of the National Research Centre, Cairo, Egypt” with agreement number 4447082022. All patients were up-to-date with the existing study’s practical phases and contracted the printed consent. The research was registered on ClinicalTrials.gov with the identifier: NCT06021847.
Sample size calculation
The Sample size was estimated liable on preceding research as a reference (Aoun et al. 2015). Accordingly, when the mean ± standard deviation of Candida albicans count in the chlorhexidine group was (8 ± 18.807), while the estimated mean difference with the other group was (17) the minimally accepted sample size was 20 per group when the power was 80% and type I error probability was 0.05. The total sample size was enlarged to 25 per group to reward 20% drop out. The independent t test was employed to estimate sample size by using P.S. power version 3.1.6.
Inclusion and exclusion criteria
The inclusion criteria were completely edentulous male patients aged from 45 to 50 years wearing heat-cured acrylic resin complete dentures and suffering from denture stomatitis. Though exclusion criteria were smokers, uncooperative patients together with those having systemically immunosuppressive diseases, Temporomandibular joint (TMJ) disorders, parafunctional habits, and history of radiotherapy or chemotherapy.
Methods
Preparation of ozonated water
Ozonated water as a mouthwash was prepared utilizing Ozone of (2–4 mg/l) for 1 min. in a 25 mg of double distilled water 37 °C employing an Ozone generator (Ozone generator type N 1888A, China.)(Celakil et al 2017).
Patient's instructions and follow-up during the healing process
All patients in this study were properly diagnosed and instructed to have strict oral and denture hygienic measures together with sticking to their frequent follow-up visits to regularly check their healing progress. Furthermore, proper elimination of all the reasons for their inflammation and pain from their prosthesis took place.
Assessment of inflammation and pain grade
Inflammation was estimated by utilizing the Schwartz et al 2016. Inflammation index comprises two color-coded sections; the yellow one represents the area where inflammation is located intraorally and the other green one symbolizes its severity. The yellow area section provides a choice of 4 answers, and each is given a score (0 = No inflammation; 1 = Inflammation of the palate extending up to 25% of the palatal denture-bearing tissue; 2 = Inflammation of the palate covering between 25 and 50% of the palatal denture-bearing tissue; 3 = Inflammation covering more than 50% of the palatal denture-bearing tissue). The green severity section provides a choice of 4 answers, and each is given a score (0 = Normal tissue; 1 = Mild inflammation (slight redness, no swelling or edema); 2 = Moderate inflammation (redness with some edema); 3 = Severe inflammation (acutely inflamed redness, edema).
Whereas, the pain scale was estimated by employing the Granick et al 1998 pain index which comprises 5 grades of pain providing a choice of 5 answers, and each is given a score (Grade 0 = No symptoms; Grade 1 = Mild discomfort and capable of eating; Grade 2 = Moderate discomfort but still capable of eating; Grade 3 = Sever discomfort and unable to eat; Grade 4 = Tolerated pain and unable to eat). The overall score was estimated by gathering the replies to all the questions. The lowest score revealed a lack of inflammation with normal tissues and asymptomatic pain, consequently a satisfactory perception of an individual’s oral condition; as displayed in Table 1.
Assessment of oral candidiasis
Oral Candidiasis was assessed employing the swab technique, as swabs were obtained for all patients from both the palate and maxillary dentures’ fitting surfaces to detect the existence or absence of C. albicans and its counting if present.
a. Preparation of chromogenic agar media for identification of Candida albicans.
A suspension was fabricated comprising 47.9 gm of the medium properly mixed in one liter of distilled water and dissolved by heating with regular whisking. Then accompanied by boiling for one minute till the entire dissolution and followed by dispersion into Petri dishes. Then a homogeneous, free-flowing, clear amber and slightly opalescent medium was ready and stored at 8–15 °C.
b. Isolation of Candida albicans.
Swabs were attained by dynamic rubbing of both palate and the entire maxillary complete dentures’ fitting surfaces by employing a sterile cotton-tipped wooden swab for 30 s/ patient. Then these cotton swabs were inoculated separately in 10.0 mL sterile screw-capped tubes, where each tube comprised 2.5 mL nutrient broth medium then incubated at 37 ºC for 48-h incubation period in a peculiar incubator (*VWR Shel-Labs 1530 Laboratory Incubator-China). Then 0.1 ml from nutrient broth medium was smeared on the surface of Sabouraud's agar plates by plate streak method. After that the plates were incubated at 37 °C for 48 h. Candida colonies appeared to be white to creamy in color, smooth and glistering. The colony forming units of organisms were quantitated and counted by naked eye as displayed in Fig. 1.

Candida albicans count decreased in both palate and denture swabs taken through the initial day of treatment and after 30 days
Statistical analysis
All numerical data were presented as mean and standard deviation values. Normality exploration of the given data was accomplished utilizing the Shapiro Wilk and Kolmogorov Smirnov test which revealed area and degree of inflammation as well as degree of pain demonstrated nonparametric data. Accordingly, a comparison between different follow-up visits was performed by employing Friedman`s test accompanied by Dunn's multiple comparisons test; while, a comparison among the two dissimilar groups was performed by utilizing Mann–Whitney`s test. On the other hand, Candida albicans growth revealed normal data distribution. Consequently, comparison between different follow-up visits was performed by employing Repetitive One-Way ANOVA test accompanied by Tukey`s Post Hoc test for multiple comparisons; while, comparison between different surfaces of both groups was accomplished via One-Way ANOVA test followed by Tukey`s Post Hoc test for multiple comparisons. The level of significance was set as p value ≤ 0.05.
Results
Assessment of inflammation and pain
The severity and area of inflammation associated with complete denture wearing were assessed by Schwartz et al 2016 inflammation index; while, the pain was evaluated by Granick et al. Pain scale after utilizing chlorhexidine mouthwash for group I and freshly prepared ozonated water for group II, as their assessment took place weekly for one month. Friedman`s test accompanied by Dunn’s multiple comparisons test revealed that there was a highly remarkable decrease in severity and areas of inflammation throughout time in the two groups. Likewise, pain showed a high significant decrease in both groups as reaching the end of the follow-up period with p < 0.0001 as displayed in Table 2 and Fig. 2.

Bar chart representing area and degree of inflammation and degree of pain regarding both groups at different follow-up visits
While Mann–Whitney’s test was employed to compare the two groups and data exhibited that there was an insignificant difference between the two groups regarding both area and severity of inflammation as well as pain scale with p > 0.05 at different visits, as displayed in Table 2 and Fig. 2.
Assessment of Candida albicans growth
The Candida albicans growth was assessed by counting the Candida forming units (CFU) from swabs taken from the patient’s palate and complete dentures of each group. A repetitive one-way ANOVA test was utilized to compare the follow-up visits in both groups and data revealed a highly significant difference in the CFU by the time p < 0.0001, accompanied by Tukey`s Post Hoc test which demonstrated the significant decrease in the CFU from the palate and denture surface of group I and II during the follow-up as displayed in Table 3 and Fig. 3.

Bar chart representing CFU value of candida strains in palatal and denture surfaces regarding both groups at different follow-up visits
Whereas one-way ANOVA test was employed to compare CFU resulting from the palate and denture swabs taken in both groups revealed highly significant difference between them as p < 0.0001, accompanied by Tukey`s Post Hoc test which demonstrated that denture surface of group I was remarkably the highest, then palatal surface of group I, then denture surface of group II, while palatal surface of group II was significantly the lowest in the all follow-up visit, as presented in Table 3 and Fig. 3.
Discussion
Denture stomatitis is multifactorial disease and characterized by the fungal and bacterial accumulations on the denture surface together with areas of oral inflammation. It has been stated that 72% of denture wearers of senior people having denture stomatitis. The appropriate dentures cleansing routine is essential to avoid denture stomatitis and ensure healthy supporting tissues. Among the oral hygiene routine is the use of chlorohexidine which is the gold standard antimicrobial mouthwash which has been broadly utilized as the antiseptic of choice for both dentures and dental plaque disinfection that might be infected with Candida albicans. It is commonly used by dental practitioners and public (Brookes et al 2020. Sartawi et al. 2021, Jeon et al. 2022, Chavarría 2022).
Ozone therapy recently showed favorable outcomes in reducing pain, treatment of inflammation, and bactericidal effect in medicine and dentistry due to its anti-inflammatory, analgesic, and anti-edema properties through the allogenic receptors oxidation and the anti-nociceptive system stimulation. The dual bond ozonolysis leads to cytoplasmic cell membrane deactivation and inducing the antibacterial effect of ozone. Its harmless impact on the human body cells is owing to its extensive antioxidant capability. Ozone can be applied in different forms such as gaseous, aqueous, and oil. The aqueous form of ozone (ozonated water) is not very stable because O3 converts to oxygen (O2) very easily. For this reason, it should be freshly prepared prior to its application. Therefore, the present study evaluated the effect of fresh prepared ozonated water in comparison with chlorhexidine mouthwash in the management of denture-induced oral stomatitis. The concentration of ozonated water is very critical for its anti-inflammatory and antibacterial effect so in this contemplate 2.4gm/l was employed as indicated in other studies that reported that this concentration is highly effective in reducing the bacterial and fungal count and has an anti-inflammatory outcome (Suh et al 2019, Barczyk 2023, Katti and Chara 2013, Lubojanski et al. 2021, Durgapal and Shetty 2022).
Outcomes of this research displayed a remarkable decrease in the area and severity of inflammation and the degree of pain by time when the patients suffering from denture stomatitis employing either chlorhexidine mouthwash or ozonated water. Chlorhexidine mouthwash has a broad-spectrum antibacterial impact by benefit of its superior intra-oral substantivity. Several considerations have revealed the chlorhexidine valuable criteria in denture stomatitis management and pain decline, but chlorhexidine utilization is inconvenienced by some obstacles that might distress patient compliance such as bad taste and staining ability (Tütüncüoğlu et al 2022, Kaur et al. 2019, James et al. 2017, Aoun et al. 2015).
The inflammatory process can be adjusted and both the immune reaction and blood circulation can be augmented via the ozonated water oxidant ability thru their impact in toxins oxidization and excretion rapidly. Moreover, it enhances the blood capability in carrying oxygen, which in turn enhances the inflamed tissues cellular metabolism and advances energy utilization via triggering aerobic metabolism (glycolysis, Krebs cycle, and b-oxidation of fatty acids). Consequently, advancement of cell regeneration, activity and tissue curing take place. This was in accordance with another study applied on a group of both male and female prostheses wearing candidates exhibited that ozone diminishes the traumatic ulcer’s size and pain, quickens the diseased tissue regeneration, and thus treatment abbreviation (Niveda and Malaiappan 2019, de Sire et al. 2022, Bocci et al 2011, Gandhi et al. 2019, Alzarea 2019).
Although a previous study found that ozonated water had a remarkable impact in diminishing both gingival and plaque index together with pocket depth probing in comparison with 0.2% chlorhexidine mouthwash when treating chronic periodontitis patients. Whereas, in the current research there was a significant decrease in both areas and severity of inflammation as well as the degree of pain by time in both groups but there was insignificant difference between the chlorhexidine mouthwash and ozonated water in denture stomatitis treatment. This was in harmony with another research reported that ozonated water and chlorhexidine mouth rinse were equally effective in reducing gingivitis and inflammation (Dodwad et al 2011; Parkar et al 2017).
Candida albicans is one of the oral lesions and denture stomatitis inducing factors. It computes around 70–80% of the isolated microorganisms from the oral mucosal infections Regarding the CFU of C. albicans isolated from patient’s palate and denture in each group were significantly decreased by time when using ozonated water and chlorohexidine mouthwash; while, there was no significant difference between the ozonated water and chlorohexidine mouthwash (Ribeiro et al. 2012).
Many researches inspected utilizing chlorhexidine both as a mouthwash and denture immersing solution for denture stomatitis management and highlighted the chlorhexidine impact in abolishing C. albicans on the PMMA denture surface and remarkably diminishing the palatal inflammation. On the other hand, ozonated water is a potential antiseptic agent that is active in inhabiting gram-positive, gram-negative bacteria and oral C. albicans thru hitting the cell membrane’s lipoproteins and phospholipids, thus inhibiting microorganisms’ development and expansion (Aoun et al. 2015, Tiwari et al 2017).
A study has investigated the ozonated water impact on Candida albicans in heat cure polymethyl methacrylate (PMMA) and highlighted the comparable effect of ozone water with the affordable denture disinfectants to the extent that within 1 min nearly all of microorganisms were withdrawn. Further study stated that soaking of acrylic denture base material in ozonated water had no effect on surface roughness but it slightly decease the surface hardness, thus ozonated water acts as a good soaking media for patients wearing PMMA prosthesis. The CFU from the patient’s palate revealed a significant decrease than patient’s denture throughout the follow-up period due to roughness of acrylic resin that facilitated C. albicans adhesion (McReynolds 2023, Sen and Sen 2020, Mostafa et al 2023). The current study findings support its previously postulated hypothesis.
Conclusions
Within limitations of the current research, it has been concluded that ozonated water is a promising alternative mouth rinse owing to its quite impact in inhibiting Candida albicans’ growth and treating denture stomatitis. Furthermore, the effortlessly ozonated water preparation makes it an adjunct to tooth brushing and flossing routine.
Limitations and recommendations
The short-range follow-up period was the limitation faced during the study. Accordingly, upcoming research with prolonged follow-up intervals to record the perception of PMMA complete denture patients to ozonated water and chlorohexidine mouthwash is suggested to take place. Furthermore, it is highly recommended to evaluate stability of ozonated water at room temperature, as well as, estimation of wide range of bacteria and fungus that initiate denture stomatitis.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article.
Abbreviations
- DS:
-
Dentures stomatitis
- C. albicans :
-
Candida albicans
- OHM:
-
Oral hygiene measures
- CFU:
-
Candida forming units
- O3 :
-
Ozone
- O2 :
-
Oxygen
- PMMA:
-
Polymethyl methacrylate
References
Abhishek S, Vishal T, Alvi F, Harees S, Shuchi S (2020) The dental applications of ozone: a review article. Int Dent J Stud Res 8(4):132–135
AlZarea B (2019) Management of denture-related traumatic ulcers using ozone. J Prosthet Dent 121(1):76–82
Aoun G, Cassia A, Berberi A (2015) Effectiveness of a chlorhexidine digluconate 0.12% and cetyl-pyridinium chloride 0.05% solution in eliminating Candida albicans colonizing dentures: a randomized clinical in vivo study. J Contemp Dent Pract. 16(6):433–436
Barczyk I, Masłyk D, Walczuk N, Kijak K, Skomro P, Gronwald H, Pawlak M, Rusińska A, Sadowska N, Gronwald B, Garstka AA (2023) Potential clinical applications of ozone therapy in dental specialties—a literature review, supported by own observations. Int J Environ Res Public Health 20(3):2048
Bocci V, Zanardi I, Travagli V (2011) Ozone acting on human blood yields a hormetic dose-response relationship. J Trans Med 9:66–77
Brookes ZLS, Bescos R, Belfield LA, Ali K, Roberts A (2020) Current uses of chlorhexidine for management of oral disease: a narrative review. J Dent 103:103497
Celakil T, Muric A, Gokcen R, Evlioglu G, Keskin H (2017) Effect of high-frequency bio-oxidative Ozone therapy for masticatory muscle pain: a double-blind randomized clinical trial. J Oral Rehabil 44(6):442–451
Chavarría-Bolaños D, Esparza-Villalpando V, Ramírez K (2022) Antibacterial and antifungal capacity of three commercially available mouthwashes with different concentrations of chlorhexidine. Odovtos-Int J Dent Sci 24(2):69–80
Claudia P, María P, Julia G (2023) Use and efficacy of mouthwashes in elderly patients: a systematic review of randomized clinical trials. Ann Anat 246:152026
de Sire A, Marotta N, Ferrillo M, Agostini F, Sconza C, Lippi L, Respizzi S, Giudice A, Invernizzi M, Ammendolia A (2022) Oxygen-ozone therapy for reducing pro-inflammatory cytokines serum levels in musculoskeletal and temporomandibular disorders: a comprehensive review. Int J Mol Sci 23(5):2528
Dodwad V, Gupta S, Kumar K, Sethi M, Masamatti S (2011) Changing paradigm in pocket therapy-Ozone vs conventional irrigation. Int J Public Heal Dent 2:7–12
Durgapal S, Shetty M (2022) Effectiveness of Ozone against common dental problems: a literature review. J Clin Diagnostic Res 1(16):14–19
Gandhi KK, Cappetta EG, Pavaskar R (2019) Effectiveness of the adjunctive use of ozone and chlorhexidine in patients with chronic periodontitis. BDJ open. 5(1):17
Granick JJ, Singh B, Winkleg G (1998) Effectiveness of a medicament containing silicon oxide, aloe, and allantoin on aphthous stomatitis. Oral Surg Oral Med Oral Pathol Oral Raiol Endod 86(5):550–556
James P, Worthington HV, Parnell C, Harding M, Lamont T, Cheung A, Whelton H, Riley P (2017) Chlorhexidine mouthrinse as an adjunctive treatment for gingival health. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD008676.pub2/full
Jeon S, Jo YH, Yoon HI, Han JS (2022) Antifungal effect, surface roughness, and cytotoxicity of three-dimensionally printed denture base with phytoncide-filled microcapsules: an in-vitro study. J Dent 120:104098
Kaio H, Parsa F, Glaciele M, Olga B, Saulo G, Cassio R (2023) Efficacy of Probiotics compared to chlorhexidine mouthwash in improving periodontal status: a systematic review and meta-analysis. Int J Dent 2023:4013004
Katti S, Chava V (2013) Effect of Ozonised water on chronic periodontitis: a clinical study. J Int Oral Health: JIOH 5(5):79
Kaur A, Bhavikatti SK, Das SS, Khanna S, Jain M, Kaur A (2019) Efficacy of ozonised water and 0.2% chlorhexidine gluconate in the management of chronic periodontitis when used as an irrigant in conjugation with phase I therapy. J Contemp Dent Pract. 20(3):318–23
Kumar A, Bhagwati S, Tyagi P, Kumar P (2014) Current interpretation and rationale of the Ozone usage in dentistry: a systemic review of literature. Eur J Gen Dent 3(3):175–180
Kumar T, Arora N, Puri G, Aravinda K, Dixit A, Jatti D (2016) Efficacy of Ozonized olive oil in the management of oral lesions and conditions: a clinical trial. Contemp Clin Dent 7(1):51–54
Lubojanski A, Dobrzynski M, Nowak N, Rewak-Soroczynska J, Sztyler K, Zakrzewski W, Dobrzynski W, Szymonowicz M, Rybak Z, Wiglusz K, Wiglusz R (2021) Application of selected nanomaterials and ozone in modern clinical dentistry. Nanomaterials 11(2):259–289
McReynolds DE, Moorthy A, Moneley JO, Jabra-Rizk MA, Sultan AS (2023) Denture stomatitis—an interdisciplinary clinical review. J Prosthodont. https://doi.org/10.1111/jopr.13687
Mostafa B, Elboraey AN, Dehis WM (2023) Impact of Ozonated water on physio-mechanical properties of PMMA denture base material. Eur Chem Bull 12(12):1177–1190
Nader N, Parham S, Alireza R (2023) Management of denture stomatitis: an overview. Acta Marisiensis Seria Med 69(1):23–29
Niveda R, Malaiappan S (2019) Comparison of the amount of bacterial microcolonies formed on using distilled water and ozonated water as an irrigating agent. Drug Invent Today. 12(8)
Orhun E, Ahmet O (2016) Influence of Ozone and paracetic acid disinfection on adhesion of resilient liners to acrylic resin. J Adv Prosthodont 8:290–295
Parkar S, Shah K, Darjee N, Sharma A (2017) Efficacy of ozonated water and chlorhexidine mouth rinse against plaque and gingivitis: a randomized clinical trial. J Clin Sci 14(2):81
Preethy S, Sabarigirinathan C (2022) Detection of the release of chlorhexidine from cured denture resins discs: subsequently deducing the ability of denture resin as a drug carrier. JDMT 11(2):127–137
Reham M, Neven S (2020) An In-vitro assessment of Physicomechanical properties of heat cured denture base resin disinfected by Ozonized water. World J Dent 11(2):146–150
Ribeiro D, Pavarina A, Dovigo L, MacHado A, Giampaolo E, Vergani C (2012) Prevalence of Candida spp. associated with bacteria species on complete dentures. Gerodontology. 29:203–208
Sansriti T, Alok A, Shashank K, Aarthi I, Suyog J (2017) Dental applications of ozone therapy: a review of literature. Saudi J Dent Res 8(1–2):105–111
Sartawi S, Abu-Hammad S, Salim NA, Al-Omoush S (2021) Denture stomatitis revisited: A summary of systematic reviews in the past decade and two case reports of papillary hyperplasia of unusual locations. Int J Dent 2021:7338143
Schwartz DM, Bonelli M, Gadina M, O’Shea JJ (2016) Type I/II cytokines, JAKs, and new strategies for treating autoimmune diseases. Nat Rev Rheumatol 12(1):25–36
Sen S, Sen S (2020) Ozone therapy a new vista in dentistry: integrated review. Med Gas Res 10(4):189
Sharabasy R, Ahmed ME, Mohammed E (2022) Comparative study of candida albicans adherence to conventional acrylic denture base materials and injection molding acrylic materials and poly ether ether ketone. Egypt Dental J 68(4):3579–85
Singh P, Sheoran K, Sikka N, Dhamija N (2017) Review of ozone and its role in prosthodontics. J Dent Sci 4(5):226–232
Suh Y, Patel S, Kaitlyn R, Gandhi J, Joshi G, Smith NL, Khan SA (2019) Clinical utility of ozone therapy in dental and oral medicine. Med Gas Res 9(3):163
Tiwari S, Avinash A, Katiyar S, Iyer A, Jain S (2017) Dental applications of ozone therapy: a review of literature. Saudi J Dent 8(1–2):105–111
Tütüncüoğlu S, Cetinkaya BO, Pamuk F, Avci B, Keles GC, Kurt-Bayrakdar S, Lütfioğlu M (2022) Clinical and biochemical evaluation of oral irrigation in patients with peri-implant mucositis: a randomized clinical trial. Clin Oral Invest 1:1–3
Acknowledgements
None.
Funding
Self-funding.
Author information
Authors and Affiliations
Contributions
BM was responsible for reviewing, article administration and submission of the manuscript to the journal. ANE helped in conceptualization, visualization, clinical investigations, validation and data curation. HMEM aided in data curation, formal analysis, laboratory and clinical investigations, interpretations and statistical analysis. WMD was responsible for conceptualization, clinical investigations, review, methodology, supervision, and editing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The current contemplate has been applied to the Code of Ethics of the World Medical Association, following the ethics stated in the Declaration of Helsinki in 1975. This research has been permitted by the “Medical Research Ethical Committee of the National Research Centre, Cairo, Egypt” with agreement number 4447082022. All patients were up-to-date with the existing study’s practical phases and contracted the printed consent. The research was registered on ClinicalTrials.gov with the identifier: NCT06021847.
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mostafa, B., Elboraey, A.N., El-Masry, H.M. et al. Evaluation of the effect of ozonated water in treatment of denture stomatitis associated with removable prosthetics. Bull Natl Res Cent 48, 1 (2024). https://doi.org/10.1186/s42269-023-01151-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42269-023-01151-5