
Abstract
Background
Severe pregabalin intoxication may cause serious symptoms, such as coma. Since pregabalin is a small molecule with no protein binding sites and has low volume of distribution, hemodialysis can be effective in eliminating pregabalin from the blood. However, in cases of emergency, it is not always possible to perform hemodialysis because of limited availability and time delay associated with using the plumbing equipment. Continuous hemodiafiltration (CHDF) can be performed without plumbing equipment; however, the knowledge on the effectiveness of CHDF in pregabalin elimination is insufficient.
Case presentation
A septuagenarian woman with normal renal function was found in a collapsed state with symptoms of coma and miosis. Empty medical bags of pregabalin (2350 mg), bepotastine besilate (600 mg), celecoxib (4600 mg), quetiapine fumarate (87.5 mg), clotiazepam (180 mg), and teprenone (50 mg) were found around her. During the patient's transfer to our hospital, her cognition worsened and she developed glossoptosis necessitating her emergent intubation upon arrival. We considered that the coma was mainly caused by pregabalin intoxication and were concerned about the consequent critical comorbidities. Thus, we performed CHDF in a high-flow setting in our intensive care unit for pregabalin elimination. After 8 h of CHDF, the patient regained consciousness, and after 6.5 h we extubated her. At a later date, we measured her serum pregabalin levels during the clinical course and estimated the blood pregabalin clearance levels depending on her metabolism as 76.8 mL/min and depending on CHDF itself as 65.1 mL/min. Based on these findings, we concluded that CHDF contributed to reducing blood pregabalin levels in this patient.
Conclusions
Our case revealed that pregabalin clearance using CHDF is similar to metabolic clearance in patients with normal renal function, indicating that CHDF decreases blood pregabalin levels and can be a potential treatment for severe pregabalin intoxication.
Similar content being viewed by others


Background
Pregabalin, an analgesic drug, has been associated with increased drug abuse/overdose, along with increased prescription frequency [1,2,3,4]. Few critically ill intoxication cases have been reported to present with severe symptoms, such as coma [5, 6].
Hemodialysis (HD) can reduce blood pregabalin levels and could be effective for the treatment of severe pregabalin intoxication [6,7,8]. However, in cases of emergency, it is not always possible to perform HD because of limited availability and time delay associated with using the plumbing equipment. Continuous hemodiafiltration (CHDF) using a multipurpose blood-processing apparatus can usually be performed without plumbing equipment. However, CHDF provides a lower dialysate flow rate compared to that of HD and, therefore, may lead to lower levels of pregabalin elimination compared to that of HD. Additionally, the knowledge of pregabalin clearance using CHDF is insufficient.
We report a case of severe pregabalin intoxication that was treated with high-flow CHDF. In this case, we measured the serum pregabalin levels during the clinical course and estimated the pregabalin clearance rate associated with CHDF.
Case presentation
A septuagenarian woman with a medical history of central cord syndrome, dementia, and eczema recently complained about unfounded things, which was considered a paranoia caused by dementia.
One night, she was found in a collapsed position by her family with multiple empty medical bags scattered around her; thus, emergency medical services (EMS) were called. At the scene, the EMS team found that she was unconscious with a Glasgow coma scale (GCS) of E1V1M5 and miosis (pupil diameters, 1/1 mm) but had no other vital sign abnormalities (heart rate, 52 beats/min; blood pressure, 111/65 mmHg; respiratory rate, 18 breaths/min; and SpO2, 99% [room air]). She was suspected of drug intoxication and transferred to the emergency department of our hospital. During the transfer, the EMS team initiated oxygen delivery to prevent hypoxemia.
On hospital arrival, the vital signs were similar to those recorded on the scene. However, the GCS was impaired to E1V1M2, and she had also developed glossoptosis. Based on the empty medical bags found at the scene, the patient was assumed to be taking drugs such as pregabalin (2350 mg), bepotastine besilate (600 mg), celecoxib (4600 mg), quetiapine fumarate (87.5 mg), clotiazepam (180 mg), and teprenone (50 mg). While the patient was taking multiple drugs, we suspected that pregabalin majorly contributed to her condition according to the intake dose and the presence of coma and miosis; overdose of clotiazepam, a benzodiazepine analog, may cause coma, but since this drug has an anticholinergic effect, we thought the miosis is inconsistent. Intubation was performed to prevent suffocation. We could drain the stomach content via a gastric tube and, hence, suspected that the duration after drug intake was short; we subsequently performed gastric lavage. The laboratory data showed malnutrition and electrolyte disorders probably due to the poor food intake owing to paranoia, but no other problems including renal dysfunction were noted (urea nitrogen 8.0 mg/dL; creatinine 0.62 mg/dL; total protein 5.6 g/dL; albumin 3.2 g/dL; sodium 126 mEq/L; potassium 2.9 mEq/L; pH 7.427; and lactate 1.0 mmol/L). The electrocardiogram revealed normal ranges of QTc (0.424 s) and PR (0.140 s) with no arrhythmia, suggesting that the cardiac system was not affected. However, we were concerned about the further worsening of her condition as her GCS was impaired in a short time; hence, we decided to perform blood purification therapy for pregabalin intoxication. Since it was late at night, there were limited resources to perform HD, and we decided to perform CHDF in the intensive care unit (ICU).
After ICU admission settings (2.5 h after hospital arrival), we initiated CHDF using a cellulose triacetate hemofilter (membrane area 2.1 m2) with the following settings: blood flow rate, 120 mL/min; dialysate flow rate, 4000 mL/h; filtration flow rate, 500 mL/h; and replacement flow rate, 500 mL/h. We didn’t use mechanical ventilation since we closely monitored her, and she had not presented any hypoxia in intubated condition. After CHDF initiation, the patient’s condition gradually improved, and she regained consciousness after 8 h of initiation (Fig. 1). We terminated CHDF 2 h after confirming the patient’s consciousness and extubated her 4.5 h after CHDF completion. Both pupil diameters were pinhole size at the CHDF initiation, but they turned into 2/2 mm at the CHDF termination. The patient had sufficient urine output during the clinical course and a good general condition even after extubation. While she presented hypercapnic acidosis during she presented coma, she had no metabolic acidosis during the clinical course (venous blood gas analysis, 4 h after hospital arrival, pH 7.285, PvCO2 58.6 mmHg, base excess − 0.1 mEq/L; 7 h after hospital arrival, pH 7.293, PvCO2 57.3 mmHg, base excess 0.2 mEq/L). She was discharged from our ICU on day 3. However, a psychiatrist diagnosed the patient as having a suspected persecutory delusional disorder, which was the cause of her intentional overdose. Thus, even though she didn’t have suicidal ideation at that time, she was recommended to continue hospitalization to get routinely examined; hence, she was transferred to another hospital on day 10.

Clinical course post-hospital arrival. GCS, Glasgow coma scale; UO, urine output; ICU, intensive care unit; RR, respiratory rate; HR, heart rate; BP, body pressure
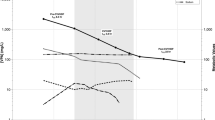
At a later date, we confirmed the serum pregabalin levels during the clinical course through stocked samples using liquid chromatography–tandem mass spectrometry. The levels after the described duration beginning from hospital arrival were as follows: 0 h: 43.8 μg/mL; 2.5 h (CHDF initiation): 31.8 μg/mL; 3.5 h: 25.3 μg/mL; 5.5 h: 16.3 μg/mL; 7.5 h:12.4 μg/mL; 12.5 h (CHDF completion): 5.0 μg/mL; and 33.5 h: 0.96 μg/mL. The serum pregabalin level at the CHDF hemofilter outlet at 7.5 h was measured as 6.1 μg/mL. We assumed the pregabalin kinetics as a one-compartment model and estimated it using the measured serum pregabalin levels in this patient and the calculation formulas illustrated in Table 1 [9, 10]. Elimination rate constants during not performing CHDF, i.e., elimination depending on the patient’s metabolism, and during performing CHDF were stated as K_Pt and K_Pt+CHDF, respectively. The half-lives of the pregabalin were calculated using the serum pregabalin levels at 0 h and 2.5 h for the duration of not performing CHDF and at 2.5 h and 3.5 h for the duration of performing CHDF, respectively. Hence, we found that the half-life of pregabalin eliminated by only the patient’s metabolism was 5.4 h and that during performing CHDF was 3.0 h in this patient. Since the pregabalin elimination by CHDF was added to that by the patient’s metabolism, the half-life of pregabalin was shortened by performing CHDF. The patient’s metabolic pregabalin clearance, calculated using the previously reported volume of distribution (Vd/F) (36 L) [11] and the serum pregabalin levels at 0 h and 2.5 h, was 76.8 mL/min; the CHDF’s pregabalin clearance, calculated using the serum pregabalin levels of the patient and the hemofilter outlet at 7.5 h, was 65.1 mL/min. Thus, total pregabalin clearance during performing CHDF was estimated as 141.9 mL/min. The estimated serum pregabalin levels in case we didn’t perform CHDF on this patient were shifted higher than the actual pregabalin levels as illustrated in Fig. 2 (estimated levels are calculated using serum pregabalin level at 2.5 h, elapsed times after the hospital arrival, and half-life of pregabalin during performing CHDF; Table 1, calculation formulas). Based on these values, it could be stated that CHDF contributed in reducing pregabalin levels in the patient.

Actual or estimated serum pregabalin levels with/without performing continuous hemodiafiltration. CHDF, continuous hemodiafiltration. The black circle indicates the actual serum pregabalin levels. The white circle indicates the estimated serum pregabalin level if the patient would not have undergone continuous hemodiafiltration. The patient’s metabolic pregabalin clearance was calculated using the serum pregabalin levels at 0 h and 2.5 h after the hospital arrival. The CHDF’s pregabalin clearance was calculated using the serum pregabalin levels of the patient and the hemofilter outlet at 7.5 h after the hospital arrival. The total pregabalin clearance during performing CHDF was the sum of the patient’s metabolic clearance and CHDF’s clearance
Discussion and conclusions
Pregabalin has a low molecular weight (159 Da), lacks protein binding, and has a low Vd/F (36 L) in healthy volunteers [11], and, therefore, can be easily eliminated using HD. A case report in a patient with renal failure requiring maintenance HD estimated the HD’s pregabalin clearance as 88.8 mL/min [8]; a previous study investigating 12 patients with renal failure requiring maintenance HD demonstrated that the HD’s mean pregabalin clearance based on patient’s plasma pregabalin levels was 207 mL/min [12]. While there were no investigations on CHDF’s pregabalin clearance, we estimated the CHDF’s pregabalin clearance as 65.1 mL/min, which is similar to the metabolic clearance in the present patient who had no renal dysfunction (76.8 mL/min). Based on these findings, CHDF was suggested to have a sufficient pregabalin elimination rate.
Pregabalin has a short half-life of approximately 6 h, and its plasma clearance is essentially equivalent to its renal clearance [11], indicating that most of the metabolic clearance is dependent on the renal function. A previous report described that a patient without renal dysfunction recovered from severe pregabalin intoxication with supportive care alone [13]. However, prolonged coma may cause comorbidities such as aspiration pneumonia [13]. Moreover, since pregabalin intoxication may cause other critical comorbidities such as complete atrioventricular block [14], it is better to prevent severe intoxication promptly. Previous reports suggest that treatment using HD contributed to improving pregabalin intoxication symptoms immediately in patients with end-stage renal failure or those who consumed a large amount of pregabalin (4200 mg) [6, 7]. While a recent systematic review investigating extracorporeal treatments (ECTRs) including HD for gabapentinoid (gabapentin or pregabalin) intoxication recommended against performing ECTRs in patients with normal renal function, it mostly included case reports (30 reports out of 33 studies), and no reports about patients who underwent CHDF for pregabalin intoxication were included [15]. Considering the cost-effectiveness, it is better not to initiate ETCRs in patients with normal renal function and less likely to have subsequent severe comorbidities. However, the cutoff value of blood pregabalin levels for patients who are likely to complicate such comorbidities is not determined [5]. Early removal of excessive pregabalin from blood may help to avoid consequent comorbidities. Thus, the indications for ECTRs for pregabalin intoxication remain unclear. We decided to initiate CHDF on the present patient because the time after the drug overdose was considered short and concerned to complicate comorbidities. Our patient improved from a severe condition after 8 h of CHDF without other comorbidities. In addition, in this report, we have added information on pregabalin clearance of CHDF.
The frequent symptoms of pregabalin intoxication are drowsiness, confusion, or apathy [5]; however, when patients consume a large amount of pregabalin, they may experience severe symptoms such as coma, seizure, respiratory suppression, or arrhythmia, including complete atrioventricular block [5, 14]. A previous case report described that the patient who ingested 8.4 g of pregabalin got deteriorated his consciousness to comatose status after 3 h of ingestion with a plasma pregabalin level of 66.5 μg/mL, and remained unconscious until plasma pregabalin level decreased to 15.2 μg/mL [13]. While there is no denying the fact that other drugs such as clotiazepam associated with coma, the serum pregabalin levels in our patient were considered high enough to present coma. Regarding pupil findings, a previous report on pediatric patients with isolated pregabalin intoxication described one patient who presented with miosis and one patient who presented with mydriasis [16]. While the patient in our report ingested multiple drugs and the effect of pregabalin on pupils is varying, no other drug was considered to be associated with miosis, except for pregabalin. It was a severe case of pregabalin intoxication with coma and miosis.
In conclusion, we report a case of severe pregabalin intoxication that was treated with high-flow CHDF. CHDF contributes to an immediate decrease in blood pregabalin levels, suggesting it to be a suitable treatment option for severe pregabalin intoxication.
Availability of data and materials
The data associated with this case report are available from the corresponding author upon reasonable request.
Abbreviations
- CHDF:
-
Continuous hemodiafiltration
- ECTRs:
-
Extracorporeal treatments
- EMS:
-
Emergency medical services
- GCS:
-
Glasgow coma scale
- HD:
-
Hemodialysis
- ICU:
-
Intensive care unit
- Vd/F:
-
Volume of distribution
References
Hirakata M, Yoshida S, Tanaka-Mizuno S, Kuwauchi A, Kawakami K. Pregabalin prescription for neuropathic pain and fibromyalgia: a descriptive study using administrative database in Japan. Pain Res Manag. 2018;2018:2786151.
Gorfinkel LR, Hasin D, Saxon AJ, Wall M, Martins SS, Cerda M, et al. Trends in prescriptions for non-opioid pain medications among U.S. adults with moderate or severe pain, 2014–2018. J Pain. 2022;23(7):1187–95.
Green K, Cooke O’Dowd N, Watt H, Majeed A, Pinder RJ. Prescribing trends of gabapentin, pregabalin, and oxycodone: a secondary analysis of primary care prescribing patterns in England. BJGP Open. 2019. https://doi.org/10.3399/bjgpopen19X101662.
Isoardi KZ, Polkinghorne G, Harris K, Isbister GK. Pregabalin poisoning and rising recreational use: a retrospective observational series. Br J Clin Pharmacol. 2020;86(12):2435–40.
Rietjens SJ, Sikma MA, Hunault CC, de Lange DW, Hondebrink L. Pregabalin poisoning: evaluation of dose-toxicity relationship. Br J Clin Pharmacol. 2022;88(3):1288–97.
Ocak M, Uçar C. The effectiveness of hemodialysis in case of intoxication with Pregabalin. J Emerg Med Case Rep. 2019;10(4):112–4.
Lee DW, Lee HJ, Kim HJ, Chang SH, Park DJ. Two cases of pregabalin neurotoxicity in chronic kidney disease patients. NDT Plus. 2011;4(2):138.
Yoo L, Matalon D, Hoffman RS, Goldfarb DS. Treatment of pregabalin toxicity by hemodialysis in a patient with kidney failure. Am J Kidney Dis. 2009;54(6):1127–30.
Seabury RW, Stork CM. Pharmacokinetic and toxicokinetic modeling. In: Wexler P, editor. Encyclopedia of toxicology. 3rd ed. Cambridge: Academic Press; 2014. p. 856–61.
Shiga H, Hirasawa H, Nishida O, Oda S, Nakamura M, Mashiko K, et al. Continuous hemodiafiltration with a cytokine-adsorbing hemofilter in patients with septic shock: a preliminary report. Blood Purif. 2014;38(3–4):211–8.
Bockbrader HN, Radulovic LL, Posvar EL, Strand JC, Alvey CW, Busch JA, et al. Clinical pharmacokinetics of pregabalin in healthy volunteers. J Clin Pharmacol. 2010;50(8):941–50.
Randinitis EJ, Posvar EL, Alvey CW, Sedman AJ, Cook JA, Bockbrader HN. Pharmacokinetics of pregabalin in subjects with various degrees of renal function. J Clin Pharmacol. 2003;43(3):277–83.
Wood DM, Berry DJ, Glover G, Eastwood J, Dargan PI. Significant pregabalin toxicity managed with supportive care alone. J Med Toxicol. 2010;6(4):435–7.
Aksakal E, Bakirci EM, Emet M, Uzkeser M. Complete atrioventricular block due to overdose of pregabalin. Am J Emerg Med. 2012;30(9):2101 e1-2104.
Bouchard J, Yates C, Calello DP, Gosselin S, Roberts DM, Lavergne V, et al. Extracorporeal treatment for gabapentin and pregabalin poisoning: systematic review and recommendations from the EXTRIP workgroup. Am J Kidney Dis. 2022;79(1):88–104.
Dufayet L, Monnet F, Laborde-Casterot H, Care W, Lekens B, Langrand J, et al. Unintentional exposure to pregabalin in </=6-year-old children: a nationwide French Poison Control Center study. Clin Toxicol (Phila). 2021;59(5):433–9.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
TS(Shimazui) contributed to the conception and design, analyzing the data, and drafting and critical revision of the manuscript for important intellectual content. NK contributed to the conception and design, analyzing the data, and critical revision of the manuscript for important intellectual content. KK(Kako), SI, TS(Suzuki), SH, and HF contributed to the critical revision of the manuscript for important intellectual content. KK(Kibayashi) and KN contributed to the measurement of the important data and critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent for publication was obtained from the legal representative of the patient.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Shimazui, T., Kitamura, N., Kako, K. et al. High-flow continuous hemodiafiltration successfully decreased blood pregabalin levels in a patient with severe pregabalin intoxication: a case report. Ren Replace Ther 8, 60 (2022). https://doi.org/10.1186/s41100-022-00449-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41100-022-00449-w