
Abstract
Background
Body-weight-supported treadmill training (BWSTT) is a treatment method to help patients with incomplete spinal cord injuries to restore the capability to walk again.
Objective
This study aimed to assess the effects of different percentages of body-weight-support locomotor training on the enhancement of gait for persons with incomplete spinal cord injuries.
Subjects and methods
Twenty male paraplegic persons, with the statistical parameters [mean ± SD] age 32.53 ± 1.793 years, height 175.71 ± 1.658 cm, weight 71.59 ± 2.442 kg, and body mass index 23.18 ± 0.828 kg/m2) were picked by convenience sampling. Ten patients were randomly allocated to the body-weight treadmill training 30% group (Group A); and ten patients to the body-weight treadmill training 40% group (Group B). The two groups were exercised for 1h every set, at two sets weekly for 1.5 months. Body-weight-supported treadmill training was divided into a 15-min warm-up on a stationary bicycle, 45-min body-weight-supported treadmill training with 30 and 40% body weight and finally, a 10-min cool down as we started loading with 10% of body weight of each patient until reach 30% or 40% according to his group.
Results
The resultant data revealed that there are significant distinctions between the body-weight treadmill training 30% and the with body-weight treadmill training 40% groups in regards to alterations in the walking speed, step length, and stride length (p < 0.001), cadence (p = 0.009).
Conclusion
Body-weight-supported treadmill training 40% in comparison with body-weight-supported treadmill training 30% can enhance both the quantity and quality of gait in paraplegic patients (ASIA B, C, and D classification).
Similar content being viewed by others


Introduction
Spinal cord trauma is a catastrophic problem with significant influence on an individual’s quality of life. Trauma to the spinal cord can be the cause of paraparesis or paraplegia and of hypothesia of the body below the level of injury. Incomplete or complete paralysis of the lower limbs makes walking challenging or even difficult and also no everyday activity can be taken for granted. The walking speed in incomplete spinal cord injury (SCI) patients varies from “unable to walk” in severe conditions to “regular walking speed” in the least severe conditions. So, one of among the key goals for subjects with SCI is enhancement of locomotor function [1]. A typical emphasis throughout rehabilitation after SCI is on promoting changes in functional walking capability. Fast and efficient enhancement of gait function can improve a patient’s independence, life satisfaction and subsequent reintegration into society as a fully participating member. Body-weight-support treadmill training has actually been considered a main rehabilitative approach for enhancing locomotion in patients with incomplete SCI [2] . Body-weight-support gait training can begin prior to participants being able to fully bear weight, before developing appropriate motor control, and as well as with better safety and less fear of falling. One of the body-weight-support strategies is body-weight-support treadmill training. A significant problem of traditional body-weight-support treadmill training is the effort needed by therapists to direct the movements of a patient’s legs. Therefore, robotic-assisted tools have been established over recent years to provide assistance and symmetrical walking in the gait-training process [3]. Subsequently, this randomized controlled trial was intended to evaluate the impacts of various percentages of body-weight-support locomotor training on the enhancement in gait for individuals with traumatic motor-incomplete SCIs.
Patients and methods
Study design
The study was designed as a quasi-experiment by using the two-group pre-test, post-test design between June 2017 and November 2018. The study was approved by the official Ethical Committee at the Faulty of Physical Therapy, Cairo University (No: P.T.REC/012/00916) and followed the Guidelines of the Declaration of Helsinki on the conduct of human research.
Participants and randomization
Twenty male participants with traumatic motor-incomplete SCI of different ages were selected. The participants were referred from a neurologist with a diagnosis of traumatic incomplete spinal cord lesion. The participants were assigned randomly into two groups (A and B). Each group consists of ten patients. Randomization was performed by a blinded and an independent research assistant using computer-generated randomization cards saved in sealed envelopes. All subjects in both groups read and signed a written informed consent according to the guidelines established. Group A received a program of stepping on a treadmill with body-weight support (BWS) equal to 30% and Group B received a program of stepping on a treadmill with BWS of 40%.
This study was conducted on the patients with persistent spinal cord trauma of not less than 1 year preceding the beginning of their participation with an age range from 18 to 40 years. The participants had spinal cord damage at T9–T12 with an AIS (American Spinal Injury Association score) of B (preservation of sensory function not motor function below the neurologic level), C (preservation of motor function below the neurologic level and more than half the key muscles below the neurologic level have less than grade fair) or D (motor function is preserved below the neurologic level and more than half of the key muscles below the neurologic level have a muscle grade of fair or more strength). All the patients had the capacity to make no less than one stride with one leg and to rise up from sitting to remaining with, at most, moderate help (half exertion) of one other individual and consented to keep up the present daily schedule of drugs and activity levels while training.
All the patients included in the both groups were subjected to a full detailed history and a full clinical examination for exclusion of the following: patients with an AIS score of A which indicates complete SCI, significant cardio-respiratory/metabolic disorder or other neurologic or orthopedic damage that may restrain exercise participation or weaken the locomotion. The patients with history of peripheral neuropathy, neoplasia, degenerative myelopathy and congenital spinal cord anomalies or those with a history of botulinum toxin treatment to the lower limbs < 6 months before enrollment or size confinements for the harness/counterweight system were also excluded from the study.
Assessment procedures
All the patients in the both groups underwent these testing procedures prior to and following the training while allowing the patients to self-select their preferred speed of walking. These are the most accurate reflection of individuals’ actual everyday performance. All patients performed a test battery containing a long-bout (2-min) walking test and a short-bout (6 m) walking test. These two tests were performed within the same week. The BWS used for each group of patients was extracted using a ground reaction force equation from force platform (load-cells) for continual measurement of BWS and regulation of the amount of weight exerted on the patient’s legs.
Outcome measures
These following outcome parameters were assessed using the force platform or video camera optional after ending of the training sessions including walking speed, step length, stride length, cadence, and step width.
General training methods
All the subjects in both groups were educated about the training methods before starting the sessions. The locomotor training gave tactile prompts and phasic data related to ambulation. These prompts are basic to initiate stepping in humans after a SCI:
-
1)
Stepping speeds roughly of typical walking speeds (0.75–1.25 m/s)
-
2)
Maximum reasonable load on stance limb
-
3)
Upright with extended trunk and head. Approximation of normal hip, knee, and ankle kinematics for walking
-
4)
Synchronize the incidence of the hip extension and unload of the limb with synchronous loading of the contralateral limb
-
5)
Avoid upper limb weight-bearing and encourage reciprocal arm swing
-
6)
Facilitate symmetrical interlimb coordination
-
7)
Reduced sensory stimulation may strife with tactile data correlated to ambulation [2].
The subjects in both groups were allocated an hour of rehabilitation for each exercising day, with installation and bring down occupying a normal of 10 to 15 min of this designated duration. The patients were expected to manage 2 days per week for about a 1.5 months [4] .
Subjects were permitted to utilize the handrails for equilibrium as required. All patients appointed to the treadmill-based rehabilitation clusters were asked to walk at their greatest conceivable velocity.
Treatment methods
Toward the beginning of every set, velocity was increased to medium at which the stepping level started to debase. At that point, speed was decreased to the medium at which the step level is satisfactory and the patient was permitted to walk at this velocity. Following 1 to 2 min at this velocity, the patient was tested through increasing the treadmill velocity increments by 0.32 km/h (0.2 miles/h). When the patient had finished ten paces at this maximum velocity, the velocity was returned to the earlier medium level. When the patient recuperated from the quicker session, the velocity again was increased until the patient could finish 20 paces at the quicker velocity. This arrangement proceeded until the patient was comfortable with the recent increase to a greater velocity. The velocity was increased as such until the point that a speed was reached at which other increments were related with a debasement of pace level.
Group A (step training on a treadmill with BWS rise to 30%):
Patients in the treadmill cluster were given help with pacing depend on the rules prescribed by Behrman and Harkema [6]. Actually, that a subject could not freely adjust or keep up their complete weight of body support during stepping and achieving proper leg kinematics, a weight of body load (BWS = 30%) was utilized with an end goal to give a protected and viable condition for ambulation. A medical harness worn by the patient and associated with an overhead-motorized load over the treadmill supplied the support. The quality of the weight load was acclimatized to expand dual leg support with no knee clasping in the stance. On the off-chance that the patient, during step rehabilitation with our modality, might not produce the proper leg and torso kinematics related to ambulation, hand help was given. Flexible lateral backings connected corner to corner to the patient and to the lateral bars for equilibrium were vital but still permitted upper limb swing. Each patient was urged to swing their upper limb equally with their legs [5].
To start ambulating on the treadmill, the patients remain with their legs in a site reenacting a stride, with one leg in extension close to the mid-stance phase of the step cycle and loading most weight. As the velocity of the treadmill increments plus conveys the leg behind to a place of final stance, the patient moves their weight along the side and in front to the contralateral lower limb because it achieved the first contact. Along these lines, the weight will be expected to rapidly exchange to the front leg, and the behind leg can then start to swing [6] .
Position of the leg on the treadmill was observed and helped if important. Proper imitation of foot motion via all phases of walking was cardinal in eliciting stepping on the treadmill. An ideal stepping design is to be accomplished when it is spatially and temporally planned and most resemble normal walking. The duration of step training sessions was controlled by (1) patient asthenia, (2) joint kinematics support lined up with ambulation, and (3) appropriate weight shift and leg supporting patterns through the feet.
Group B (step training on a treadmill with BWS squares of 40%):
the same procedures were used with Group A of participants were of Group B with the difference that the (BWS = 40%).
Statistical analysis
Information was investigated utilizing IBM Statistical Package for the Social Sciences (SPSS) Advanced Statistics version 22.0 (SPSS Inc., Chicago, IL, USA). All values are displayed as mean ± standard deviation (SD). All evaluation factors were examined for normality of distribution (Shapiro-Wilks test). An independent t test was utilized to contrast the measure of variations in the BWSTT 30% and BWSTT 40% groups following 1.5 months. A p value of less than 0.05 was considered significant [7].
Results
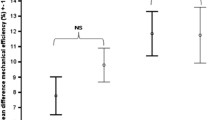
The results were based on the observations of the patients with incomplete SCI in Group A and Group B. Table 1 presents the results after 6 weeks of body-weight-supported treadmill training (BWSTT) in line with the two unique protocols (30% versus 40% of BWS). The resultant data revealed that there were highly significant distinctions among the two groups regarding the changes of walking speed (23.84% vs. 89.36%, respectively, p = 0.001) after 6 weeks of treatment. The resultant data declared that there were significant distinctions among the two groups with respect to alterations of step length (0.89% vs. 17.23%, p = 0.001). A comparison of the alterations in the results recommended that there was better enhancement in stride length (13.66% vs. 51.81%, p = 0.001) and no significant difference in step width between the two groups. Finally, there is significant difference in cadence results (4.69% vs. 16.07%, p = 0.009).
Discussion
BWSTT conditions are currently established by physiotherapists based on what looks right and allows the subjects be involved in the exercises. This kind of subjective determination leads to the use of a variety of treadmill speeds and levels of BWS during the intervention for persons with SCI. The amount of BWS examined in this study falls within the range of conditions used at rehabilitation centers across the country. The strength of BWSTT therapy for SCI, its capability to provide the patient with the forces and motions associated with walking. This study aimed to determine how kinematic and temporal gait patterns are affected by BWS. The results of this study can assist therapists to make more enlightened decisions think about the treadmill velocity and amounts of body weight load during BWSTT for SCIs patients.
We inspected the two various types of body-weight-load treadmill training (30% in comparison with 40%) on gait work of persons with paraplegia. This examination is the prime way of observing the after effects of 6 weeks of body-weight-support treadmill training either with 30% or 40% on gait functions of subjects with incomplete SCI. There are many discharged distributed examinations and audits in the literature portraying the consequence of BWSTT on individuals with different types of SCI contrasting with customary exercise training. Utilizing customary BWSTT has been illustrated to recuperate the capability of walking following SCI [8]. A few examinations likewise uncovered that BWSTT can be an approach that will not just enhance the amount and nature of walking but can likewise cause incremental musculoskeletal changes; for example, bone and bulk, and also modify osteoporosis [9, 10]. Doubtlessly, BWSTT can trigger and prepare central pattern generators (CPGs) within the spinal cord [11] and be mindful to haveing a rhythmic, alternating hind-limb stepping pattern. CPGs can stimulate the afferents appropriately according to the external needs, as there is a lack of utilization of afferent inputs after SCI. Several researches have stated the beneficial effects of BWSTT on the function of incomplete SCI as it might help in recovering mobility function with locomotor training [12].
The essential finding of the current work was that 6 weeks of directed BWSTT created critical restorative outcomes on quality and speed of walking. The outcomes strengthened the theory of our present examination that BWSTT would lead to an enhanced recovery. It was noticeable that no research has contrasted these impacts previously in the literature. The momentum discoveries appear to be unfaltering with other studies, which discovered that BWSTT was desirable over other training cures [13].
The walking training permits people with SCI and independently employed gait capability to attempt gait training. Besides, Hicks and colleagues (2005) showed that the Laufband fix is further developed than customary recovery programs of gait without assistance from others [14]. Moreover, Hicks and colleagues (2005) affirmed that BWSTT is a powerful treatment to recoup walking capability and the vast majority of these enhancements held for around 8 months following training [15]. Different examinations likewise recommended that BWSTT is a robust treatment to recoup gait capability in clients with SCI [16, 17]. Additionally, Behrman and Harkema (2000) discovered that weight-support training on SCI (ASIA C, D) has added to enhancement in gait acceleration [18]. In previous research, Protas and colleagues (2001) mentioned that loaded-machine gait rehabilitation upgraded walking in persons with incomplete SCI. The use of 40% of weight support was fortified in this present research [19].
Field-Fote and colleagues (2005) demonstrated that ambulation reclamation capacity would rely upon training strategy. They found that persons with SCI profited the most from locomotor training [20]. Contrasting BWSTT with a physical therapy program, Lucareli and colleagues (2011) pronounced that body-loaded exercising was far better than a customary physical therapy program on boosting the quality and amount of walking among individuals with incomplete SCI [21]. Even though the advantages were comparable, the members experienced distinct degrees of damage (ASIA B, C).
The outcomes in this study show that ambulation-acceleration decrement within BWSTT was better than a land-based remedy after 3 months of exercising. A couple of these dissimilarities are foreseen to affect duration and affected level of subjects [22]. Likewise, in another examination, Dobkin and colleagues (2007) delineated that consequent 3 months of BWSTT in comparison to land-based rehabilitation, there are the same consequences concerning gait speed and LEMS evaluations [23]. Besides, Field-Fote and Roach (2011) proved that there is similarity among body-support locomotion and landed treatment management seeking after 12 weeks of training in subjects with SCI (ASIA C, D) [24]. The disparity in consequences might be relied upon to produce refinements in treatment quality, quantity of sets per week, patient age, and segmental damage.
The ambulation approach with a weight bolster expanded walking steadiness by creating an increase in step length, bringing down the duration stance phase and expanding the swing. This approach likewise progressed after being executed by a person by means of expanded speed, cadence, distance covered and duration of the gait cycle. These outcomes demonstrate similarity to those found by different specialists who affirmed that there have been enhancements in autonomy and walking ability, in addition to boosts in gait speed [25].
Expanded hip extension enhances the step length; however different variables could likewise meddle: more noteworthy extension and consequent decrease measure of knee flexion at initial contact, enhancement of hip flexion, increased pelvic rotation, and enhancement of muscle strength and damping of spasticity [26]. In spite of the way that all the angular parameters may meddle with step length, absolutely that the restoration with weight load rise the sufficiency of hip extension and rise the step length.
This study found that increasing levels of BWS change the kinematics and temporal patterns significantly. It is important to ascertain that differences in lower-extremity kinematics and temporal patterns do exist with changing treadmill speed and BWS.
The change observed in study Group B may be due to stepping practice via treadmill practicing which enforces and stabilizes the neural network affected in producing this pattern and increases the specific postural control mechanism needed to maintain the balance when transferring the weight from one leg to the other. So, the treadmill, as an example of stepping practice, facilitates and strengthens the neural connections that arise from the coupling of the multimodal sensory input generated [28].
Established from the results of this study, the influence of treadmill speed and BWS does not seem to have the same impact on temporal patterns. Further work is needed to determine the underlying biomechanical mechanisms in charge of changing joint kinematics. This study and the future work to be performed should shed light regarding which training parameters could provide patients with kinematics and kinetics that will be beneficial to successful recovery of walking over ground.
Limitations
The relatively small sample size is the major limitation in our study that has to be recognized. The inability of the researchers to be blinded to the study strategies in the two study groups could have been an additional limitation of the present study.
Conclusion
In conclusion, body-weight-supported treadmill training 40% in comparison with body-weight-supported treadmill training 30% can enhance the quantity and quality of gait in paraplegic patients .
Abbreviations
- ASIA:
-
American Spinal Injury Association
- BWS:
-
Body-weight support
- BWST:
-
Body-weight support
- BWSTT:
-
Body-weight-support treadmill training
- SCI:
-
Spinal cord injury
- SPSS:
-
Statistical Package for the Social Sciences
References
Kirshblum SC, Priebe MM, Ho CH, Scelza WM, Chiodo AE, Wuermser LA. Spinal cord injury medicine. 3. Rehabilitation phase after acute spinal cord injury. Arch Phys Med Rehabil. 2007;88(3 (1)):62–70.
Harkema S. Plasticity of inter neuronal networks of the functionally isolated human spinal cord. Brain Res Rev. 2008;57(1):255–64.
Vieira R, Oliveira R, Barros C, Caixeta L, Machado S. Effects of body weight-support treadmill training in incomplete spinal cord injury: a critical review. Am Med J. 2012;3:203–9.
Hornby TG, Zemon DH, Campbell D. Robotic-assisted body-weight-supported treadmill training in individuals following motor incomplete spinal cord injury. Phys Ther. 2005;85(1):52–66.
Behrman A, Harkema S. Physical rehabilitation as an agent for recovery after spinal cord injury. Phys Med Rehabil Clin N Am. 2007;18:183–202.
Field-Fote EC. Combined use of body weight support, functional electric stimulation, and treadmill training to improve walking ability in individuals with chronic incomplete spinal cord injury. Arch Phys Med Rehabil. 2001;82:818–24.
Edelle C, Field-Fote P, Stephen D, Lindley M, et al. Locomotor training approaches for individuals with spinal cord injury: preliminary report of walking-related outcomes. J Neurol Phys Ther. 2005;29(3):127–37.
Coupaud S, Jack LP, Hunt KJ, Allan DB. Muscle and bone adaptations after treadmill training in incomplete spinal cord injury: a case study using peripheral quantitative computed tomography. J Musculoskelet Neuronal Interact. 2009;9(4):288–97.
Carvalho DCL, Garlipp CR, Bottini PV, Afaz SH, Moda MA, Cliquet Jr A. Effect of treadmill gait on bone markers and bone mineral density of quadriplegic subjects. Braz J Med Biol Res. 2006;39(10):1357–63.
DePaul V, Wishart L, Richardson J, Lee T, Thabane L. Varied over ground walking-task practice versus body-weight supported treadmill training in ambulatory adults within one year of stroke: a randomized controlled trial protocol. BMC Neurol. 2011;11(1):129.
Singh A, Balasubramanian S, Murray M, Lemay M, Houle J. Role of spared pathways in locomotor recovery after bodyweight-supported treadmill training in contused rats. J Neurotrauma. 2011;28(12):2405–16.
Dietz V. Body weight supported gait training: from laboratory to clinical setting. Brain Research Bulletin. 2009;78(1):I–VI.
Wernig A, Müller S, Nanassy A, Cagol E. Laufband therapy based on “rules of spinal locomotion” is effective in spinal cord injured persons. Eur J Neurosci. 1995;7(4):823–9.
Hicks A, Adams M, Ginis KM, Giangregorio L, Latimer A, Phillips S, et al. Long-term body-weight-supported treadmill training and subsequent follow-up in persons with chronic SCI: effects on functional walking ability and measures of subjective well-being. Spinal Cord. 2005;43(5):291–8.
Wernig A, Nanassy A, Müller S. Maintenance of locomotor abilities following Laufband (treadmill) therapy in para- and tetraplegic persons: follow-up studies. Spinal Cord. 1998;36(11):744–9.
Nymark J, DeForge D, Barbeau H, Badour M, Bercovitch S, Tomas J, et al. Body weight support treadmill gait training in the subacute recovery phase of incomplete spinal cord injury. Neurorehabil Neural Repair. 1998;12(3):119–36.
Behrman AL, Harkema SJ. Locomotor training after human spinal cord injury: a series of case studies. Phys Ther. 2000;80(7):688–700.
Protas EJ, Holmes S, Qureshy H, Johnson A, Lee D, Sherwood AM. Supported treadmill ambulation training after spinal cord injury: a pilot study. Arch Phys Med Rehabil. 2001;82(6):825–31.
Field-Fote EC, Lindley SD, Sherman AL. Locomotor training approaches for individuals with spinal cord injury: a preliminary report of walking-related outcomes. J Neurol Phys Ther. 2005;29(3):127–37.
Lucareli P, Lima M, Lima F, de Almeida J, Brech G, Greve JDA. Gait analysis following treadmill training with body weight support versus conventional physical therapy: a prospective randomized controlled single blind study. Spinal Cord. 2011;49(9):1001–7.
Dobkin B, Apple D, Barbeau H, Basso M, Behrman A, Deforge D, et al. Weight-supported treadmill vs over-ground training for walking after acute incomplete SCI. Neurology. 2006;66(4):484–93.
Dobkin B, Barbeau H, Deforge D, Ditunno J, Elashoff R, Apple D, et al. The evolution of walking-related outcomes over the first 12 weeks of rehabilitation for incomplete traumatic spinal cord injury: the multicenter randomized Spinal Cord Injury Locomotor Trial. Neurorehabil Neural Repair. 2007;21(1):25–35.
Field-Fote EC, Roach KE. Influence of a locomotor training approach on walking speed and distance in people with chronic spinal cord injury: a randomized clinical trial. Phys Ther. 2011;91(1):48–60.
Hossain MA, Hossain KMA, Hossain M, Rahaman I, Taoheed F, Hoque KI, et al. Effectiveness of gait training supported by overhead harness in patients with spinal cord injury (SCI) at rehabilitation centre in Bangladesh. Int J Neurorehabil Eng. 2018;5(5):1–3.
Ditunno J, Scivoletto G. Clinical relevance of gait research applied to clinical trials in spinal cord injury. Brain Res Bull. 2009;78:35–42.
Harvey LA. Physiotherapy rehabilitation for people with spinal cord injuries. J Phys. 2016;62(1):4–11.
Acknowledgements
Not applicable.
Funding
No funding resources were declared for this research.
Availability of data and materials
The dataset cannot be publicly available due to institutional rules.
Author information
Authors and Affiliations
Contributions
MMS: was responsible for conception of the work, analyzing, interpreting the data and approval of the final reversion of the work. LID: collection of data, communicating with the journal during the manuscript submission, peer review, and publication process. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the official Ethical Committee at the Faulty of Physical Therapy, Cairo University (No: P.T.REC/012/00916) on Sunday 4/12/2016 and followed the Guidelines of Declaration of Helsinki on the conduct of human research. Written informed consent was obtained from all the patients and control volunteers before study initiation.
Consent for publication
Not applicable.
Competing interests
The authors have no conflicts of financial interest to declare in relation to this study. We confirm that we have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
El Semary, M.M., Daker, L.I. Influence of percentage of body-weight support on gait in patients with traumatic incomplete spinal cord injury. Egypt J Neurol Psychiatry Neurosurg 55, 40 (2019). https://doi.org/10.1186/s41983-019-0076-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41983-019-0076-9