
Abstract
Background
Low-density lipoprotein cholesterol (LDL-c) is the major determinant of cardiovascular disease burden. This study critically reviewed the published literature and performed a meta-analysis to compare and to determine which other equations provide the best means of estimating LDL-c in clinical settings.
Method
English articles indexed in PubMed, Science Open, Biomed central and SpringerLink databases were searched with searches being conducted in or after 2001 up to date. According to the predefined inclusion and exclusion criteria, 22 articles out of the 17,970 retrieved were eligible for quantitative analysis. Data were pooled and meta-analysis performed using a random-effects model, and the results are described as event rates (pooled correlation coefficient).
Main body of the abstract
All the twelve equations showed positive correlation with the respective direct low-density lipoprotein-cholesterol measurements. The pooled estimates showed a stronger positive correlation between Martin’s low-density lipoprotein-cholesterol equation and the direct low-density lipoprotein-cholesterol measurement [0.96 (95% CI 0.94–0.98)] as compared to Friedewald’s equation and the direct method [0.94 (95% CI 0.92–0.96)]. At triglycerides levels > 400 mg/dl, Martin’s low-density lipoprotein-cholesterol equation established better performance (77.78%) than the Friedewald’s equation. In studies where triglycerides levels > 400 mg/dl were excluded Martin’s low-density lipoprotein-cholesterol equation still established better performance (83.33%) than the Friedewald’s equation.
Short conclusion
Our data suggest that Martin’s equation showed a better performance than Friedewald equation. Martin’s equation can serve as a more accurate method to estimate low-density lipoprotein cholesterol as compared to Friedewald’s equation especially in situations of the same racial background.
Similar content being viewed by others


Background
Cardiovascular diseases (CVD) in recent times have been reported by the world health organization (WHO) as the leading cause of death worldwide, with high serum low-density lipoprotein cholesterol (LDL-c) a major risk factor of CVD worldwide (Ephraim et al. 2018). It is estimated by WHO that about 17.9 million lives are lost every year due to CVD. Many studies have consistently reported a strong positive correlation between CDV and high serum LDL-c, hence the need for an accurate estimation of LDL-c in clinical practice to monitor and evaluate patients risk of developing CVD (Martin et al. 2013; Ephraim et al. 2018).
Several novel formulas for calculating serum LDL-c have been reported in many research studies all over the world as an ideal formula better with regard to accuracy (Puavilai and Laoragpongse 2004; Puavilai et al. 2009; Martin et al. 2013; Mehta et al. 2018; Alpdemir and Alpdemir 2021) yet there seems to be no consensus on the best method of estimating serum LDL-c with regard to accuracy of results and convenience. The direct estimation method of measuring serum LDL-c is widely accepted as the most accurate method of estimating LDL-c but this method cannot be routinely employed in many clinical settings due to cost and the fact that it is quite complex to use (Puavilai et al. 2009). So due to cost and complexity of direct estimation of serum LDL-c, the indirect method of estimating serum LDL-c using standardized Friedewald’s equation (sFE) is routinely employed in many clinical settings for assessing the coronary risk of patients (Ballantyne et al. 2000). Many other studies compared several other indirect serum LDL-c measurement formulas which were generally referred to as modified Friedewald’s equation (mFE) in many of those research studies and reports from those research studies indicate that most of proposed modified formulas are more accurate in estimating serum LDL-c in instances of hypertriglyceridemia (Puavilai and Laoragpongse 2004; Alpdemir and Alpdemir 2021).
Elevated triglycerides often above 300 mg/dl in serum results in a significant accuracy decline in the indirect estimation of serum LDL-c using standardized Friedewald’s equation according to many research studies, and this is the practical limitation of the standardized Friedewald’s equation (Puavilai and Laoragpongse 2004; Ephraim et al. 2018; Mehta et al. 2018). This leads to a misclassification of patients with high coronary risk index as patients with low or normal coronary risk index (Mehta et al. 2018). Another significant limitation of sFE is that serum LDL-c of a non-fasting sample cannot be accurately measured (Puavilai et al. 2009).
Regardless of the reported limitations of sFE, a research study conducted by Puavilai and Laoragpongse (2004) reported that calculating LDL-c using the sFE produced results that strongly correlates with direct measurement of LDL-c which is used as a reference (gold standard) in many of the research works which seeks to assess the validity or accuracy of sFE results compared to other modified LDL-c calculation method. However, the researchers of this study noticed that the LDL-c level from the direct measurement (reference standard) was higher than calculating one using sFE if the serum triglyceride is higher than 300 mg/dL (Puavilai and Laoragpongse 2004).
Hence, due to the lack of consensus on the best means of calculating an important clinical parameter as serum LDL-c there is a need for a broader or a more holistic approach in determining the best means of estimating LDL-c in serum in terms of accuracy and a systematic review which seeks to deliver a meticulous analysis and summary of all relevant research works about this subject can best achieve that.
Methods
Literature research
This review study systematically identified and critically evaluated and analyzed existing primary literature to make recommendations on the best equation to estimate LDL-c in resource limited areas. In this literature review, the Medline (PubMed), ScienceOpen, Biomedcentral and SpringerLink electronic databases were searched. The search was based on the following keyword terms or their derivatives or synonyms: LDL cholesterol and equation. The search used ‘free terms’ and ‘index terms’ funneled using the Boolean operators (OR, AND), into the search string; (LDL cholesterol OR low-density Lipoprotein cholesterol) AND (equation OR formula) as described in Table 1.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting and reporting systematic review were followed.
Criteria for considering studies for this review
Studies whose report did not present enough information to allow full assessment of eligibility or studies reported only in a non‐English language were excluded. Published studies which are not original or primary research articles such patents, reviews, reports, newsletters, book, book chapters and conference papers were excluded from this study. Primary studies that employed diagnostic method comparison or method validation of calculated LDL-c were considered eligible for this study. Studies that were published earlier than 2001 were considered ineligible for review (Table 2).
Participants
Studies recruiting or involving populations of healthy and diseased subjects who meet the condition required for testing for serum lipids including being in a fasting state were eligible for inclusion (Table 2).
Index test and reference standards
Studies were required to estimate LDL-c using methods of direct measurement/assay of LDL as reference standard with or without an added test method as reference standard. Studies evaluating, validating or comparing any equation for LDL-c estimation in addition to the Friedewald’s LDL-c equation were considered eligible for inclusion. Studies that evaluated only one LDL-c equation were considered ineligible (Table 2).
Data collection
Search results from the various databases were subjected to automated screening for eligibility using electronic filters available in the electronic databases based on pre-determined eligibility criteria as described in Table 2. Using pro-forma, eligibility of potentially relevant articles was assessed based on full text publications excluding non‐English language reports. Due to the number of studies identified, hand search and search of bibliography of included studies were not sourced. The outcomes of the selection process are described in Fig. 1.

PRISMA flowchart on selection of studies in this review
Appraisal of included studies and risk of bias
Two authors independently assessed the risk of bias of included studies, and disagreements were resolved through discussion. The Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) was employed to evaluate the methodological quality. Four domains of entries were participant’s selection, index test, reference standard and flow and timing. Definitions and judgment criteria for each domain are available in Cochrane Handbook.
Data extraction and management
Data relating to the correlation coefficient ‘r’ (Pearson correlation coefficient, Spearman rank correlation and intraclass correlation coefficient) estimation of each comparison of index test (calculated LDL-c equation) with reference test (direct LDL-c assays) were extracted and used for the meta-analysis. In three studies where coefficient of determination (r2) was reported, correlations coefficient was recalculated using the formulae, and direction of slope (√r2) was reported. In studies where estimates of coefficients were reported in strata or subgroups, the pooled or overall correlation coefficient was estimated by using the Schmidt–Hunter’s method for estimating pooled correlation coefficients. Also, characteristics of each study (such as the year of study publication, method of direct LDL-c used, type of study, location and sample size) were extracted from each study (Table 3). The author’s surname and year of publication of the study were used as identities for each study (Table 3).
Statistical analysis and data synthesis
For each test type, we plotted estimates of the observed correlation coefficients in forest plots. These plots illustrate the variation in test performance between studies. The Hedges–Olkin method for pooled correlation coefficient was used to calculate overall correlation coefficients. The summary estimates were plotted using forest plots. The random effect model was used as significantly large heterogeneity was observed among the studies. The StatsDirect statistical tool was used for the meta-analysis.
Investigations of heterogeneity
We inspected forest plots to visually assess heterogeneity between study-specific estimates of correlation. A heterogeneity test (I2 heterogeneity test) was also performed to ascertain the variations in the outcomes of interest among the various studies.
Results
Pooled correlation coefficients
See Figs. 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13 and 14.

The pooled correlation coefficient of Friedewald’s LDL-c equation compared to direct measurement in determining levels of LDL-c from all included studies. There was a positive correlation between Friedewald’s LDL-c equation and direct measurement in determining levels of LDL-c [0.94 (95% CI 0.92–0.96)]

The pooled correlation coefficient of Friedewald’s and Martin’s LDL-c equation compared to direct measurement in determining levels of LDL-c from matching studies. The pooled correlation between Martin’s LDL-c equation and the direct measurement in determining levels of LDL-c as well as the correlation between the Friedewald’s LDL-c equation and the direct measurement in determining levels of LDL-c. This correlation pooled 12 studies in the analysis. There was a positive correlation between Martin’s LDL-c equation and the direct measurement in determining levels of LDL-c [0.96 (95% CI 0.94–0.98)]. Similarly, Friedewald’s LDL-c equation positively correlated with the direct measurement in determining levels of LDL-c [0.94 (95% CI 0.92–0.96)]. However, there was a stronger positive correlation between Martin’s LDL-c equation and the direct measurement in determining levels of LDL-c compared to Friedewald’s equation and the direct method

The correlation coefficient of Friedewald’s and the Anandaraja’s LDL-c equations with direct measurement in determining levels of LDL-c from 9 matching studies. The Anandaraja’s LDL-c equation and the direct method of determining LDL-c gave a positive correlation [0.90 (0.85–0.93)] as well as positive correlation between the Friedewald’s equation and the direct method [0.94 (95%0.89–0.96)]. However, there was a stronger positive correlation between the Friedewald’s equation and the direct method compared to the Anandaraja’s equation

The correlation coefficients of Friedewald’s and the Chen’s LDL-c equations with direct measurement in determining levels of LDL-c from 8 pooled matching studies. The two equations established a positive correlation between the direct method of determining LDL-c [0.95 (95% CI 0.90–0.97)]. There was no statistical difference between the correlation coefficients of Chen’s equation and the direct measurement as well as Friedewald’s equation and the direct method

The correlation coefficients of the Friedewald’s and the de Cordova’s LDL-c equations with the direct measurement in determining levels of LDL-c pooled from 6 matching studies. The de Cordova’s LDL-c equations and the Friedewald’s equation both demonstrated a positive correlation with the direct method of measuring LDL-c [0.87 (95% CI 0.76–0.93) and 0.94 (95% CI 0.88–0.97), respectively]. However, the Friedewald’s equation established a stronger positive correlation with the direct method of determining LDL-c compared with the de Cordova’s LDL-c equation

The correlation coefficients of Friedewald’s and the Puavilai’s LDL-c equations with direct measurement in determining levels of LDL-c from 6 matching studies. Both equations demonstrated a positive correlation with the direct method of measuring LDL-c. However, the Puavilai’s equation established a stronger correlation with the direct method [0.95 (95% CI 0.91–0.97)] than Friedewald’s LDL-c equation [0.93 (95% CI 0.89–0.95)]

The correlation coefficients of Friedewald’s and Ahmadi’s LDL-c equations with direct measurement in determining levels of LDL-c from 5 matching studies. Though both equations established a positive correlation with the direct method of measuring LDL-c, the Friedewald’s LDL-c equation presented with a stronger positive correlation with the direct method [0.95 (95% CI 0.90–0.98)] than the Ahmadi’s LDL-c equation [0.65 (95% CI 0.46–0.78)]

The correlation coefficients of Friedewald’s and the Hattori LDL-c equations with direct measurement in determining levels of LDL-c from 4 matching studies. Both the Friedewald’s and the Hattori LDL-c equations demonstrated a positive correlation with the direct method of measuring LDL-c. There was no statistical difference in their correlation coefficients

The correlation coefficients of Friedewald’s and the Vujovic’s LDL-c equations with direct measurement in determining levels of LDL-c pooled from 4 from matching studies. Both equations established a positive correlation with the direct method. Nevertheless, Vujovic’s LDL-c equation demonstrated a stronger positive correlation with the direct method [0.95 (95% CI 0.93–0.96)] than Friedewald’s equation [0.88 (95% CI 0.84–0.93)]

The correlation coefficients Friedewald’s and the DeLong’s LDL-c equations with direct measurement in determining levels of LDL-c pooled from 3 matching studies. Both equations had a positive correlation with the direct method, but DeLong’s LDL-c equation gave a strong correlation with the direct method [0.96 (95% CI 0.90–0.99)] compared with Friedewald’s equation [0.95 (95% CI 0.82–0.99)]

The correlation coefficients of Friedewald’s and the Rao’s LDL-c equations with direct measurement in determining levels of LDL-c from 3 matching studies. Both equations established a positive correlation with the direct method of measuring LDL-c; however, Friedewald’s equation demonstrated a stronger positive correlation with the direct method [0.95 (95% CI 0.82–0.99)] than the Rao’s LDL-c equation [0.93 (95% CI 0.60–0.99)]

The correlation coefficients of Friedewald’s and the Sampson’s LDL-c equations with direct measurement in determining levels of LDL-c from 3 matching studies. Though both equations had a positive correlation with the direct method of measuring LDL-c, the Sampson’s LDL-c equation showed a stronger positive correlation with the direct method [0.95 (95% CI 0.89–0.98)] as compared with the Friedewald’s equation [0.92 (95% CI 0.92–0.92)]

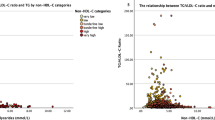
The proportions of LDL-c equations performing better than Friedewald’s equation in studies where TG > 400 mg/dl were included or excluded. A Triglycerides levels > 400 mg/dl included. About 6 matching studies that included serum triglycerides levels > 400 mg/dl, 100% of these studies established better performance of the Choi, DeLong and Molavi LDL-c equations than the Friedewald’s equation (Fig. 14A). B: Triglycerides levels > 400 mg/dl excluded. However, in about 24 studies, 100% of the studies demonstrated better performance of the Puavilai LDL-c equation compared with Friedewald’s equation. In about 13 studies that excluded serum triglycerides levels > 400 mg/dl, 100% recorded better performance of the Ephraim’s LDL-c equation than the Friedewald’s equation. This was followed by the Martin’s LDL-c equation with 83% out of the 75 studies assessed (Fig. 14B)
Discussion
A causal relationship between LDL-c levels and CV outcomes has been demonstrated in countless randomized controlled clinical trials (Steinberg 2005; Baigent et al. 2010; Levinson 2020; Mach et al. 2020; Piani et al. 2021). Direct measurements of LDL-c are still costly, time-consuming, not fully standardized and not universally available (Nauck et al. 2002; Miller et al. 2010; Langlois et al. 2018; Piani et al. 2021). Generally, LDL-c is alternatively estimated using the empirical Friedewald equation in most clinical environments (Bairaktari et al. 2005; Brown 2020). Nevertheless, many groups have consistently evaluated the accuracy of the Friedewald equation in different ethnicities or various disease entities and proposed alternative formulas for more precise LDL-c estimation until today (Table 4). To date, none of the proposed alternative methods have replaced the Friedewald equation in routine clinical practice and the lack of consensus on the best means of calculating LDL-c necessitated this study. Thus, to determine the best means of estimating LDL-c, this study evaluates the accuracy of the different equations known to calculate LDL-c levels.
Indeed, our data showed a positive correlation between Friedewald’s LDL-c equation and direct measurement of LDL-c (D-LDL-c) from all the included studies [0.94 (95% CI 0.92–0.96)] (Fig. 2). Overall, all the twelve formulas showed a good positive correlation with the respective D-LDL-c (Figs. 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12 and 13) and Martin’s equation (ME) had the highest correlation with D-LDL-c level measurement compared to all other formulas (Fig. 3). This present result can be validated from a study conducted by Rim et al. (2016) which reported that ME provided best agreement in a large Asian cohort as compared to other equations. Similarly, another study conducted on Korean population also showed that ME provided better results compared to other equations (Kang et al. 2017). However, our finding is not in agreement with the work of Cordova et al. (2020) who revealed that Martin’s equation is not accurate for estimating LDL-c in Southern Brazilians unless TG is between 300 and 400 mg/dl as well as Khan et al. (2017) whose work among the Pakistani population showed that the Teerakanchana equation (TE) provided higher correlation with D-LDL-c level followed closely by Martin equation. Also, our present results contradict studies conducted among the Indian population. They validated from their study that TE provided stronger correlation with the D-LDL-c level, followed by Vujovic equation (Dar et al. 2022), while in another study conducted among the Indian population Vujovic equation was preferred over others for calculating LDL-c level (Wadhwa and Krishnaswamy 2016). The differences in the performance (i.e., correlation with D-LDL-c level) of the equations in measuring D-LDL-c levels could be associated with the racial differences.
Again, a study conducted by Piani et al. (2021) on a large, random and blinded Italian population showed that Sampson equation provided higher correlation to measured D-LDL-c level. This outcome is not in keeping with our present data which revealed that ME is highly correlated with measured LDL-c levels. Here, we strongly believe that the difference in the outcomes could be due to the techniques employed in the estimation of the lipid levels. While Piani et al. (2021) estimated D-LDL-c level by employing the Sampson equation after all lipid samples were analyzed using direct homogeneous assay, Martin’s equation estimated D-LDL-c levels after cholesterol concentrations (LDL-c, VLDL-c and HDL-c) and triglycerides were directly measured by density-gradient ultracentrifugation and the ARCHITECT C-8000 system, respectively. These methodologies have different underlying principles and could possibly influence the estimated D-LDL-c level.
Moreover, our study found the lowest correlation between Ahmadi’s equation (AE) and the measurement of D-LDL-c level [0.65 (95% CI 0.46–0.78)] (Fig. 8). Interestingly, our findings are consistent with the results of Karkhaneh et al. (2019) and Molavi et al. (2020), where AE provided lowest correlation for Iranian population likewise in the Pakistani population (Khan et al. 2022). The reason why Ahmadi equation does not perform well could be due to the fact that this equation was derived only from the patients with high cholesterol (> 250 mg/dL, > 6.45 mmol/L) (Rim et al. 2016).
In addition, one interesting finding in our study is that studies that used LDL-c equations (Choi, DeLong, Puavilai and Molavi) established better performance (100%) than the Friedewald equation (FE) at serum triglycerides (TG) levels > 400 mg/dl (Fig. 14A). This is partly in conformity with the report of Wadhwa and Krishnaswamy (2016) who compared LDL cholesterol estimated using various formulae with directly measured LDL cholesterol in Indian population. While our study validates that Choi, DeLong, Puavilai and Molavi LDL-c equations gave better performance (100%) than the Friedewald equation (FE) at TG levels > 400 mg/dl, they reported that for TG range > 400 mg/dL, Vujovic equation correlated best with direct measurement of LDL-c levels. Nonetheless, this is contradictory to the study conducted by Sha et al., in Bangladeshi population who concluded that FE can be used up to serum TG concentration of 700 mg/dL (Sha et al. 2015). Here, the variance in the performance of the equations in estimating D-LDL-c levels at serum triglycerides (TG) levels > 400 mg/dl may be associated with sample size, fasting and non-fasting state of study participants, ethnicity and procedures employed in estimating lipid levels.
Furthermore, Cordova and Cordova suggested a new formula that performed better than Friedewald formula in Brazilian population over a wide TG range (de Cordova and de Cordova 2013). The results of this present study show FE performed better than Cordova equation (CE). Hence, we are in support of the findings of Wadhwa and Krishnaswamy (2016) that Cordova formula does not provide any significant advantage over Friedewald formula in Indian population. This study supports the study done by Gupta and Singh (2012), which concluded that Anandaraja formula does not provide any advantage over Friedewald formula for LDL-c estimation in Indian population (Gupta and Singh 2012). This is contradictory to the study done by Anandaraja et al., which found their formula more accurate than Friedewald formula for TG < 350 mg/dL (Anandaraja et al. 2005). Also, the modified Friedewald equation developed by Puavilai also correlated well with direct measurement and performed better than Friedewald formula at TG range > 200 mg/dL in Thai population (Puavilai and Laoragpongse 2004). It could be observed clearly that changes in TG range have the ability to affect the final value of the D-LDL-c irrespective of the equations that would be used.
Again, Ahmadi equation (AE) has been validated in Iranian subjects at TG < 300 mg/dL (Ahmadi et al. 2008). In our study, it performed better than FE at TG > 400 mg/dL. However, when TG > 400 mg/dL were excluded, it performed poorly than FE (Fig. 14A and B). Hence, it might not be suitable to be used in other populations.
Besides, Hattori equation (HE) developed by Hattori et al. had shown to perform better than FE in Japanese population which does not provide any advantage over FE in Indian population (Hattori et al. 1998). Our study outcome indicates that HE performed better than FE at TG > 400 mg/dL. However, without TG > 400 mg/dl inclusion, it performed poorly than FE (Fig. 14A and B). Again, this supports the claim that some of the D-LDL-c might not be suitable to be used in other populations because of racial differences.
Strength and limitations
The present study has one major strength and some limitations. We have analyzed all the principal LDL-c estimation formulas used in several studies. Hence, we strongly believe that our study is a representative of various racial origins and gives a generalizability to other populations. However, one major limitation in this study is that some studies were not included in the meta-correlational analysis due to insufficient information. In addition, several studies that we used in our study measured direct LDL-c by different assay methods such as Roche analyzer and Sekisui reagent instead of the recommended gold standard method of beta quantification. This could lead to incorrect comparisons of formulas with direct LDL-c data obtained from different methods.
Even though Martin’s equation has proven to be a better assessment tool than the other equations, it is limited by several factors. First, the Martin’s equation requires validation in an independent population and using other laboratory techniques. Second, factors such as race/ethnicity, obesity, diabetes and insulin resistance, which may affect variance in the adjustable factor (TG/VLDL-c ratio), were not available for analysis during the formulation of the Martin’s equation. Finally, the study that formed the Martin’s equation examines 1-time estimation of lipid levels. This is a major limitation because the study did not address the problem of intraindividual variation in lipid levels which has a greater potential to influence the adjustable factor.
Conclusion
Our data suggest that all the twelve formulas showed positive correlation with the respective D-LDL-c measurements. Martin’s equation provided the highest correlation with D-LDL-c measurement than the most used Friedewald equation. Again, at high TG ranges (i.e., TG > 400 mg/dl), Martin’s equation gave a better performance than Friedewald equation. Therefore, Martin’s equation can serve as a more accurate method to estimate LDL-c as compared to Friedewald equation especially is situations of the same ethnicity or race.
Availability of data and materials
All data supporting the case are included in the manuscript.
Abbreviations
- AE:
-
Ahmadi’s equation
- CI:
-
Confidence interval
- CVD:
-
Cardiovascular diseases
- CE:
-
Cordova equation
- D-LDC:
-
Direct low-density lipoprotein cholesterol
- FE:
-
Friedewald’s equation
- HE:
-
Hattori’s equation
- ME:
-
Martin’s equation
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QUADAS-2:
-
Quality Assessment of Diagnostic Accuracy Studies-2
- TE:
-
Teerakanchana’s equation
- TG:
-
Triglyceride
- WHO:
-
World Health Organization
References
Ahmadi SA, Boroumand MA, Gouhari MK, Tajik P, Dibaj SM (2008) The impact of low serum triglyceride on LDL-cholesterol estimation. Arch Iran Med 11(3):318–321
Alpdemir M, Alpdemir MF (2021) Comparison of Martin and Friedewald equation for estimated LDL-C in adults. Turk Kardiyoloji Dernegi Arsivi 49(8):619
Anandaraja S, Narang R, Godeswar R, Laksmy R, Talwar KK (2005) Low-density lipoprotein cholesterol estimation by a new formula in Indian population. Int J Cardiol 102(1):117–120
Atabi F, Mohammadi R (2020) Clinical validation of eleven formulas for calculating LDL-C in Iran. Iran J Pathol 15(4):261
Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, Collins R (2010) Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet 376(9753):1670–1681
Bairaktari ET, Seferiadis KI, Elisaf MS (2005) Evaluation of methods for the measurement of low-density lipoprotein cholesterol. J Cardiovasc Pharmacol Ther 10(1):45–54
Ballantyne CM, Grundy SM, Oberman ALBERT, Kreisberg RA, Havel RJ, Frost PH, Haffner SM (2000) Hyperlipidemia: diagnostic and therapeutic perspectives. J Clin Endocrinol Metab 85(6):2089–2112
Brown WV (2020) Methods of calculating low-density lipoprotein cholesterol level. JAMA Cardiol 5(5):502–503
Chaen H, Kinchiku S, Miyata M, Kajiya S, Uenomachi H, Yuasa T, Ohishi M (2016) Validity of a novel method for estimation of low-density lipoprotein cholesterol levels in diabetic patients. J Atheroscler Thromb 23(12):1355–1364
Choi R, Park MJ, Oh Y, Kim SH, Lee SG, Lee EH (2021) Validation of multiple equations for estimating low-density lipoprotein cholesterol levels in Korean adults. Lipids Health Dis 20(1):1–11
Chung S (2018) Usefulness of the Martin Method for estimation of low-density lipoprotein cholesterol in coronary atherosclerosis. Med Princ Pract 27(1):8–14
Cordova CMM, Portal AS, Cordova MM (2020) Martin’s, Friedewald’s and Cordova’s formulas compared to LDL-C directly measured in Southern Brazil. J Brasil de Patologia e Med Lab 56:1–6
Dansethakul P, Thapanathamchai L, Saichanma S, Worachartcheewan A, Pidetcha P (2015) Determining a new formula for calculating low-density lipoprotein cholesterol: data mining approach. EXCLI J 14:478
Dar GM, Dash M, Mahajan B (2022) Teerakanchana’s equation transcends over 12 other LDL-C quantification formulae in the North Indian population. Clin Chim Acta 531:168–176
de Cordova CMM, de Cordova MM (2013) A new accurate, simple formula for LDL-cholesterol estimation based on directly measured blood lipids from a large cohort. Annals Clin Biochem 50(1):13–19
Ephraim RK, Acheampong E, Swaray SM, Odame AE, Agbodzakey H, Adoba P, Amoah B (2018) Developing a modified low-density lipoprotein (M-LDL-C) Friedewald’s equation as a substitute for direct LDL-C measure in a Ghanaian population: a comparative study. J Lipids 2018:1–9
Ferrinho C, Alves AC, Bourbon M, Duarte S (2021) Applicability of Martin-Hopkins formula and comparison with Friedewald formula for estimated low-density lipoprotein cholesterol in e_COR study population. Rev Port De Cardiol (engl Ed) 40(10):715–724
Gasko R (2006) Low-density lipoprotein cholesterol estimation by the Anandaraja’s formula–confirmation. Lipids Health Dis 5(1):1–2
Ghasemi A, Asgari S, Hadaegh F, Kheirandish M, Azimzadeh I, Azizi F, Tohidi M (2018) New modified Friedewald formulae for estimating low-density lipoprotein cholesterol according to triglyceride levels: extraction and validation. Endocrine 62(2):404–411
Gupta S, Verma M, Singh K (2012) Does LDL-C estimation using Anandaraja’s formula give a better agreement with direct LDL-C estimation than the Friedewald’s formula? Indian J Clin Biochem 27(2):127–133
Hattori Y, Suzuki M, Tsushima M, Yoshida M, Tokunaga Y, Wang Y, Harano Y (1998) Development of approximate formula for LDL-chol, LDL-apo B and LDL-chol/LDL-apo B as indices of hyperapobetalipoproteinemia and small dense LDL. Atherosclerosis 138(2):289–299
Kang M, Kim J, Lee SY, Kim K, Yoon J, Ki H (2017) Martin’s equation as the most suitable method for estimation of low-density lipoprotein cholesterol levels in Korean adults. Korean J Family Med 38(5):263
Karkhaneh A, Bagherieh M, Sadeghi S, Kheirollahi A (2019) Evaluation of eight formulas for LDL-C estimation in Iranian subjects with different metabolic health statuses. Lipids Health Dis 18(1):1–11
Khan M, Ain QT, Nawaz A, Khan MI, Sadiq F (2022) Indirect calculation of LDL using thirteen equations in Pakistani population. Clinica Chimica Acta 536:77–85
Langlois MR, Chapman MJ, Cobbaert C, Mora S, Remaley AT, Ros E, European Atherosclerosis Society (EAS) and the European Federation of Clinical Chemistry and Laboratory Medicine (EFLM) Joint Consensus Initiative (2018) Quantifying atherogenic lipoproteins: current and future challenges in the era of personalized medicine and very low concentrations of LDL cholesterol. A consensus statement from EAS and EFLM. Clin Chem 64(7):1006–1033
Levinson SS (2020) Non–high-density lipoprotein cholesterol and guidelines for cholesterol lowering in recent history. Lab Med 51(1):14–23
Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, Wiklund O (2020) 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur Heart J 41(1):111–188
Martin SS, Blaha MJ, Elshazly MB, Toth PP, Kwiterovich PO, Blumenthal RS, Jones SR (2013) Comparison of a novel method vs the Friedewald equation for estimating low-density lipoprotein cholesterol levels from the standard lipid profile. JAMA 310(19):2061–2068
Martínez-Morillo E, García-García M, Concha MAL, Varas LR (2021) Evaluation of a new equation for estimating low-density lipoprotein cholesterol through the comparison with various recommended methods. Biochem Med 31(1):54–65
Mehta R, Reyes-Rodríguez E, Bello-Chavolla OY, Guerrero-Díaz AC, Vargas-Vázquez A, Cruz-Bautista I, Aguilar-Salinas CA (2018) Performance of LDL-C calculated with Martin’s formula compared to the Friedewald equation in familial combined hyperlipidemia. Atherosclerosis 277:204–210
Miller WG, Myers GL, Sakurabayashi I, Bachmann LM, Caudill SP, Dziekonski A, Remaley AT (2010) Seven direct methods for measuring HDL and LDL cholesterol compared with ultracentrifugation reference measurement procedures. Clin Chem 56(6):977–986
Molavi F, Namazi N, Asadi M, Sanjari M, Motlagh ME, Shafiee G, Kelishadi R (2020) Comparison common equations for LDL-C calculation with direct assay and developing a novel formula in Iranian children and adolescents: the CASPIAN V study. Lipids Health Dis 19(1):1–8
Nauck M, Warnick GR, Rifai N (2002) Methods for measurement of LDL-cholesterol: a critical assessment of direct measurement by homogeneous assays versus calculation. Clin Chem 48(2):236–254
Piani F, Cicero AF, Ventura F, Dormi A, Fogacci F, Patrono D, Rossolini A (2021) Evaluation of twelve formulas for LDL-C estimation in a large, blinded, random Italian population. Int J Cardiol 330:221–227
Pradhan S, Gautam K, Pyakurel D (2020) Comparison of calculated LDL-cholesterol using the Friedewald formula and de Cordova formula with a directly measured LDL-cholesterol in Nepalese population. Pract Lab Med 20:e00165
Puavilai W, Laoragpongse D (2004) Is calculated LDL-C by using the new modified Friedewald equation better than the standard Friedewald equation? J Med Assoc Thail 87(6):589–593
Puavilai W, Laorugpongse D, Deerochanawong C, Muthapongthavorn N, Srilert P (2009) The accuracy in using modified Friedewald equation to calculate LDL from non-fast triglyceride: a pilot study. Med J Med Assoc Thail 92(2):182
Razi F, Forouzanfar K, Bandarian F, Nasli-Esfahani E (2017) LDL-cholesterol measurement in diabetic type 2 patients: a comparison between direct assay and popular equations. J Diabetes Metab Disord 16(1):1–5
Rim JH, Lee YH, Lee MH, Kim HY, Choi J, Lee BW, Cha BS (2016) Comparison and validation of 10 equations including a novel method for estimation of LDL-cholesterol in a 168,212 Asian population. Medicine 95(14):1–8
Sampson M, Ling C, Sun Q, Harb R, Ashmaig M, Warnick R, Remaley AT (2020) A new equation for calculation of low-density lipoprotein cholesterol in patients with normolipidemia and/or hypertriglyceridemia. JAMA Cardiol 5(5):540–548
Sha MFR, Siddique AH, Saiedullah M, Khan MAH (2015) Evaluation of recently developed regression equation with direct measurement of low-density Lipoprotein Cholesterol in a Bangladeshi population. J Enam Med College 5(2):75–79
Singh G, Hussain Y, Xu Z, Sholle E, Michalak K, Dolan K, Al’Aref S J, (2020) Comparing a novel machine learning method to the Friedewald formula and Martin-Hopkins equation for low-density lipoprotein estimation. PLoS ONE 15(9):e0239934
Song Y, Lee HS, Baik SJ, Jeon S, Han D, Choi SY, Chang HJ (2021) Comparison of the effectiveness of Martin’s equation, Friedewald’s equation, and a Novel equation in low-density lipoprotein cholesterol estimation. Sci Rep 11(1):1–11
Sonoda T, Takumi T, Miyata M, Kanda D, Kosedo I, Yoshino S, Ohishi M (2018) Validity of a novel method for estimating low-density lipoprotein cholesterol levels in cardiovascular disease patients treated with statins. J Atheroscler Thromb 25(7):643–652
Sonsok S, Sarakarn P, Sanchaisuriya P (2020) Comparison of three equations for estimating low-density lipoprotein-cholesterol in the rural northeastern region of Thailand. J Clin Lab Anal 34(10):e23429
Steinberg D (2005) An interpretive history of the cholesterol controversy, part III: mechanistically defining the role of hyperlipidemia. J Lipid Res 46(10):2037–2051
Wadhwa N, Krishnaswamy R (2016) Comparison of LDL-cholesterol estimate using various formulae with directly measured LDL-cholesterol in Indian population. J Clin Diagn Res JCDR 10(12):BC11
Acknowledgements
Not applicable.
Funding
The work was fully funded by the authors.
Author information
Authors and Affiliations
Contributions
RKDE and AAY conceived the idea; AAY, EA and SAA did the search, collected the data and did the analysis; and RKDE, KOD, EA and SAA prepared the first draft of the manuscript. All the authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ephraim, R.K.D., Ativi, E., Ashie, S.A. et al. Assessment of estimated low-density lipoprotein-cholesterol (LDL-c) equations: a systematic review and meta-analysis. Bull Natl Res Cent 47, 71 (2023). https://doi.org/10.1186/s42269-023-01046-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42269-023-01046-5