
Abstract
Purpose
To evaluate the measurement properties of the Oxford Hip Score (OHS), EQ-5D-5L utility index and EQ-5D-5L visual analogue scale (EQ-VAS) in patients undergoing elective total hip arthroplasty in Australia.
Methods
In this prospective multi-centre study, the OHS and EQ-5D-5L were collected preoperatively, six weeks (6w) and six months (6m) postoperatively. The OHS, EQ-VAS and EQ-5D-5L index were evaluated for concurrent validity, predictive validity (Spearman's Rho of predicted and observed values from a generalised linear regression model (GLM)), and responsiveness (effect size (ES) and standard response mean (SRM)).
Results
362 patients were included in this analysis for 6w and 269 for 6m. The EQ-5D-5L index showed good concurrent validity with the OHS (r = 0.71 preoperatively, 0.61 at 6w and 0.59 at 6m). Predictive validity for EQ-5D-5L index was similar to OHS when regressed (GLM). Responsiveness was good at 6w (EQ-5D-5L index ES 1.53, SRM 1.40; OHS ES 2.16, SRM 1.51) and 6m (EQ-5D-5L index ES 1.88, SRM 1.70; OHS ES 3.12, SRM 2.24). The EQ-VAS returned poorer results, at 6w an ES of 0.75 (moderate) and SRM 0.8. At 6m the EQ-VAS had an ES of 0.92 and SRM of 1.00. It, however, had greater predictive validity.
Conclusions
The EQ-5D-5L index and the OHS demonstrate strong concurrent validity. The EQ-5D-5L index demonstrated similar predictive validity at 6w and 6m, and both PROMs had adequate responsiveness. The EQ-VAS should be used routinely together with the EQ-5D-5L index. The EQ-5D-5L is suitable to quantify health-related quality of life in Australian hip arthroplasty patients.
Similar content being viewed by others

Introduction
Total hip arthroplasty (THA) is a common operation, with 32,929 replacements performed annually in Australia (133 per 100,000) in 2017–2018 [1]. Learmonth et al. called it “the operation of the century” in The Lancet [2], citing improvements in quality of life following this procedure and naming cost-effectiveness as the main factor that would determine further developments in this area. Health economics and patient recovery are used as part of the evaluation of patient outcomes. Patient outcomes can be measured using patient-related outcome measures (PROMs).
The 3-level version of the EuroQol 5 Dimensions (EQ-5D-3L) is such a PROM. It is a standardized health-related quality of life (HRQoL) questionnaire that was developed in 1990 and designed to assess general health at three different levels for five dimensions [3, 4]. In 2011, it was further revised to a 5-level version (EQ-5D-5L) with five levels and five dimensions [5]. This was done to measure more nuanced differences in health response and reduce the ceiling effect. The EQ-5Dsuite of questionnaires are some of the most widely used PROMs globally. In the United Kingdom, for instance, the EQ-5D is an instrument recommended by the National Institute for Health and Clinical Excellence (NICE), the premier health technology assessment body, for calculating quality adjusted life years used in cost-utility analysis [6,7,8].
A validated outcome measure is one that has been tested to ensure the production of reliable, accurate results. The EQ-5D-5L has not yet been validated for the Australian orthopaedic population for HRQoL assessment. The results of the PROM are converted into ‘vectors’. These are five-digit codes representing a health state. For example, 11,111 is full health, and 55,555 represents the worst health. There are 3125 possible health states. These health states are then mapped onto a single EQ-5D-5L utility index using a country-specific value set. If a country-specific value set is not yet validated, the scores can be examined using the EQ-5D-3L value sets using a “crosswalk” method [9]. Alternatively, the generic Western Preference Pattern [10] can be used. Both of these choices come with issues related to nonspecificity and lack of validation. To date, 28 countries have validated country-specific EQ-5D-5L value sets, including England, Uruguay, Japan, Canada, The Netherlands and South Korea [11].
The EQ-VAS is a stand-alone component of the EQ-5D-5L, a rating system for the patient to self-report how they feel their general health is. The EQ-VAS is seen as a simple and unambiguous manner for a patient to communicate overall functionality and is conceptually different to the question-and-answer based nature of the rest of the PROM [12]. The Oxford Hip Score (OHS) is a PROM that was specifically developed to assess function and pain in patients undergoing a THA [13]. It has been previously utilised for assessing the concurrent validity of the EQ-5D-5L index score in THA patients in other countries [14]. A copy of the Oxford Hip Score PROM is attached as Appendix 1, while that for the EQ-5D-5L PROM is attached as Appendix 2.
This study aims to test the concurrent and predictive validity of the EQ-5D-5L (EQ-5D-5L utility index and the EQ-VAS) when compared against the OHS in the Australian hip arthroplasty population. We test concurrent and predictive validity. Concurrent validity describes the extent to which the measure to be tested correlates with an established method to measure the same. In this case, the measure to be tested is the EQ-5D-5L, and the established measurement tool is the OHS. Predictive validity describes the association between baseline and follow-up outcomes. Predictive validity is highly valued in this cohort, as this has implications for surgical suitability for individual patients. We also test responsiveness, which is defined as a measure of the sensitivity of PROMs to reflect the change in health status over time.
Patients and methods
This multi-centre prospective study was conducted at two tertiary teaching hospitals in Australia. Orthopaedic surgeons operate routinely at both hospitals, performing approximately 500 hip arthroplasty procedures per year. Due to SARS Covid-19 related restrictions on elective operations, in 2020, this number was reduced to approximately 300 patients. The local Human Research Ethics Committee granted multi-centre approval (SALHN/329.17).
All consecutive adult patients undergoing elective total hip arthroplasty surgery were prospectively enrolled over an almost three-year period from 8th January 2018 to 1st of October 2020, with a six-month follow-up until 2nd April 2021. Informed consent was obtained from all participants. Baseline demographics were recorded for all patients, including age, gender, body mass index (BMI) and Charlson comorbidity index (CCI) [15].
Data were recorded by a dedicated research assistant, using scripted questionnaires either via telephone or via a written survey sent by postal mail. The same English language script was used at three different time points: preoperatively and six weeks and six months postoperatively. At all three time points, two validated PROMs were used: the Oxford Hip Score (OHS) [16] and the EQ-5D-5L [3] including the EQ-VAS stand-alone component. Data were entered into a password secured database and stored on the hospital computer network.
Patients were included for analysis if they had complete quality of life data. This was defined as completing the EQ-5D-5L and OHS preoperatively and at six weeks postoperatively. The validation of the EQ-5D-5L utility values was established using a discrete choice experiment approach [17].
Oxford Hip Score
The OHS is a joint-specific PROM [18] that has been used extensively over the last 20 years [19,20,21]. It assesses six fields, each with 2 questions (12 questions total). These fields are pain, walking, physical activity, function, quality of life and psychological wellbeing. Each question is scored on a 5-point discrete visual analogue scale, with higher numbers correlating with better function. (Appendix 1). The final score is a total of the individual question scores. In this study, it effectively functioned as a comparative control.
EQ-5D-5L index and EQ-VAS
The EQ-5D-5L is a standardized health-related quality of life (HRQoL) PROM that the EuroQol Group designed to quantify generic health in the adult population in the fields of mobility, self-care, usual activities, anxiety/depression and pain/discomfort. Response levels are on a 5-point scale of none, slight, moderate, severe and extreme/unable to perform. Based on Australian general population preference weights determined through a discrete choice experiment approach [17], a utility index ranging from − 0.676 to 1 can be attached to each of the EQ-5D-5L health states. Higher utilities represent better HRQoL.
The EQ-VAS is a vertical visual analogue scale that forms part of the EQ-5D-5L. It asks patients to rate their general health from 0 to 100. Higher numeric scores represent better patient function.
Statistical analysis
All statistical analyses were performed using STATA version 17 (StataCorp, Texas, USA). Continuous variables (age, BMI, CCI) were expressed as mean and standard deviation, whereas the categorical variable (gender) was expressed as percentages (counts). A p-value of < 0.05 was considered statistically significant.
Concurrent validity, predictive validity and agreement
For analysis of concurrent validity, the Spearman’s correlation coefficient (rho, ρ) was utilised to compare the EQ-5D-5L index score, dimension scores of the EQ-5D-5L and EQ-VAS against the OHS. The strength of the relationship was considered low/weak (ρ < 0.25), fair (ρ = 0.25–0.50), good (ρ = 0.50–0.75), and excellent (ρ > 0.75). This magnitude of rank order correlations was sourced from previous publications on the same area [22, 23]. Predictive validity was ascertained using a regression framework whilst controlling for confounders. We utilised generalized linear models with the 6-week and 6-month postoperative PROMs as the dependant variables and preoperative values and baseline characteristics as independent variables. The average marginal effect regarding preoperative score was used to compare models if different distribution families were utilised. Agreement between the EQ-5D-5L index score and the OHS was measured using Krippendorff’s alpha, which is a reliability coefficient designed to measure the agreement among observers, coders, judges, raters, or measuring instruments [7, 24]. The following interpretations of agreement were applied: below 0.0—poor, 0.00 to 0.20—slight, 0.21 to 0.40—fair, 0.41 to 0.60—moderate, 0.61 to 0.80—substantial and 0.81 to 1.00—almost perfect [25]. Two measures of absolute agreement were considered as alternatives to Krippendorff’s alpha: Lin’s Concordance Correlation Coefficient (CCC), which is robust to departures from normality [26] and Intraclass Correlation Coefficient (ICC), with PROM data transformed using power analysis to conform to assumptions of normality and stable variance required for ICC [27,28,29]. The ICC was based on a two-way mixed-effect model where the individual effect was random and the effect of the instrument was fixed. Data were analyzed using Intercooled Stata software version 17.1 for Windows (Stata Corp. College Station, TX, USA). Values of the ICC and CCC higher than 0.9 were considered to indicate excellent reliability, good between 0.9 and 0.75, moderate between 0.75 and 0.5, and poor below 0.5 [27].
Responsiveness
Responsiveness is a measure of the sensitivity of PROMs to reflect the change in health status over time. For this study, we compared measures at baseline and at 6 weeks and 6 months follow-up using paired t-tests. Further assessment of responsiveness was quantified using effect size (ES) and standardized response mean (SRM).
Effect size was calculated using the formula:
Standard response mean was calculated using the formula:
ES and SRM were classified according to Cohen’s rule of thumb, as large (≥ 0.8), moderate (0.5–0.79) or small (< 0.5). Both ES and SRM are standardized measures of change over time in health, independent of sample size.
Influence of baseline characteristics on PROMs
Regression analysis using generalised linear models was performed with respect to baseline characteristics (age, gender, BMI and CCI), using the preoperative EQ-5D-5L index score, EQ-VAS and OHS as independent variables. The postoperative PROMs were used as the dependent variables. Depending on the distribution of the dependant variable, an appropriate distribution family and canonical link function were chosen. Multiple families were trialled when there was difficulty ascertaining the appropriate family of distribution, and the best fitting model was selected based on low Akaike's Information Criteria and Bayesian Information Criteria score. The coefficient, standard error and p-values were recorded.
Since the EQ-5D-5L index scores had negative values, it was determined that the Gaussian family of distribution with a canonical identity link was most appropriate. Both OHS and EQ-VAS had a non-negative distribution. Multiple families and their canonical links were fitted, including Gaussian, inverse Gaussian, Poisson, and Gamma distributions were tested for best fit. In both OHS and EQ-VAS, it was determined that the Gamma distribution provided the best fit and was hence used for the final model.
Results
In total, 362 hip arthroplasty patients were identified from the database. These had complete data for preoperative and 6 weeks postoperatively and could be included in these two analyses. Of these, 269 were included in the study, with postoperative PROMs at 6 months available. This is due to a 26% attrition rate at 6 months.
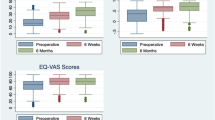
The mean age of our cohort at the time of surgery was 68.5 (SD = 12.5) years old, and 55.8% (202/362) were female. The mean preoperative BMI was 30.8 (SD = 5.6), and the mean CCI was 73.7% (SD = 22.5). A summary of baseline characteristics can be found in Table 1. Boxplots for the distributions of scores at baseline (preoperative), 6 weeks and 6 months is shown in Fig. 1.

Boxplots showing distribution of PROMs scores over time
Concurrent validity, predictive validity and agreement
The EQ-5D-5L index showed good concurrent validity when compared to OHS at baseline, 6 weeks, and 6 months postoperative, with a Spearman’s coefficient of 0.71, 0.61 and 0.59, respectively. EQ-VAS had good concurrent validity at 6 weeks when compared to OHS, and fair concurrent validity at baseline and 6 months, with a Spearman’s coefficient of 0.53, 0.37 and 0.45, respectively (Table 2).
In Table 3, the dimensions of the EQ-5D-5L index showed good concurrent validity when compared to the corresponding OHS at baseline, 6 weeks, and 6 months postoperative, with a Spearman’s coefficient ranging from 0.52 to 0.62 (good) for Mobility, Self-Care, Usual Activities and Pain. Concurrent validity was only fair for the Anxiety/Depression dimension, with a Spearman’s coefficient of 0.28 (preoperative), 0.33 (6 weeks) and 0.37 (6 months).
The predictive validity of each score generated by the three different scores was determined using generalized linear models, with regression to baseline scores and covariates. In all cases, the distribution that provided the best model fit was the Gamma distribution with a canonical negative inverse link. The average marginal effects for the preoperative score were recorded and displayed in Table 2. The EQ-5D-5L index score showed similar predictive validity when compared to OHS at 6 weeks (average marginal effect of 0.19 and 0.18 respectively) and 6 months (average marginal effect of 0.23 and 0.16 respectively). However, EQ-VAS showed greater predictive validity than both OHS and EQ-5D-5L index score at 6 weeks and 6 months (average marginal effect of 0.37 and 0.31 respectively).
As shown in Table 4, the agreement between the EQ-5D-5L utility and OHS total scores ranged from moderate to substantial/good when measured using all three agreement indices (Krippendorff’s alpha, ICC and CCC). The best agreement was seen at the preoperative stage, while the least agreement was at 6 weeks. There was less agreement between the EQ-VAS and OHS total scores, ranging from poor/fair to moderate. The best agreement was seen at 6 weeks, while the least agreement was at the preoperative stage.
Responsiveness
These findings are detailed in Table 5. At 6 weeks, all three PROMs showed significant differences between baseline and follow-up scores. Both OHS and EQ-5D-5L had a large ES and SRM. The ES for OHS and EQ-5D-5L index was 2.16 and 1.53, respectively, and the SRM was 1.51 and 1.40, respectively, p < 0.0001. The EQ-VAS had a moderate ES of 0.75 and a large SRM of 0.80, p < 0.0001.
At 6 months, all three PROMs again showed a significant difference between baseline and follow-up scores: The ES for OHS, EQ-5D-5L index and EQ-VAS was 3.12, 1.88 and 0.92, respectively, and the SRM was 2.24, 1.70 and 1.00, respectively.
Influence of baseline characteristics on PROMs
There was a statistically significant positive association between higher preoperative OHS scores on one end and both male gender and BMI. However, higher EQ-5D-5L index and EQ-VAS scores were only significantly associated with higher BMI and male gender, respectively.
Discussion
This analysis is an empirical validation of the EQ-5D-5L for suitability of HRQoL assessment for hip arthroplasty patients using experienced-based patient data from a prospective multi-centre study database, with the correlation between the Oxford Hip Scores, EQ-VAS, and the EQ-5D-5L PROMs examined. The findings support the utilization of EQ-5D-5L index score as a valid and reliable instrument in assessing HRQoL amongst these patients.
The limits of agreement were good between the EQ-5D-5L index score and the OHS, and they can be considered similar to each other in terms of concurrent validity. However, the OHS is a joint-specific PROM, whereas the EQ-5D-5L index score is designed to assess overall functionality. For example, someone who can compensate enough to perform daily tasks and cope well with the mental burden of an arthritic hip on the EQ-5D-5L index score, may record gait disturbances and set specific difficulties with mobility on the OHS. We chose the OHS as a comparator for this validation as it is a widely used PROM, with significant overlap in terms of items with the EQ-5D-5L index score. For example, both feature mobility, pain/discomfort and usual activities. This was shown in more detail when the OHS was compared against the dimensions of the EQ-5D-5L. There is a high degree of correlation between the dimensions for the EQ-5D-5L and the OHS for the most part. The exception is the relationship between the Anxiety/Depression dimension of the EQ-5D-5L and the OHS, where the correlation is only fair. This is in line with evidence from the literature [30,31,32] that shows that strong correlations exist between instruments and dimensions that measured similar constructs. Hence, they should be utilised concurrently to complement each other, instead of being considered as substitutes for one another.
The longitudinal nature of this study with multiple time points lends itself well to assessing incremental changes in the population and detecting differences in the performance of both PROMs. The experience-based and prospective nature of this data is also a strong point.
The EQ-VAS as a stand-alone measure showed a smaller ES than the EQ-5D-5L index score at both six weeks (0.75 versus 1.53 respectively, p < 0.0001) and six months (0.80 versus 1.40 respectively, p < 0.0001). SRM was also large for both scores at the six-week and six-month time points. However, the EQ-VAS has better predictive validity than the EQ-5D-5L index score and OHS. This suggests that it has a higher predictive value for postoperative recovery and should be routinely used as an adjunct to the EQ-5D-5L index score. A reason for this better predictive validity may be the much broader nature of the VAS (i.e. not proscribed by the domains or items as in the OHS or EQ-5D-5L descriptive system) which allows the patients to include more in their subjective rating of health. This is beneficial for patient stratification and counselling with regards to realistic rehabilitation expectations and postsurgical results.
An assessment of the agreement between the EQ-5D-5L and the EQ-VAS on one hand and the OHS on the other showed acceptable agreement (moderate to good/substantial for most comparisons). This suggests that while the ratings from the instruments were not identical, they were moderately close and should be considered complements rather than substitutes of one another.
Some limitations of this study have to be addressed. There were approximately 25% missing data for patients at six months. Therefore, these patients had to be excluded, introducing a response bias. There was also an incomplete recording of patients’ baseline characteristics, with 90.6% (328/362) patients having their BMI recorded and 94.2% (341/362) having their CCI recorded.
Conclusions
In conclusion, The EQ-5D-5L index score and the Oxford Hip Score demonstrate good concurrent validity in this study. The EQ-5D-5L index score revealed a large effect size at six weeks and six months postoperatively, and both PROMs had adequate responsiveness. The EQ-5D-5L index score PROM is suitable to quantify general health-related quality of life in the Australian hip arthroplasty patient population.
Availability of data and supporting materials
Data available upon request.
Abbreviations
- THA:
-
Total hip arthroplasty
- 6w:
-
Six weeks
- 6m:
-
Six months
- ES:
-
Effect size
- SRM:
-
Standardized response mean
- PROMs:
-
Patient reported outcome measures
- OHS:
-
Oxford Hip Score
- VAS:
-
Visual analogue scale
- CCI:
-
Charleson Comorbidity Index
- HRQoL:
-
Health Related Quality of Life
- TMLE:
-
Targeted maximum likelihood estimation
- BMI:
-
Body mass index
- TTO:
-
Time trade off
References
Osteoarthritis. https://www.aihw.gov.au/reports/phe/232/osteoarthritis/contents/treatment-management
Learmonth ID, Young C, Rorabeck C (2007) The operation of the century: total hip replacement. Lancet 370(9597):1508–1519
EuroQol G (1990) EuroQol–a new facility for the measurement of health-related quality of life. Health Policy 16(3):199–208
Brooks R (1996) EuroQol: the current state of play. Health Policy 37(1):53–72
Herdman M, Gudex C, Lloyd A, Janssen M, Kind P, Parkin D et al (2011) Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 20(10):1727–1736
Maignen F, Osipenko L, Pinilla-Dominguez P, Crowe E (2017) Integrating health technology assessment requirements in the clinical development of medicines: the experience from NICE scientific advice. Eur J Clin Pharmacol 73(3):297–305
Kaambwa B, Bulamu NB, Mpundu-Kaambwa C, Oppong R (2021) Convergent and discriminant validity of the Barthel Index and the EQ-5D-3L when used on older people in a rehabilitation setting. Int J Environ Res Public Health 18(19):66
Guide to the Methods of Technology Appraisal 2013 (2013) NICE process and methods guides. London
Klapproth CP, van Bebber J, Sidey-Gibbons CJ, Valderas JM, Leplege A, Rose M et al (2020) Predicting EQ-5D-5L crosswalk from the PROMIS-29 profile for the United Kingdom, France, and Germany. Health Qual Life Outcomes 18(1):389
Olsen JA, Lamu AN, Cairns J (2018) In search of a common currency: a comparison of seven EQ-5D-5L value sets. Health Econ 27(1):39–49
Gerlinger C, Bamber L, Leverkus F, Schwenke C, Haberland C, Schmidt G et al (2019) Comparing the EQ-5D-5L utility index based on value sets of different countries: impact on the interpretation of clinical study results. BMC Res Notes 12(1):18
Ernstsson O, Burstrom K, Heintz E, Molsted AH (2020) Reporting and valuing one’s own health: a think aloud study using EQ-5D-5L, EQ VAS and a time trade-off question among patients with a chronic condition. Health Qual Life Outcomes 18(1):388
Murray DW, Fitzpatrick R, Rogers K, Pandit H, Beard DJ, Carr AJ et al (2007) The use of the Oxford hip and knee scores. J Bone Joint Surg Br 89(8):1010–1014
Conner-Spady BL, Marshall DA, Bohm E, Dunbar MJ, Noseworthy TW (2018) Comparing the validity and responsiveness of the EQ-5D-5L to the Oxford hip and knee scores and SF-12 in osteoarthritis patients 1 year following total joint replacement. Qual Life Res 27(5):1311–1322
Schmolders J, Friedrich MJ, Michel R, Strauss AC, Wimmer MD, Randau TM et al (2015) Validation of the Charlson comorbidity index in patients undergoing revision total hip arthroplasty. Int Orthop 39(9):1771–1777
Yeo MGH, Goh GS, Chen JY, Lo NN, Yeo SJ, Liow MHL (2020) Are Oxford Hip Score and Western Ontario and McMaster Universities Osteoarthritis index useful predictors of clinical meaningful improvement and satisfaction after total hip arthroplasty? J Arthroplasty 35(9):2458–2464
Norman R, Cronin P, Viney R (2013) A pilot discrete choice experiment to explore preferences for EQ-5D-5L health states. Appl Health Econ Health Policy 11(3):287–298
Dawson J, Fitzpatrick R, Carr A, Murray D (1996) Questionnaire on the perceptions of patients about total hip replacement. J Bone Joint Surg Br 78(2):185–190
Rolfson O, Eresian Chenok K, Bohm E, Lubbeke A, Denissen G, Dunn J et al (2016) Patient-reported outcome measures in arthroplasty registries. Acta Orthop 87(Suppl 1):3–8
Haragus H, Prejbeanu R, Poenaru DV, Deleanu B, Timar B, Vermesan D (2018) Cross-cultural adaptation and validation of a patient-reported hip outcome score. Int Orthop 42(5):1001–1006
Uesugi Y, Makimoto K, Fujita K, Nishii T, Sakai T, Sugano N (2009) Validity and responsiveness of the Oxford Hip Score in a prospective study with Japanese total hip arthroplasty patients. J Orthop Sci 14(1):35–39
Weber M, Van Ancum J, Bergquist R, Taraldsen K, Gordt K, Mikolaizak AS et al (2018) Concurrent validity and reliability of the Community Balance and Mobility scale in young-older adults. BMC Geriatr 18(1):156
Lamu AN, Bjorkman L, Hamre HJ, Alraek T, Musial F, Robberstad B (2021) Validity and responsiveness of EQ-5D-5L and SF-6D in patients with health complaints attributed to their amalgam fillings: a prospective cohort study of patients undergoing amalgam removal. Health Qual Life Outcomes 19(1):125
Krippendorff K (2004) Content analysis: an introduction to its methodology. Sage, Thousand Oaks
ten Hove D, Jorgensen TD, van der Ark LA (2018) In: Wiberg M, Culpepper S, Janssen R, González J, Molenaar D (eds). Quantitative psychology: the 82nd annual meeting of the psychometric society, chapter: on the usefulness of interrater reliability coefficients. Springer, Zurich. https://doi.org/10.1007/978-3-319-77249-3_6
Lin LI (1989) A concordance correlation coefficient to evaluate reproducibility. Biometrics 45(1):255–268
Koo TK, Li MY (2016) A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med 15(2):155–163
Bobak CA, Barr PJ, O’Malley AJ (2018) Estimation of an inter-rater intra-class correlation coefficient that overcomes common assumption violations in the assessment of health measurement scales. BMC Med Res Methodol 18(1):93
Gwet KL (2014) Handbook of inter-rater reliability: the definitive guide to measuring the extent of agreement among raters, 4th edn. STATAXIS Publishing Company/Advanced Analytics, LLC, Gaithersburg
Kaambwa B, Gill L, McCaffrey N, Lancsar E, Cameron ID, Crotty M et al (2015) An empirical comparison of the OPQoL-Brief, EQ-5D-3 L and ASCOT in a community dwelling population of older people. Health Qual Life Outcomes 13:164
Mulhern B, Meadows K (2014) The construct validity and responsiveness of the EQ-5D, SF-6D and Diabetes Health Profile-18 in type 2 diabetes. Health Qual Life Outcomes 12:42
Peters LL, Boter H, Slaets JP, Buskens E (2013) Development and measurement properties of the self assessment version of the INTERMED for the elderly to assess case complexity. J Psychosom Res 74(6):518–522
Acknowledgements
Not applicable.
Funding
The authors have no sources of funding to declare for this manuscript.
Author information
Authors and Affiliations
Contributions
D-YL, MBBS—This author conceived, designed, and submitted to Ethics and Governance the relevant protocols. This author also prepared the drafts, analyzed and prepared the data, and approved and submitted the final manuscript. TSC, MD—This author conceived, assisted with designing, conducted the statistical analysis, critically revised the drafts, and approved the final manuscript. AJS, BMBS—This author conceived, designed and realized the study protocol, supervised the database, realized the study, acquired the data, and approved the final manuscript. BB, BMBS—This author conceived and designed the study, and approved the final manuscript. BK, PhD—This author supervised the statistical analysis, and approved the final manuscript. HMK, MD, PhD.—This author conceived, assisted with designing, critically revised the drafts, and approved the final manuscript. Professor RLJ, MD, PhD.—This author conceived, assisted with designing, realized the study, lended departmental support, revised the drafts, and approved the final manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The local Human Research Ethics Committee granted multi-centre approval (SALHN/329.17). Informed consent was obtained from all participants.
Consent for publication
Consent for publication was included in the initial informed consent from all participants. We as an author group also approve this manuscript and give consent for publication.
Competing interests
All authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Oxford Hip Score.
Additional file 2.
EQ-5D-5L.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lin, DY., Cheok, T.S., Samson, A.J. et al. A longitudinal validation of the EQ-5D-5L and EQ-VAS stand-alone component utilising the Oxford Hip Score in the Australian hip arthroplasty population. J Patient Rep Outcomes 6, 71 (2022). https://doi.org/10.1186/s41687-022-00482-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41687-022-00482-7