
Abstract
Background
Considering that modification in body composition and growth velocity leads to alterations in zinc and copper nutritional status, the purpose of the study was to assess erythrocyte zinc and serum copper in adolescents of both genders, according to the stage of sexual maturity at different growth phases.
Methods
Two hundred and eighty-six adolescents were assessed, 157 were female, with body mass index Z-score between −2 and +2. Clinical biochemical measurements were assessed using atomic absorption spectrophotometry. Student’s t, Kruskal-Wallis, and Bonferroni tests were used.
Results
Median serum copper was superior, and zinc was inferior to respective reference values in all groups. Serum copper presented significant reduction in the final stages of pubertal development in males; in turn, erythrocyte zinc values increased linearly with the evolution of puberty stages in both genders. Comparison between genders in each stage of growth showed significant difference in peak acceleration and in deceleration for erythrocyte zinc and serum copper, with both being higher in females.
Conclusions
Serum copper is inversely influenced by modifications that occur with the evolution of puberty in males, whereas erythrocyte zinc is directly influenced in both genders, although always with deficient deposition. At peak acceleration and deceleration of growth, there is greater mobilization of erythrocyte zinc and serum copper in males, when compared with females, which does not occur at the onset of the acceleration of growth.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Modifications in body composition and growth velocity that occur in adolescence differ according to gender and stage of pubertal development, leading to alterations in zinc and copper nutritional status. Variability of erythrocyte and serum levels of these oligoelements may not be exclusively due to increased needs [1, 2] and low intake [2–4] frequently found in this age group. Even after completion of the pubertal growth spurt, requirements continue to elevate, seeking the replenishment of stocks depleted by high demand.
The importance of zinc during adolescence may be differentiated in four distinct aspects: in the regulation of food intake, in RNA and DNA synthesis, hormonal control, and bone growth. In the latter, it stimulates cell replication and differentiation of chondrocytes, osteoblasts (directly activates aminoacyl-tRNA synthetase stimulating protein synthesis), and fibroblasts [5]; it participates in the cell transcription culminating in the synthesis of somatomedin-C (IGF-1) (liver), alkaline phosphatase, collagen, and osteocalcin (bone) [5, 6]; it enhances the action of 1,25-hydroxyvitamin D3 and exerts an inhibitory effect on osteoclast activity [7]. In the endocrine system, zinc promotes the dimerization of the growth hormone (GH) granting greater stability; it participates in the synthesis of somatomedin-C and GH receptors at hepatic level and in spermatogenesis and oogenesis [7, 8].
Zinc deficiency is known to suppress the synthesis and secretion of gonadotropins compromising normal ovarian development and the estrogen cycle [9] as well as the testicular development [8].
Regarding copper, it is known that it performs, among others, an important role in iron metabolism, and that during puberty, requirements are high due to increased erythrocyte mass and connective tissue growth [1]; it also exerts an influence on the concentration of sexual hormones [10]. According to Bedwal and Bahuguna [9], existing hormonal differences between genders influence body mass distribution and copper requirements [11].
Increased adiposity may also determine a rise in copper concentrations due to an increase in the conversion of androgens and estrogens [12].
Considering the importance of zinc and copper in the processes involved with growth and sexual maturity, and in the virtue of the lack of research related to this subject during the period of adolescence, justifies this current study, which had an objective to assess the levels of serum copper and erythrocyte zinc in adolescents of both genders, according to the stages of sexual maturity at different growth phases.
Methods
This is a prospective and cross-sectional study involving 286 adolescents, with 157 females, between the ages of 10 and 20 years, students from public schools of the city of Curitiba-PR. This study was approved by the School Administration, and the Ethics Committee in Research at the Federal University of Sao Paulo, with prior written consent from participants and/or parents/legal guardians.
The inclusion criteria are body mass index Z-score between −2 and +2.
The exclusion criteria are the presence of chronic illness, use of nutritional supplements or medications containing iron, copper, or zinc, smoking, use of oral or injectable contraceptives, and the practice of extra-curricular physical activity.
Sample procedures
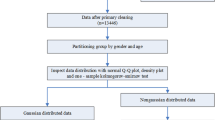
The Curitiba education network consists of 184 high schools. Because of operational difficulties related to the proximity to the health center with appropriate conditions for the collection of blood samples, the City Department of Health indicated a health center and three schools that were located geographically near this center. Thus, the 301 adolescents eligible for the study, enrolled in these three schools, composed the study sample. Although they have been called three times for data collection, 15/301 did not attend for blood sampling, leading to a sample loss of 4.9 %. It characterized a sample that includes the universe under study, when the three schools are considered, thus presenting a great internal validity. For generalization purposes to the universe of adolescents enrolled in public network, there may be difficulties. However, there is no evidence that the students enrolled in the sample schools are different from those enrolled in other network schools.
To calculate the number of sample units in each pubertal stage of each sex, the reference value for erythrocyte zinc was used, estimating a probability of type I error (α) of 0.05 and a probability of type II error (β) of 80 %. However, in some groups, greater numbers of adolescents were included because they were allocated after the classification of pubertal stage. This fact has allowed the reduction of variability of the measures, increasing the significance of the sample. The study participants were divided into two groups, according to gender and grouped according to stage of sexual maturity.
Anthropometric assessment
Weight and height were measured according to internationally recommended standards [13], calculating the body mass index Z-score [14].
Puberty staging
The model of sexual maturity staging proposed by Marshall and Tanner [15, 16] was adopted, by means of self-assessment [17]. Both breast development (B) and male genital development (G) were taken into account. This model uses the breast development to stage female sexual maturity (stages from B1 to B5) and genital development for male sexual maturity (stages from G1 to G5). The biochemical variables were analyzed according to puberty stages, taking into account similar physiological states between genders for comparison. In other words, the onset of the growth spurt: B2xG3; peak acceleration: B3xG4, and deceleration of growth: B4xG5 and B5xG5.
Biochemical assessment
Blood samples (5 mL) were collected between 8 and 9 a.m., after 12 h fasting. All chemicals used were of analytical grade. Acid-washed glassware was used throughout the study.
Erythrocyte zinc: erythrocyte mass was obtained according to method described by Whitehouse et al. [18] and stored at −18 °C until measurement. Hemoglobin concentration was determined using the cyanmethemoglobin method, soon after collection, and read at 540 nm. Results were expressed in μgZn/gHb, considering 35.6 to 47.8 μgZn/gHb, as reference value [19].
Serum copper and erythrocyte zinc concentrations were determined using atomic absorption spectrophotometry (Perkin Elmer AA Spectrometer Model 5100 PC) under the following conditions: hollow-cathode lamp; wavelength, 324.8 nm (Cu) and 213.9 nm (Zn); slit, 0.7 nm; an oxidizing air-acetylene flame; energy, 71 (Cu) and 65 (Zn); and duplicate reading with a 2-s integration time. Stock standard solutions of 1000 mg metal/L (Perkin-Elmer, PEN 4300183 for Cu) were diluted with glycerol at 3 % for erythrocyte zinc and in Milli-Q® water (Millipore Corporation, Darmstadt, Germany) for serum copper, resulting in working standard solutions containing 0.1; 0.2; 0.3; 0.5, and 1.0 mg Cu/mL. Accuracy of determinations was monitored through comparison with the commercial Quality Control Standard 21 (Perkin-Elmer, PEN 9300281) for both elements. Results for copper were expressed as μgCu/dL; the <70 μgCu/dL cutoff point was adopted to identify deficiency [20].
Statistical analysis
The Kruskal-Wallis and Bonferroni tests were used to compare biochemical variables between the different puberty stages, in each gender. For the comparison between genders at different growth phases, the Student’s t test was used. α < 0.05 was adopted.
Results
Most of the adolescents assessed were in the G3 (13.12 %) and B3 puberty stages (13.83 %) (data not shown), presenting values below the cutoff points for erythrocyte zinc and serum copper, 96.9 and 5.6 % in males and 93.0 and 3.2 % in females, respectively (data not shown). Median serum copper was greater than the respective reference values and erythrocyte zinc was lower, in all groups (Tables 1 and 2).
Median erythrocyte zinc values increased linearly with the evolution of puberty stages; the difference presented between stages 1 and 4 was statistically significant, in both genders (Fig. 1). Serum copper, in turn, decreased significantly in the final two stages in males, which was not observed in females (Fig. 2).

Median values of erythrocyte zinc (μgZn/gHb) of male and female adolescents during the different puberty stages

Median values of serum copper (μg/dL) of male and female adolescents during the different puberty stages
Median erythrocyte zinc and serum copper values did not present statistically significant differences between genders at the onset of the growth spurt (B2 and G3). Nevertheless, at peak acceleration of growth (B3 and G4), there was significant difference for erythrocyte zinc, p = 0.03 and serum copper values, p = 0.002, with higher levels of both minerals in females (Tables 3 and 4).
In the deceleration of growth phase, stages B4 and B5 were compared to stage G5, serum copper and erythrocyte zinc presented statistically higher values for females in both comparisons, p = 0.01 and 0.003 for serum copper, and p = 0.042 and 0.007 for erythrocyte zinc, respectively (Tables 3 and 4).
Discussion
Erythrocyte zinc deficiency was identified in 49.7 % of the adolescents assessed. Erythrocyte zinc is considered a constant parameter since the half-life of erythrocytes is 110 to 120 days, not representing an indicative of acute deficiency or recent dietary inadequacy [21, 22]. Due to the lack of researches on erythrocyte zinc, especially during adolescence, it was not possible to compare the results obtained. When normal values are reported in literature (39.4 ± 3.7 μgZn/gHb) [23], these are reported in groups of both prepubertal and pubertal adolescents, without identifying differences imposed by puberty.
The depletion of zinc as a result of zinc-dependent processes, such as growth, has been shown by other researchers. Therefore, it is possible to infer that zinc stored in red blood cells is mobilized by some organs and/or organic fluids [24, 25].
Similar to the results in this study, another study registered erythrocyte zinc during growth spurt, with higher values in females [26].
Differences between genders, in regard to erythrocyte zinc, are lower median values in males during peak acceleration and deceleration phases of growth, which may be attributed to the elevated need for zinc in males, as the growth rate and proportion of muscle per kilogram of body weight are higher when compared to the need for zinc in females. The participation of zinc in the mechanisms involved in the absorption and retention of nitrogen is unquestionable, being necessary for the formation of lean body mass and structures that compose the body [27].
It is estimated that there is a lower retention of zinc in females during puberty as a result of lower growth velocity [28]. However, this micronutrient is of fundamental importance for the proper functioning of female sexual organs due to the role played in oocyte maturation and, consequently, in estrogen synthesis. It was observed that the elevated frequency of erythrocyte deficiency, in the adolescents assessed, was probably caused by difficulties related to impaired erythrocyte zinc uptake, which occurs as a result of some nutritional deficiencies [6].
Median concentration of copper was greater, in all groups, than the adopted reference value (70 μg/dL); however, literature reports diverse cutoff points [2, 19, 29, 30] which hinder the comparison of results.
Other studies describe copper concentrations in serum or plasma in adolescents; however, they do not consider puberty stages, grouping the samples according to chronological age [31–33], or assessing a broad age range [34, 35], which also impedes the comparison of results.
The level of serum copper in males presented a statistically significant reduction, in the final two stages, that is, G1, G2, G3 > G4, G5, which was not observed in females. It is known that serum copper levels are positively associated with serum leptin concentrations [36, 37] in adults and adolescents [36, 38]. This association suggests that copper may be involved in the synthesis and metabolism of leptin, and leptin may be a copper metabolism regulator [36]. The same result was presented in the study of Horlick et al. [38] which reports that the leptin profile differs according to gender, describing greater plasmatic concentration in stages 1, 2, and 3 of pubertal development in males. It is important to highlight that the serum copper profile throughout pubertal development observed in this study perfectly overlaps the leptin profile described by these authors.
Assessment of serum copper levels in an age range that included newborns, children, and adolescents of both genders presented a statistically significant reduction in males [39]. Other study with 320 children (160 boys and 160 girls) aged between 7 and 14 years showed a statistically significant reduction in serum copper concentration in male children [31]. However, another study observed that serum copper decreased slightly with the increase of age, without difference between genders, through the assessment of 1098 boys and 1017 girls, aged 0.5 to 18 years [40].
Another study suggests that in men, the levels of testosterone have an influence on copper deficiency, as there is a reduction in the levels of testosterone and an increase in copper concentration in blood in castrated rats. According to the authors, women seem to be protected from copper deficiency due to estrogen, a hormone which alters the distribution of copper in the liver and increases its plasmatic levels [9].
The comparison of serum copper concentrations between genders, at peak acceleration and deceleration of growth, presented higher values in females. Estévez et al. [34] compared serum copper concentrations between men and women in fertile age and reported elevated levels in females. However, in the age range that comprises adolescence, pubertal development was not considered, which impedes a better comparison with our results.
Concerning serum copper, there was a low prevalence of deficiency. This result is consistent with the study by Estévez et al. [34] which reports the prevalence of copper deficiency, in male and female adolescents, at 3.6 and 2.1 %, respectively.
Alterations in the biochemical indices of erythrocyte zinc and serum copper that occur during adolescence not only reflect the specific nutritional status of these nutrients but also seem to be a result of physiological hormonal alterations in this period. Nevertheless, there were numerous difficulties for this investigation, since the hormonal alterations that accompany the period of puberty lead to major modifications in different areas of the body, and, consequently, in the distribution of zinc and copper.
Conclusions
The level of erythrocyte zinc is directly influenced by modifications that occur with the evolution of puberty in both genders, although always with deficient deposition.
The level of serum copper is inversely influenced by modifications that occur with the evolution of puberty in males, which does not occur in females.
At peak acceleration and deceleration of growth, there is a greater mobilization of erythrocyte zinc and serum copper in males, when compared to females, which does not occur at the onset of the acceleration of growth.
Abbreviations
B, female breast development; G, male genital development
References
Institute of Medicine (US). Dietary reference intake for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium and zinc. Washington DC: National Academy Press; 2000.
Gibson RS, Heath ALM, Ferguson EL. Risk of suboptimal iron and zinc nutriture among adolescent girls in Australia and New Zealand: causes, consequences, and solutions. Asia Pac J Clin Nutr. 2002;11(3):543–52.
Olivares M, Uauy R. Copper as an essential nutrient. Am J Clin Nutr. 1996;63(Suppl):791–6.
Fischer Walker CL, Ezzati M, Black RE. Global and regional child mortality and burden of disease attributable to zinc deficiency. Eur J Clin Nutr. 2009;63:591–7.
Brandão-Neto J, Stefan V, Mendonça BB. The essential role of zinc in growth. Nutr Res. 1995;15(3):335–52.
Gat-Yablonski G, Yackobovitch-Gavan M, Phillip M. Nutrition and bone growth in pediatrics. Pediatr Clin North Am. 2011;58(5):1117–40.
Kaji M. Zinc in endocrinology. Int Pediatr. 2001;16(3):1–7. https://www.researchgate.net/publication/264868754_Zinc_in_Endocrinology. Accessed 25 Jun 2014.
Nishi Y. Zinc and growth. J Am Coll Nutr. 1996;15(4):340–4.
Bedwal RS, Bahuguna A. Zinc, copper and selenium in reproduction. Experientia. 1994;50(7):626–40.
Saylor WW, Downer JV. Copper and zinc distribution in the liver and oviduct of estrogen and testosterone treated hens. Nutr Res. 1986;6(3):181–90.
Sloane BA, Gibbons CC, Hegsted M. Evaluation of zinc and copper nutritional status and effects upon growth of southern adolescent females. Am J Clin Nutr. 1985;42(2):235–41.
Henkin RI. Trace metals in endocrinology. Med Clin North Am. 1976;60(4):779–97.
Jelliffe DB. Evaluación del estado de nutrición de la comunidad. Serie de monografias n. 53. Geneve: WHO; 1968.
World Health Organization. Physical status: the use and interpretation of anthropometry. Technical Report Series n. 854. Geneve: WHO; 1995.
Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Arch Dis Child. 1969;44(235):291–303.
Marshall WA, Tanner JM. Variations in pattern of pubertal changes in boys. Arch Dis Child. 1970;45(239):13–23.
Matsudo VKR, Matsudo SM. Validade da auto-avaliação na determinação da maturação sexual. Rev Bras Ciênc Mov. 1991;5(2):18–35.
Whitehouse RC, Prasad AS, Rabbani PI, Cossack ZT. Zinc in plasma, neutrophils, lymphocytes, and erythrocytes as determined by flameless atomic absorption spectrophotometry. Clin Chem. 1982;28(3):475–80.
Gibson RS. Principles of nutritional assessment. New York: Oxford University Press; 1990.
Laitinen R, Vuori E, Dahlstrom S, Akerblom HK. Zinc, copper, and growth status in children and adolescents. Pediatr Res. 1989;25(4):323–6.
Aggett PJ, Favier A. Zinc. Int J Vitam Nutr Res. 1993;63(4):301–7.
Voskaki I, Arvanitidou V, Athanasopoulou H, Tzagkaraki A, Tripsianis G, Giannoulia-Karantana A. Serum copper and zinc levels in healthy greek children and their parents. Biol Trace Elem Res. 2010;134:136–45.
Marreiro DN, Fisberg M, Cozzolino SMF. Zinc nutritional status in obese children and adolescents. Biol Trace Elem Res. 2002;86(2):107–12.
Krebs NF, Hambidge KM. Zinc metabolism and homeostasis: the application of tracer techniques to human zinc physiology. Bio Metals. 2001;14(3–4):397–412.
King JC. Zinc: an essential but elusive nutrient. Am J Clin Nutr. 2011;94(Suppl):679–84.
Mahmoodi MR, Kimiagar SM. Prevalence of zinc deficiency in junior high school students of Tehran City. Biol Trace Elem Res. 2001;81(2):93–103.
IOM- Institute of Medicine (US). Dietary intake references for zinc. Washington DC: National Academy of Sciences; 2003. p. 442–501.
World Health Organization. Zinc. In: WHO, editor. Trace elements in human nutrition and health. Geneve: WHO; 1996. p. 72–104.
Agte VV, Nagmote RV, Chiplonkar SA. Role of vitamin-zinc interactions on in vitro zinc uptake by human erythrocytes. Biol Trace Element Res. 2004;99(1–3):99–111.
Marino DD, King JC. Nutritional concerns during adolescence. Pediatr Clin North Am. 1980;27(1):125–39.
Alarcon OM, Reinosa Fuller J, Silva TM, Angarita C, Teran E, Navas M, et al. Serum level of Zn, Cu and Fe in healthy schoolchildren residing in Merida, Venezuela. Arch Latinoam Nutr. 1997;47(2):118–22.
Rükgauer M, Klein J, Kruse-Jarres JD. Reference values for the trace elements copper, manganese, selenium, and zinc in the serum/plasma of children, adolescents, and adults. J Trace Elements Med Biol. 1997;11(2):92–8.
De la Cruz-Góngora V, Gaona B, Villalpando S, Shamah-Levy T, Robledo R. Anemia and iron, zinc, copper and magnesium deficiency in Mexican adolescents: National Health and Nutrition Survey 2006. Salud Publica Mex. 2012;54(2):135–45.
Estevéz J, Bonilla LC, Bonilla E, Villalobos R. Concentraciones séricas de cobre y cinc en una población suburbana del estado Zulia, Venezuela. Invest Clin. 1988;29(3):97–109.
Abiaka C, Olusi S, Al-Awadhi A. Reference ranges of copper and zinc and the prevalence of their deficiencies in an arab population aged 15–80 years. Biol Trace Elem Res. 2003;91(1):33–43.
Olusi S, Al-Awadhi A, Abiaka C, Abraham M, George S. Serum cooper levels and not zinc are positively associated with serum leptin concentrations in the healthy adult population. Biol Trace Elem Res. 2003;91(2):137–44.
Chen MD, Song YM, Tsou CT. Leptin concentration and the Zn/Cu ratio in plasma in women with thyroid disorder. Biol Trace Element Res. 2000;75(1–3):99–105.
Horlick MB, Rosenbaum M, Nicolson M, Levine LS, Fedun B, Wang J, et al. Effect of puberty on the relationship between circulating leptin and body composition. J Clin Endocrinol Metab. 2000;85(7):2509–18.
Lockitch G, Halstead AC, Wadsworth L, Quigley G, Reston L, Jacobson B. Age and sex-specific pediatric reference intervals and correlations for zinc, copper, selenium, iron, vitamins A and E, and related proteins. Clin Chem. 1988;34(8):1625–8.
Lin C, Wilson A, Church BB, Ehman S, Roberts WL, McMillin GA. Pediatric reference intervals for serum copper and zinc. Clin Chim Acta. 2012;413:612–5.
Authors’ contributions
AGM, LAL, and OMSA contributed to the conception and design of the study. AGM was responsible for the acquisition of data. LAL and ELJ performed the biochemical analysis. ELJ performed the statistic analysis. AGN, LAL, ROSS, ELJ, and OMSA participated in the analysis and interpretation of data. OMSA gave the final approval. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Ethics approval and consent to participate
This study was approved by the School Administration and the Ethics Committee in Research at the Federal University of Sao Paulo, with prior written consent from participants and/or parents/legal guardians.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Marques, A.G., Sarni, R.O.S., Lopes, L.A. et al. Erythrocyte zinc and serum copper in male and female adolescents according to puberty stage at different growth phases. Nutrire 41, 9 (2016). https://doi.org/10.1186/s41110-016-0010-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41110-016-0010-1