
Abstract
Background
The lack of an appropriate retina-specific patient-reported outcome instrument restricts the understanding of the full impact of hereditary retinal diseases and other less common but potentially blinding acquired retinal diseases such as, vascular occlusions, epiretinal membrane, macular hole, central serous retinopathy and other vitreoretinopathies on quality of life. This study aims to explore the quality of life issues in people with hereditary retinal diseases and acquired retinal diseases to develop disease-specific patient-reported outcome instruments.
Methods
A qualitative research methodology to understand the lived experiences of people with retinal diseases was carried out. Data were collected through semistructured interviews. The coding, aggregation and theme development was carried out using the NVivo −10 software.
Results
Seventy-nine interviews were conducted with participants with hereditary retinal diseases (n = 32; median age = 57 years) and acquired retinal diseases (n = 47; median age = 73 years). We identified nine quality of life themes (domains) relevant to people with retinal diseases. Difficulty in performing important day-to-day activities (activity limitation) was the most prominent quality of life issue in the hereditary retinal diseases group whereas concerns about health, disease outcome and personal safety (health concerns) was the most prominent quality of life issue in the acquired retinal diseases group. Participants with hereditary retinal diseases had more issues with social interaction (social well-being), problems with mobility and orientation (mobility), and effect on work and finance (economic) than participants with acquired retinal diseases. On the contrary, participants with acquired retinal diseases reported more inconveniences (conveniences) than participants with hereditary retinal diseases, which were mostly attributed to treatment. Participants with hereditary retinal diseases were coping better compared to participants with acquired retinal diseases.
Conclusions
Our study found that participants with both hereditary and acquired retinal diseases are living with myriad of disease-specific quality of life issues. Many of these issues are completely different and unique to each disease group. Hence, these group of diseases would need separate patient-reported outcome instruments to capture the disease-specific quality of life impacts.
Similar content being viewed by others

Background
Quality of life is severely compromised in people with major blinding retinal diseases such as age related macular degeneration and diabetic retinopathy [1,2,3,4,5,6]. Very little is known about quality of life impacts in people with other vitreoretinal diseases (i.e. hereditary degenerations, vascular occlusions, macular hole, epiretinal membrane and other vitreoretinopathies). Research exploring the impact of other vitreoretinal diseases on quality of life has been restricted by the lack of appropriate patient-reported outcome instruments. To date, only a few retina-specific patient-reported outcome instruments are available for other vitreoretinal diseases [7,8,9]. Moreover, these patient-reported outcome instruments have undergone only basic validation procedures and the content coverage is limited to measuring only a few quality of life domains (mostly activity limitation) [10]. Moreover, there are no patient-reported outcome instruments developed for vascular occlusions, macular hole and epiretinal membrane. Quality of life impacts in these retinal conditions are mostly assessed using non-disease-specific patient-reported outcome instruments (ophthalmic instruments that have been originally developed for other eye disease/s) and generic instruments (instruments developed for non-ocular diseases) [11,12,13,14,15,16,17]. In some contexts, the generic and non-disease-specific instruments (e.g., Health Utilities Index used as an outcome measure on macular degeneration and cataract surgery) have been shown to be responsive, [18,19,20,21,22] but they do not contain disease-specific items and hence may be less sensitive in assessing the quality of life impacts of people with specific diseases compared to the disease-specific instruments [10]. The lack of an appropriate retina-specific patient-reported outcome measure restricts our understanding of the full impact of these vitreoretinal diseases and their treatment on quality of life. Understanding patients’ perspective is critical as new treatment modalities such as anti-vascular endothelial growth factor intravitreal injections and gene therapy are gaining momentum especially for vascular occlusive diseases and hereditary degenerations.
The commonly occurring retinal diseases in terms of the number of patients affected such as age related macular degeneration, diabetic retinopathy, and retinal detachment deserve to have separate patient-reported outcome instruments. However, it is not feasible to develop separate patient-reported outcome instruments for the less common vitreoretinal diseases such as hereditary degenerations, vascular occlusions, and other vitreoretinopathies. Nevertheless, these less common retinal diseases do need more targeted and specific patient-reported outcome instrument/s that could accurately measure quality of life impact and be sensitive to the treatment outcomes. A way forward would be to lump or split these vitreoretinal diseases into groups based on similar quality of life issues to develop group-specific patient-reported outcome instruments.
We are developing technologically advanced patient-reported outcome measures in the form of item banks implemented via computerized adaptive testing for other vitreoretinal diseases. Item banks are a large collection of calibrated items that measure an underlying latent trait (e.g., functional limitation, emotional well-being) [23]. The computerized adaptive testing selects the items from the item banks that closely match the participant’s ability level. The computerized adaptive testing iteratively administers items based on the participant’s responses to previous questions and therefore the computerized adaptive testing requires very few items to provide a precise and accurate assessment of patient-reported outcome measures [24, 25]. Item banking implemented via computerized adaptive testing can provide solutions to the issues associated with the traditional paper-and pencil based questionnaires which are static, have limited applicability to population, outdated and do not provide a holistic assessment of quality of life [23, 26,27,28,29]. Item banks have been successfully developed and implemented in other fields of health care [30,31,32]. Item banks have been developed for other ocular diseases such as glaucoma, age related macular degeneration and diabetic retinopathy [1, 33, 34]. This study aims to qualitatively explore the quality of life issues of people with other vitreoretinal diseases to develop group-specific item banks.
Methods
The qualitative theoretical framework that was used to explore the quality of life issues of people with retinal diseases was phenomenology. Phenomenology is concerned with in-depth understanding of the participants’ lived experiences and the meanings that the participants perceive of those experience [35]. A non-probability, convenience sampling technique was used to recruit 79 participants with different retinal diseases. For adequate number of participants’ recruitment, we categorized the vitreoretinal diseases into hereditary retinal diseases and acquired retinal diseases. This was done because hereditary retinal diseases and acquired retinal diseases differ vastly in terms of the nature, age of onset, laterality, and progression of the disease. Hereditary retinal diseases tend to occur at an early age; they are mostly bilateral and progressive in nature. On the other hand, acquired retinal diseases have a late onset and mostly unilateral to begin with [36,37,38,39]. Hereditary retinal diseases includes retinitis pigmentosa, macular dystrophies, choroidal dystrophies, and other hereditary vitreoretinopathies. Acquired retinal diseases group includes relatively less common but potentially blinding retinal diseases such as vascular occlusions, macular hole, epiretinal membrane, and other rare vascular disorders. As the aim of this study was to develop item banks for other vitreoretinal diseases, we excluded people with major blinding retinal conditions such as age related macular degeneration, diabetic retinopathy and retinal detachment.
Participants for the hereditary retinal diseases group were recruited from welfare and charity organizations (The Royal Society for the Blind and Retina Australia) through emails and flyers. Participants for the acquired retinal diseases group were recruited from the retina clinics of two major metropolitan public health care facilities (The Royal Adelaide Hospital and The Queen Elizabeth Hospital). Clinical records were used to identify potential participants who were then approached to discuss their possible involvement in the study. Participants for the hereditary retinal diseases group were recruited from charity organizations and not hospitals because hereditary retinal diseases are a rare group of disorders, which are mostly untreatable and hence not commonly seen in hospitals. Hereditary retinal diseases are progressive in nature that ultimately cause blindness and participants with hereditary retinal diseases are more likely to join organizations to seek information and support. They are also more likely to take part in research. On the contrary, acquired retinal diseases are relatively common retinal conditions that are mostly treatable and so commonly seen in hospitals. Hence, participants for the acquired retinal diseases group were recruited from retina clinics. Participants who were interested in participating in the study were sent out an information pack with an invitation letter, participation information sheet, consent form and a demographic form. Upon receiving the consent form, the participants were contacted through telephone to organize a date and time for the interview. Informed consent was obtained from all individual participants included in the study. All the participants were recruited to a single in-depth interview. Ethical approval was obtained from the Southern Adelaide Clinical Human Research Ethics Committee and the study adheres to the Tenets of Declaration of Helsinki.
A semi-structured interview guide was developed from existing literature (pre-existing patient-reported outcome instruments and qualitative studies) and was validated by a panel of experts (MP, JK, KP, GS & SS). The authors JK and KP are internationally recognised experts in patient-reported outcome development and validation. They are also optometrists with extensive clinical experience. The authors MP, GJ, and SS are ophthalmologists with clinical experiences in retinal diseases. The authors MP, JK and KP are located at Flinders University and the authors GJ and SS are located at The University of Adelaide.
The aim of this semi-structured interview guide was to include questions that would help to uncover all aspects of quality of life (physical, mental, and social) (Additional file 1). One of the authors (MP) did the interviews either by face-to face or over the telephone. All interviews were audio recorded and transcribed. There was no predetermined number of participants to be recruited at the start of the study. The sampling process continued until the emerging theoretical categories were saturated.
Data analysis
The data analysis occurred after the data collection was complete. An open coding technique was adopted to analyze the textual data. In an open coding technique, the data was broken down into first level concepts, or major themes, and second-level categories, or sub-themes. For example, interviewees frequently reported difficulty in performing important day-to-day activities such as reading, driving, and playing sports. Difficulty in performing day-to-day activities became a concept or a major theme and the related things (reading, driving, and playing sports) became categories, or sub-themes (Fig. 1). One of the authors (MP) did the coding. Once the coding was completed, the concepts and the categories were re-assessed by the authors (JK & KP) to decide whether they formed major or sub themes. Any discrepancies between the authors were resolved by discussion. Comparison within and between the two groups (hereditary retinal diseases vs acquired retinal diseases) were carried out based on number of issues (i.e. coded by nodes) identified across common themes. The qualitative software program QSR NVivo 11 (QSR International Pty Ltd) was used to systematically code the transcripts.

Process of data analysis and themes development
Results
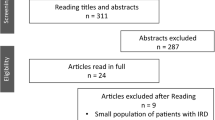
Seventy-nine semi-structured interviews were conducted with participants with hereditary retinal disease (n = 32) and acquired retinal diseases (n = 47). In the acquired retinal diseases group, 80 participants were approached, 15 participants declined, 13 participants were excluded from the study (could not speak English = 6, hearing loss = 4, had multiple ocular comorbidities = 3) and 5 did not show interest in participating in the study. In the hereditary retinal diseases group, 41 participants were approached and 9 declined to participate. Participants in the hereditary retinal diseases group were younger, mostly working, had bilateral eye diseases and more visually impaired compared to the participants with acquired retinal diseases who were older, had unilateral eye disease, and were mostly retired and less visually impaired (Table 1). The hereditary retinal diseases group comprised of retinitis pigmentosa (n = 23), cone dystrophy (n = 2) and macular dystrophy (n = 7) and the acquired retinal diseases group comprised of vascular occlusions (n = 18), epiretinal membrane (n = 20) and macular hole (n = 9).
We identified nine quality of life themes (domains) relevant to both the groups. The themes were: (1) difficulty in performing important day-to-day activities (activity limitation), (2) facing emotional and psychological challenges (emotional well-being), (3) struggle with social interaction (social well-being), (4) having a myriad of ocular and visual symptoms (symptoms), (5) concerns about health, disease outcome and personal safety (health concerns), (6) problems with mobility and orientation (mobility), (7) inconveniences associated with eye condition (conveniences), (8) effect on work and finance (economic), and (9) coping with the eye condition (coping). These themes were further synthesized to identify whether they could emerge as important domains of ophthalmic quality of life. These themes conform to the existing ophthalmic quality of life domains proposed by our group.
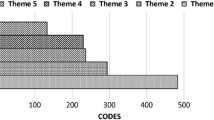
Generally, the hereditary retinal diseases group had expressed more issues (denoted by number of coded segments) across all domains except one than the acquired retinal diseases group (Fig. 2). Activity limitation was the most prominent quality of life issue among participants with hereditary retinal diseases and health concerns was the most prominent quality of life issue among participants with acquired retinal diseases (Fig. 2). We compared the quality of life issues between the two groups to identify common and unique issues. Common and unique issues were based on the iteration. Common issues are quality of life issues that were reported in both the groups and unique issues were those, which were reported in only one group. Within the groups, the quality of life issues were similar. More than 80% of the quality of life issues were common between retinitis pigmentosa, cone dystrophy and macular dystrophy and more than 70% of the issues were common between vascular occlusion, epiretinal membrane and macular hole.

Quality of life (QoL) themes/domains in hereditary retinal diseases (HRD) and acquired retinal diseases (ARD). Codes = number of times the issue was discussed across all the transcripts analyzed. X-axis represents QoL themes/domains and Y-axis represents number of coded segments for each QoL theme/domain. AL, activity limitation; CV, convenience; EM, emotional well-being; HC, health concerns; MB, mobility; SC, social well-being; SY, symptoms; EC, economic; CP, coping
However, between the disease groups, some of the quality of life issues were common, but overall; we found that many of the quality of life issues were unique to the disease groups.
The quality of life issues in people with hereditary retinal diseases and acquired retinal diseases are discussed below.
Theme 1: People with both acquired retinal diseases and hereditary retinal diseases had trouble in performing important day-to-day activities (Activity limitation)
Activity limitation was identified as the major quality of life issue in participants with hereditary retinal diseases (Fig. 2). The major activity limitations were difficulty in reading, driving, seeing in poor lighting conditions, shopping, using computers and playing sports. They reported difficulty in reading small prints, numbers, and labels. Most participants expressed that using large print books or voice-activated books enabled them to continue reading. Difficulties in being able to see at night caused frustrations. Not being able to drive was reported as a big loss as they had to depend on friends or family members for daily commute (Table 2). Frequent re-organizing or re-arranging things in the supermarket and inability to read price tags made shopping a huge challenge. They also reported difficulty in playing outdoor games especially ball games.
In the acquired retinal diseases group, activity limitation was only the fourth biggest issue (Fig. 2). The major activity limitations in this group were difficulty in reading, driving, watching television, and engaging in leisure activities (Table 2). They reported difficulty especially reading fine prints and street/road signs. In contrast to people with hereditary retinal diseases who had difficulty in playing outdoor games, people with acquired retinal diseases had difficulties in playing indoor games such as board games and doing puzzles. In contrast to people with hereditary retinal diseases who could not drive, people with acquired retinal diseases were driving but expressed that driving had become challenging especially at night. As these eye conditions predominantly involved the central retina, they often reported difficulty in recognizing people’s faces.
Theme 2: Participants with both hereditary retinal diseases and acquired retinal diseases faced emotional and psychological challenges (Emotional well-being)
Participants with both hereditary retinal diseases and acquired retinal diseases expressed positive and negative emotional comments. However, people with hereditary retinal diseases expressed more negative comments than positive comments. The commonly expressed emotional comments in the hereditary retinal diseases group were frustration, anxiety, shock, depression, and anger. There was an inability to do things like others such as to read, to drive and to find a suitable job, which often resulted in frustrations. Having to keep up with the technology and not knowing how their eye conditions were going to progress caused anxiety. They expressed that being diagnosed as legally blind was more shocking than being diagnosed with the eye condition. Uncertainty about the future and having to lose their driving license caused depression.
In contrast to participants with hereditary retinal diseases, participants with acquired retinal diseases were more optimistic about their eye condition. They believed that treatment would make their eye condition better. Participants whose vision had not improved with treatment worried about losing their sight and involvement of the other eye. Having to wait for long hours in the clinics, frequent eye appointments and repeated eye tests were some of the reasons for their frustrations. They feared the repeated eye injections and laser treatments.
Theme 3: Participating in social activities was problematic (Social well-being)
People with hereditary retinal diseases reported difficulties with social interaction. They experienced more difficulty in getting help and support from friends and family members compared to participants with acquired retinal diseases. Some participants experienced strain in their personal relationship especially with their partners due to their eye condition. Despite the lack of support, many expressed that they overcame the hurdles by learning strategies to be independent. Difficulty in recognizing faces, social cues and body language made them feel isolated in social gatherings. They frequently associated themselves with societies/government organizations to keep themselves updated about their eye condition.
Participants with acquired retinal diseases did not have to rely as much on friends and family members for support. Meeting up regularly with family members and friends and being part of social activity groups such as Facebook groups, church groups and book clubs were some of the social activities among them. The participants shared that they had often discussed their eye condition with their family members to increase awareness.
Theme 4: Concerns about health and safety were significant (Health concerns)
Health concern was a major issue in both the disease groups and was the major quality of life issue in the acquired retinal diseases group (Fig. 2). Participants in the hereditary retinal diseases group were often concerned about accidents such as falling, tripping, and bashing into things due to their limited peripheral vision. Many of them articulated that their experiences with their specialist were unpleasant, as they felt that their specialists could not understand their visual loss. They often worried about going blind and having to live on their own. Generally, this group of participants felt that their friends and family members did not understand their visual impairment. Not knowing what is going to happen in the future, fear of passing the disease to the kids, and fear of losing their partners were some of the other important concerns in this group.
Most participants in the acquired retinal diseases group were not aware of their eye condition before diagnosis. In most of them, an optometrist diagnosed their eye condition on routine examination. They expressed unhappiness towards their medical service providers who often did not communicate well about their disease/s. Treatment outcomes were the main concern among participants who were undergoing treatments. Participants with treatment failure expressed concerns about the possibilities of disease recurrence.
Theme 5: Visual symptoms were abundant in both the groups (Symptoms)
Participants in both the disease groups reported a myriad of visual symptoms. Night blindness, restricted field of vision, difficulty in discerning colours and difficulty in light adaptation were the prominent symptoms in retinitis pigmentosa [40] and difficulty with central vision was the prominent symptom in macular dystrophies.
Difficulty with central vision was common to participants with vascular occlusion, epiretinal membrane and macular hole. Individuals with vascular occlusions experienced sudden loss of vision, distortion of vision and seeing floaters. Eye pain and bloodshot eyes were reported after receiving anti-vascular endothelial growth factor eye injections. Participants with epiretinal membrane reported distortion of vision and difficulty in focussing. Participants who have undergone vitrectomy and gas tamponade reported double vision and wobbly vision.
Theme 6: Problems with mobility and orientation (Mobility)
Mobility was a major issue in participants with hereditary retinal diseases especially in retinitis pigmentosa [40]. They often reported difficulty walking outdoors, walking in a cluttered environment and navigation in unfamiliar places. They also reported difficulty using steps and escalators. Stepping on or off a train or a tram was a challenge. Difficulty in negotiating obstacles while walking and difficulty in navigating in the dark/night were some of the mobility difficulties unique among these participants.
The major mobility difficulties among participants with acquired retinal diseases were crossing a street/road, walking in the dark/night, and walking on uneven grounds. Difficulty in walking on uneven grounds and negotiating bumps/cracks in the path were some unique mobility difficulties in this group.
Theme 7: Impact on work and finance (Economic)
Work and finance was one of the major issues among the participants with hereditary retinal diseases because most of them were young and working (Table 1). Participants in this group reported that they were unable to pursue the career of their choice. Not being able to get employment often caused fear and anxiety. Lack of mobility and inability to drive restricted their job opportunities. They also reported difficulty in getting help and support from government and other social welfare organizations. Costs associated with looking after guide dogs and attending training courses were some of the other financial implications specific to participants with hereditary retinal diseases.
Participants with acquired retinal diseases had less job-related constraints due to their eye disease as most of them were retired. Some of the financial implications were due to the costs associated with seeing a specialist, costs associated with buying medications and undergoing eye procedures.
Theme 8: Inconveniences in day-to-day life were very common (Conveniences)
Participants with both hereditary retinal diseases and acquired retinal diseases reported myriad of inconveniences for having to live with their diseases. Between two groups, participants with acquired retinal diseases expressed more inconveniences in their day-to-day life (Fig. 2). Most of the inconveniences in participants with acquired retinal diseases were associated with their treatment. Having to keep face/head position (e.g. face down positioning after vitrectomy) for a prolonged time was reported as a major inconvenience by participants with epiretinal membrane and macular hole. Those individuals with vascular occlusions reported that the major inconveniences were undergoing repeated laser treatment, injections and having repeated eye tests. Long waiting hours in the clinic and having to go for frequent eye appointments were some of inconveniences unique to this group.
The major inconveniences in the hereditary retinal diseases group often resulted from having to depend on others for transportation and travelling by public transport. Not being able to read without assistance was also a major inconvenience. Inability to participate in things spontaneously and losing or misplacing things frequently were some of the other inconveniences.
Theme 9: Despite all the odds many participants coped well (Coping)
The use of coping strategies to manage the stress of vision loss was common in both the disease groups. Participants with hereditary retinal diseases were coping better compared to participants with acquired retinal diseases. Most of the participants learned to accept their eye condition and maintained a positive attitude. The participants also kept themselves distracted by engaging in useful activities such as listening to audio books, playing sports, and engaging in adventurous activities such as skydiving, skiing and SCUBA diving. Some of them learned to understand the diseases, which helped them to deal with it. Being independent also helped them to get on with life. Seeing other family members adapt to the eye condition also helped them to cope better.
Attributing their eye condition to ageing was a common coping response used by participants with acquired retinal diseases. The other coping responses were trying to ignore their eye condition and indulging in engaging activities such as knitting, reading and gardening. Trusting their doctors, praying, and meditating were some of the unique coping strategies in this group.
Discussion
Our study revealed that participants with hereditary retinal diseases experience more quality of life issues compared to participants with acquired retinal diseases. Participants with hereditary retinal diseases were more visually impaired compared to participants with acquired retinal diseases and that could be one of the reasons for a greater number of quality of life issues iterated in the hereditary retinal diseases group. The quality of life themes/domains across the disease groups were identical, but when compared with the domains specific issues, they were mostly different. The apparent differences could be due to the differences in the disease in terms of age of onset, duration of the disease, severity of visual loss and employment status. In the hereditary retinal diseases group, the predominant loss of vision was peripheral and binocular, however, in the acquired retinal diseases group; it was mostly central and monocular. The duration of the disease was longer in hereditary retinal diseases and shorter in acquired retinal diseases. Most of the participants in the hereditary retinal diseases group were working and most of the participants in the acquired retinal diseases group were retired (Table 1). Participants with hereditary retinal diseases had severe visual impairment and participants with acquired retinal diseases had only mild to moderate visual impairment. The quality of life issues of people with retinitis pigmentosa has been previously published [40], in this paper we are comparing the quality of life issues of people with hereditary retinal diseases and acquired retinal diseases .
The nine domains were determined from the emerging themes during the analysis. These domains conform to the important ophthalmic domains of quality of life identified in other eye diseases [1, 5, 33, 34]. We found stark differences in types of quality of life issues across these domains between acquired retinal diseases and hereditary retinal diseases. The most prominent quality of life parameter among participants with hereditary retinal diseases was activity limitation, which might be attributed to the fact that participants with hereditary retinal diseases had bilateral eye condition and living with severe visual impairment. On the contrary, health concerns (e.g. concerns of going blind, treatment outcomes etc.) was the prominent quality of life issue in acquired retinal diseases. This could be because most of the acquired retinal diseases are acute and treatable. Similarly, participants with hereditary retinal diseases continuously face progressive loss of vision, which may be one of the reason they express negative emotional comments much more than when compared to positive comments. Frustration, worry, shock, and depression were some of the commonly expressed emotional comments in our study and similar findings were reported in previous studies [41, 42].
Participants with hereditary retinal diseases had more issues with social interaction and mobility compared to participants with acquired retinal diseases. Inability to identify social clues, facial expressions, body language and difficulty in participating in social activities at night affected the social life of participants with hereditary retinal diseases. The mobility issues may be attributable to the loss of the peripheral visual field. Effect on work and finance was an important quality of life theme among participants with hereditary retinal diseases. They had greater economic and financial impacts due to their diseases compared to participants with acquired retinal diseases because most of these participants were working (Table 1). The economic effects may not be part of the health related quality of life but forms a part of quality of life, which is a broader concept than health related quality of life. Participants with hereditary retinal diseases were symptomatic than participants with acquired retinal diseases because hereditary retinal diseases are progressive diseases. Night blindness, progressive visual field loss and difficulty in light adaptation were the common symptoms reported by participants with retinitis pigmentosa in this study [40]. In contrast, a previous study has reported a different set of symptoms (day-to-day visual fluctuations, intermittent diplopia, photopsia, high glare and visual hallucinations) [42].
The type of coping strategies used by an individual depends on the situation they must face. Coping that implies a positive attitude has shown to improve health related quality of life and a passive attitude has shown to worsen the health related quality of life [43, 44]. The coping strategies used by participants with hereditary retinal diseases mostly implied positive attitude (e.g. trying to be positive and acceptance of their eye condition). The coping strategies used by participants with acquired retinal diseases implied passive attitude (e.g. trying not to think about their eye condition and attributing their eye disease to ageing). Participants with hereditary retinal diseases were reported to cope better than participants with acquired retinal diseases as they used positive attitude.
Despite the low prevalence, hereditary retinal diseases and acquired retinal diseases can lead to severe visual impairment and blindness. As new advancements in treatments for hereditary retinal diseases and acquired retinal diseases such as anti-vascular endothelial growth factor injections and gene therapy continue to gain momentum, a comprehensive patient-reported outcome instrument will be invaluable for use in clinical trials to compare the impact of novel treatment modalities from patients’ perspective. However, there are no comprehensive and widely validated patient-reported outcome instrument for these diseases. The way forward is to develop one for each retinal disease. However, it is not feasible to do so because there are too many retinal diseases with low prevalence rate in general population. The best way forward is to lump/split these diseases into groups.
The results of this study provide a scientific basis for splitting vs lumping less common but potentially blinding retinal diseases to develop retina-specific patient-reported outcome instruments. There are several ways of lumping/splitting the retinal diseases. One way is to group them based on the disease pathology into congenital, vascular, infection/inflammatory, trauma and tumours. This type of grouping would create many disease groups and affect the sample size of the groups. The second way is to split them into central retinal diseases and peripheral retinal diseases based on the anatomical location of the disease. The problem with this lumping is that some retinal diseases involve both the central and the peripheral retina and hence may be difficult to group. The third and a simple way would be to lump all the inherited degenerations together and acquired retinal diseases together. Hereditary retinal diseases differ from acquired retinal diseases in the onset, presentation, and manifestation. The division into hereditary retinal diseases and acquired retinal diseases is also supported by our qualitative findings, which compared quality of life issues within and between these two groups. Putting together these findings, we could argue that a single patient-reported outcome instrument would not serve both the disease groups. Therefore, we propose to split other vitreoretinal diseases into two groups for the sake of developing group-specific patient-reported outcome instruments.
This study had some limitations. The method of data collection was interviews and not focus groups. Focus groups are the gold standard method for exploring people’s feelings, motivations, insight, and experience on any topic. As this study involved uncommon retinal conditions, organizing focus groups was difficult. The other limitation was that the hereditary retinal diseases group had fewer people with macular dystrophies and cone dystrophies than retinitis pigmentosa. This could have contributed to some bias in the data interpretation. Having equal number of participants with cone dystrophy and macular dystrophies could have avoided the bias. However, macular dystrophies and cone dystrophies are relatively uncommon inherited retinal disorders and it was difficult to have an equal number of participants with these retinal conditions in this group. Moreover, the acquired retinal diseases group had only participants with vascular occlusions, macular hole and epiretinal membrane and did not have participants with other retinal condition such hemoglobinopathies. This might limit the relevance and generalizability of our findings to all acquired retinal diseases.
Conclusions
Quality of life are different between the two disease groups, which may be due to the difference in the onset, presentation, and manifestation of the retinal diseases. Hence, these two disease groups would need separate patient-reported outcome instruments to capture group-specific quality of life impact.
References
McCloud, C., Khadka, J., Gilhotra, J. S., & Pesudovs, K. (2014). Divergence in the lived experience of people with macular degeneration. Optom Vis Sci, 91, 966–974.
Wong, E. Y. H., Guymer, R. H., Hassell, J. B., & Keeffe, J. E. (2004). The experience of age-related macular degeneration. J Visual Impair Blin, 98, 629–640.
Moore, L. W. (2000). Severe visual impairment in older women. West J Nurs Res, 22, 571–588 discussion 588-595.
Moore, L. W., & Miller, M. (2003). Older men’s experiences of living with severe visual impairment. J Adv Nurs, 43, 10–18.
Fenwick, E. K., Pesudovs, K., Khadka, J., Dirani, M., Rees, G., Wong, T. Y., & Lamoureux, E. L. (2012). The impact of diabetic retinopathy on quality of life: qualitative findings from an item bank development project. Qual Life Res, 21, 1771–1782.
Coyne, K. S., Margolis, M. K., Kennedy-Martin, T., Baker, T. M., Klein, R., Paul, M. D., & Revicki, D. A. (2004). The impact of diabetic retinopathy: perspectives from patient focus groups. Fam Pract, 21, 447–453.
Turano, K. A., Geruschat, D. R., Stahl, J. W., & Massof, R. W. (1999). Perceived visual ability for independent mobility in persons with retinitis pigmentosa. Invest Ophthalmol Vis Sci, 40, 865–877.
Szlyk, J. P., Fishman, G. A., Alexander, K. R., Revelins, B. I., Derlacki, D. J., & Anderson, R. J. (1997). Relationship between difficulty in performing daily activities and clinical measures of visual function in patients with retinitis pigmentosa. Arch Ophthalmol, 115, 53–59.
Szlyk, J. P., Seiple, W., Fishman, G. A., Alexander, K. R., Grover, S., & Mahler, C. L. (2001). Perceived and actual performance of daily tasks: relationship to visual function tests in individuals with retinitis pigmentosa. Ophthalmology, 108, 65–75.
Prem Senthil, M., Khadka, J., Pesudovs, K. (2017). Assessment of patient-reported outcomes in retinal diseases: a systematic review. Surv Ophthalmol, 62, 546-582.
Tranos, P. G., Ghazi-Nouri, S. M., Rubin, G. S., Adams, Z. C., & Charteris, D. G. (2004). Visual function and subjective perception of visual ability after macular hole surgery. Am J Ophthalmol, 138, 995–1002.
Fukuda, S., Okamoto, F., Yuasa, M., Kunikata, T., Okamoto, Y., Hiraoka, T., & Oshika, T. (2009). Vision-related quality of life and visual function in patients undergoing vitrectomy, gas tamponade and cataract surgery for macular hole. Br J Ophthalmol, 93, 1595–1599.
Ghazi-Nouri, S. M., Tranos, P. G., Rubin, G. S., Adams, Z. C., & Charteris, D. G. (2006). Visual function and quality of life following vitrectomy and epiretinal membrane peel surgery. Br J Ophthalmol, 90, 559–562.
Okamoto, F., Okamoto, Y., Hiraoka, T., & Oshika, T. (2009). Effect of vitrectomy for epiretinal membrane on visual function and vision-related quality of life. Am J Ophthalmol, 147, 869–874 874 e861.
Conrad, R., Weber, N. F., Lehnert, M., Holz, F. G., Liedtke, R., & Eter, N. (2007). Alexithymia and emotional distress in patients with central serous chorioretinopathy. Psychosomatics, 48, 489–495.
Brown, D. M., Heier, J. S., Clark, W. L., Boyer, D. S., Vitti, R., Berliner, A. J., Zeitz, O., Sandbrink, R., Zhu, X., & Haller, J. A. (2013). Intravitreal aflibercept injection for macular edema secondary to central retinal vein occlusion: 1-year results from the phase 3 COPERNICUS study. Am J Ophthalmol, 155, 429–437 e427.
Deramo, V. A., Cox, T. A., Dyed, A. B., Lee, P. P., & Fekrat, S. (2003). Vision-related quality of life in people with central retinal vein occlusion using the 25-item national eye institute visual function questionnaire. Arch Ophthalmol, 121, 1297–1302.
Asakawa, K., Rolfson, D., Senthilselvan, A., Feeny, D., & Johnson, J. A. (2008). Health Utilities index mark 3 showed valid in Alzheimer disease, arthritis, and cataracts. J Clin Epidemiol, 61, 733–739.
Espallargues, M., Czoski-Murray, C. J., Bansback, N. J., Carlton, J., Lewis, G. M., Hughes, L. A., Brand, C. S., & Brazier, J. E. (2005). The impact of age-related macular degeneration on health status utility values. Invest Ophthalmol Vis Sci, 46, 4016–4023.
Feeny, D., Spritzer, K., Hays, R. D., Liu, H., Ganiats, T. G., Kaplan, R. M., Palta, M., & Fryback, D. G. (2012). Agreement about identifying patients who change over time: cautionary results in cataract and heart failure patients. Med Decis Mak, 32, 273–286.
Groessl, E. J., Liu, L., Sklar, M., Tally, S. R., Kaplan, R. M., & Ganiats, T. G. (2013). Measuring the impact of cataract surgery on generic and vision-specific quality of life. Qual Life Res, 22, 1405–1414.
Kaplan, R. M., Tally, S., Hays, R. D., Feeny, D., Ganiats, T. G., Palta, M., & Fryback, D. G. (2011). Five preference-based indexes in cataract and heart failure patients were not equally responsive to change. J Clin Epidemiol, 64, 497–506.
Pesudovs, K. (2010). Item banking: a generational change in patient-reported outcome measurement. Optom Vis Sci, 87, 285–293.
Wainer, H. (2000). Computerized adaptive testing. A primer. Mahway: Lawerance Erlbaum.
Wang, Y. C., Hart, D. L., Cook, K. F., & Mioduski, J. E. (2010). Translating shoulder computerized adaptive testing generated outcome measures into clinical practice. J Hand Ther, 23, 372–382.
Khadka, J., Pesudovs, K., McAlinden, C., Vogel, M., Kernt, M., & Hirneiss, C. (2011). Reengineering the glaucoma quality of life-15 questionnaire with rasch analysis. Invest Ophthalmol Vis Sci, 52, 6971–6977.
Lundstrom, M., & Pesudovs, K. (2011). Questionnaires for measuring cataract surgery outcomes. J Cataract Refract Surg, 37, 945–959.
McAlinden, C., Gothwal, V. K., Khadka, J., Wright, T. A., Lamoureux, E. L., & Pesudovs, K. (2011). A head-to-head comparison of 16 cataract surgery outcome questionnaires. Ophthalmology, 118, 2374–2381.
Gothwal, V. K., Wright, T. A., Lamoureux, E. L., & Pesudovs, K. (2009). Rasch analysis of visual function and quality of life questionnaires. Optom Vis Sci, 86, 1160–1168.
Lai, J. S., Cella, D., Dineen, K., Bode, R., Von Roenn, J., Gershon, R. C., & Shevrin, D. (2005). An item bank was created to improve the measurement of cancer-related fatigue. J Clin Epidemiol, 58, 190–197.
Kopec, J. A., Sayre, E. C., Davis, A. M., Badley, E. M., Abrahamowicz, M., Sherlock, L., Williams, J. I., Anis, A. H., & Esdaile, J. M. (2006). Assessment of health-related quality of life in arthritis: conceptualization and development of five item banks using item response theory. Health Qual Life Outcomes, 4, 33.
Jette, A. M., Slavin, M. D., Ni, P., Kisala, P. A., Tulsky, D. S., Heinemann, A. W., Charlifue, S., Tate, D. G., Fyffe, D., Morse, L., Marino, R., Smith, I., & Williams, S. (2015). Development and initial evaluation of the SCI-FI/AT. J Spinal Cord Med, 38, 409–418.
Fenwick, E. K., Pesudovs, K., Khadka, J., Rees, G., Wong, T. Y., & Lamoureux, E. L. (2013). Evaluation of item candidates for a diabetic retinopathy quality of life item bank. Qual Life Res, 22, 1851–1858.
Khadka, J., McAlinden, C., Craig, J. E., Fenwick, E. K., Lamoureux, E. L., & Pesudovs, K. (2015). Identifying content for the glaucoma-specific item bank to measure quality-of-life parameters. J Glaucoma, 24, 12–19.
Benner P. (1994). Interpretive phenomenology: Embodiment, caring, and ethics in health and illness. California: Sage publications.
Laouri, M., Chen, E., Looman, M., & Gallagher, M. (2011). The burden of disease of retinal vein occlusion: review of the literature. Eye (Lond), 25, 981–988.
McCarty, D. J., Mukesh, B. N., Chikani, V., Wang, J. J., Mitchell, P., Taylor, H. R., & McCarty, C. A. (2005). Prevalence and associations of epiretinal membranes in the visual impairment project. Am J Ophthalmol, 140, 288–294.
Lewis, M. L., Cohen, S. M., Smiddy, W. E., & Gass, J. D. (1996). Bilaterality of idiopathic macular holes. Graefes Arch Clin Exp Ophthalmol, 234, 241–245.
Leavitt, J. A., Larson, T. A., Hodge, D. O., & Gullerud, R. E. (2011). The incidence of central retinal artery occlusion in Olmsted County, Minnesota. Am J Ophthalmol, 152, 820–823 e822.
Prem Senthil, M., Khadka, J., & Pesudovs, K. (2017). Seeing through their eyes: lived experiences of people with retinitis pigmentosa. Eye (Lond), 31, 741–748.
Fourie, R. J. (2007). A qualitative self-study of retinitis pigmentosa. Br J Vis Impair, 25, 217–232.
Bittner, A. K., Edwards, L., & George, M. (2010). Coping strategies to manage stress related to vision loss and fluctuations in retinitis pigmentosa. Optometry, 81, 461–468.
Rinaldi, S., Ghisi, M., Iaccarino, L., Zampieri, S., Ghirardello, A., Sarzi-Puttini, P., Ronconi, L., Perini, G., Todesco, S., Sanavio, E., & Doria, A. (2006). Influence of coping skills on health-related quality of life in patients with systemic lupus erythematosus. Arthritis Rheum, 55, 427–433.
Savelkoul, M., de Witte, L. P., Candel, M. J., van der Tempel, H., & van den Borne, B. (2001). Effects of a coping intervention on patients with rheumatic diseases: results of a randomized controlled trial. Arthritis Rheum, 45, 69–76.
Acknowledgments
We would like to thank all the staffs of The Royal Adelaide Hospital, The Queen Elizabeth Hospital, and Flinders Vision. We would like to acknowledge all the members of The Royal Society for the Blind and members of Retina Australia (QLD, VC, WA, NSW, ACT). We would also like to thank our research assistant Susan Aldhous.
Funding
This study is funded by National Health and Medical Research Council (grant no.1031838).
Mallika Prem Senthil is supported by the Australian Government Research Training Scholarship program.
Availability of data and materials
The data will not be shared as it contains confidential information about the participants.
Author information
Authors and Affiliations
Contributions
MPS Contributed to the conception of the work, data collection, data analysis and interpretation, drafting the manuscript, revision, proof editing and submission. JK Contributed to the design of the work, data interpretation, manuscript evaluation, revisions and final approval. JSG Data interpretation, editing and final approval of the manuscript. SS Data interpretation, revision, editing and final approval of the manuscript. KP Contributed to the conception of the work, editing and final approval of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Authors’ information
MP is an ophthalmologist pursuing her PhD at Optometry and Vision Science, Flinders University, Adelaide. Her research is about understanding the quality of life issues among patients with retinal diseases and developing and validating technologically advanced survey questionnaires to measure quality of life impacts among these patients. JK is a research associate in Optometry and Vision Science, Flinders University. KP is the Foundation Chair of Optometry and Vision Science. The authors JK and KP are internationally recognised experts in PRO development and validation. JK and KP are also optometrists with an extensive clinical experience. JG and SS are retinal specialist at the University of Adelaide.
Ethics approval and consent to participate
Ethical approval was obtained from the Southern Adelaide Clinical Human Research Ethics Committee and the corresponding ethics committees at health care facilities (469.11) and the study adheres to the Tenets of Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
Semi-structured interview guide for hereditary retinal diseases/acquired retinal diseases. (DOCX 19 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Prem Senthil, M., Khadka, J., Gilhotra, J.S. et al. Exploring the quality of life issues in people with retinal diseases: a qualitative study. J Patient Rep Outcomes 1, 15 (2017). https://doi.org/10.1186/s41687-017-0023-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41687-017-0023-4