
Abstract
Background
Parkinson's disease (PD) is the second most prevalent neurodegenerative ailment affecting aged people. Several motor and non-motor symptoms appearing with this disease are linked to reduction in dopamine levels. Parkinson’s disease manifested by a wide range of symptoms, including gait instability, voice impairments, bradykinesia, hypomimia, tremors, and cognitive dysfunctions, where the concern is its steady global progression. Therefore, by evaluating the stage-specific retention and transition thresholds, the suggested work attempts to detect the progression of PD. Similarly, the assessment of the annual rate of deterioration of symptoms aids in assessing the influence of medications on four stages and six prime symptoms.
Results
During the 9-year period following clinical diagnosis, a symptomatic deterioration of 34.995% is observed in untreated patients compared to treated patients. Furthermore, the experimental analysis illustrates that medicines assist in regulating only bradykinesia, tremors, hypomimia, and speech impairment, which lasts for 4.8 years on average. A saturation period is also identified during the moderate phase, where the computed average depreciation in the Unified Parkinson’s Disease Rating Scale (UPDRS) is the least. Similarly, from stages 1 to 4, medicines might improve stage retention by 4.44, 3.5, 2.72, and 1.6 years, respectively. It demonstrates that, despite transient advantages and adverse effects, medications also have an optimistic impact on PD patients.
Conclusions
Here, we show that medication can extend the lifespan of PD patients up to 12 years cumulatively. Furthermore, the proposed work suggests that stagewise alternative remedies for improving quality of life, boosting the benefits of medicines, and eliminating their side effects. These include counselling, diet changes, yoga asanas, herbal medicines, bio-cleansing and other therapies. The current work does not consider the temporary transition among stages; nonetheless, further investigation regarding PD could open avenues for more worthy treatments with fewer side effects.
Similar content being viewed by others


Background
Impaired lifestyle, environmental toxins, deficiency of certain nutrients, abnormal secretion of hormones, and genetic alterations are enough to produce any health disorder in humans. One such health hazard is Parkinson's disease (PD) whose actual cause is still unidentified. At a glance, PD is a movement disorder symptomized by stiff muscles, impaired balance, difficulty in walking, and most importantly, tremors in the affected part when kept at rest. In general, Parkinsonian patients manifest two kinds of symptoms, one is motor, and the other is non-motor [1].
Tremors at rest, the rigidity of muscles, bradykinesia (slowness of movement), impaired posture, micrographia (decreased size of handwriting), masked face (hypomimia), and voice disorders such as dysphonia and dysarthria are some of the several motor impairments visible in this disease. Similarly, the non-motor symptoms include bradyphrenia (slowness in processing any information), sleep disturbances, decreased mental capabilities, depression, and others. Research revealed that the progressive depletion of dopamine neurotransmitters in the substantia nigra pars compacta region of basal ganglia in the midbrain is accountable for motor abnormalities appearing during this disease [2].
However, apart from the loss of dopaminergic neurons, cholinergic neurons in the basal forebrain, serotonergic and noradrenergic neurons in the brain stem, and preganglionic neurons in the intermediolateral columns of the spine can also severely affect the cognitive and autonomic systems of humans on getting depleted [3]. According to an estimation, the preliminary symptoms of PD emerge when these neurotransmitters are approximately 50–90% damaged and neuronal plasticity of the brain can no longer compensate for this loss of functional neurons [4]. Other factors reported behind cellular destruction in PD are related to the increased amount of nigral iron and reduced levels of glutathione (GSH) antioxidant [5]. A research by Tanaka and colleagues suggested that any hindrance in normal brain development during the early years of life could produce neurodegenerative as well as neuropsychiatric disorders afterwards [6]. Tanaka and colleagues further investigated the relationship between increased anti-inflammatory cytokines and reduction in neuro-modulatory function owing to kynurenine (KYN) neurotoxicity during PD [7]. This causes persistent low-grade inflammation, which contributes to motor impairment, autonomic dysfunction, and psycho-behavioral problems. It further highlights the presence of Lewy bodies in patients with PD (PwPD) with cognitive disorders.
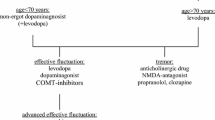
Some researches compared the characteristics of PwPD at the Young (before the age of 49), Middle (between 50 and 69 years of age), and Late (70 years or above) onset of the disease [8, 9]. They found that gait instability was frequent in the late-onset group, while tremors were common in the young-onset group. However, no significant difference was observed in gastrointestinal issues and bradykinesia. Furthermore, they also revealed that levodopa-related complications were mostly found in patients with young onset of PD.
In a nutshell, PD progresses in five stages (as shown in Fig. 1 with pathognomic indicators), which can be viewed in three phases [10,11,12]. The early phase includes stages 1 and 2, the third stage is defined under the Moderate phase and the Advance phase consists of stages 4 and 5. In the Early phase, the appearance of symptoms is a very gradual process with minimal functional impairment [11]. Thus, this phase can be easily misinterpreted as aging [13]. Then, the symptoms from the previous phase become more severe and show varying rates of deterioration for each patient. It is referred to as the Moderate phase. During this phase, minor postural impairments are visible and consequently, a patient finds it difficult to make quick reflex adjustments necessary to prevent falling. From the beginning of the Advance phase, the patient becomes severely disabled and needs round-the-clock assistance. Even in the final years, months, weeks, or days, ‘dictates of the will’ are conveyed to muscles, but their actions are perverted [14]. Although this neurodegenerative disorder is considered non-fatal, Pneumonia and any injury due to falls can cause death [15, 16].

Five significant stages of Parkinson’s disease progression
In recent years, several studies have been carried out to determine the rate of progression of Parkinsonian symptoms. One such effort utilized the metabolic profile of human serum samples collected within 3 years of the onset of PD symptoms. It revealed the elevated presence of N8-acetyl spermidine known to regulate apoptosis, which resulted in the uncontrolled death of neurons in PD patients and accelerated deterioration of associated symptoms [17]. Two other studies analyzed the wide spectrum of initial motor and non-motor dysfunctions [18], and resting-state EEG [19] to prognosticate PD into three clinical subtypes. These subtypes were motor, malignant, and intermediate progression, where the patients of the malignant group showed rapid deterioration in cognitive abilities, sleep behavior, and autonomous system. Similarly, Vijiyakumari and colleagues utilized imaging data and associated motor scores to identify further three subtypes of PD [20]. Patients classified as subtype-1 had minor motor symptoms that worsened over time, but no neuroanatomical issues were noticed. PD patients with cortical atrophy and substantially deteriorated motor symptoms were classified as subtype-2. In contrast to the other two categories, no additional deterioration of motor symptoms or cortical difficulties was noticed in individuals with subtype-3. However, axonal damage was found in diffusion tensor imaging, as well as severely compromised motor signs of the condition.
Mancy and colleagues attempted to identify patients who exhibited expeditious degeneration of symptoms in the first 2 years of the onset of PD [21]. For this, they analyzed early speech impairment, stiffed muscles, reflexes, and smell-related issues as the preliminary indicators of rapidly progressing PD. Then, to determine the deterioration rate factor over the first 2 years as well as the condition of patients, they generated the quantile partitions based on the total Unified Parkinson’s Disease Rating Scale (UPDRS) score of PwPD. In this, only a few cases of rapidly worsening PD were recognized, which were lying in the top 5% of each quantile. Similarly, Tsiouris and colleagues estimated the rate of change of Parkinsonian symptoms by categorizing the entire course of Parkinson’s treatment into (i) detection phase, (ii) hospital phase, and (iii) patient follow-up [22]. From the appearance of preliminary symptoms to continuous and consistent treatment, they applied the Hidden Markov model. It analyzed the steady-state probability distribution and assessed the rate of change in PD symptoms. In this way, it helped in the investigation of the likelihood of PD patients retaining the same stage for a longer duration. Their steady-state probability computation even revealed that the patients who can remain in the mild stage for a prolonged duration were low in percentage. Thus, it not only indicated the slow progression of the disease but the steady deterioration of symptoms also.
With an experimental setup, Chen and Zhang identified that the Brain-Derived Neurotrophic Factor (BDNF), which is known for contributing to the development of dopaminergic neurons in Substantia Nigra, was lower in PwPD compared to Healthy Subjects (HS) regardless of depression [23]. They also suggested rigorous exercise and consistent physical training to improve the levels of this serum in the brain. Moreover, Cao and colleagues utilized a tensor regression model to analyze the influence of depression in the brains of PD patients [24]. Aside from the basal ganglia, alterations in the left temporal lobe, corpus callosum, cerebellum, right temporal gyrus, fronto-occipital lobe, and thalamus were detected in individuals with both PD and depression. Nyatega and colleagues looked for abnormalities in the cerebrospinal fluid, Substantia Grisea (or Gray Matter), and Substantia Alba (or White Matter) caused due to PD [25]. From the voxel-based morphometry of PwPD and HS, low volumes of both White Matter and Gray Matter were noticed in the right calcarine and left lingual gyrus of PD patients. Contrariwise, a high volume of cerebrospinal fluid was identified in the left caudate. Furthermore, the presence of such abnormalities indicates problems, such as physical fragility as well as cognitive impairment. In addition, for identifying stages of cognitive dysfunction during PD, Brien and others utilized video-based eye tracking data of saccade, pupil, and blink activities [26].
Although blood plasma study of PD patients shows a low risk of cardiovascular issues, it also shows an increase in α-synuclein buildup, which is related to neuroinflammation and degeneration [27]. Hu and colleagues sought to limit neuroinflammation with Nitric Oxide gas (NO) and Upconversion Nanoparticle treatment, which further reduce dopaminergic neuron loss and motor problems [28]. A review study discussed the role of digital equipment, Internet-enabled devices, and electronic health records in the efficient management of PD [29]. Li and others demonstrated Multidisciplinary Comprehensive Care (MCC) methods for improving the quality of life in PD [30]. MCC involves combined care provided by the psychiatrist, neurologist, gastroenterologist, family, technology, self-support, urologist, general practitioner, pulmonologist, ophthalmologist, vascular medicine specialist, geriatrician, dentist and palliative care specialist. In contrast to standard care routine, results exhibited improved motor UPDRS and quality of life among PD patients. While no change has been observed in caregiver strain and medicinal dosage. Fujioka and colleagues conducted a survey among PwPD and neurologists to determine the optimal treatment during the later stages of PD [31]. Both participant groups turned down invasive treatments such as Deep Brain Stimulation (DBS) and intestinal gel infusion of levodopa–carbidopa and opted in favor of ingestion.
In this series, Caulfield and colleagues investigated the effect of Calcium channels in Substantia Nigra Pars Compacta in delaying the progression of PD [32] Another study suggested that PD patients with Rapid Eye Movement Sleep Behavior Disorder (REM) had more severe autonomic dysfunction than those who were not suffering from REM [33]. Moreover, such patients were also identified with an increased risk of cognitive decline as well as more deteriorated motor and non-motor functions. However, till today, the formal clinical diagnosis of PD is possible during the Moderate phase only. Nevertheless, to abate the progression of this neuronal disaster the general course of treatment prescribed by neurologists involves the use of medicines, as mentioned in Table 1 [29] 34,35,36,37,38,39,40,41 .
As evident in Table 1, most of the other disorders that arise in the later stages of Parkinson’s appear to be the side effects of increasing doses of these medicines. Besides the fact that current medical treatment can delay the rate of progression of the disease, these medicines also have harsh and long-term adverse effects on the patients [38, 41]. Moreover, another worth mentioning point is that no two PD patients have the same kind and severity of symptoms. It means that both patients experience the appearance of different symptoms at different times depending on the area of the most depleted neurons. Therefore, the present work contributes to the field of diagnosing and managing PD in the following ways:
Based on the UPDRS score of appeared symptoms in Parkinsonian patients, the present approach calculated numerical criteria for determining the stage-specific transition and retention thresholds. Furthermore, it evaluated the impact of medicines on the progression of PD both graphically and numerically. For this, the average rate of deterioration of symptoms in treated and untreated patients using the cumulative UPDRS score of different symptoms is calculated. A time delay pattern is calculated that depicts the average maximum stage retention time of treated and untreated patients at each stage. The study investigated the duration regulation provided by medicines over the worsening of six prime and earlier symptoms. A saturation period is also identified during which a proper treatment can minimize PD progression to negligible. Finally, the present work suggests an alternative line of remedies for Parkinson’s patients to improve PD management.
The work continues with the Methods in Sect. 2, which gives an insight into the proposed work along with the data sets used. Results are included in Sect. 3, and alternative remedies are suggested and discussed in Sect. 4, followed by Conclusion in Sect. 5.
Methods
The complex character exhibited by non-fatal and incurable PD differs from patient to patient [2, 10]. Studies regarding its stages [10, 42], progression [13, 17, 18, 20,21,22, 43, 44], and treatments [34,35,36,37,38,39, 45,46,47,48,49,50,51] altogether indicate the timely identification and management of such a disease must be of utmost concern. To ensure that PD patients’ quality of life can never be compromised, and they may live a totally normal life free of issues caused by the illness, except at the final stage. With this in mind, we tried to estimate the stage transition and retention thresholds, and the rate of deterioration of symptoms in untreated patients. This helps in computing the time that prescribed therapies and medications add in the stages as improvements in the prevailing symptoms. In addition, we suggest counselling, herbal medicines, home remedies, bio-cleansing therapies, yoga asanas, and physio-, psycho-, socio-, and speech therapies as alternative lines of medications to slow down the progression of PD by increasing the stage retention time. In this way, a better quality of life can be ensured for each patient at any stage of PD excluding the last one (stage 5).
The Parkinson’s Progression Markers Initiative (PPMI) has developed multiple data sets funded by the Michael J Fox Foundation for PD Research [52]. These data sets comprise data obtained from various kinds of tests, including UPDRS, neurological, motor, non-motor, medical history, sleep behavior, digital sensors, imaging, and others. To accomplish the proposed work, UPDRS Part-I, II, and III, diagnostic features, determination of falls, Epworth sleepiness scale, REM Sleep Disorder Questionnaire, diagnostic features, Physical Activity Scale for the Elderly (PASE), University of Pennsylvania Smell ID test, Household activities and Use of Medicines are some of the data sets by PPMI, which are selected to acquire the features required for achieving the proposed objectives.
In general, UPDRS was developed in the 1980s as a gold standard for monitoring the severity and progression of PD [19]. It can be analyzed in six parts by means of Intellectual Functions (Mood, Behavior, and Mentation), Activities of Daily Living, Motor Examination, Complications of therapy, Hohen and Yahr Scale (HY), and Schwab and England Activities of Daily Living (SE-ADL) [53]. In the proposed approach, out of six, only the first three parts are analyzed. The scoring of UPDRS ranges from 0 to 4, which represents No, slight, mild, moderate, and severe symptoms in their consecutive order. The olfactory issues associated with PD can be detected effectually with the help of the Smell Identification Test [10, 54]. This test was introduced by the University of Pennsylvania, also known as UPSIT. It comprises 40 items arranged in the four booklets. In general, the UPSIT score for a normal olfactory function is greater than 35. It means that the more the number of smells identified correctly, more is the UPSIT score. Thus, a UPSIT score of less than 18 clearly defines anosmia, and partial loss of sense of smell (hyposmia) can be interpreted with a score ranging between 18 and 34. Enacting dreams during sleep with vocal sounds and physical actions is considered REM [33, 55, 56]. The actions performed by REM patients during sleep include murmuring, laughing, crying, shouting, kicking, punching, waving arms, or even falling from bed. These symptoms can be numerically interpreted with 0 (NO SYMPTOM) and 1 (SYMPTOMS OBSERVED).
Similarly, a questionnaire for assessing the age-specific physical ability and lifestyle behaviors in aged patients is referred to as PASE [57]. It is based on the time devoted to routine activities, such as walking, gardening, exercise, and other household chores. The overall PASE score ranges from 0 to 793, considering the intensity and frequency of activity, such as light or heavy activity, amount of work done in hours, and so forth. The higher scores represent greater levels of physical activity. Epworth sleepiness scale measures the rate of the tendency of the patient to become sleepy in eight different situations elaborately mentioned in [56, 58]. The maximum score is 24. Now, if the obtained score lies between 0 and 7, it means that the patient does not suffer daytime sleepiness. A score between 8–9 and 10–15 can be interpreted as average daytime sleepiness and situation-dependent excessive sleepiness, respectively. While a score between 16 and 24 indicates that the patient is suffering from a sleep disorder. The data set named Diagnostic Features and Use of Medicines includes all symptoms that appeared during the various phases of PD and the medicines commonly used for PD treatment.
The stage-specific retention and transition thresholds are evaluated for the first four stages of PD, since after stage 5 no further stage transition is possible. The symptoms selected for evaluating these thresholds can be arranged in ascending order of stages as follows:
Symptoms for stage 1 include \({\mathbf{F}\mathbf{e}\mathbf{a}\mathbf{t}\mathbf{s}}_{\mathbf{s}1}=\{\)Depression, Hallucinations, Anxiety, Fatigue, Occasional tremors, Increased voice tone, Rigidity, Bradykinesia\(\}\). Symptoms for stage 2 comprise \({\mathbf{F}\mathbf{e}\mathbf{a}\mathbf{t}\mathbf{s}}_{\mathbf{s}2}=\{\)Rapid speech, Micrographia, Unilateral tremors, Decreased Facial expressions, Bulbar dysfunction, Akinesia, hyperkinesia, Postural hypotension, Oculomotor disturbances, Rapid progression of the disease\(\}\). Symptoms for stage 3 include \({\mathbf{F}\mathbf{e}\mathbf{a}\mathbf{t}\mathbf{s}}_{\mathbf{s}3}=\{\)Sleep disturbances, pain and other sensations, Urine and constipation problems, Lightheadedness, freezing of gait, Postural and bilateral tremors, Difficulty in maintaining hygiene, Mild problems in eating, walking, turning in bed, and getting out of bed or chair, Daytime sleepiness, Hyposmia\(\}\). And, symptoms for stage 4 contain \({\mathbf{F}\mathbf{e}\mathbf{a}\mathbf{t}\mathbf{s}}_{\mathbf{s}4}=\{\) Issues in finger and toe-tapping, Difficulty in making hand movements, Pronation and supination, Increased leg agility, Difficulty in arising from chair or car, Global spontaneity of movement, Violent and kinetic tremors, Motor ataxia, Tendency to fall, Dystonia, Severe urinary and bowel dysfunction, Little or no response to levodopa, Prominent and increased intensity of freezing of gait in last year, Inability to perform routine household activities, Epworth sleepiness score ranging between 18 and 24 representing a severe condition, REM Sleep disorder, Anosmia \(\}\)
Now, depending on the presence and severity of the symptom in the patient under consideration, each of the aforesaid symptoms holds a UPDRS score of either 0, 1, 2, 3, or 4. Therefore, Eq. (1) can be used to obtain the numeric values of these thresholds by aggregating these UPDRS scores.
where \(i=1 \space \mathrm{to} \space 4\) represents stages 1 to 4.
\({Feats}_{si}\) includes the UPDRS score associated with each above-mentioned symptom.
\(n\) stands for the number of patients in \({Feats}_{si}\).
\({s}_{i}\) stores the average total sum of the obtained scores, which is the threshold point of that particular stage.
Now, if a patient attains a value above the threshold point calculated for a particular stage, then it represents a stage transition. Otherwise, it signifies stage retention. It is worth mentioning that in each stage, each considered symptom is given equal importance.
To assess the impact of medications on the progression of PD, four sets of symptoms are used. These symptoms are taken from the parameters included in UPDRS Part I, II, and III. Set 1 includes symptoms related to intellectual impairment, thought disorder, depression, and anxiety. Set 2 includes symptoms associated with sleep disturbances, daytime sleepiness, lightheadedness, fatigue, constipation, and urinary problems. Similarly, Parkinson’s symptoms which are allied with activities of daily living such as speech, dressing, hygiene, eating, walking, and maintaining balance along with occasional unilateral tremors, and mild micrographia are included within Set 3. Set 4 is inclusive of parameters akin to bradykinesia, bilateral and violent tremors, severe speech impairment, postural stability, leg agility, issues in the toe and finger tapping, facial expression, gait, and other motor symptoms from UPDRS part III.
In general, patients under treatment can either be in the later years of stage 2 or any of the stages from 3 to 5. On the other hand, the patients in the non-treatment-taking group are in the initial stages of PD. Therefore, the patients are firstly segregated into treatment and non-treatment-taking groups by using the Use of Medicines data set. Then, the numerical values for evaluating the rate at which Parkinsonian symptoms deteriorate are obtained from UPDRS Part I, II, and III and calculated as per Eq. (2). This difference between the average UPDRS score of patients under treatment and the same of not taking any treatment yields an experimental estimation of the average rate of deterioration of symptoms:
where \(wot\) stands for the UPDRS score of untreated patients.
\(wt\) stands for the UPDRS score of patients under treatment.
Several studies remarked that the formal clinical diagnosis of PD after the age of 65 years cannot support a patient to live a long and healthy life even after medication. However, if this diagnosis is made before 55 years of age then the chances of longer survival increase [43]. Moreover, even the patient sometimes will never have to experience the symptoms of the Advance phase. Therefore, utilizing the available literature, and from the experimental assessment of the UPDRS score, the present work provides a graphical representation of the impact of medicines on four subsets of symptoms, six preliminary prime symptoms of PD, and a time scale representing the progression time of each stage. These six prime symptoms are bradykinesia, gait disorder, masked face, tremors, voice impairment, balance and walking difficulties.
Although PD is a multifactorial disease, its symptoms differ from one patient to another. This variation can be seen in terms of the appearance of symptoms, timing of onset, duration of progression, and severity of symptoms. Thus, it is important to monitor even slight impairments in the normal functioning of the human system to understand the role of time bounds in the appearance and progression of PD. These impairments can be observed in day-to-day activities, such as minor loss of sense of smell, monotonous speech, trivial hoarseness in voice, and increased slowness in daily routine chores. However, some patients also experience cognitive troubles, such as increased time of solving simple arithmetic calculations and recalling. Hence, early detection of PD and the commencement of associated remedies are essential to improve the stage-retention time and the quality of life.
Results
Using the UPDRS score of 500 patients collected during 2011–19 at intervals of 3 months from PPMI, the four threshold points to predict stage retention or transition are depicted in Fig. 2.

Parkinson’s disease stage transition or retention thresholds. Here, the blue circles represent each of the five stages of PD. The orange arrows represent the transition from stage \({{\varvec{s}}}_{{\varvec{i}}}\) to \({{\varvec{s}}}_{{\varvec{i}}+1}\) with numerical threshold probabilities and the green arrows depict stage retention
As evident only two movements are possible. A forward movement with stage transition and a hold action during stage retention. It signifies that with PD, it is not possible to go back to the previous stage. These thresholds are also expressed in Table 2, where S represents stages, and the number followed by it denotes the stage number.
Accordingly, the first threshold is S1 at 6.574, the second threshold is S2 at 11.242, the third threshold is S3 at 23.02 and the fourth threshold is S4 at 47.672. Consequently, if the estimated threshold point for a sample subject is 24, it represents a transition from stage 3 to stage 4. It also signifies that the patient is in the earlier years of stage 4. Similarly, if the estimated threshold point for a sampled subject is 10.33, the subject will continue in stage 2. Even this indicates that the patient is in the later years of stage 2.
A comparison between the collective UPDRS scores of 1000 PD patients, out of which 500 are taking medicines and the rest are untreated helps in evaluating the average rate of deterioration of Parkinsonian symptoms. The experimental calculations according to Eq. (2) yield a variation of 15.345% in the rate of deterioration of symptoms. The probable cause of such variation is the heterogeneous nature of this malady. Therefore, the overall rate of deterioration of symptoms lies between UPDRS scores of 32.31 and 37.68 annually considering the various combinations of patients within the sample size. It means that symptoms of PD deteriorate 34.995% averagely faster in untreated persons rather than in those who receive treatments. The same comparison is graphically demonstrated in Fig. 3a, b.

a Impact of treatments on overall UPDRS scores of Parkinsonian patients. b Impact of treatments on six-prime symptoms of Parkinson’s disease. The bar graph in (a) plots a comparison between the overall UPDRS score obtained from four sets of symptoms, and (b) depicts the impact of medicines on six prime symptoms mentioned in Sect. 2
As evident from both illustrations, the cumulative UPDRS score of treated Parkinson’s patients is less than untreated patients. However, only a slight difference is observed in the case of the Balance symptom, which represents postural instability.
Moreover, a saturation period can exist during the progression of PD. It is the time when the rate of change in cumulative UPDRS score becomes steady in comparison with other stages. In terms of stages, the duration between the initial years of the third stage and the final years of the second stage is identified as the saturation period. Table 3 tabulates the deterioration in the average UPDRS scores during the initial 2–2.5 years of the three phases of PD computed experimentally.
As assessed the deterioration rate of the UPDRS score during the initial 2.5 years of moderate phase is minimal, thus it can be considered a saturation period. Any accurate course of treatment during this period can reduce the progression of the disease to negligible. Another perceptible observation is the duration of regulations provided by medicines during ON and OFF times. However, some temporary improvements are visible in the symptoms during ON times which subside near OFF times. However, if the patients are examined within 1 to 2 h of medication, no improvement is visible. If the time between medication and examination is increased, an impermanent improvement of symptoms is seen. Such an improvement can be quantitively measured by assessing HY stages and UPDRS scores of six prime symptoms.
As evident from Fig. 4, medicines successfully control bradykinesia, masked face, and speech issues; however, only minor improvements are visible in tremors, gait, balance, and walking. Analyzing these charts exhibits a 6–7 year long regulation over the degression of five out of six prime symptoms. It means that the effect of treatment on these prime symptoms only lasts for about an average of 4.8 years. After which, modifying or increasing the dosage of medicines is needed. In summary, the regular course of prescribed medicines will improve only the movement-associated symptoms not the coordination of muscles. However, a temporary backward transition from stage \(i\) to \(i-1\) is visible during the ON times of medicines. Since such a transition prevails for a shorter duration only, therefore we do not consider this transition in our proposed work.

Deterioration of six prime symptoms with and without medicines. This figure portrays the positive impact of medicines on regulating the deterioration of six prime Parkinsonian symptoms observed for 9 years, which is from January 2011 to January 2019, according to the data set obtained from PPMI. The average UPDRS score is shown on the y-axis, and time (in years) is indicated on the x-axis. The green color represents Parkinsonian patients under treatment and the red color shows untreated patients. Similarly, the deterioration of symptoms is illustrated by the increase in the average UPDRS score
Experimentally, the minimum retention time of any stage before the symptoms begin to further deteriorate for both treated and untreated patients can be presumed as 2.5 years for stages 1, 2, and 3. This time is reduced by 6 months for patients in stage 4 depicting that a patient can remain in stage 4 for 2 years only. In this way, the maximal time for which an untreated PD patient can retain a stage is 12 years for stage 1, 10 years for stage 2, 8 years for stage 3, and 5 years for stage 4. Thus, the overall progression of PD for an untreated patient can be portrayed on a time scale of 15 years, as shown in Fig. 5a also.

a Progression of Parkinson’s disease for untreated patients (represented by orange arrows). b Parkinson’s disease progression for patients taking medicines (represented by green arrows)
Experimental results revealed a delay pattern in the progression of PD after medication. Although the slow deterioration of symptoms is achieved from the benefits of treatments, nevertheless the reduction in delay percentage is due to the gradually subsiding effect of those treatments. This delay in Parkinson’s progression is 37.68%, 35.86%, 34.27%, and 32.31%, respectively, from stages 1 to 4. Thus, for patients taking medicines, the progression of PD can be further increased for 5 years generating a time scale of 20 years. As shown in Fig. 5b, this delay in the progression of PD can be stated in years as 4.44 for stage 1, 3.5 for stage 2, 2.72 for stage 3, and 1.6 for stage 4. Therefore, the experimentally evaluated maximum stage retention time of treated PD patients is 6 years 6 months for stage 1, 10 years 7 months for stage 2, 13 years 5 months for stage 3, and 16 years 4 months for stage 4. Consequently, compared to untreated patients, medicines can improve the overall life span of PD patients by further 12 years. Table 4 summarizes the stage retention time of both treated and untreated PD patients.
In short, the stagewise thresholds are derived by empirically examining the UPDRS scores from the PPMI data [52], which are 6.574, 11.242, 23.02, and 47.672 for stages 1, 2, 3, and 4, respectively. The yearly rate of worsening of the average UPDRS score in untreated PwPD is 34.995% engenders as a result of the heterogeneous nature of the malady. In addition, during the early years of stage 3 and later years of stage 2, the least progression in UPDRS score is observed, which is 0.072 on average. This can be referred to as saturation point in PD. Eventually, medications successfully reduced bradykinesia, masked face, and speech difficulties. While only slight improvements in tremors, gait, walking, and balance have been observed. It illustrates the effect of treatments on these primary symptoms lasting just 4.8 years at most. Following that, a change in medication dose is required.
Discussion
With a thought to improve the quality of life of PD patients, and ensure that prescribed drugs would provide the maximum benefit with no adverse effects. It becomes essential to understand how disease progresses and how long treatments may relieve symptoms so that the affected person can live a normal life. The evaluation of stage retention and transition threshold is carried out for this aim. These thresholds not only aid in determining the stage, but also whether a patient is in the early, middle, or later years of a certain stage.
Similarly, the estimated rate of deterioration indicates that, in comparison with treated patients, untreated patients experienced 34.995% of progressively deteriorated symptoms on average per year. It implies that treated PwPD have a lower cumulative UPDRS score than untreated ones, and medicines can help regulate specific symptoms. This also highlights a saturation period, which appears during the initial years of stage 3 and the later years of stage 2, such that 0.072 is the smallest decline in UPDRS score across the three phases. It implies that any proper treatment administered during this time period can minimize the progression to almost negligible.
Despite temporary benefits and side effects, medicines leave a positive impact on PD symptoms. Bradykinesia, tremors, masked face, speech problems, gait, balance, and walking are among the six prime symptoms. With the aid of treatments, patients with Bradykinesia, masked face, and speech impairments experience more control over these symptoms than the rest of the symptoms. The effect of treatment on these prime symptoms lasts for at most 4.8 years. Furthermore, the experimental research demonstrated that with the help of medications, a PD patient's life may be extended for 12 more years, during which a patient can live a nearly normal life, with the exception of patients in advanced phase.
Taking into account computed stage retention time, and to further improve the benefits of medicines, and simultaneously eliminating their side-effects, we suggest a series of therapeutics. These include counselling, diet changes, yoga asanas, bio-cleansing therapies, and herbal medicines as home remedies.
Alternative therapies
The current pharmacological treatment of Parkinsonian patients is done with large oral doses of dopamine supplements and steroids [34, 37, 38, 45, 46]. It, unfortunately, causes irreversible damage to the liver and kidney. In addition, the net efficacy of dopamine agonist treatments diminishes with time and these Parkinsonian symptoms return once the effect of the drug dosage wears off. Although timely treatments for PD increase life expectancy, nevertheless have a certain number of side effects too (mentioned in Table 1). Therefore, we suggest the use of alternative therapies for an unobtrusive appearance of PD symptoms. Besides this, these treatments can even be taken with the prescribed medicines.
According to Madhav Nidan of Ayurveda, the human body is made up of five elements. These are air, fire, water, space, and earth. The combination of these elements generates three doshas named Vata, Pitta, and Kapha. PD, also known as ‘Kampvata’ is caused due to the toxins formed by highly unstable Vata dosha [59,60,61]. During this, the air element in the human body gets accumulated in the free spaces (Space element) and forms free radicals. Hence, Ayurveda and Naturopathy focus on balancing the Vata dosha by boosting the antioxidant levels because they are renowned to stabilize free radicals. In addition, they enhance immunity, increase the rate of neurogenesis, protect neurons from further damage, and help in maintaining autonomous control and coordination of human body functions.
The lifestyle management counseling suggested in the proposed work includes diet plans, yoga asanas (exercises with regulated breathing), panchakarma (bio-cleansing), and drug therapies, for earlier and more effective management of PD [47, 59,60,61,62,63].
Preventive therapies help in maintaining good physical and mental health by suggesting some diet and lifestyle changes, exercises, and increased activities of the affected part [29, 59, 62,63,64,65,66]. It further intensifies brain communication and nerve functions.
The diet of a Parkinsonian patient should contain foods rich in fiber, such as whole-grain cereals, brown rice, and ketones. Coconut and red palm oil are good-source of ketones. It must also include green leafy vegetables, flax seeds, milk from the Bos Indicus cow breed, antioxidants, garlic, and plenty of water. Withania somnifera (Ashwagandha) renowned to treat general weakness should be consumed with vitamins B6, C, and E. It helps to enhance the normal functioning of human autonomous systems and protects Parkinson’s patients from further neuronal damage. During PD, it is insisted to avoid foods with high sugar content, such as glucose, wine, and refined flour. Moreover, it is also suggested to limit the intake of salt, protein, and manganese, and refrain from carbonated drinks, saturated foods, and fast foods.
Psychological support helps a patient to feel independent and reinforced with stabilized emotions [67,68,69]. Such kind of mental support helps in slowing down the pace of neuronal degeneration.
Speech Therapy helps in treating dysphonia and dysarthria [70,71,72]. During this therapy, patients are trained to regulate breathing and control the utterance of words while talking.
Physio-therapy with Occupational Exercise assists in controlling agitation of the affected portion by keeping it busy with hobbies and daily activities. The patients in the third or later stages are advised to indulge in excessive training of the affected part to improve posture instability and coordination of muscles [8, 9, 44, 64, 73]. Similarly, Stretching exercises and balance training eliminate rigidity and tackle scelotybre festinatinans. It also helps to correct altered balance and posture to reduce the risk of frequent falls.
The best bio-cleansing therapy (or Panchakarma treatment) is massage with medicated herbal oils, such as sesame, Brahmi, coconut, and olive oils. It reduces stiffness and pain. It is prescribed for either 7, 14, or 21 days depending on the severity of symptoms [59, 60, 62]. Other therapies of Panchakarma include Shirodhara, Nasya, Basti, and Njavarakhizi therapy. Shirodhara relaxes the hypothalamus gland to induce sound sleep, calm emotions, and control Parkinsonian tremors. Nasya therapy stimulates the pineal gland and nourishes the frontal lobe of the nervous system for optimal function of motor nerves. Basti detoxifies the body and Njavarakhizi nourishes, rebuilds, and regenerates the damaged musculoskeletal tissue.
Yogic practices focuses on overcoming several Parkinsonian symptoms by relaxing the brain, training affected organs, and rejuvenating body cells. It also helps in expelling exaggerated Vata dosha through several posture exercises (asanas) and regulated breathing training (pranayama). Ten yoga asanas helpful in managing PD are described in Table 5 [60,61,62,63].
Apart from various therapies, herbal medicines also play a significant role in controlling various Parkinsonian symptoms. These herbal medicines can be consumed for short intervals of 15–21 days. It effectively promotes neuroprotection, controls tremors, and slowly alleviates other symptoms. Alternative treatments do not repair the damage that has been done yet, although they can help to delay further damage without side effects. In some cases, trivial replenishment of damaged neurons is also observed [45]. Thus, it helps the patient to remain in the same stage of PD for a longer duration.
A comparison between traditionally prescribed treatments and the proposed remedies is tabulated in Table 6 [29, 34,35,36,37, 45,46,47, 59,60,61,62,63, 73].
The present study also has some limitations. First, we could not account for the transient backward transition noticed during medication ON time. As a result, further tests and investigations may be conducted to identify various methods of stabilizing such transient backward transitions. More work can be done to study the progression of each associated symptom separately, such as smell dysfunction, hypomimia, and so forth. Thus, further analysis of such kinds regarding this heterogeneous-natured disease can pave the way for more customized treatments with minimal noxious effects.
Conclusion
The proposed approach concentrates on examining the four-stage retention and transition thresholds of PD patients evaluated using UPDRS scores of certain symptoms. Irrespective of gender and heterogeneity, these threshold points signify the current stage as well as the time spent in that stage. The experimentally calculated average rate of deterioration of symptoms in untreated PwPD is 34.995%, demonstrating the influence of medications in regulating symptoms and reducing their progression. A saturation period is discovered in which the average annual decline of the UPDRS score is 0.072, and with the right medication, its further progression can be minimized to negligible. In addition, the usage of conventionally prescribed medications such as levodopa, MAO-B inhibitors, dopamine agonists, and anticholinergic medications offers an average relief of 4.8 years in five out of six prime PD symptoms. Such a time delay pattern in the PD progression represents the enhanced stage retention time. As a result, the overall life span of such patients can be extended for 12 more years. Finally, to improve the quality of life of PwPD and minimize the adverse aftereffects of traditional PD treatments, early stage counseling, diet changes, herbal home remedies, yogic practices, bio-cleansing, and other different therapies are suggested. Studies for understanding and stabilizing the transient backward transition observed during the ‘ON’ time of medication, and analyzing the progression of each symptom separately can be carried out in the future to aid in identifying more customized treatments with minimal noxious effects.
Availability of data and materials
The data sets generated and/or analysed during the current study are available from the Parkinson’s Progression Markers Initiative (PPMI). https://www.ppmi-info.org/ [52].
Abbreviations
- UPDRS:
-
Unified Parkinson’s Disease Rating Scale
- PD:
-
Parkinson’s disorder
- REM:
-
Rapid eye movement sleep behaviour disorder
- HY:
-
Hoehn and Yahr Stages
- SE-ADL:
-
Schwab and England Activities of Daily Living
- PPMI:
-
Parkinson’s Progression Marker’s Initiative
- PwPD:
-
Patients with Parkinson’s disease
- EEG:
-
Electroencephalography
- BDNF:
-
Brain-derived neurotrophic factor
- HS:
-
Healthy subjects
- MRI:
-
Magnetic resonance imaging
- MCC:
-
Multidisciplinary comprehensive care
- DBS:
-
Deep brain stimulation
- MAO-B:
-
Monoamine oxidase-type B
References
Gokcal E, Gur VE, Selvitop R, BabacanYildiz G, Asil T. Motor and non-motor symptoms in Parkinson’s disease: effects on quality of life. Noro Psikiyatr Ars. 2017;54:143–8.
Bhat S, Acharya UR, Hagiwara Y, Dadmehr N, Adeli H. Parkinson’s disease: cause factors, measurable indicators, and early diagnosis. Comput Biol Med. 2018;102:234–41.
Elias S, Israel Z, Bergman H. Physiology of Parkinson’s disease. In: Hallett M, Poewe W, editors. Therapeutics of Parkinson’s disease and other movement disorders. United Kingdom: Wiley-Blackwell; 2008. p.25–36. https://doi.org/10.1002/9780470713990.ch2.
Gutteridge JMC, Halliwell B. Oxidative stress, brain iron and neurodegeneration. Basic principles. In: Olanow CW, Jenner P, Youdim M, editors. Neurodegeneration and neuroprotection in Parkinson's disease. London: Academic; 1996. p. 1–21.
Jenner P, Olanow CW. Pathological evidence for oxidative stress in Parkinson’s disease and related degenerative disorders. In: Olanow CW, Jenner P, Youdim M, editors. Neurodegeneration and neuroprotection in Parkinson’s Disease. London: Academic; 1996. p. 23–45.
Tanaka M, Spekker E, Szabó Á, Polyák H, Vécsei L. Modelling the neurodevelopmental pathogenesis in neuropsychiatric disorders. Bioactive kynurenines and their analogues as neuroprotective agents—in celebration of 80th birthday of Professor Peter Riederer. J Neural Transm. 2022; 129:627–42.
Tanaka M, Toldi J, Vécsei L. Exploring the etiological links behind neurodegenerative diseases: inflammatory cytokines and bioactive kynurenines. Int J Mol Sci. 2020;21:2431.
Mehanna R, Moore S, Hou JG, Sarwar AI, Lai EC. Comparing clinical features of young onset, middle onset and late onset Parkinson’s disease. Parkinson Relat Disord. 2014;20:530–4.
Mehanna R, Jankovic J. Young-onset Parkinson’s disease: its unique features and their impact on quality of life. Parkinson Relat Disord. 2019;65:39–48.
Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry. 2008;79:368–76.
Dalvi A. Premotor symptoms. In: Pahwa R, Lyons KE, editors. Handbook of Parkinson’s disease. 5th ed. Boca Raton: CRC; 2013. p. 93–102.
Indu R, Chandra Dimri S. Diagnosing Parkinson’s Disease: its evolution to future. 2022 International Conference on Computational Intelligence and Sustainable Engineering Solutions (CISES). IEEE; 2022. p. 108–115.
Samii A. Cardinal features of early Parkinson’s disease. In: Factor SA, Weiner WJ, editors. Parkinson’s disease: diagnosis and clinical management. 2nd ed. New York: Demos; 2008. p. 45–54.
Lees A. An essay on the shaking palsy. Brain. 2017;140:843–8.
Kuo WY, Huang KH, Kuan YH, Chang YC, Tsai TH, Lee CY. Antidepressants usage and risk of pneumonia among elderly patients with the parkinson’s disease: a population-based case-control study. Front Med. 2022;9:740182. https://doi.org/10.3389/fmed.2022.740182.
Won JH, Byun SJ, Oh BM, Park SJ, Seo HG. Risk and mortality of aspiration pneumonia in Parkinson’s disease: a nationwide database study. Sci Rep. 2021;11(1):6597. https://doi.org/10.1038/s41598-021-86011-w.
Roede JR, Uppal K, Park Y, Lee K, Tran V, Walker D, et al. Serum metabolomics of slow vs rapid motor progression Parkinson’s disease: a pilot study. PLoS One. 2013;8: e77629.
Fereshtehnejad SM, Romenets SR, Anang JB, Latreille V, Gagnon JF, Postuma RB. New clinical subtypes of Parkinson disease and their longitudinal progression: a prospective cohort comparison with other phenotypes. JAMA Neurol. 2015;72(8):863–73. https://doi.org/10.1001/jamaneurol.2015.0703.
Yassine S, Gschwandtner U, Auffret M, Duprez J, Verin M, Fuhr P, et al. Identification of Parkinson’s disease subtypes from resting-state electroencephalography. Mov Disord. 2023;38:1451–60.
Vijayakumari AA, Fernandez H, Walter B. Data-driven approach to identify subtypes and progression of Parkinson’s disease using multimodal imaging data (P6-11.006). Neurology. Ovid Technologies (Wolters Kluwer Health); 2023. https://doi.org/10.1212/WNL.0000000000201861.
Mancy KM, Suresh G, Vijayalakshmi C. Implementation of a Markov model for the analysis of Parkinson’s disease. In: Luhach A, Kosa J, Poonia R, Gao XZ, Singh D, editors. First International Conference on Sustainable Technologies for Computational Intelligence. Advances in Intelligent Systems and Computing. Singapore: Springer; 2020. p. 481–493.
Tsiouris KM, Rigas G, Gatsios D, Antonini A, Konitsiotis S, Koutsouris DD, et al. Predicting rapid progression of Parkinson’s Disease at baseline patients evaluation. 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). IEEE; 2017. p. 3898–3901.
Chen Z, Zhang H. A meta-analysis on the role of brain-derived neurotrophic factor in Parkinson’s disease patients. Adv Clin Exp Med. 2022;32:285–95.
Cao X, Yang F, Zheng J, Wang X, Huang Q. Aberrant structure mri in parkinson’s disease and comorbidity with depression based on multinomial tensor regression analysis. J Pers Med. 2022;12(1):89. https://doi.org/10.3390/jpm12010089.
Nyatega CO, Qiang L, Adamu MJ, Kawuwa HB. Gray matter, white matter and cerebrospinal fluid abnormalities in Parkinson’s disease: a voxel-based morphometry study. Front Psychiatry. 2022;13:1027907. https://doi.org/10.3389/fpsyt.2022.1027907.
Brien DC, Riek HC, Yep R, Huang J, Coe B, Areshenkoff C, et al. Classification and staging of Parkinson’s disease using video-based eye tracking. Parkinsonism Relat Disord. 2023;110:105316. https://doi.org/10.1016/j.parkreldis.2023.105316.
Bartl M, Dakna M, Schade S, Otte B, Wicke T, Lang E, et al. Blood markers of inflammation, neurodegeneration, and cardiovascular risk in early Parkinson’s disease. Mov Disord. 2023;38:68–81.
Hu B, Fang H, Huang Z, Huang W, Huang L, Liu H, et al. An upconversion nanoplatformbased multi-effective theatment for Parkinson’s disease. Chem Eng J. 2023;465:142959. https://doi.org/10.1016/j.cej.2023.142959.
Gupta R, Kumari S, Senapati A, Ambasta RK, Kumar P. New era of artificial intelligence and machine learning-based detection, diagnosis, and therapeutics in Parkinson’s disease. Ageing Res Rev. 2023;90:102013. https://doi.org/10.1016/j.arr.2023.102013.
Li T, Zou X, Kang Y, Sun M, Huang X, Duan X. A meta-analysis of the effect of multidisciplinary comprehensive care on health-related quality of life and Unified Parkinson’s Disease Rating Scale in Parkinson’s disease. Adv Clin Exp Med. 2023;32:623–31.
Fujioka S, Mishima T, Yamazaki T, Bebrysz M, Nomoto M, Yamaguchi J, et al. Neurologists’ preferences for device-aided therapy for advanced Parkinson’s disease in Japan. Curr Med Res Opin. 2023;39:91–104.
Caulfield ME, Manfredsson FP, Steece-Collier K. The role of Striatal Cav1.3 calcium channels in therapeutics for Parkinson’s Disease. In: Striessnig J, editor. Voltage-gated Ca2+ channels: pharmacology, modulation and their role in human disease. Handbook of experimental pharmacology. Cham: Springer. 2023. p. 107–137.
Figorilli M, Meloni M, Lanza G, Casaglia E, Lecca R, Saibene FL, et al. Considering REM sleep behavior disorder in the management of Parkinson’s disease. Nat Sci Sleep. 2023;15:333–52.
Simuni T, Hurtig H. Levodopa: a pharmacologic miracle four decades later. Parkinson’s disease: diagnosis and clinical management. In: Factor SA, Weiner WJ, editors. Parkinson’s Disease: diagnosis and clinical management, 2nd edn. New York: Demos; 2008. p. 471–490.
Adler CH. Amantadine and anticholinergics. In: Factor SA, Weiner WJ, editors. Parkinson’s disease: diagnosis and clinical management. 2nd ed. New York: Demos; 2008. p. 491–8.
Rajput A, Zesiewicz T, Hauserin R. Monoamine oxidase inhibitors. In: Factor S, Weiner W, editors. Parkinson’s disease: diagnosis and clinical management. 2nd ed. New York: Demos; 2008. p. 499–514.
Nisipeanu P, Korczynin A. Dopamine agonists. In: Factor S, Weiner W, editors. parkinson’s disease: diagnosis and clinical management. 2nd ed. New York: Demos; 2008. p. 515–32.
Rinaldi D, Imbalzano G, Galli S, Bianchini E, Ledda C, De Carolis L, et al. The impact of dysphagia in Parkinson’s disease patients treated with levodopa/carbidopa intestinal gel. Parkinsonism Relat Disord. 2023;109:105368. https://doi.org/10.1016/j.parkreldis.2023.105368.
Rinaldi D, Alborghetti M, Bianchini E, Sforza M, Galli S, Pontieri FE. Monoamine-oxidase type B inhibitors and cognitive functions in Parkinson’s disease: beyond the primary mechanism of action. Curr Neuropharmacol. 2023;21:1214–23.
Alrouji M, Al-Kuraishy HM, Al-Gareeb AI, Saad HM, Batiha GE-S. A story of the potential effect of non-steroidal anti-inflammatory drugs (NSAIDs) in Parkinson’s disease: beneficial or detrimental effects. Inflammopharmacology. 2023; 31:673–688.
Leta V, Klingelhoefer L, Longardner K, Campagnolo M, Levent HÇ, Aureli F, et al. Gastrointestinal barriers to levodopa transport and absorption in Parkinson’s disease. Eur J Neurol. 2023;30:1465–80.
Jankovic J, Mehanna R. Pathophysiology and clinical assessment. In: Pahwa R, Lyons KE, editors. Handbook of Parkinson’s Disease. 5th ed. Boca Raton: CRC; 2013. p.61–92.
Hawkes CH, Del Tredici K, Braak H. A timeline for Parkinson’s disease. Parkinsonism Relat Disord. 2010;16:79–84.
Kilinc B, Cetisli-Korkmaz N, Bir LS, Marangoz AD, Senol H. The quality of life in individuals with Parkinson’s Disease: is it related to functionality and tremor severity? A cross-sectional study. Physiother Theory Pract. 2023. https://doi.org/10.1080/09593985.2023.2236691.
Connolly BS, Lang AE. Pharmacological treatment of Parkinson disease. JAMA. 2014;311:1670–83.
Lee TK, Yankee EL. A review on Parkinson’s disease treatment. Neuroimmunol Neuroinflamm. 2022;8:222–44.
Sy MAC, Fernandez HH. Pharmacological treatment of early motor manifestations of Parkinson disease (PD). Neurotherapeutics. 2020;17:1331–8.
Mantovani E, Zucchella C, Argyriou AA, Tamburin S. Treatment for cognitive and neuropsychiatric non-motor symptoms in Parkinson’s disease: current evidence and future perspectives. Expert Rev Neurother. 2023;23:25–43.
Gasser T. Genetic testing for Parkinson’s disease in clinical practice. J Neural Transm. 2023;130:777–82.
Dumbhare O, Gaurkar SS. A review of genetic and gene therapy for Parkinson’s disease. Cureus. 2023;15(2):e34657. https://doi.org/10.7759/cureus.34657.
Chopade P, Chopade N, Zhao Z, Mitragotri S, Liao R, Chandran Suja V. Alzheimer’s and Parkinson’s disease therapies in the clinic. Bioeng Transl Med. 2023;8(1):e10367. https://doi.org/10.1002/btm2.10367.
PPMI. PPMI Dataset. Parkinson’s Progression Marker’s Initiative. https://www.ppmi-info.org/. Accessed 20 Oct 2020.
Martinez-Martin P, Rodriguez-Blazquez C, Forjaz MJ, Chaudhuri KR. Guide to assessment scales in Parkinson’s Disease. 1st ed. Tarporley: Springer; 2014.
Doty RL. Olfaction in Parkinson’s disease and related disorders. Neurobiol Dis. 2012;46:527–52.
Boeve BF. REM sleep behavior disorder. Ann N Y Acad Sci. 2010;1184:15–54.
Maggi G, Vitale C, Cerciello F, Santangelo G. Sleep and wakefulness disturbances in Parkinson’s disease: a meta-analysis on prevalence and clinical aspects of REM sleep behavior disorder, excessive daytime sleepiness and insomnia. Sleep Med Rev. 2023;68:101759. https://doi.org/10.1016/j.smrv.2023.101759.
Washburn RA, McAuley E, Katula J, Mihalko SL, Boileau RA. The physical activity scale for the elderly (PASE): evidence for validity. J Clin Epidemiol. 1999;52:643–51.
Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14:540–5.
Baidyanath. Ayurvedic Sar-Sangrah. Allahabad: Kitab Mahal; 2017.
Sharma H, Clark C. Ayurvedic Healing: Contemporary Maharishi Ayurveda Medicine and Science. Second. Philadelphia: Singing Dragon; 2012.
Srikanth N, Lavekar GS, Padhi MM, Bandi V. Ayurvedic Management of Select Geriatric Disease Conditions,(WHO India Office Collaborative project on Development of Treatment Protocols and costing guidelines for Geriatric Disorders). First. New Delhi: Central Council for Research in Ayurveda and Siddha, Department of Ayush, Ministry of Health & Family Welfare, Govt. of India; 2011.
Sharma N. Ayurvedic Treatment for Parkinson. https://cureparkinsonsnaturally.com. Accessed 21 Sep 2021.
Smith A. Ayurvedic medicine for westerners: application of ayurvedic treatments throughout life. California: Createspace Independent Pub; 2016.
Yuen C-S, Chua K-K, Lau W-H, Zhuang Z-Y, Chow H-Y, Li M. The effect of conduction exercise and self-acupressure in treatment of Parkinson’s disease: a pilot study. Evid Based Complement Altern Med. 2020;2020:1–9.
Pontone GM, McDaniels B, Keener AM, Subramanian I. A wellness prescription for Parkinson’s: mid to late-stage disease. Am J Geriatr Psychiatry. 2023;31:737–47.
Biswas S, Bagchi A. Study of the effects of nicotine and caffeine for the treatment of Parkinson’s disease. Appl Biochem Biotechnol. 2023;195:639–54.
Rider JV, Longhurst JK, Lekhak N, Navalta JW, Young DL, Landers MR. Psychological factors associated with fear of falling avoidance behavior in Parkinson’s disease: the role of depression, anxiety, and catastrophizing. J Geriatr Psychiatry Neurol. 2023;36:215–24.
Vann-Ward T, Morse JM, Charmaz K. Preserving self: theorizing the social and psychological processes of living with Parkinson disease. Qual Health Res. 2017;27:964–82.
Latella D, Maresca G, Formica C, Sorbera C, Bringandì A, Di Lorenzo G, et al. The role of telemedicine in the treatment of cognitive and psychological disorders in Parkinson’s disease: an overview. Brain Sci. 2023;13(3):499. https://doi.org/10.3390/brainsci13030499.
EkmekyaparFırat Y, Turgay T, Soğan SS, Günel KP. Effects of LSVT-BIG via telerehabilitation on non-motor and motor symptoms and quality of life in Parkinson’s disease. Acta Neurol Belg. 2023;123:207–14.
Mohseni Z, Mohamadi R, Habibi SAH, Saffarian A, Abolghasemi J. Voice improvement following conventional speech therapy combined with singing intervention in people with Parkinson’s disease: a three-arm randomised controlled trial. Int J Lang Commun Disord. 2023;58:1752–67.
Talebi AH, Ypinga JHL, De Vries NM, Nonnekes J, Munneke M, Bloem BR, et al. Specialized versus generic allied health therapy and the risk of Parkinson’s disease complications. Mov Disord. 2023;38:223–31.
Hoseinipalangi Z, Kan FP, Hosseinifard H, Doustmehraban M, Masoumi M, Rafiei S, et al. Systematic review and meta-analysis of the quality-of-life of patients with Parkinson’s disease. East Mediterr Health J. 2023;29:63–70.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
SCD conceptualized the work and provided the critical revision of the article from the first draft to the final one. RI analyzed and interpreted data, and drafted the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Due to the lack of a sufficient amount of patients and their data, we are bound to analyse third-party data, available from the Parkinson’s Progression Markers Initiative (PPMI) during the current study. Thus, the present research work in the manuscript is not carried out practically on our side and we only used the values reported in the data set. Hence, this declaration is not applicable to the current work.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Indu, R., Dimri, S.C. Customized treatment for Parkinson’s disease: extending lifespan and improving symptoms. Egypt J Neurol Psychiatry Neurosurg 60, 71 (2024). https://doi.org/10.1186/s41983-024-00844-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-024-00844-6