
Abstract
Background
Low-grade inflammation plays significant role in the development of diabetes mellitus type 2 (DM2) and impaired glucose tolerance (IGT), but immune regulatory mechanisms involved in these processes are studied incompletely. The purpose of the present study was to characterize the subsets of T-helper-1 (Th1), Th17 and T-regulatory lymphocytes (Treg) in hypertensive patients with DM2 or IGT according to the clinical variant of the disease.
Methods
Hypertensive patients with DM2 (n = 20) and IGT (n = 7) were recruited in the study. Hypertensive patients without carbohydrate disturbances (n = 7) and healthy volunteers (n = 12) constituted comparison groups. All patients underwent thorough clinical examination. Th1-, Th17- and Th1/Th17-lymphocytes were assessed in peripheral blood mononuclear cells (PBMC) according to intracellular production of interferon (IFN)-γ and interleukin (IL)-17. Expression of receptor to IL-23 (IL-23R) by PBMC was evaluated. Treg-lymphocytes were detected in PBMC by expression of transcription factor FoxP3. Cells were analyzed using flow cytometry.
Results
We found that ratio Treg/Th17 was lower and numbers of IL-23R-positive cells were higher in hypertensive patients with IGT. Patients with DM2 were characterized by elevated numbers of Th17-lymphocytes in intact PBMC culture and Th1-lymphocytes after PBMC activation, as well as decreased ratios Treg/Th17 and Treg/Th1, and reduced numbers of Tregs that were inversely related to visceral adiposity index. In hypertensive patients with DM2 glomerular filtration rate was related to numbers of intact Th17- and IL-23R+ cells and FoxP3+ Treg-lymphocytes, while values of Treg/Th1 ratio were interconnected with visceral adiposity index and concentrations of total cholesterol and LDL-cholesterol.
Conclusions
Our study underlines the importance of immune imbalance in the development of carbohydrate metabolism perturbations in hypertensive patients even at the stage of impaired glucose tolerance. Further prospective research is needed to elaborate the possible strategy of the risk evaluation for hypertensive DM2 and IGT patients according to their current inflammatory status and propose therapeutic approaches for its correction.
Similar content being viewed by others


Background
The presence of diabetes mellitus type 2 (DM2) in patients with arterial hypertension (AH) significantly amplifies development of microvascular and macrovascular complications, and results in increased mortality [1, 2]. DM2 is an independent risk factor for the development of cardiovascular events [3, 4]. The risk of infarction and coronary heart disease death in DM2 patients is as high as in patients with the history of previous myocardial infarction [5, 6]. The widespread of DM2, observed nowadays, may partially be explained by the fact that people with impaired glucose tolerance (IGT, may also be referred as “prediabetes”) remain undiagnosed [3]. During IGT the regulation of carbohydrate metabolism is already disturbed, but the fasting glucose and glycated hemoglobin (HbA1c) levels are lower than those observed during DM, or may even remain in the range of normal values [7]. IGT precedes the development of DM2 in 25 % of cases, and patients with IGT also have high risk of vascular complications [3, 7].
It had been shown that chronic low-grade inflammation plays significant role in the development of DM2 and insulin resistance, but its mechanisms are not yet thoroughly explored [8–10]. There is no general consensus if inflammation during DM2 has pathogenic role or may fulfill the protective function, while its agents may be regarded as biomarkers of the disease [11, 12]. Macrophages are considered to be the main effector cells during metabolic inflammation during DM2 and its complications [13]. However it had been shown that T-lymphocytes may also be found in the adipose tissue, kidney parenchyma and other target tissues during DM2 [14, 15]. These findings confirmed that cells of adaptive immunity may act as important regulators during the development of DM2-associated inflammation.
Imbalance between inflammatory T-helper subpopulations (Th17 and Th1) and immunosuppressive regulatory T-lymphocytes (Tregs) had proven to be of great significance in many diseases accompanied by inflammation, such as rheumatoid arthritis, systemic sclerosis, diabetes mellitus type 1, acute coronary syndrome etc. [16–18]. Among the consequences of imbalance between proinflammatory T-helpers and Tregs one may list elevated production of inflammatory cytokines, predisposition to autoimmunity, increased autoantibody production [19, 20]. All these factors are favorable for the creation of inflammatory milieu and may contribute to the development and maintenance of insulin resistance during DM2 [8–10].
Multiple experimental works specify association of insulin resistance, obesity and increased numbers of Th17, as well as Th1 lymphocytes, together with reduction of FoxP3+ Tregs’ frequency in adipose tissue and spleen [21, 22]. But we have encountered just a limited number of studies exploring functioning of Th17 and Treg cells in DM2 patients, where the clinical implications of immune dysregulation were not sufficiently addressed [23, 24]. It had been shown that functioning of Th17-lymphocytes has its peculiarities in humans compared to mice, that is why not all the data obtained in experimental models of DM2 and AH can be extrapolated into patients’ cohort [25]. To our knowledge no works were undertaken to estimate the functional activity of Th1/Th17/Treg-lymphocytes in patients with IGT.
The purpose of the present study was to characterize the subsets of Th1, Th17 and Treg-lymphocytes in hypertensive patients with DM2 or IGT, and to conduct analysis of relationships between immune dysregulation and clinical features of patients with DM2.
Methods
Patients
The study protocol was approved by the local Biomedical Ethics Committee of RI Cardiology (protocol number 62 from 07.04.2010). All the patients gave the informed consent to participate in the study. All the procedures were performed in accordance with the Helsinki Declaration, Good Clinical Practice (GCP) and Good Laboratory Practice (GLP).
During the case–control study all the patients were stratified into 3 groups: hypertensive patients with DM2, hypertensive patients with IGT and hypertensive patients without carbohydrate disturbances (constituted comparison group). Control group of healthy volunteers was also recruited and constituted the fourth group. Characteristics of patients and healthy volunteers are represented in Table 1.
All patients recruited in the study received regular antihypertensive therapy, including combination of renin-angiotensin-aldosterone system blockers (83 % AH patients; 65 % DM2 patients and 71 % IGT patients), indapamide retard (67 % AH patients; 45 % DM2 patients and 57 % IGT patients), calcium channel blockers (33 % AH patients; 40 % DM2 patients and 14 % IGT patients), beta-blockers (17 % AH patients; 30 % DM2 patients and 30 % IGT patients). 10 recruited patients (29 % of all patients) received low doses of statins (atorvastatin in the mean dose 15 mg and rosuvastatin in the mean dose 7.5 mg). 70 % DM2 patients received oral glucose-lowering medications, including biguanides and sulphonylurea derivatives. Healthy volunteers did not receive any medication at least 3 weeks prior to the recruitment in the study.
Glomerular filtration rate (GFR) was calculated using Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation. All the patients and healthy volunteers recruited in the study had preserved renal function with GFR > 60 ml/min/1.73 m2.
Visceral index of adiposity (VAI) was calculated using the formula for male patients: VAI = (WC/(39.68 + (1.88 x BMI))) x (TG/1.03) x (1.31/HDL); for female patients: VAI = (WC/(36.58 + (1.89 x BMI))) x (TG/0.81) x (1.52/HDL), where WC – waist circumference; BMI – body mass index [26].
Fasting samples of peripheral blood were obtained into 4 ml heparinized tubes, 4 ml tubes with EDTA and in 10 ml tubes without anticoagulant.
Biochemical analyses
Insulin and C-peptide concentrations were evaluated in serum by enzyme-linked immunosorbent assay (AccuBind, USA; Diagnostic System Laboratories, USA). Serum concentration of glucose was measured by glucose oxidase method using analyzer BIOSEN C-line Clinic (EKF diagnostic, Germany). Enzyme colorimetric method was used to estimate serum concentration of total cholesterol, triacylglycerol, high-density lipoprotein (HDL) cholesterol (Diakon, Russia). Concentration of low-density lipoprotein (LDL) cholesterol (using formula [LDL] = [Total cholesterol] – [Triacylglycerol (TG)] – [HDL]) and LDL/HDL ratio was calculated. Glycated hemoglobin (HbA1c) content was measured by immunoturbidimetric method (DiaSys, Germany).
Homeostatic model assessment for insulin resistance (HOMA) was calculated according to equation: HOMA = ([fasting glucose, mmol/l] × [fasting insulin, μIU/ml]) /22,5.
Flow cytometry
Peripheral blood mononuclear cells (PBMC) were isolated from heparinized blood by centrifuging on Histopaque 1077 (Sigma-Aldrich, USA).
Th1-lymphocytes and Th17-lymphocytes were identified by intracellular production of interferon-gamma (IFN-γ) and interleukin 17 (IL-17) respectively. For this purpose PBMC were cultured on the RPMI 1640 medium supplemented with heat inactivated fetal bovine serum (10 %), L-glutamine (1 %) and penicillin/streptomycin (1 %) at 37 °C, 5 % CO2 in the presence of GolgiPlug, containing brefeldin A (BD Pharmingen, USA). Phorbol-12-miristate-13-acetate (PMA) in the final concentration 50 ng/ml (Sigma-Aldrich, USA) and ionomycin (1 μg/ml, Sigma-Aldrich, USA) were used to induce cytokine production. Intact unstimulated PBMC were run in parallel as a control sample and to evaluate spontaneous cytokine production ex vivo, which was regarded as a sign of prior in vivo stimulation [27]. In 6 h 100 μl of PBMC suspension were stained with PE-Cy5-labeled anti-CD4 (Becton Dickinson, USA) and APC-labeled anti-IL23R (R&D, USA), fixed, treated with 1x permeabilizing buffer (BD Pharmingen, USA), stained with PE-labeled anti-IL17A (R&D, USA) and FITC-labeled IFN-γ (Becton Dickinson, USA). Stained cells were stored in the fixing buffer (BD Pharmingen, USA) and analyzed not later than 12 h after preparation of the sample. Cells producing both IL-17 and IFN-γ were referred as double-positive Th1/Th17-lymphocytes. Numbers of IL-17+ and IFN-γ + cells were evaluated as well as mean fluorescence intensity (MFI), which reflected relative cytokine production at a single-cell level.
FoxP3+ Tregs were identified by the presence of intracellular transcription factor FoxP3. To identify this cell subpopulation PBMC were stained with FITC-labeled anti-CD4 and APC-labeled anti-CD25 (Becton Dickinson, USA), fixed and permeabilized with matching buffer set (Becton Dickinson, USA), stained with PE-labeled anti-FoxP3 antibodies (Becton Dickinson, USA) and stored in the fixing buffer up to the final analysis not later than 12 h after preparation.
Cells were analyzed on a FACSCalibur flow cytometer using CellQuestPro software (BD Biosciences, USA).
Statistical analyses
Analyses were performed in Statistica 10 (StatSoft Inc., USA). The Mann-Witney U-test was used to estimate the reliability of differences between groups. Spearman’s rank correlation coefficient (r) was used to estimate statistical dependence between variables. A value of p < 0.05 was considered statistically significant.
Results
Analysis of Th1, Th17 and Th1/Th17 lymphocytes showed that patients with DM2 had elevated numbers of Th17 in intact PBMC culture, elevated numbers of Th1 after stimulation of PBMC with PMA + ionomycin and lowered numbers of Th1/Th17 double-positive lymphocytes compared to healthy volunteers (Fig. 1). Numbers of Th1, Th17 and Th1/Th17 lymphocytes did not significantly differ between patients groups (Fig. 1). Of note that several patients with IGT were characterized by significantly elevated frequency of Th17-lymphocytes after PMA + ionomycin stimulation, which reached numbers twice as high as in the group of patients with DM2 and AH and healthy volunteers (Fig. 1a; one representative result out of two). However the whole group of patients with IGT was rather heterogeneous and relatively low number of patients in the group did not allow performing any stratification. Due to this reason no statistically significant differences was shown compared to patients with DM2 and AH.

T-helper subpopulations in patients with AH, DM2 and IGT. a Representative dot-plots showing numbers of Th1-, Th17-, Th1/Th17-lymphocytes in healthy volunteer (first column) and groups of patients (second column – patient with arterial hypertension; third column – hypertensive patient with DM2; fourth column – hypertensive patient with IGT). Cells were gated according to their expression of CD4. Only CD4+ cells are shown. b Numbers of Th1-, Th17-, Th1/Th17-lymphocytes in healthy volunteers (n = 12) and patients with AH (n = 7), DM2 (n = 20), IGT (n = 7) in intact PBMC culture (Media) and after stimulation (PMA + ionomycin). Data represent the mean and SEM; p-values represented above the bars are calculated by Mann–Whitney U test. All other comparisons were statistically insignificant (p > 0.05)
Hypertensive patients with DM2 had higher MFI of IFN-γ in Th1-lymphocytes from intact and PMA + ionomycin stimulated PBMC culture compared to healthy volunteers (Table 2). Analysis of MFI for IL-17 and IFN-γ in Th1/Th17 lymphocytes showed different kinds of cytokine production in double positive cells depending on circumstances of cell cultivation and pathology involved. Th1/Th17-cells of IGT patients were characterized by lower MFI of IL-17 in intact CD4+ lymphocytes compared to patients with AH (p = 0.018), with DM2 (p = 0.001) and healthy volunteers (p = 0.008) (Table 2). MFI of IFN-γ in Th1/Th17 lymphocytes after PMA + ionomycin stimulation in patients with IGT was lower compared to patients with DM2 (p = 0.003; Table 2). Moreover, all the groups of hypertensive patients had lower MFI of IFN-γ in intact Th1/Th17-lymphocytes compared to healthy volunteers, while MFI of IL-17 in PMA-activated Th17-lymphocytes was lower in patients with AH and DM2 compared to healthy volunteers (Table 2).
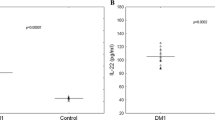
We have examined number of cells expressing receptor to IL-23 (IL-23R+ cells). It turned out that patients with IGT were characterized by the highest expression of IL-23R compared to patients with AH and healthy volunteers (Fig. 2). Number of IL-23R+ cells was also elevated in the group of patients with DM2 compared to healthy volunteers (Fig. 2). IL-23 is known to play the crucial role in the functional activity of Th17 [28].

The expression of receptors to IL-23. a Representative flow cytometry analysis of IL-23R expression in intact PBMC (left graph; media) and PBMC after stimulation with PMA + ionomycin (right graph; PMA). Data for one representative of healthy volunteers and patients with AH, DM2 and IGT are represented in each histogram. b Number of cells, positive for expression of IL-23R in patients with AH (n = 7), DM2 (n = 20), IGT (n = 7) in intact PBMC culture (Media) and after stimulation (PMA + ionomycin). Data represent the mean and SEM; p-values represented above the bars are calculated by Mann–Whitney U test. All other comparisons were statistically insignificant (p > 0.05)
Numbers of FoxP3+ T-regulatory lymphocytes in patients with DM2 were lower than in patients with AH and healthy volunteers (Fig. 3). Correlation analysis showed that numbers of FoxP3+ Tregs were negatively related to VAI in patients with DM2 (R = −0.517; p = 0.034; Fig. 4).

FoxP3+ T-regulatory cells. a Representative dot-plots showing numbers of FoxP3+ T-regulatory cells in healthy volunteers and patients with AH, DM2, IGT. Percentage indicates number of cells among all CD4 + −lymphocytes. b Numbers of FoxP3+ T-regulatory lymphocytes in healthy volunteers (n = 12) and patients with AH (n = 7), DM2 (n = 20), IGT (n = 7). Data represent the mean and SEM; p-values represented above the bars are calculated by Mann–Whitney U test. All other comparisons were statistically insignificant (p > 0.05). c Relationship between visceral adiposity index (x-axis) and numbers of FoxP3+ T-regulatory lymphocytes (y-axis) in patients with DM2. The p-value indicated in (c) was calculated using Spearman correlation; Spearman’s rank correlation coefficient (r) is indicated above p

Relationships between clinical and immune parameters in patients with DM2. a Relationship between numbers of Th17-lymphocytes in intact PBMC culture (x-axis) and glomerular filtration rate (y-axis); b relationship between numbers of IL-23R+ cells in intact PBMC culture (x-axis) and glomerular filtration rate (y-axis); c relationship between numbers of FoxP3+ Treg-lymphocytes (x-axis) and glomerular filtration rate (y-axis); d relationship between values of Treg/Th1 ratio in intact PBMC culture (x-axis) and visceral adiposity index (y-axis); e relationship between values of Treg/Th1 ratio in PMA + ionomycin stimulated PBMC culture (x-axis) and concentration of total cholesterol (y-axis); f relationship between values of Treg/Th1 ratio in PMA + ionomycin stimulated PBMC culture (x-axis) and concentration of LDL-cholesterol (y-axis). The p-value indicated in all the graphs was calculated using Spearman correlation; Spearman’s rank correlation coefficient (r) is indicated above p
We calculated ratios Treg/Th17 and Treg/Th1 for intact and PMA + ionomycin cell culture. We regarded this ratio as the representation of the severity of imbalance in immune dysregulation in patients: the lower it was – the more pronounced immune imbalance was considered to be. Our data showed that patients with DM2 had lower ratios Treg/Th17 and Treg/Th1 both in intact and PMA + ionomycin activated PBMC culture compared to healthy volunteers (Table 3). Patients with DM2 were also characterized by the lower ratios Treg/Th17 and Treg/Th1 in intact PBMC culture and lower Treg/Th1 ratio after PMA + ionomycin stimulation compared to non-diabetic AH patients (Table 3). Ratio Treg/Th17 in patients with IGT was lower compared to patients with AH (p = 0.042) while ratio Treg/Th1 after PMA-induced activation was lower compared to healthy volunteers (Table 3). As for non-diabetic patients with AH, the only difference between this group and group of healthy volunteers was decreased Treg/Th17 ratio after PMA-activation (Table 3).
We performed correlation analysis, trying to elucidate if immunoregulatory imbalance revealed in patients’ groups was associated with any clinical or biochemical changes. Multiple correlations were observed in the group of hypertensive patients with DM2. Glomerular filtration rate was negatively related to numbers of Th17-lymphocytes, IL-23R+ cells and FoxP3+ Treg-lymphocytes (Fig. 4). Decrease of Treg/Th1 ratio was associated with elevation of visceral adiposity index, while lowered ratio Treg/Th1 (after stimulation with PMA + ionomycin) was accompanied by increase of concentrations of total cholesterol and LDL-cholesterol (Fig. 4). These correlations were absent in other groups of patients and healthy volunteers.
Discussion
Our study revealed that perturbations of carbohydrate metabolism are accompanied by distinguishable changes in the immune-regulatory status of hypertensive patients. The changes are observed already at the stage of IGT and are still present in patients with DM2, even though parameters involved are different.
To our knowledge no previous works evaluated T-helper subpopulations in patients with IGT. Normally these patients remain undiagnosed and untreated unless they have another associated pathology. This made recruitment of patients into this group rather a complicated task, with the small number of IGT patients being one of the limitations of our study. Although, there were no significant differences in numbers of T-helpers’ subpopulations in this group, some patients with IGT were characterized by pronounced activation of Th17-lymphocytes. Also, we revealed elevated expression of IL-23R, necessary for IL-17 production in all patients with IGT. Probably, some additional factor is required for T-helpers to differentiate into Th17-lineage in these patients. We also revealed lowered ratio Treg/Th17 in IGT patients, as an indicator of Th17 cells’ excessive activation during IGT. Th17 cells are known to play the leading role at the beginning of the development of various diseases [29–31]. It had been shown that their activity subsides through the progression of the disease with Th1-lymphocytes taking over the leading position in the development of inflammation [30, 31]. Further studies are required to address the functioning of Th17-lymphocytes in hypertensive patients with IGT.
Increased numbers of Th17-lymphocytes were observed in patients with DM2 only in intact unstimulated PBMC culture, but not after stimulation with PMA + ionomycin. Intensity of IL-17 production at a single cell level after PMA stimulation was also lower in patients with DM2, compared to healthy volunteers (Table 2). Most probably, Th17-cells were already activated in vivo during DM2, and exhibited functional exhaustion during additional stimulation ex vivo. Exposure to chronic inflammation may diminish effector functions of T-lymphocytes, which may impair protection against infections and cause predisposition to cancer, which is typical to diabetic patients [32–34]. It had also been shown that patients with DM2 are characterized by lower numbers of Th17, specific to infectious pathogens [35].
Our results point out that important role in pathogenesis of inflammation during DM2 belongs to Th1-lymphocytes, as we observed elevation of IFN-γ + cells’ percentage in PMA + ionomycin stimulation and MFI of IFN-γ in intact and stimulated Th1 compared to control groups (Fig. 1; Table 2). Number of works pointing out the role of Th1 lymphocytes in pathogenesis of insulin resistance and DM2 is abundant [24, 36–38]. It was shown that IFN-γ deficiency was associated with improved insulin sensitivity and glucose homeostasis in experimental models [38]. IFN-γ, produced by Th1 in obesity, participates in the recruitment of proinflammatory M1-macrophages and other inflammatory cells to adipose tissue with subsequent induction of insulin resistance [37]. In many experimental works Th1 and FoxP3+ Treg-lymphocytes displayed antagonistic relationships: increase in Th1 numbers was associated with the decline of Treg frequency and increase of insulin resistance [21, 38]. Our study showed that decreased Treg/Th1 ratio in DM2 patients is associated with increase of visceral index of adiposity, elevation of total cholesterol and LDL cholesterol concentrations (Fig. 4).
Surprisingly, number of double-positive Th1/Th17 lymphocytes in intact PBMC culture tended to be lower in all groups of patients compared to healthy volunteers and significantly lower in the group of patients with DM2 (Fig. 1). These cells are involved in the development of tissue inflammation, are less susceptible to suppression by FoxP3+ Treg-lymphocytes and are present in rather high numbers in healthy adult persons [39, 40]. Both Th17- and Th1/Th17-lymphocytes are characterized by high plasticity and can be polarized into different T-helper subpopulations if proper micro-environmental milieu is created [25, 39, 41]. Being placed in polarizing conditions favorable for the differentiation of Th1, double-positive lymphocytes may cease the production of IL-17 and start producing solely IFN-γ [42]. Possible explanation for decreased numbers of double-positive Th1/Th17-lymphocytes in hypertensive DM2 patients observed in our study is transformation of pool of cells, constituting this subpopulation, into Th1-cells, which were found in elevated numbers, as we discussed above. We have also observed lowered MFI for IL-17 in Th1/Th17-lymphocytes from DM2 patients, while MFI for IFN-γ tended to be higher than in AH patients and healthy volunteers, and was significantly higher than in IGT patients (Table 2). In our opinion increase in the production of IFN-γ observed in Th1/Th17 lymphocytes in DM2 patients may reflect the beginning of the skewing of Th1/Th17 differentiation axis to the side of Th1 and may be typical to the progression of the disease from the subclinical (IGT) to the clinically manifested stage (DM2).
Reverse relationship between visceral adiposity index (VAI) and number of FoxP3+ Treg-lymphocytes represent another important finding in our study. It had been shown that both subcutaneous (SAT) and visceral adipose tissue (VAT) compartments are characterized by inflammation during obesity [43]. But VAT depot possesses unique pathogenic properties and is even termed an endocrine organ due to its ability to secrete an impressive number of vasoactive substances including adipokines [44]. BMI is a typical method used to assess adiposity, but it has a number of shortcomings and is not useful for evaluation of visceral adiposity [45]. VAI represents mathematical model aimed to evaluate body fat distribution [26]. Even though this method is not that precise as computer tomography or magnetic resonance imaging for estimation of visceral fat volume, it appeared to be more sensitive marker of cardiometabolic risk than BMI or waist circumference alone [26, 44, 46]. In our study VAI values observed in patients with DM2 tended to be higher than in other groups, and were significantly higher compared to healthy volunteers (Table 1). It was shown that repertoire of T cells in adipose tissue vary depending on the degree of obesity [21]. There is a hypothesis that peripherally induced FoxP3+ Treg cells may be recruited in the inflamed VAT, while thymic-derived natural Tregs are represented in VAT during obesity insufficiently [47]. We may speculate that there are two possible ways to explain the reverse correlation between FoxP3+ Treg numbers and VAI observed in DM2 patients in our study. It may reflect the universally diminished numbers of Treg lymphocytes typical for diseases accompanied by chronic inflammation [48–50]. In this case systemic decrease of Treg cells may be associated with the increase of adipose tissue volume and elevated local production of inflammatory cytokines and adipokines. Or the decline in peripheral blood numbers of Tregs may be the consequence of FoxP3+ Tregs recruitment to adipose tissue in order to control the local inflammation: the process which tends to proceed more actively with the increase of visceral adiposity, estimated by elevated VAI in our study [47].
Another clinical parameter closely related to immune factors in DM2 patients was glomerular filtration rate. It was inversely related to numbers of FoxP3+ Treg-lymphocytes, numbers of Th17- and IL-23R+ cells in intact PBMC culture [Fig. 4]. Baban B. et al. (2013) revealed accumulation of IL-17 and IL-23 in kidneys of db/db mice (animal model for type 2 diabetic nephropathy) [15]. Zhang C. et al. (2014) demonstrated that alteration of Th17/Treg ratio is typical for DM2 nephropathy [51]. The fact that patients recruited in our study were characterized by normal renal function indicates that disturbances of immune regulation during DM2 are distinguishable even before the involvement of kidneys into pathological process, but are still interconnected with renal function in these patients. Of interest remains relationships between immune parameters and kidney function in IGT patients, who had the highest GFR-values, but no correlations were revealed in this group. Possible explanation is a small number of recruited patients with IGT.
We acknowledge the difference in the age of the healthy volunteers and groups of patients as one of the limitations in our study (Table 1). Incidence of insulin resistance, arterial hypertension and conditions associated with them, as well as incidence of inflammatory diseases, markedly increases with age, which significantly limits number of individuals who may be considered as “healthy” in general population aged 50 – 60 years old [52, 53]. That is why we regarded group of hypertensive patients without carbohydrate disturbances as a comparison group, and differences revealed between hypertensive patients and hypertensive patients with DM2 or IGT were considered to be due to the presence of carbohydrate disturbances.
Conclusions
Overall, our study underscores the involvement of immune imbalance in the development of carbohydrate metabolism perturbations and indicates possible directions of the future application of our current knowledge to clinical practice. Immune imbalance revealed in our study in hypertensive patients with IGT included lowered ratio Treg/Th17 and elevated expression of IL-23-receptor by PBMC. Elevated numbers of Th17-lymphocytes in intact PBMC culture and Th1-lymphocytes after PBMC activation, as well as reduced ratios Treg/Th17 and Treg/Th1 appeared to be the most important parameters in hypertensive DM2 patients. Visceral adiposity index, concentrations of total and LDL-cholesterol and glomerular filtration rate were clinical factors most closely related to immune imbalance in hypertensive patients with DM2. Further prospective research is needed to elaborate the possible strategy of the risk evaluation for the DM2 patients according to their current inflammatory status and propose therapeutic approaches for its correction.
Abbreviations
- AH:
-
Arterial hypertension
- DM2:
-
Diabetes mellitus type 2
- GFR:
-
Glomerular filtration rate
- HDL:
-
High density lipoproteins
- HOMA:
-
Homeostatic model assessment for insulin resistance
- IGT:
-
Impaired glucose tolerance
- LDL:
-
Low density lipoproteins
- PBMC:
-
Peripheral blood mononuclear cells
- Th1:
-
T-helper lymphocytes type 1
- Th17:
-
T-helper lymphocytes type 17
- Treg:
-
T-regulatory lymphocytes
- VAI:
-
Visceral adiposity index
- VAT:
-
Visceral adipose tissue.
References
Levin G, Kestenbaum B, Ida Chen YD, Jacobs Jr DR, Psaty BM, Rotter JI, et al. Glucose, insulin, and incident hypertension in the multi-ethnic study of atherosclerosis. Am J Epidemiol. 2010;172(10):1144–54.
Sampanis C, Zamboulis C. Arterial hypertension in diabetes mellitus: from theory to clinical practice. Hippokratia. 2008;12(2):74–80.
Hewitt J, Castilla Guerra L, Fernández-Moreno M del C, Sierra C. Diabetes and stroke prevention: a review. Stroke Res Treat. 2012; doi: 10.1155/2012/673187.
Heidemann C, Boeing H, Pischon T, Nöthlings U, Joost HG, Schulze MB. Association of a diabetes risk score with risk of myocardial infarction, stroke, specific types of cancer, and mortality: a prospective study in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Potsdam cohort. Eur J Epidemiol. 2009;24(6):281–8.
Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med. 1998;339(4):229–34.
Juutilainen A, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Type 2 diabetes as a “coronary heart disease equivalent”: an 18-year prospective population-based study in Finnish subjects. Diabetes Care. 2005;28(12):2901–7.
Nathan DM, Davidson MB, DeFronzo RA, Heine RJ, Henry RR, Pratley R, et al. Impaired fasting glucose and impaired glucose tolerance: implications for care. Diabetes Care. 2007;30(3):753–9.
Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444:860–7.
Kolb H, Madrup-Poulsen T. An immune origin of type 2 diabetes? Diabetologia. 2005;48:1038–50.
Tilg H, Moschen AR. Inflammatory mechanisms in the regulation of insulin resistance. Mol Med. 2008;14(3–4):222–31.
Pederson BK, Febbraio MA, Mooney RA. Interleukin-6 does/does not have a beneficial role in insulin sensitivity and glucose homeostasis. J Appl Physiol. 2007;102:814–6.
Butcher M, Galkina E. Current views on the functions of interleukin-17A-producing cells in atherosclerosis. Thromb Haemost. 2011;106(5):787–95.
Shoelson SE, Lee J, Goldfine AB. Inflammation and insulin resistance. J Clin Invest. 2006;116(7):1793–801.
Donath MY, Shoelson SE. Type 2 diabetes as an inflammatory disease. Nat Rev Immunol. 2011;11:98–107.
Baban B, Liu JY, Mozaffari MS. Endoplasmic reticulum stress response and inflammatory cytokines in type 2 diabetic nephropathy: role of indoleamine 2,3-dioxygenase and programmed death-1. Exp Mol Pathol. 2013;94(2):343–51.
Cheng X, Yu X, Ding YJ, Fu QQ, Xie JJ, Tang TT, et al. The Th17/Treg imbalance in patients with acute coronary syndrome. Clin Immunol. 2008;127:89–97.
Ryba-Stanisławowska M, Skrzypkowska M, Myśliwiec M, Myśliwska J. Loss of the balance between CD4(+)Foxp3(+) regulatory T cells and CD4(+)IL17A(+) Th17 cells in patients with type 1 diabetes. Hum Immunol. 2013;74(6):701–7.
Tesmer LA, Lundy K, Sarkar S, Fox DA. Th17 cells in human disease. Immunol Rev. 2008;223:87–113.
Hirata T, Osuga Y, Hamasaki K, Yoshino O, Ito M, Hasegawa A, et al. Interleukin (IL)-17A stimulates IL-8 secretion, cyclooxygenase-2 expression, and cell-proliferation of endometriotic stromal cells. Endocrinology. 2008;149(3):1260–7.
Leaungwutiwong P, Ittiprasert W, Saikhun K, Tong-Ngam P, Akapirat S, Chattanadee S, et al. Impairment of CD4 + CD25+ regulatory T cells in C4-deficient mice. Asia Pac J Allergy Immunol. 2011;29(3):220–8.
Feuerer M, Herrero L, Cipoletta D, Naaz A, Wong J, Nayer A, et al. Lean, but not obese, fat is enriched for a unique population of regulatory T cells that affect metabolic parameters. Nat Med. 2009;15:930–9.
Winer S, Chan Y, Paltser G, Truong D, Tsui H, Bahrami J, et al. Normalization of obesity associated insulin resistance through immunotherapy. Nat Med. 2009;15:921–9.
Jagannathan-Bogdan M, McDonnell ME, Shin H, Rehman Q, Hasturk H, Apovian CM, et al. Elevated proinflammatory cytokine production by a skewed T cell compartment requires monocytes and promotes inflammation in type 2 diabetes. J Immunol. 2011;186:1162–72.
Zeng C, Shi X, Zhang B, Liu H, Zhang L, Ding W, et al. The imbalance of Th17/Th1/Tregs in patients with type 2 diabetes: relationship with metabolic factors and complications. J Mol Med (Berl). 2012;90(2):175–86.
Annunziato F, Romagnani S. Do studies in humans better depict Th17 cells? Blood. 2009;114(11):2213–9.
Amato MC, Giordano C. Visceral adiposity index: an indicator of adipose tissue dysfunction. Int J Endocrinol. 2014; doi: 10.1155/2014/730827.
Walker D, Jason J, Wallace K, Slaughter J, Whatley V, Han A, et al. Spontaneous cytokine production and its effects on induced production. Am J Reprod Immunol. 2002;47(3):159–66.
Volpe E, Servant N, Zollinger R, Bogiatzi SI, Hupé P, Barillot E, et al. A critical function for transforming growth factor beta, interleukin 23 and proinflammatory cytokines in driving and modulating human Th-17 responses. Nat Immunol. 2008;9:650–7.
Leipe J, Grunke M, Dechant C, Reindl C, Kerzendorf U, Schulze-Koops H, et al. Role of Th17 cells in human autoimmune arthritis. Arthritis Rheum. 2010;62(10):2876–85.
Lee YK, Turner H, Maynard CL, Oliver JR, Chen D, Elson CO, et al. Late developmental plasticity in the T helper 17 lineage. Immunity. 2009;30:92–107.
Palmer MT, Weaver CT. Autoimmunity: increasing suspects in the CD4+ T cell lineup. Nat Immunol. 2010;11(1):36–40.
Wherry EJ, Kurachi M. Molecular and cellular insights into T cell exhaustion. Nat Rev Immunol. 2015;15(8):486–99.
Casqueiro J, Casqueiro J, Alves C. Infections in patients with diabetes mellitus: A review of pathogenesis. Indian J Endocrinol Metab. 2012;16 Suppl 1:S27–36.
Wojciechowska J, Krajewski W, Bolanowski M, Kręcicki T, Zatoński T. Diabetes and cancer: a review of current knowledge. Exp Clin Endocrinol Diabetes. 2016;124(5):263–75.
Martinez PJ, Mathews C, Actor JK, Hwang SA, Brown EL, De Santiago HK, et al. Impaired CD4+ and T-helper 17 cell memory response to Streptococcus pneumoniae is associated with elevated glucose and percent glycated hemoglobin A1c in Mexican Americans with type 2 diabetes mellitus. Transl Res. 2014;163(1):53–63.
McGillicuddy FC, Chiquoine EH, Hinkle CC, Kim RJ, Shah R, Roche HM, et al. Interferon gamma attenuates insulin signaling, lipid storage, and differentiation in human adipocytes via activation of the JAK/STAT pathway. J Biol Chem. 2009;284(46):31936–44.
Wali JA, Thomas HE, Sutherland APR. Linking obesity with type 2 diabetes: the role of T-bet. Diabetes Metab Syndr Obes. 2014;7:331–40.
Stolarczyk E, Lord GM, Howard JK. The immune cell transcription factor T-bet: A novel metabolic regulator. Adipocyte. 2014;3(1):58–62.
Annunziato F, Cosmi L, Santarlasci V, Maggi L, Liotta F, Mazzinghi B, et al. Phenotypic and functional features of human Th17 cells. JEM. 2007;204(8):1849–61.
Holcar M, Goropevšek A, Ihan A, Avčin T. Age-related differences in percentages of regulatory and effector T lymphocytes and their subsets in healthy individuals and characteristics STAT1/STAT5 signaling response in helper T lymphocytes. J Immunol Res. 2015; doi: 10.1155/2015/352934.
Reinert-Hartwall L, Honkanen J, Salo HM, Nieminen JK, Luopajärvi K, Härkönen T, et al. Th1/Th17 plasticity is a marker of advanced β-cell autoimmunity and impaired glucose tolerance in humans. J Immunol. 2015;194:68–75.
Damsker JM, Hansen AM, Caspi RR. Th1 and Th17 cells: adversaries and collaborators. Ann N Y Acad Sci. 2010;1183:211–21.
Pou KM, Massaro JM, Hoffmann U, Vasan RS, Maurovich-Horvat P, Larson MG, et al. Visceral and subcutaneous adipose tissue volumes are cross-sectionally related to markers of inflammation and oxidative stress. Circulation. 2007;116:1234–41.
Fox CS, Massaro JM, Hoffmann U, Pou KM, Maurovich-Horvat P, Liu CY, et al. Abdominal visceral and subcutaneous adipose tissue compartments: association with metabolic risk factors in the Framingham Heart Study. Circulation. 2007;116:39–48.
Lavie CJ, McAuley PA, Church TS, Milani RV, Blair SN. Obesity and cardiovascular diseases: implications regarding fitness, fatness, and severity in the obesity paradox. J Am Coll Cardiol. 2014;63(14):1345–54.
Al-Daghri NM, Al-Attas OS, Wani K, Alnaami AM, Sabico S, Al-Ajlan A et al. Sensitivity of various adiposity indices in identifying cardiometabolic diseases in Arab adults. Cardiovasc Diabetol. 2015; doi: 10.1186/s12933-015-0265-5.
Eller K, Kirsch A, Wolf AM, Sopper S, Tagwerker A, Stanzl U, et al. Potential role of regulatory T cells in reversing obesity-linked insulin resistance and diabetic nephropathy. Diabetes. 2011;60:2954–62.
Sakaguchi S, Nomura T, Ono M. Regulatory T cells and immune tolerance. Cell. 2008;133:775–87.
Viglietta V, Baecher-allan C, Weiner HL, Hafler DA. Loss of functional suppression by CD4 + CD25+ regulatory T cells in patients with multiple sclerosis. J Exp Med. 2004;199:971–9.
Chavele KM, Ehrenstein MR. Regulatory T-cells in systemic lupus erythematosus and rheumatoid arthritis. FEBS Lett. 2011;585(23):3603–10.
Zhang C, Xiao C, Wang P, Xu W, Zhang A, Li Q, et al. The alteration of Th1/Th2/Th17/Treg paradigm in patients with type 2 diabetes mellitus: Relationship with diabetic nephropathy. Exp Mol Pathol. 2013;94(2):343–51.
Krentz AJ, Viljoen A, Sinclair A. Insulin resistance: a risk marker for disease and disability in the older person. Diabet Med. 2013;30:535–48.
Ramos-Casals M, García-Carrasco M, Brito MP, López-Soto A, Font J. Autoimmunity and geriatrics: clinical significance of autoimmune manifestations in the elderly. Lupus. 2003;12(5):341–55.
Acknowledgements
We thank Anna M. Gusakova, PhD, Nina M. Zheltonogova, Elena S. Kravchenko who performed supplementary laboratory analysis during the study and Olga A. Zhuravleva, PhD, who participated in the recruitment of patients.
Funding
The research leading to these results has received funding from the European Union Seventh Framework Program [FP7/2007–2013] under grant agreement number 241558 (SICA-HF).
The research leading to these results has received funding from the Russian Ministry of Science and Education within the FTP “R&D in priority fields of the S&T complex of Russia 2007–2012” under state contract number 02.527.11.0007.
Availability of data and materials
The dataset supporting the conclusions of this article is included within the article (Additional file 1).
Authors’ contributions
IK participated in the design of study, performed flow cytometry analyses, enzyme-linked analyses, statistical analysis of the obtained data, drafted the manuscript; TS conceived the study, participated in its design and coordination, revised manuscript; OK participated in the design and coordination of the study, revised manuscript; IV recruited patients in the study, obtained patients’ clinical data used in the manuscript; SP have given final approval for the manuscript. All authors read and approved the final manuscript.
Authors’ information
IK, PhD works as a research fellow at the Department of Functional and Laboratory Diagnostics of Cardiology Research Institute, Tomsk NRMC; TS, PhD, leading research fellow, head of the clinical diagnostics laboratory at the Department of Functional and Laboratory Diagnostics of Cardiology Research Institute, Tomsk NRMC; OK, MD, PhD, Professor, leading research fellow at the Department of Chronic Ischemic Heart Disease and Atherosclerosis of Cardiology Research Institute, Tomsk NRMC; IV works as a research fellow at the Department of Chronic Ischemic Heart Disease and Atherosclerosis of Cardiology Research Institute, Tomsk NRMC; SP, MD, PhD, Professor, temporary director of Cardiology Research Institute, Tomsk NRMC.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
The study protocol was approved by the local Biomedical Ethics Committee of RI Cardiology (protocol number 62 from 07.04.2010). All the patients gave the informed consent to participate in the study.
Author information
Authors and Affiliations
Corresponding author
Additional file
Additional file 1:
Dataset. (XLS 72 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Kologrivova, I.V., Suslova, T.E., Koshelskaya, O.A. et al. T-helper-1, T-helper-17, T-regulatory lymphocytes in hypertensive patients with diabetes mellitus type 2 or impaired glucose tolerance: association with clinical and metabolic parameters in a case control study. transl med commun 1, 2 (2016). https://doi.org/10.1186/s41231-016-0003-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41231-016-0003-3