
Abstract
Background
Patients with rheumatoid arthritis (RA) have difficulties maintaining employment due to the impact of the disease on their work ability. This review aims to investigate the employment rates at different stages of disease and to identify predictors of employment among individuals with RA.
Methods
The study was carried out according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines focusing on studies reporting employment rate in adults with diagnosed RA. The literature review included cross-sectional and cohort studies published in the English language between January 1966 and January 2023 in the PubMed, Embase and Cochrane Library databases. Data encompassing employment rates, study demographics (age, gender, educational level), disease-related parameters (disease activity, disease duration, treatment), occupational factors, and comorbidities were extracted. Quality assessment was performed employing Newcastle–Ottawa Scale. Meta-analysis was conducted to ascertain predictors for employment with odds ratios and confidence intervals, and test for heterogeneity, using chi-square and I2-statistics were calculated. This review was registered with PROSPERO (CRD42020189057).
Results
Ninety-one studies, comprising of a total of 101,831 participants, were included in the analyses. The mean age of participants was 51 years and 75.9% were women. Disease duration varied between less than one year to more than 18 years on average. Employment rates were 78.8% (weighted mean, range 45.4–100) at disease onset; 47.0% (range 18.5–100) at study entry, and 40.0% (range 4–88.2) at follow-up. Employment rates showed limited variations across continents and over time. Predictors for sustained employment included younger age, male gender, higher education, low disease activity, shorter disease duration, absence of medical treatment, and the absence of comorbidities.
Notably, only some of the studies in this review met the requirements for high quality studies. Both older and newer studies had methodological deficiencies in the study design, analysis, and results reporting.
Conclusions
The findings in this review highlight the prevalence of low employment rates among patients with RA, which increases with prolonged disease duration and higher disease activity. A comprehensive approach combining clinical and social interventions is imperative, particularly in early stages of the disease, to facilitate sustained employment among this patient cohort.
Similar content being viewed by others


Background
Rheumatoid arthritis (RA) is a chronic, inflammatory joint disease that can lead to joint destruction. RA particularly attacks peripheral joints and joint tissue, gradually resulting in bone erosion, destruction of cartilage, and, ultimately, loss of joint integrity. The prevalence of RA varies globally, ranging from 0.1- 2.0% of the population worldwide [1, 2]. RA significantly reduces functional capacity, quality of life, and results in an increase in sick leave, unemployment, and early retirement [3,4,5]. The loss of productivity due to RA is substantial [2, 5,6,7]. A 2015 American study estimated the cost of over $250 million annually from RA-related absenteeism in United States alone [8].
Research has highlighted the importance of maintaining a connection to the labour market [3, 9], Even a short cessation from work entails a pronounced risk of enduring work exclusion [10]. In Denmark merely 55% on sick leave for 13 weeks succeeded in re-joining the workforce within one year. Among those on sick leave for 26 weeks, only 40% returned to work within the same timeframe [11]. Sustained employment is associated with an improved health-related quality of life [12, 13]. Early and aggressive treatment of RA is crucial for importance in achieving remission and a favourable prognosis reducing the impact of the disease [2, 14,15,16]. Therefore, initiating treatment in a timely manner and supporting patients with RA in maintaining their jobs with inclusive and flexible workplaces if needed is critical [3, 17].
International studies have indicated, that many patients with RA are not employed [18]. In 2020, the average employment rate across Organization for Economic Co-operation and Development (OECD) countries was 69% in the general population (15 to 64 years of age), exhibiting variations among countries, ranging from 46–47% in South Africa and India to 85% in Iceland [19]. Employment rates were lower for individuals with educational levels below upper secondary level compared to those with upper secondary level or higher education [19]. For individuals suffering with chronic diseases, the employment rates tend to be lower. Prognostic determinants for employment in the context of other chronic diseases encompasses the disease’s severity, employment status prior to getting a chronic disease, and baseline educational level [20,21,22]. These somatic and social factors may similarly influence employment status of patients with RA. Several factors, including the type of job (especially physically demanding occupations), support from employers and co-workers, social safety net, and disease factors such as duration and severity, could have an impact on whether patients with RA are employed [17, 23, 24]. Over the years, politicians and social welfare systems have tried to improve the employment rates for patients with chronic diseases. In some countries, rehabilitation clinics have been instrumental in supporting patients to remain in paid work. Healthcare professionals who care for patients with RA occupy a pivotal role in preventing work-related disability and support the patients to remain in work. Consequently, knowledge of the factors that contribute to retention of patients with RA at work is imperative [17, 25].
The aim of this study is therefore to conduct a systematic review, with a primary focus on examining employment rates among patients with RA at the onset of the disease, at study entry, and throughout follow-up. Additionally, this study intends to identify predictors of employment. The predefined predictors, informed by the author’s comprehensive understanding of the field and specific to RA, encompass socioeconomic factors such as age, gender, level of education, employment status prior to the disease, disease stage and duration, treatment modalities, and comorbidities, including depression, which are relevant both to RA and other chronic conditions [26].
Methods
Protocol
This systematic review was carried out according to Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) for studies that included employment rate in patients with rheumatoid arthritis [27]. PROSPERO registration number: CRD42020189057.
Selection criteria and search strategies
A comprehensive literature search was conducted, covering the period from January 1966 to January 2023 across the PubMed, Embase, and Cochrane Library databases using the following search terms: (Rheumatoid arthritis OR RA) AND (employment OR return to work). Only studies featuring a minimum cohort size of thirty patients and articles in the English language were deemed eligible for inclusion.
The initial screening of articles was based on the titles and abstracts. Studies comprising a working-age population, with current or former employment status, and with no limitations to gender, demographics, or ethnicity were included in this review. Articles addressing topics of employment, work ability or disability, return to work or disability pension were encompassed within the scope of this review. Full-time and part-time employment, but not ‘working as housewives’ was included in this review’s definition of employment. Studies involving other inflammatory diseases than RA were excluded. Reference lists in the selected articles were reviewed, and more articles were included if relevant. A review of the reference lists in the initially selected articles was conducted, with additional articles incorporated if they proved relevant to the research objectives. The eligible study designs encompassed cohort studies, case–control studies, and cross-sectional studies. All other study designs, including reviews, case series/case reports, in vitro studies, qualitative studies, and studies based on health economics were systematically excluded from the review.
Data extraction, quality assessment and risk-of-bias
The data extraction from the selected articles included author names, year of publication, study design, date for data collection, employment rate, study population, age, gender, educational level, ethnicity, disease duration, and pharmacological treatment. To ensure comprehensive evaluation of study quality and potential bias, quality assessment was independently assessed by two reviewers (LK and KB) using the Newcastle–Ottawa Scale (NOS) for cross-sectional and cohort studies [28]. Any disparities in the assessment were resolved by discussion until consensus was reached. For cross-sectional studies the quality assessment included: 1) Selection (maximum 5 points): representativeness of the sample, sample size, non-respondents, ascertainment of the risk factor; 2) Comparability (maximum 2 points); study controls for the most important, and any additional factor; 3) Outcome (maximum 3 points): assessment of outcome, and statistical testing. For cohort studies the assessment included: 1) Selection (maximum 4 points): representativeness of the exposed cohort, selection of the non-exposed cohort, ascertainment of exposure, demonstration that the outcome of interest was not present at start of study; 2) Comparability (maximum 2 points): comparability of cohorts on the basis of the design or analysis; 3) Outcome (maximum 3 points): assessment of outcome, was the follow-up long enough for outcomes to occur, and adequacy of follow up of cohorts. The rating scale was based on 9–10 items dividing the studies into high (7–9/10), moderate (4–6) or low (0–3) quality. A low NOS score (range 0–3) indicated a high risk of bias, and a high NOS score (range 7–9/10) indicated a lower risk of bias.
Analytical approach
For outcomes reported in numerical values or percentages, the odds ratio along with their 95% confidence intervals (CI) were calculated, whenever feasible. Weighted means were calculated, and comparisons between these were conducted using t-test for unpaired data. Furthermore, meta-analysis concerning the pre-determined and potentially pivotal predictors for employment status, both at disease onset, study entry, and follow-up was undertaken. The predictors included age, gender, ethnicity, level of education, duration of disease, treatment, and the presence of comorbities, contingent upon the availability of the adequate data. Additionally, attempts have been made to find information regarding on job categorizations, disease activity (quantified through DAS28; disease activity score for number of swollen joints), and quality of life (SF-36 scores ranging from 0 (worst) to 100 (best)). Age was defined as (< = 50/ > 50 years), gender (male/female), educational level college education or more/no college education), race (Caucasian/not Caucasian), job type (non-manual/manual), comorbidities (not present/present), MTX ever (no/yes), biological treatment ever (no/yes), prednisolone ever (no/yes), disease duration, HAQ score (from 0–3)), joint pain (VAS from 1–10), and DAS28 score. Age, disease duration, HAQ score, VAS score, SF36 and DAS28 were in the studies reported by mean values and standard deviations (SD). Challenges were encountered during attempts to find data which could be used for analysing predictors of employment status before disease onset, and at follow-up, as well as factors related to treatments beyond MTX, prednisolone, and biological as predictors for being employed after disease onset. Test for heterogeneity was done using Chi-squared statistics and I2, where I2 below 40% might not be important; 30–60% may represent moderate heterogeneity; 50–90% substantial heterogeneity; and 75–100% considerable heterogeneity. Meta-analysis for predictors for employment and odds ratio; confidence intervals; and test for heterogeneity were calculated using the software Review Manager (RevMan, version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
General description of included studies
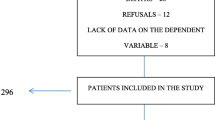
The search yielded a total of 2277 references addressing RA its association with employment. Following the initial title screen, 199 studies were considered relevant for further evaluation. Of those, 91 studies ultimately met the inclusion criteria. Figure 1 shows the results of the systematic search strategy.

Flow chart illustrating the systematic search for studies examining employment outcome in patients with rheumatoid arthritis
Table 1 summarizes the general characteristics of the included studies. The publication year of the included studies ranged from 1971 to 2022. Among the studies, 60 (66%) adopted a cross-sectional research design [13, 18, 29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88, 129] with a total of 41,857 participants analysing data at a specific point in time. Concurrently, 31 studies (34%) adopted a cohort design [89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122, 130] with a total of 59,974 participants. Most of these studies exhibited a small to moderate sample size, with a median of 652 participants. Additionally, single centre studies and studies from high-income countries were predominant. Study details are shown in Table 1.
General description of study participants
On average, patients with RA were 51 years old, with an age range spanning from 42 to 64 years. Furthermore, the female population accounted for 75.9% of the patient cohort, with a range from 41 to 92%. The duration of the disease at study entry exhibited significant variability, ranging from less than one year up to more than 18 years on average.
Employment rate
At disease onset, the employment rate was 78.8% (weighted mean, range 45.4–100), at study entry 47.0% (range 18.5–100), and during the follow-up period 40.0% (range 4–88.2), as shown in Table 2. Notably, a comparative analysis of the employment rates between Europe and North America indicated no substantial difference (p = 0.93). However, the comparison between Europe, North America and ‘other continents’ did yield significant differences (or nearly differences) with p-values of 0.003 and 0.08, respectively.
The employment rate exhibited no change, when comparing studies from the 1980s through to 2022. Specifically, the weighted mean for the years 1981–2000 was 49.2%, aligning closely with the corresponding figures for the years 2001–2010 (49.2%) and 2011–2022 43.6%. These findings were statistically non-significant, with p-values of 0.80 for comparison between year 1981–2000 and 2001–2010; 0.66 for 2001–2010 and 2011–2022, and 0.94 for 1981–2000 and 2011–2022, shown in Figure S1, see Additional file.
Among the studies included in the analysis, nineteen studies included data of employment at follow-up, with durations ranging from 1 to 20 years, Table 2. For instance, Jäntti, 1999 [97] reported an employment rate 69% one year after disease onset, which gradually declined to 50% after 15 years and further to 20% after 20 years. Similarly, Mäkisara, 1982 [63] demonstrated that 60% of the patients were employed 5 years after disease onset, 50% after 10 years, and 33% after 15 years. Nikiphorou, 2012 [101] reported an employment rate of 67% at study entry, which decreased to 43% after 10 years.
In addition, seven studies included data of employment rate among patients comparing different medical treatments [18, 44, 56, 91, 105, 110, 119]. These studies indicated that, on average, 55.0% (weighted mean) of the patients were employed after receiving treatment with MTX, while 42.8% after undergoing treatment with a combination of MTX + Adalimumab (all patients were employed at disease onset in these specific studies).
Predictors for employment
Information of normative comparison data to use for meta-analysis of predictors for employment at study entry was available for age, gender, educational level, race, job type, comorbidities, MTX at any time, biological treatment at any time, prednisolone at any time, disease duration, HAQ score, joint pain (VAS-score), and disease activity (DAS28 score). Predictors for employment at study entry was being younger /age below 50 years, being a male, higher educational level (college or more), non-manual work, having no comorbidities, no medical treatment, short disease duration, and low HAQ score, VAS-score, or DAS28 score. Heterogeneity was small for age, gender, medical treatment, and moderate for educational level, and job type as indicted by the I2 values, Table 3, and shown in detail in Figures S2, S3, S4, S5, S6, S7, S8, S9, S10, S11, S12, S13, S14, S15 and S16, see Additional file.
Assessment of quality of included studies
All studies were subject to rigorous quality assessment. These assessments resulted in categorisation of either medium quality (n = 64; 70%) or high-quality studies (n = 27; 30%), with no studies falling into the low-quality category. The quality assessment is shown in Tables 4 and 5.
Notably, many studies were characterised by several common attributes, including cross-sectional study design, single-centre-settings, relatively small sample sizes, and the reliance on self-reported patient data. When including only the high-quality studies in the analyses, the employment rates at study entry changed from 47% (weighted mean, all studies) to 50% (weighted mean, high quality studies).
Discussion
Key findings
This systematic review has identified a decline in the employment rate among patients with RA, with a notable decrease from disease onset during the study entry to follow-up, where only half of the patients were employed. These findings corroborate earlier research that indicated a substantial decline in employment rates among patients with RA over time. Notably, previous studies have reported that approximately one third of patients with RA stopped working within 2 to 3 years after disease onset, and more than half was unable to work after 10 to 15 years [23, 63, 93, 97, 101]. Only few studies have included data from the general population, comparing the employment rates with the rates for patients with RA [89, 90]. Comparisons with the general population further underscored the challenges faced by RA patients, as their employment rates were consistently lower.
Despite changes in medical treatment, social security systems, and societal norms over the past decades, there was no significant improvement in the employment for patients with RA. This pattern aligns with data from the Global Burden of Disease studies, highlighting the persistent need for novel approaches and dedicated efforts to support patients with RA in sustaining employment [2, 123]. Recent recommendations from EULAR (European Alliance of Associations for Rheumatology) and ACR (American College of Rheumatology) have emphasized the importance of enabling individuals with rheumatic and musculoskeletal diseases to engage in healthy and sustainable work [17, 124, 125].
While different countries possess different social laws and health care systems for supporting patients with chronic diseases, the variations in the weighted mean of employment rates across countries were relatively minor.
In the meta-analysis, one of the strongest predictors for maintaining employment was younger age at disease onset [43, 51, 101, 116]. Verstappen, 2004 found that older patients with RA had an increased risk of becoming work disabled, potentially caused by the cumulative effects of long-standing RA, joint damage, and diminished coping mechanisms, compared to younger patients [23].
More women than men develop RA, however this study showed that a higher proportion of men managed to remain employed compared to women [18, 36, 42, 43, 46, 62, 71, 89, 101, 116]. Previous studies have shown inconsistent results in this regard. Eberhart, 2007 found that a significantly higher number of men with RA worked even though there was no difference in any disease state between the sexes [93]. De Roos,1999 showed that work-disabled women were less likely to be well-educated and more likely to be in a nonprofessional occupation than working women. Interestingly, there was no association of these variables among men. Type of work and disease activity may influence work capacity more in women than in men [46]. Sokka, 2010 demonstrated a lower DAS28 and HAQ-score in men compared to women among the still working patients with RA, which indicated that women continued working at higher disability and disease activity levels compared with men [18].
Disease duration also played a significant role as a predictor of employment outcomes [33, 36, 45, 71, 77, 86, 102, 111]. Longer disease duration correlate with decreased employment likelihood, which could be attributed to older age and increased joint damage and disability in patients with longer-standing RA.
Higher educational levels were associated with a greater possibility of employment [30, 43, 45, 46, 51, 62, 86]. This is probably due to enhanced job opportunities, flexibility, lower physical workload, better insurance coverage, and improved health care for well-educated individuals. This is further supported by the fact that having a manual work was a predictor for not being employed [30, 39, 43,44,45].
Furthermore, health-related quality of life, as measured by SF 36, lower disease activity (DAS28 scores), reduced joint pain (VAS-score), and lower disability (HAQ score) were additionally predictors for being employed [33, 35, 36, 45, 71, 86]. This support the statement that the fewer symptoms from RA, the greater the possibility of being able to work.
The results showed that the presence of comorbidity was a predictor for not being employed, aligning with findings from previous studies that chronic diseases such as cardiovascular disease, lung disease, diabetes, cancer, and depression reduced the chances of being employed [126]. Moreover, the risk of exiting paid work increased with multimorbidity [127].
While limited data were available for assessing the impact of treatment on employment, indications suggested that patients with RA were receiving medical treatments, such as MTX or biological medicine, were more likely to be unemployed. One possible explanation for this phenomenon could be that patients with RA, who were receiving medical treatment, had a more severe and a longer duration of RA compared to those, who had never been on medical treatment. However, the scarcity of relevant studies necessitates caution when drawing definitive conclusions in this regard.
Therefore, the predictors for employment found in this review were being younger, being a male, having higher education, low disease activity, low disease duration, and being without comorbidities. This is supported by previous studies [93, 116]
In summary, this review underscores the importance of managing disease activity, offering early support to patients upon diagnosis, and reducing physically demanding work to maintain employment among patients with RA. Achieving success in this endeavour requires close cooperation among healthcare professionals, rehabilitation institutions, companies, and employers. Furthermore, it is important that these efforts are underpinned by robust social policies that ensure favourable working conditions and provide financial support for individuals with physical disabilities, enabling them to remain active in the labour market.
Strengths and limitations
The strength of this review and meta-analysis lies in the inclusion of a large number of articles originating from various countries. Furthermore, the data showed a consistent employment rate in high quality studies compared to all studies. However, there are some limitations to this review. No librarian was used to define search terms and only three databases were searched. Furthermore, the initial search, selection of articles, data extraction, and analysis was undertaken only by one author, potentially leading to the omission of relevant literature and data. The review also extended back to 1966, with some articles from the 1970s and 1980s included. Given the significant changes in medical treatment, social security systems, and society over the past decades, the generalizability of the findings may be limited.
Moreover, the majority of studies did not include a control group from the general population, which limited the ability to compare employment rates with the general population in the respective countries. Many studies were cross-sectional in design, which limits the evidence of causality between employment rate and having RA. However, the employment rate was approximately the same in high quality studies compared to all studies, which supports an association. A substantial number of studies relied on self-reported employment rates, introducing the potential for recall bias. Additionally, many studies did not account for all relevant risk factors for unemployment failing to control for all relevant confounders.
EULAR have made recommendation for point to consider when designing, analysing, and reporting of studies with work participation as an outcome domain in patients with inflammatory arthritis. These recommendations include study design, study duration, and the choice of work participation outcome domains (e.g., job type, social security system) and measurement instruments, the power to detect meaningful effects, interdependence among different work participation outcome domains (e.g., between absenteeism and presentism), the populations included in the analysis of each work participation outcome domain and relevant characteristics should be described. In longitudinal studies work-status should be regularly assessed and changes reported, and both aggregated results and proportions of predefined meaningful categories should be considered [128]. Only some of the studies in this review met the requirements for high quality studies. In both older and newer studies methodological deficiencies persisted in study design, analysis, and reporting of results, as recommended by EULAR.
Perspectives for future studies
Future research in this area should focus on developing and evaluating new strategies to address the ongoing challenges faced by patients with RA in maintaining employment. Despite many initiatives over the years, there has been no success in increasing employment rates for patients with RA in many countries. Therefore, there is a pressing need for controlled studies that investigated the effectiveness of interventions such as education, social support, and workplace adaptations in improving employment outcomes for these individuals.
Conclusion
This systematic review underscores the low employment rate among patients with RA. Key predictors of sustained employment include being younger, having higher educational level, short disease duration, and lower disease activity, along with fewer comorbidities. Importantly, the review reveals that the employment rate has not changed significantly across different time periods. To support patients with RA in maintaining their employment, a comprehensive approach that combines early clinical treatment with social support is crucial. This approach can play a pivotal role in helping patients with RA stay connected to the labour market.
Availability of data and materials
The datasets used and/or analyzed during the current study are available in the supplementary file.
Abbreviations
- RA:
-
Rheumatoid arthritis
- MTX:
-
Methotrexate
- Yr:
-
Year
- NOS:
-
Newcastle Ottawa Quality Assessment Scale
- SD:
-
Standard deviation
- n.a.:
-
Not analyzed
- n.r.:
-
Not relevant
- yr:
-
Year
- DAS:
-
Disease activity
- HAQ:
-
Health Assessment Questionnaire
- VAS:
-
Visual analog scale for pain
- EULAR:
-
European Alliance of Associations for Rheumatology
- ACR:
-
American College of Rheumatology
References
Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol Int. 2021;41:863–77.
Safiri S, Kolahi AA, Hoy D, Smith E, Bettampadi D, Mansournia MA, et al. Global, regional and national burden of rheumatoid arthritis 1990–2017: a systematic analysis of the Global Burden of Disease study 2017. Ann Rheum Dis. 2019;78:1463–71.
Verstappen SMM. Rheumatoid arthritis and work: The impact of rheumatoid arthritis on absenteeism and presenteeism. Best Pract Res Clin Rheumatol. 2015;29:495–511.
Madsen CMT, Bisgaard SK, Primdahl J, Christensen JR, von Bülow C. A systematic review of job loss prevention interventions for persons with inflammatory arthritis. J Occup Rehabil. 2021;4:866–85.
Kessler RC, Maclean JR, Petukhova M, Sarawate CA, Short L, Li TT, et al. The effects of rheumatoid arthritis on labor force participation, work performance, and healthcare costs in two workplace samples. J Occup Environ Med. 2008;50:88–98.
Filipovic I, Walker D, Forster F, Curry AS. Quantifying the economic burden of productivity loss in rheumatoid arthritis. Rheumatology. 2011;50:1083–90.
Burton W, Morrison A, Maclean R, Ruderman E. Systematic review of studies of productivity loss due to rheumatoid arthritis. Occup Med. 2006;56:18–27.
Gunnarsson C, Chen J, Rizzo JA, Ladapo JA, Naim A, Lofland JH. The employee absenteeism costs of reumatoid arthritis. Evidence from US National Survey Data. J Occup Environ Med. 2015;57:635–42.
van der Noordt M, Ijzelenberg H, Droomers M, Proper KI. Health effects of employment: a systematic review of prospective studies. Occup Environ Health. 2014;71:730–6.
Virtanen M, Kivimäki M, Vahtera J, Elovainio M, Sund R, Virtanen P, et al. Sickness absence as a risk factor for job termination, unemployment, and disability pension among temporary and permanent employees. Occup Environ Med. 2006;63:212–7.
Vilhelmsen J. Længerevarende sygefravær øger risikoen for udstødning [long-term sick-leave increase the risk of job termination]. 2007. https://www.ae.dk/analyse/2007-10-laengerevarende-sygefravaer-oeger-risikoen-for-udstoedning.
Grønning K, Rødevand E, Steinsbekk A. Paid work is associated with improved health-related quality of life in patients with rheumatoid arthritis. Clin Rheumatol. 2010;29:1317–22.
Chorus AMJ, Miedema HS, Boonen A, van der Linden S. Quality of life and work in patients with rheumatoid arthritis and ankylosing spondylitis of working age. Ann Rheum Dis. 2003;62:7.
Ma MHY, Kingsley GH, Scott DL. A systematic comparison of combination DMARD therapy and tumour necrosis inhibitor therapy with methotrexate in patients with early rheumatoid arthritis. Rheumatology (Oxford). 2010;49:91–8.
Vermeer M, Kuper HH, Hoekstra M, Haagsma CJ, Posthumus MD, Brus HL, et al. Implementation of a treat-to-target strategy in very early rheumatoid arthritis. Results of the Dutch arthritis monitoring remission induction cohort study. Arthritis Rheum. 2011;63:2865–72.
Vermeer M, Kuper HH, Bernelot Moens HJ, Drossaers-Bakker KW, van der Bijl AE, van Riel PL, et al. Sustained beneficial effects of a protocolized treat-to-target strategy in very early rheumatoid arthritis: three-year results of the Dutch rheumatoid arthritis monitoring remission induction cohort. Arthritis Care Res. 2013;65:1219–26.
Boonen A, Webers C, Butink M, Barten B, Betteridge N, Black DC, et al. 2021 EULAR points to consider to support people with rheumatic and musculoskeletal diseases to participate in healthy and sustainable paid work. Ann Rheum Dis. 2023;82:57–64.
Sokka T, Kautianen H, Pincus T, Verstappen SMM, Aggarwai A, Alten R, et al. Work disability remains a major problem in rheumatoid arthritis in the 2000s: data from 32 countries in the QUEST-RA study. Arthritis Res Ther. 2010;1(R42):1–10.
OECD. Employment rate (indicator). 2020. https://dataoecd.org/emp/employment-rate.htm. Assessed on 11 May.
Hannerz H, Pedersen BH, Poulsen OM, Humle F, Andersen LL. A nationwide prospective cohort study on return to gainful occupation after stroke in Denmark 1996–2006. BMJ Open. 2011;1:1–5.
Tumin D, Chou H, Hayes D Jr, Tobias JD, Galantowicz M, McConnell PI. Employment after hearth transplantation among adults with congenital heart disease. Congenit Heart Dis. 2017;12:794–9.
Islam T, Dahlui M, Majid HA, Nahar AM, MohdTaib NA, Su TT, MyBCC study group. Factors associated with return to work of breast cancer survivors: a systematic review. BMC Public Health. 2014;14:1–13.
Verstappen SMM, Bijlsma JWJ, Verkleij H, Buskens E, Blaauw AAM, Borg EJ, Jacobs JWG. Overview of work disability in rheumatoid arthritis patients as observed in cross-sectional and longitudinal surveys. Arthritis Rheum. 2004;51:488–97.
Wilkie R, Bjork M, Costa-Black KM, Parker M, Pransky G. Managing work participation for people with rheumatic and musculoskeletal diseases. Best Pract Res. 2020;34:1–16.
Varekamp I, Haafkens JA, Detaille SI, Tak PP, van Dijk FJH. Preventing work disability among employees with rheumatoid arthritis: what medical preofessionals can learn form patients’ perspective. Arthritis Rheum. 2005;53:965–72.
Kirkeskov L, Carlsen RK, Lund T, Buus NH. Emloyment of patients with kidney failure treated with dialysis or kidney transplantation - a systematic review and metaanalysis. BMC Nephrol. 2021;22–348:1–17.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2020;2021:372. https://doi.org/10.1136/bmj.n71.
Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. Newcastle-Ottawa Scale (NOS) for assessing the quality if nonrandomized studies in meta-analyses. 2009. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
Al-Jabi SW, Seleit DI, Badran A, Koni A, Zyoud SH. Impact of socio-demographic and clinical characteristics on functional disability and health-related quality of life in patients with rheumatoid arthritis: a cross-sectional study from Palestine. Health Qual Life Outcomes. 2021;19:241.
Allaire SH, Anderson JJ, Meenan RF. Reducing work disability associated with rheumatoid arthritis: Identifiction of additional risk factors and persons likely to benefit from intervention. Arthritis Care Res. 1996;9(5):9.
Allaire S, Wolfe F, Niu J, Lavalley MP. Comtemporary prevalence and incidence of work disability associated with rheumatoid arthritis in the US. Arthritis Rheum. 2008;59(4):7.
Anno S, Sugioka Y, Inui K, Tada M, Okano T, Mamoto K. Evaluation of work disability in Japanese patients with rheumatoid arthritis: from the TOMORROW study. Clin Rheumatol. 2018;37:9.
Azevedo ABC, Ferraz MB, Ciconelli RM. Indirect costs of rheumatoid arthritis in Brazil. Value Health. 2008;11:869–77.
Backman CL, Kennedy SM, Chalmers A, Singer J. Participation in paid and unpaid work by adults with rheumatoid arthritis. J Rheumatol. 2004;31:47–57.
Berner C, Haider S, Grabovac I, Lamprecht T, Fenzl KH, Erlacher L, et al. Work ability and employment in rheumatoid arthritis: a cross-sectional study on the role of muscle strength and lower extremity function. Int J Rheumatol. 2018;2018:11.
Bertin P, Fagnani F, Duburcq A, Woronoff AS, Chauvin P, Cukierman G, et al. Impact of rheumatoid arthritis on career progression, productivity, and employability: the PRET Study. Joint Bone Spine. 2016;83:6.
Bodur H, Borman P, Alper B, Keskin D. Work status and related variables in patients with rheumatoid arthitis and ankylosing spondylitis. Turk J Rheumatol. 2011;26(2):19.
Cadena J, Vinaccia S, Perez A, Rico MI, Hinojosa R, Anaya JM. The impact of disease activity on the quality of life, mental health status, and family dysfunction in Colombian patients with rheumatoid arthritis. Clin Rheumatol. 2003;9:142–50.
Callahan LF, Bloch DA, Pincus T. Identification of work disability in rheumatoid arthritis : physical, radiographic and laboratory variables do not add explanatory power to demographic and functional variables. J Clin Epidemiol. 1992;45(2):12.
Camilleri JP, Jessop AM, Davis S, Jessop JD, Hall M. A survey of factors affecting the capacity to work in patients with rheumatoid arthritis in South Wales. Clin Rehabil. 1995;9:4.
Chen MH, Lee MH, Liao HT, Chen WS, Lai CC, Tsai CY. Health-related quality of life outcomes in patients with rehumatoid arthritis and ankylosing spondylitis after tapering biologic treatment. Clin Rheumatol. 2018;37:429–38.
Chorus AMJ, Miedema HS, Wevers CJ, van der Linden S. Labour force participation among patients with rheumtoid arthritis. Ann Rheum Dis. 2000;59:6.
Chorus AMJ, Miedema HS, Wevers CJ, van der Linden S. Work factors and behavioural coping in relation to withdrawal from the labour force in patients with rheumatoid arthritis. Ann Rheum Dis. 2001;60:8.
Chung CP, Sokka T, Arbogast PG, Pincus T. Work disability in early rheumatoid arthritis: higher rates but better clinical status in Finland compared with the US. Ann Rheum Dis. 2006;65:5.
Dadoniene J, Stropuviene S, Venalis A, Boonen A. High work disability rate among rheumatoid arthritis patients in Lithuania. Arthritis Rheum. 2004;51:433–9.
De Roos AJ, Callahan LF. Differences by sex in correlates of work status in rheumatoid arthritis patients. Arthritis Care Res. 1999;12:381–91.
Dejaco C, Mueller T, Zamani O, Kurtz U, Egger S, Resch-Passini J, et al. A prospective study to evaluate the impact of Golimumab therapy on work productivity and activity, and quality of life in patients with rheumatoid arthritis, psoriatic arthritis and axil spondylarthritis in a real life setting in AUSTRIA. The Go-ACTIVE Study. Front Med. 2022;9:1–9.
Doeglas D, Suurmeijer T, Krol B, Sanderman R, van Leeuwen M, van Rijswijk M. Work disability in early rheumatoid arthritis. Ann Rheum Dis. 1995;54:6.
Fara N, Recchia O, Sequeira G, Sanchez K. Disability due to rheumatic diseases in the city of Junín, Argentina. Rheumatol Int. 2019;39:729–33.
Fifield J, Reisine S, Sheehan TJ, McQuillan J. Gender, paid work, and symptoms of emotional distress in rheumatoid arthritis patients. Arthritis Rheum. 1996;39:427–35.
Gomes RKS, Schreiner LC, Vieira MO, Machado PH, Nobre MRC. Staying in the labor force among patients with rheumatoid arthritis and associated factors in Southern Brazil. Adv Rheumatol. 2018;58(14):1–9.
Hamdeh HA, Al-Jabi SW, Koni A, Zyoud SH. Health-related quality of life and treatment satisfaction in Palestinians with rheumatoid arthritis: a cross-sectional study. BMC Rheumatol. 2022;6(19):1–12.
Hazes JM, Taylor P, Strand V, Purcaru O, Coteur G, Mease P. Physical function improvements and relief from fatigue and pain are associated with incresed productivity at work and at home in rheumatoid arthritis patients treated with certolizumab pegol. Rheumatology. 2010;49:1900–10.
Hulander E, Lindqvist HM, Wadell AT, Gjertsson I, Winkvist A, Bärebring L. Improvements in body composition after a proposed anti-inflammatory diet are modified by employment status in weight-stable patients with rheumatoid arthritis, a randomized controlled crossover trial. Nutrients. 2022;14:1058.
Intriago M, Maldonado G, Guerrero R, Moreno M, Moreno L, Rios C. Functional disability and its determinants in Ecudorian patients with rheumatoid arthritis. Open Access Rheumatol. 2020;12:97–104.
Kavanaugh A, Smolen JS, Emery P, Purcaru O, Keystone E, Richard L, et al. Effect of certolizumab pegol with ethotrexate on home and work place productivity and social activities in patients with active rheumatoid arthritis. Arthritis Rheum. 2009;61:1592–600.
Kwon JM, Rhee J, Ku H, Lee EK. Socioeconomic and employment status of patients with rheumatoid arthritis in Korea. Epidemiol Health. 2003;34:1–7.
Lacaille D, Sheps S, Spinelli JJ, Chalmers A, Esdaile JM. Identification of modifiable work-related factors that influence the risk of work disability in rheumatoid arthritis. Arthritis Rheum. 2004;51:843–52.
Lahiri M, Cheung PPM, Dhanasekaran P, Wong SR, Yap A, Tan DSH, et al. Evaluation of a multidisciplinary care model to improve quality of life in rheumatoid arthritis: a randomised controlled trial. Qual Life Res. 2022;31:1749–59.
Lapcevic M, Vukovic M, Gvozdenovic BS, Mioljevic V, Marjanovic S. Socioeconomic and therapy factor influence on self-reported fatigue, anxiety and depression in rheumatoid arthritis patients. Rev Bras Reumatol. 2017;57(6):12.
Mattila K, Buttgereit F, Tuominen R. Impact of morning stiffness on working behaviour and performance in people with rhematoid arthritis. Rheumatol Int. 2014;34:1751–8.
McQuillan J, Andersen JA, Berdahl TA, Willett J. Associations of rheumatoid arthritis and depressive symptoms over time: Are there differences by education, race/ethnicity, and gender? Arthritis Care Res. 2022;0:1–9.
Mäkisara GL, Mäkisara P. Prognosis of funcrional capacity and work capacity in rheumatoid arthritis. Clin Rheumatol. 1982;1(2):9.
Meenan RF, Yelin EH, Nevitt M, Epstein WV. The impact of chronic disease. A sociomedical profile of rheumatoid arthritis. Arthritis Rheum. 1981;24:544–9.
Morf H, Castelar-Pinheiro GR, Vargas-Santos AB, Baerwald C, Seifert O. Impact of clinical and psychological factors associated with depression in patients with rheumatoid arthritis: comparative study between Germany and Brazil. Clin Rheumatol. 2021;40:1779–87.
Newhall-Perry K, Law NJ, Ramos B, Sterz M, Wong WK, Bulpitt KJ, et al. Direct and indirect costs associated with the onset of seropositive rheumatoid arthritis. J Rheumatol. 2000;27:1156–63.
Osterhaus JT, Purcaru O, Richard L. Discriminant validity, responsiveness and reliability of the rheumatoid arthritis-specific Work Productivity Survey (WPS-RA). Arthritis Res Ther. 2009;11(R73):1–12.
Pieringer H, Puchner R, Pohanka E, Danninger K. Power of national economy, disease control and employment status in patients with RA - an analytical multi-site ecological study. Clin Rheumatol. 2016;35:5.
Rosa-Gocalves D, Bernardes M, Costa L. Quality of life and functional capacity in patients with rheumatoid arthritis - Cross-sectional study. Reumatol Clin. 2018;14:360–6.
Sacilotto NC, Giorgi RDN, Vargas-Santos AB, Albuquerque CP, Radominski SC, Pereira IA, et al. Real - rheumatoid arthritis in real life - study cohort: a sociodemographic profile of rheumatoid arthritis in Brazil. Adv Rheumatol. 2020;60:20.
Shanahan EM, Smith M, Roberts-Thomson L, Esterman A, Ahern M. Influence of rheumatoid arthritis on work participation in Australia. Intern Med J. 2008;38:166–73.
Smolen JS, van der Heijde DM, Keystone EC, van Vollenhoven RF, Golding MB, Guérette B, et al. Association of joint space narrowing with impairment of physical function and work ability in patients with early rheumatoid arthritis: protection beyond disease control by adalimumab plus methotrexate. Ann Rheum Dis. 2012;72:1156–62.
Syngle D, Singh A, Verma A. Impact of rheumatoid arthritis on work capacity impairment and its predictors. Clin Rheumatol. 2020;39:1101–9.
Tamborenea MN, Pisoni C, Toloza S, Mysler E, Tate G. Pereira D et al Work instability in rheumatoid arthritis patients from Argentina: prevalence and associated factors. Rheumatol Int. 2015;35:107–14.
Tanaka Y, Kameda H, Saito K, Kanedo Y, Tanaka E, Yasuda S, et al. Response to tocilizumab and work productivity in patients with rheumatoid arthritis: 2-year follow-up of FIRST ACT-SC study. Mod Rheumatol. 2021;21:42–52.
van der Zee-Neuen A, Putrik P, Ramiro S, Keszei AP, Hmamouchi I, Dougados M, Boonen A. Large country differences in work outcomes in patients with RA - an analysis in the multinational study COMORA. Arthritis Res Ther. 2017;19:216.
van Jaarsveld CHM, Jacobs JWG, Schrijvers AJP, van Albada-Kuipers GA, Hofman DM, Bijlsma JWJ. Effects of rheumatoid arthritis on employment and social participation during the first years of disease in the Netherlands. Br J Rheumatol. 1998;37:848–53.
Verstappen SMM, Boonen A, Bijlsma JWJ, Buskens E, Verkleij H, Schenk Y, et al. Working status among Dutch patients with rheumatoid arthritis: work disability and working conditions. Rheumatology. 2005;44:202–6.
Vliet Vlieland TPM, Buitenhuis NA, van Zeben D, Vandenbroucke JP, Breedveld FC, Hazes JMW. Sociodemographic factors and the outcome of rheumatoid arthritis in young women. Ann Rheum Dis. 1994;53:803–6.
Li F, Ai W, Ye J, Wang C, Yuan S, Xie Y, et al. Inflammatory markers and risk factors of RA patients with depression and application of different scales in judging depression. Clin Rheumatol. 2022;41:2309–17.
Wan SW, He HG, Mak A, Lahiri M, Luo N, Cheung PP, et al. Health-related quality of life and its predictors among patients with rheumatoid arthritis. Appl Nurs Res. 2016;30:176–83.
Xavier RM, Zerbini CAF, Pollak DF, Morales-Torres JLA, Chalem P, Restrepo JFM, et al. Burden of rheumatoid arthritis on patients’ work productivity and quality of life. Adv Rheumatol. 2019;59:47.
Yajima N, Kawaguchi T, Takahashi R, Nishiwaki H, Toyoshima Y, Oh K, et al. Adherence to methotrexate and associated factors considering social desirability in patients with rheumatoid arthritis: a multicenter cross-sectional study. BMC Rheumatol. 2022;6(75):1–8.
Yates M, Ledingham JM, Hatcher PA, Adas M, Hewitt S, Bartlett-Pestell S, et al. Disease activity and its predictors in early inflammatory arthritis: findings from a national cohort. Rheumatology. 2021;60:4811–20.
Yelin E, Henke C, Epstein W. The work dynamics of the person with rheumatoid arthritis. Arthritis Rheum. 1987;30:507–12.
Zhang W, Bansback N, Guh D, Li X, Nosyk B, Marra CA, et al. Short-term influence of adalimumab on work productivity outcomes in patients with rheumatoid arthritis. J Rheumatol. 2008;35:1729–36.
Żołnierczyk-Zreda D, Jędryka-Góral A, Bugajska J, Bedyńska S, Brzosko M, Pazdur J. The relationship between work, mental health, physical health, and fatigue in patients with rheumatoid arthritis: a cross-sectional study. J Health Psychol. 2020;25:665–73.
da Rocha Castellar Pinheiro G, Khandker RK, Sato R, Rose A, Piercy J. Impact of rheumatoid arthritis on quality of life, work productivity and resource utilisation: an observational, cross-sectional study in Brazil. Clin Exp Rheumatol. 2013;31:334–40.
Albers JMC, Kuper HH, van Riel PLCM, Prevoo MLL, Van’t Hof MA, van Gestel AM, et al. Socio-economic consequences of rheumatoid arthritis in the first year of the disease. Rheumatology. 1999;38:423–30.
Barrett EM, Scott DGI, Wiles NJ. The impact of rheumatoid arthritis on employment status in the early years of disease: a UK community-based study. Rheumatology. 2000;39:7.
Bejano V, Quinn M, Conaghan PG, Reece R, Keenan AM, Walker D, et al. Effect of the early use of the anti–tumor necrosis factor Adalimumab on the prevention of job loss in patients with early rheumatoid arthritis. Arthritis Care Res. 2008;59:1467–74.
Eberhardt K, Larsson BM, Nived K. Early rheumatoid arthritis – some social, economical, and psychological aspects. Scand J Rheum. 1993;22:119–23.
Eberhardt K, Larsson BM, Nived K, Lindqvist E. Work disability in rheumatoid arthritis- development over 15 years and evaluation of predictive factors over time. J Rheumatol. 2007;34:481–7.
Halpern MT, Cifaldi MA, Kvien TK. Impact of adalimumab on work participation in rheumatoid arthritis: comparison of an open-label extension study and a registry-based control group. Ann Rheum Dis. 2009;68:930–7.
Herenius MMJ, Hoving JI, Sluiter JK, Raterman HG, Lems WF, Dijkmans BAC, et al. Improvement of work ability, quality of life, and fatique in patients with rheumatoid arthritis treated with adalimumab. J Occup Environ Health. 2010;52:618–21.
Hoving JL, Bartelds GM, Sluiter JK, Sadiraj K, Groot I, Lems WF, et al. Perceived work ability, quality of life, and fatigue in patients with rheumatoid arthritis after a 6-month course of TNF inhibitors: prospective intervention study and partial economic evaluation. Scand J Rheumatol. 2009;38:246–50.
Jäntti J, Aho K, Kaarela K, Kautiainen H. Work disability in an inception cohort of patients with seropositive rheumatoid arthritis: a 20 year study. Rheumatology. 1999;38:4.
Kaarela K, Lehtinen K, Luukkainen R. Work capacity of patients with inflammatory joint diseases: an eight-year follow-up study. Scand J Rheumatol. 1987;16:403–6.
McWilliams DF, Varughese S, Young A, Kiely PD, Walsh DA. Work disability and state benefit claims in early rheumatoid arthritis: the ERAN cohort. Rheumatology. 2014;53:9.
Mau W, Bornmann M, Weber H, Weidemann HF, Hecker H, Raspe HH. Prediction of permanent work disability in a follow-up study of early rheumatoid arthritis: results of a tree structured analysis using RECPAM. Br J Rheumatol. 1996;35:652–9.
Nikiphorou E, Guh D, Bansback N, Zhang W, Dixey J, Williams P, et al. Work disability rates in RA. Results from an inception cohort with 24 years follow-up. Rheumatology. 2012;51:8.
Nordmark B, Blomqvist P, Andersson B, Hägerström M, Nordh-Grate K, Rönnqvist R, et al. A two-year follow-up of work capacity in early rheumatoid arthritis: a study of multidisciplinary team care with emphasis on vocational support. Scand J Rheumatol. 2006;35:7–14.
Pincus T, Callahan LF, Sale WG, Brooks AL, Payne LE, Vaughn WK. Severe functional declines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over mine years. Arthritis Rheum. 1984;27:864–72.
Puolakka K, Kautiainen H, Möttönen T, Hannonen P, Hakala M, Korpela M, et al. Predictors of productivity loss in early rheumatoid arthritis: a 5 year follow up study. Ann Rheum Dis. 2005;64:130–3.
Puolakka K, Kautiainen H, Möttönen T, Hannonen P, Korpela M, Julkunen H, et al. Impact of initial aggressive drug treatment with a combination of disease-modifying antirheumatic drugs on the development of work disability in early rheumatoid arthritis. Arthritis Rheum. 2004;50:55–62.
Reisine S, Fifield J, Walsh S, Feinn R. Factors associated with continued employment among patients with rheumatoid arthritis: a survival model. J Rheumatol. 2001;28:2400–8.
Reisine S, Fifield J, Walsh S, Dauser D. Work disability among two cohorts of women with recent onset rheumatoid arthritis: a survival analysis. Arthritis Rheum. 2007;57:372–80.
Robinson HS, Walters K. Return to work after treatment of rheumatoid arthritis. Can Med Assoc J. 1971;105:166–9.
Smolen JS, Han C, van der Heijde D, Emery P, Bathon JM, Keystone E, et al. Infliximab treatment maintains employability in patients with early rheumatoid arthritis. Arthritis Rheum. 2006;54:716–22.
van Vollenhoven RF, Cifaldi MA, Ray S, Chen N, Weisman MH. Improvement in work place and household productivity for patients with early rheumatoid arthritis treated with adalimumab plus methotrexate: work outcomes and their correlations with clinical and radiographic measures from a randomized controlled trial companion study. Arthritis Care Res. 2010;62:226–34.
Vazquez-Villegas ML, Gamez-Nava JI, Celis A, Sanchez-Mosco D, de la Cerda-Trujillo LF, Murillo-Vazquez JD, et al. Prognostic factors for permanent work disability in patients with rheumatoid arthritis who received combination therapy of conventional synthetic disease-modifying antirheumatic drugs. A retrospective cohort study. J Clin Rheumatol. 2017;23:376–82.
Verstappen SMM, Jacobs JWG, Kruize AA, Erlich JC, van Albada-Kuipers GA, Verkleij H, et al. Trends in economic consequences of rheumatoid arthritis over two subsequent years. Rheumatology. 2007;46:968–74.
Vlak T, Eldar R. Disability in rheumatoid arthritis after monotherapy with DMARDs. Int J Rehabil Res. 2003;26:207–12.
Yelin E, Trupin L, Katz P, Lubeck D, Rush S, Wanke L. Association between etanercept use and employment outcomes among patients with rheumatoid arthritis. Arthritis & Rheum. 2003;48:3046–54.
Young A, Dixey J, Cox N, Davies P, Devlin J, Emery P, et al. How does functional disability in early rheumatoid arthritis (RA) affect patients and their lifes? Results of 5 years of follow-up in 732 patients from the Early RA Study (ERAS). Rheumatology. 2000;39:603–11.
Young A, Dixey J, Kulinskaya E, Cox N, Davies P, Devlin J, et al. Which patients stop working because of rheumatoid arthritis? Results of five years’ follow up in 732 patients from the Early RA Study (ERAS). Ann Rheum Dis. 2002;61:335–40.
Zirkzee EJM, Sneep AC, de Buck PDM, Allaart CF, Peeters AJ, Ronday HK, et al. Sick leave and work disability in patients with early arthritis. Clin Rheumatol. 2008;27:9.
Reisine S, McQuillan J, Fifield J. Predictors of work disability in rheumatoid arthritis patients. Arthritis Rheum. 2005;38:1630–7.
Verstappen SMM, Watson KD, Lunt M, McGrother K, Symmons PM, Hyrich KL. Working status in patients with rheumatoid arthritis, ankylosing spondylitis and psoriatic arthritis: results from the British Society for Rheumatology Biogics Register. Rheumatology. 2010;49:1570–7.
Nissilä M, Isomäki H, Kaarela K, Kiviniemi P, Martio J, Sarna S. Prognosis of inflammatory joint diseases. A three-year follow-up study. Scand J Rheumatol. 1983;12:33–8.
Han C, Smolen J, Kavanaugh A, St.Clair EW, Baker D, Bala M. Comparison of employability outcomes among patients with early or long-standing rheumatoid arthritis. Arthritis Rheum. 2008;59:510–4.
Gwinnutt JM, Leggett S, Lunt M, Barton A, Hyrich KL, Walker-Bone K, et al. Predictors of presenteeism, absenteeism and job loss in patients commencing methotrexate or biologic therapy for rheumatoid arthritis. Rheumatology. 2020;59:2908–19.
Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020. https://doi.org/10.1016/S0140-6736(20)32340-0:1-12.
Gwinnutt JM, Wieczorek M, Balanescu A, Bischoff-Ferrari HA, Boonen A, Cavalli G, et al. 2021 EULAR recommendations regarding lifestyle behaviours and work participation to prevent progression of rheumatic and musculoskeletal diseases. Ann Rheum Dis. 2023;82:48–56.
England BR, Smith BJ, Baker NA, Barton JL, Oatis CA, Guyatt G, et al. 2022 American College of Rheumatology Guideline for exercise, rehabilitation, diet, and additional integrative interventions for rheumatoid arthritis. Arthritis Care Res. 2023;75:1603–15.
Vu M, Carvalho N, Clarke PM, Buchbinder R, Tran-Duy A. Impact of comorbid conditions on healtcare expenditure and work-related outcomes in patients with rheumatoid arthritis. J Rheumatol. 2021;48:1221–9.
Amaral GSG, Ots P, Brouwer S, van Zon SKR. Multimorbidity and exit from paid employment: the effect of specific combinations of chronic health conditions. Eur J Public Health. 2022;32:392–7.
Boonen A, Putrik P, Marques ML, Alunno A, Abasolo L, Beaton D, et al. EULAR Points to Consider (PtC) for designing, analysing and reporting of studies with work participation as an outcome domain in patients with inflammatory arthritis. Ann Rheum Dis. 2021;80:1116–23.
Lajas C, Abasolo L, Bellajdel B, Hernandez-Garcia C, Carmona L, Vargas E, et al. Costs and predictors of costs in rheumatoid arthritis: A prevalence-based study. Arthritis Care Res. 2003;49:64–70.
Reisine S, McQuillan J, Fifield J. Predictors of work disability in rheumatoid arthritis patients. Arthritis Rheum. 1995;38:1630–7.
Acknowledgements
None.
Funding
Open access funding provided by Royal Library, Copenhagen University Library
Author information
Authors and Affiliations
Contributions
LK performed the systematic research, including reading articles, performed the blinded quality assessment and the meta-analysis, and drafted and revised the article. KM performed the blinded quality assessment and the discussion afterwards of articles to be included in the research and the scores, and drafted and revised the article.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable as this is a systematic review. All the studies that are included have obtained ethical approval and consent as appreciated by the journal in which they have been published.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Figure S1.
Employment; year of investigation.
Additional file 2: Figure S2.
Forest Plot of Comparison: Predictors for employment. Outcome: Younger or older age.
Additional file 3: Figure S3.
Forest Plot of Comparison: Predictors for employment. Outcome: >50 yr or <50 yr of age.
Additional file 4: Figure S4.
Forest Plot of Comparison: Predictors for employment. Outcome: Gender: Male or Female.
Additional file 5: Figure S5.
Forest Plot of Comparison: Predictors for employment. Outcome: Educational level: no college education or college education or higher.
Additional file 6: Figure S6.
Forest Plot of Comparison: Predictors for employment. Outcome: no comorbidities present or one or more comorbidities present.
Additional file 7: Figure S7.
Forest Plot of Comparison: Predictors for employment. Outcome: Ethnicity: Caucasian or other than Caucasian.
Additional file 8: Figure S8.
Forest Plot of Comparison: Predictors for employment. Outcome: Short or long disease duration.
Additional file 9: Figure S9.
Forest Plot of Comparison: Predictors for employment. Outcome: Low or high Health Assessment Questionnaire, HAQ-score.
Additional file 10: Figure S10.
Forest Plot of Comparison: Predictors for employment. Outcome: Low or high VAS-score.
Additional file 11: Figure S11.
Forest Plot of Comparison: Predictors for employment. Outcome: Job type: blue collar workers or other job types.
Additional file 12: Figure S12.
Forest Plot of Comparison: Predictors for employment. Outcome: No MTX or MTX.
Additional file 13: Figure S13.
Forest Plot of Comparison: Predictors for employment. Outcome: No biological or biological.
Additional file 14: Figure S14.
Forest Plot of Comparison: Predictors for employment. Outcome: No prednisolone or prednisolone.
Additional file 15: Figure S15.
Forest Plot of Comparison: Predictors for employment. Outcome: Low or high DAS score.
Additional file 16: Figure S16.
Forest Plot of Comparison: Predictors for employment. Outcome: Low or high SF 36-score.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Kirkeskov, L., Bray, K. Employment of patients with rheumatoid arthritis - a systematic review and meta-analysis. BMC Rheumatol 7, 41 (2023). https://doi.org/10.1186/s41927-023-00365-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41927-023-00365-4