
Abstract
Background
Poor infant and young child feeding (IYCF) practices are a significant issue both globally and in developing nations, and they have a significant role in undernutrition, healthy growth, and development, particularly in the first 2 years of life. Improving children's general health and wellbeing requires recognizing and decreasing preventable drivers of malnutrition. Hence, this study aimed to assess the prevalence and possible determinants of minimum dietary diversity among 6–23 months old babies in the Gambia.
Methods
Data from the 2019–2020 Gambia demographic and health survey were used. The study included a total of 2100 weighted 6–23 months old children. To identify characteristics significantly linked with minimum dietary diversity among infants, a multilevel fixed-effect analysis approach was used. After adjusting other confounding variables, variables with a p value of 0.25 were incorporated into a multivariable multilevel regression analysis to determine associated variables. An adjusted odds ratio with a 95% confidence interval was then applied.
Results
Only 22.22% (95% CI 18.55, 21.99) of infants had received the minimum dietary diversity. Mothers, who had mass media exposure (aOR = 2.71, CI = (1.02, 6.21), wealthier (aOR = 1.70, CI = 1.02, 2.85), child age of (aOR = 4.14, CI = 2.98, 5.76), and (aOR = 4.97, CI = 3.54, 6.98), have shown a positive statistical association with the outcome variable, respectively. Regarding regions mothers who came from Kanifing (aOR = 0.49, CI = 0.25, 0.94), Janjanbureh (aOR = 0.38, CI = 0.18, 0.82), and Basse (aOR = 0.51, CI = 0.26, 0.99) had showed less likelihood odds to provide the minimum dietary diversity (MDD) for their babies compared to Banjul local government area, respectively.
Conclusion
The World Health Organization dietary evaluation tool suggests that the MDD value be extremely low, even though it might be slightly higher than the numbers for some nations. The country may need to take drastic measures to tackle child malnutrition.
Similar content being viewed by others


Introduction
Nutritional status and micronutrient intake in children are currently predicted by dietary diversity (DD). DD is a straightforward indicator that is frequently used as a stand-in for dietary quality, sufficiency in micronutrients, and food accessibility [1, 2]. The World Health Organization (WHO) defines DD as eating foods from the key nutritionally important diet kinds while keeping a balance between meals derived from plant and animal sources [3, 4]. For higher dietary quality and to meet daily energy and nutrient needs, minimum dietary diversity (MDD) is the consumption of five or more food groups from the eight recommended food groups, including breast milk, grains, roots, and tubers, legumes, and nuts; dairy products (infant formula, milk, yoghurt, and cheese); flesh foods (meat, fish, poultry, and liver/organ meats); eggs; vitamin A-rich fruits and vegetables; and other fruits and vegetables [3,4,5].
Children mainly under five are suffering tremendously by malnutrition in all regions of the globe; however, its negative consequences are deeply rooted in Africa [6, 7]. All of those African nations are severely hit by this public challenges socially, economically, and politically [8]. All nations, stakeholders, intersectoral organizations, governmental and non-governmental bodies should put their positive impact to reduce the severity of malnutrition around the globe. Given the scale and severity of the problem, various health care organizations have made significant contributions by regularly creating awareness, assigning and training health professionals, and developing materials and treatment guidelines [9]. In 2002, the WHO, in collaboration with the UNICEF, launched a global feeding strategy called infant and child feeding (IYCF) to reverse the low trends of child feeding practices [9].
The importance of halting undernutrition from getting children is because of, it affects about 149.2 million children of under 5 years of age were stunted and 45 million are exposed to wasted globally in 2020, with 75% of such children living in the African and Southeast Asia Regions [10, 11]. The 2019 regional analysis report indicated that 57.5 million, 11.8 million and 3.0 million under five children were exposed to stunting, wasting and severely wasting [7]. To maintain proper physical growth and metal development, young children and infants should take a minimum of five from the total balanced foods of namely, grains, roots, and tubers; legumes and nuts; dairy products; flesh foods (meat, fish, poultry, and organ meats); eggs; vitamin-A-rich fruits and vegetables; and other fruits and vegetables according to WHO recommendation [12,13,14], nevertheless, the recommendation did not accomplish as it stated by many developing nations [15, 16]. From the perspective of these studies, it is possible to conclude that household food insecurity is a factor for inadequate dietary consumption in Africa [17, 18]
According to the facts of several studies, inadequate dietary intake is one of the major causes of life-threatening illnesses by leading children to stunting, underweight and wasting [12]. Malnutrition can have a long-lasting impact on children's health and well-being. It can lead to chronic diseases, such as heart disease, stroke, and diabetes, later in life. It can also reduce children's chances of success in school and in life [10]. Children don not only endanger the lives of children, but also challenge the survival of their families and nations by predisposing them from other diarrheal diseases and infections, as well as inadequate participation, performance in their communities and schools also have great chance to happened [19,20,21]. Studies depicted that place of residence, age of the child, maternal education, birth order, wealth index and number of children in the household, high burden of disease and malnutrition practices, home gardening and media exposure were some of the factors which associated with MDD [22,23,24,25]
Nutrition is one of the major issues the world is implementing on by 2030 to eradicate hunger [26]. However, most parents and care givers in the developing countries find it difficult to provide adequate and diversified nutrition for their children [27]. This is likely to be a major challenge for the world in its 2030 to eradicate hunger, and various remedial measures are needed [15, 16].
According to the 2018 UNICEF MICS report, malnutrition is keeping going as a big deal of Gambian children. As a result of poor health services, limited knowledge of parents, most children did not feed vitamins, proteins and minerals reduction [28]. This finding is supported by the 2021 Global Nutrition Report, which noted that the Gambia has not made much progress in reducing stunting among young children and noncommunicable diseases linked to diet [29]. This role of this study is to prove information to the harmed of the inadequate dietary nutrition in Gambia, particularly those aged 6–23 months for the implementation to reduce undernutrition among infants and young children in Gambia.
Methods and materials
Study design and setting
The Gambia Demographic Health Survey (GDHS), a secondary, sizable community-based cross-sectional survey that was carried out in the Gambia from November 21, 2019, to March 30, 2020, served as the foundation for this investigation. The Gambia Bureau of Statistics (GBoS) in collaboration with the Ministry of Health and Social Welfare performed the 2019–2020 Gambia Demographic and Health Survey (GDHS 2019–2020) between October 2019 and February 2020. The Gambia Demographic and Health Survey (GDHS 2019–2020) is the second DHS survey that was conducted in the Gambia in cooperation with the global Demographic and Health Survey Program. The Gambia is a country in West Africa. The Republic of Senegal forms its northern, southern, and eastern borders, while the Atlantic Ocean forms its western boundary. The nation experiences two distinct seasons, the rainy season (June to October) and the dry season (November to May) [30].
Source population and sampling technique
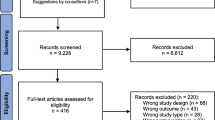
Stratified, two-stage cluster sampling was used for the survey. Enumeration areas (EAs) inside each sampling stratum were initially chosen with a probability proportional to their size. The households were carefully sampled in the second step. Each of the chosen clusters or EAs were chosen with a probability proportional to their size inside each sampling stratum in the first step. A total of 281 EAs were chosen. A set number of 25 households were systematically chosen from the resulting lists of households as the sampling frame, yielding a total sample size of 7025 selected households. Results from this sample are reflective of those found across the nation, in urban, rural, and local government areas [30]. Mothers who had children with 6–23 months old 24 h before to the survey made up the source population. In order to correct for unequal sample distributions during data collection, the estimation process applied the weightings for the children's sample. As a result, 2100 weighted samples of children at age of 6–23 months were used in the study. The detail can be accessed from the GDHS report (https://dhsprogram.com/pubs/pdf/FR369/FR369.pdf).
Study tools and measurement
Dependent variable
The 24-h recall of food groups from the GDHS survey was used to build the dietary diversity indicator that was used in the study [30]. Guidelines from WHO and UNICEF define the MDD score for children aged 6–23 months as the percentage of children who ate anything from at least five of the eight food groups within a 24-h period. 1-grains, roots and tubers, 2-legumes and nuts, 3-dairy products, 4-meat, fish, poultry, and liver/organ meats, 5-eggs, 6-vitamin A-rich fruits and vegetables, 7-other fruits and vegetables, and 8-breast milk are the eight food groups [4, 30, 31]. In this study, the MDD score of the children was divided into two categories. Children between the ages of 6 and 23 months who ate at least five different food types in the 24 h before an interview are deemed to have complied with the MDD requirements and their MDD score is classified as having sufficient minimal dietary diversity. Additionally, kids between the ages of 6 and 23 months who ingested fewer than five food categories in the 24 h preceding an interview were deemed to have fallen short of the MDD standards, with their MDD score being classified as having inadequate minimal dietary diversity [31].
Independent variable
The literature review of factors linked to children's DD served as a guide for the study's design and creation of the conceptual framework. As result, both individual and community level factors were assessed to determine the highest potential factors that are linked with MDD in the Gambia. Personal-related factors such as maternal age, educational attainment, sex of the household head, wealth index, marital status, child age, ANC, PNC after 02 months, place of delivery, family size, twins, under five children, size of the child, media exposure (watching to TV, listening to radio and reading to magazine/newspapers), breast feeding status, order of birth, occupation, whereas, in the community level factors such as region, residence, community level poverty, community level education, community media exposure, community, and ANC utilization were included in the model.
Data management and analysis process
We did a secondary analysis of the GDHS 2019–2020 using the Kids Records (KR) dataset. STATA version 17 and Microsoft Excel version 19 were used for data purification. Calculations and descriptive statistics, such as frequency and percentages of different variables, were provided using texts, tables, and graphs. A multilevel mixed effect logistic regression model was applied to each independent variable, and only variables with p values lower than 0.25 were considered. The adjusted odds ratio was used to calculate the degree of connection between the dependent and independent variables, and variables with a p value of < 0.05 were regarded as statistically significant.
In the GDHS data, the infant is contained within a cluster, and neonates from the same cluster showed more resemblance than neonates from other clusters. As a result, the common regression model's assumptions regarding observation independence and equal variance across clusters are broken. This suggests that in order to take into consideration between-cluster effects, a complex model must be used. A multilevel random intercept logistic regression model was created to ascertain the association between individual-level and community-level characteristics and the chance that a newborn will not receive postnatal care within 2 days of birth.
There was a total of four models created. Without any explanatory variables, the first model—also referred to as an empty or null model—was fitted. The disparities across communities were lessened by using this tactic. Understanding community variances requires knowledge of the null model. As a starting point, we evaluated how much the observed discrepancies in mothers' behavior regarding MDD may be attributed to societal influences. Additionally, this model served as evidence in favor of the adoption of a multi-level statistical framework and a yardstick for determining whether to utilize multi-level or traditional logistic regression. It was evaluated using the proportional change of variance (PCV), the log-likelihood ratio test (LLR), the median odds ratio (MOR), the intraclass correlation coefficient (ICC), and the AIC. Only individual-level characteristics were included in the second model. Only community-level features were present in the third. In contrast, the final (fourth) model included both elements at the individual and community levels. Additionally, when comparing models using model deviance, the model with the lowest deviation was picked for reporting and result interpretation.
In order to compare the layered models, deviation (2log likelihood) was utilized. The intracellular correlation coefficient (ICC) and log-likelihood were used to calculate the variation between clusters. The ICC displays the degree of variability among infants who do not receive MDD before 24 h of the interview. A multilevel binary logistic regression analysis was conducted to identify the individual and societal variables that influence 6–23-month-old infants' MDD before 24 h of the interview.
where πij is the likelihood that no iron will be consumed, and ij is the likelihood that it will. When none of the explanatory factors are present, the influence on MDD is represented by the intercept, or β0. The variables at the individual and community levels for the ith person in group j are βxij, respectively. Also, because the β's are fixed coefficients, a rise in X can result in an increase in the risk of ingesting iron by an additional ß unit. The UK demonstrates the jth community's random effect—the influence of the community on the mother's decision to intake MDD. Assuming that each cluster has a unique intercept (β0) and fixed coefficient (β), the clustered nature of the data as well as between and between community variances were taken into consideration.
The likelihood test was used to compare the models, and model 4 was found to have the greatest value and be the best fit. All variables had VIF values less than 10, and the mean VIF value of the final model was 1.50, which was utilized to identify multicollinearity. Crude odds ratio (COR) and adjusted odds ratio were used to measure the relationship between the dependent and independent variables (AOR). For the final model, factors having a p value of less than 0.25 in COR have been chosen as contenders. Adjusted odds ratios and 95% confidence intervals with a p value of 0.05 were used to determine the strength of associations between dependent and independent factors. The median odds ratio (MOR), which is defined as the median value of the odds ratio between the area at the lowest risk and the highest risk when randomly choosing two clusters, was used to assess the measure of variance. MOR = e0.95√VA or, MOR = exp. [√(2 × VA) × 0.6745], where VA is the area level variance [32, 33]. The Proportional Change in Variance (PCV) reveals the variation in MDD intake among children 6–23 months explained by factors. The PCV is calculated as = \(\frac{{{\text{Vnull}} - {\text{VA}}}}{{{\text{Vnull}}}}\)*100, where Vnull is the initial model's variance, and VA is the model's variance with additional terms. Also, the intraclass correlation coefficient (ICC), a measurement of the variation in bottle feeding between clusters, is computed as; ICC = VA ÷ VA + 3.29 ∗ 100%, where VA = area/cluster level variance [32, 33].
Operational definitions
Community women education This represents the overall worth of women's educational attainment as determined by the median distribution of educational attainment in the neighborhood. The ratio of women in the community with at least a secondary education was considered low if it fell below the median (0–8.33%), and high if it rose above the median (8.34–100%).
Community media exposure This variable was derived from individual responses to radio or television media exposure. It was defined as low if the proportion of women exposed to media in the community was 0–66% and high if the proportion was 66.67–100%.
Community ANC utilization rate This variable is also produced from the various ANC utilization individual values. If the proportion of women who attended at least three ANC visits in the community ranged from 0 to 82%, it was considered low. 0.83 was the median value.
Community poverty The same process is used to get this variable from each household's wealth index. It was deemed high if the proportion of women in a community's two lowest wealth quintiles was between 56 and 100%, and low if it was between 0 and 55%.
Results
Sociodemographic characteristics of the study participants
To assess the MDD intake a total of 2100 weighted mothers were included in this study. Slightly more than half 1126 (53.63%), of them and nearly half 940 (44.77%) of the study participants were with an estimated age range of 25–34 years old and did not enroll in formal education, respectively; however almost nearly all of them 1969 (93.79%) were married and 472 (22.50%) were came from poorest household, respectively. Regarding ANC visits and types of place of delivery of the house about 1702 (81.03%), and 1846 (87.93%), had shown at least three visits and institutional delivery, respectively. Majority 1733 (82.55%) and slightly higher half 1172 (55.86%) of the study participants have shown currently working status and baby PNC checkup after 02 months. Moreover, about 1212 (57.73%) mothers came from large family members (more than 10), and large portion of household heads are male 1798 (85.61%). Regarding children’s profile about 922 (43.92%), 1094 (52.11%), and 916 (43.64%) of them were found in at large birth weight, male and fourth and more order of birth, respectively. About 782 (37.23%), and 2058 (98.02%) babies are found from 11 to 17 months old and single birth, respectively (Table 1).
Community level factors characteristics of the study participants
As it illustrated in the following table regarding community literacy, media exposure, ANC utilization, regions, residence, and poverty proportions nearly half of them 1127 (53.67%) had low ANC follow-ups, low community poverty level, 1381 (65.74%) media exposure 1138 (54.17%). Large portion of the study participants came from Brikama, and urban areas 866 (41.23%), and 1378 (65.64%), respectively (Table 2)
Highlights of random effect analysis
Due to the hierarchical nature of the DHS data, we assessed the clustering effect. The null model's ICC in the random-effects investigation had a high value. This shows that the variance within clusters accounted for about 12.04% of the variety in MDD provision for babies, leaving individual variation to explain for the remaining 87.96%. The empty model's higher MOR value revealed a wide range in MDD provision between clusters. The MOR value of the empty model showed that if we observed two children from two different clusters, one would be more likely to use MDD provision than the other: a child in the cluster with high MDD utilization had a 1.90 times higher likelihood of using MDD provision than a child in the cluster with lower MDD intake. The model with the lowest deviation—in this case, Model III with a deviance of 2001.14—was chosen as the best-fit model since it was the smallest value. Deviation was also utilized to assess model fitness. Model III (Table 2) is the one to use in the ideal situation (Table 2).
Determinants associated with MDD among 6–23-month-old children in the Gambia
This study declared some determinants including child age, wealth index, mass media exposure, and region were statistically significant in the multilevel mixed effect of logistic regression model with the outcome variable. It was evident that those mothers who have mass media exposure of reading to magazines/newspapers had revealed higher odds to provide the MDD supply for their children compared to their counterparts (aOR = 2.71, CI = (1.02, 6.21). Similarly, it was also revealed that those who have classified under richer wealth index, had higher odds to feed the MDD for their kids compared to with poorest mothers (aOR = 1.70, CI = 1.02, 2.85). Children whose age found from 12–17 and 18–23 months old have a higher odd of (aOR = 4.14, CI = 2.98, 5.76), and (aOR = 4.97, CI = 3.54, 6.98) times to receive the MDD compared to with 6–11 months old children, respectively. Conversely, regarding regions mother who came from Kanifing (aOR = 0.49, CI = 0.25, 0.94), Janjanbureh (aOR = 0.38, CI = 0.18, 0.82), and Basse (aOR = 0.51, CI = 0.26, 0.99) had showed less likelihood odds to provide the MDD for their babies compared to their compared to Banjul local government area, respectively (Table 3).
Discussion
Using the most recent nationally representative data from the National Centre for demography and Health Statistics, this study examined mothers of 6- to 23-month-old children for minimum dietary diversity feeding in the Gambia. We found statistically significant relationships between local government areas, household wealth index, age of the child, and mass media exposure for reading newspapers or books with minimum dietary diversity feeding among mothers of 6–23-month-old children in the Gambia in multiple mixed effects multilevel logistic regressions or the final model of analysis that adjust for confounders. Based on this, just 20.22% (95% CI 18.55–21.99) of children aged 6–23 months in the Gambia had access to sufficient MDD, or around one in five children only. This is a worrying indication that the problem still poses a serious nutritional issue that the Gambia has to address by developing comprehensive nutritional strategy. This finding is nearly in line with studies conducted in Rwanda [34] and India [21]; however, this figure has shown a less MDD coverage compared to literatures done in Ethiopia, Bangladesh [35], and Nepal [36]. With contrast to studies conducted in Ethiopia [37], and 33 SSA recent study [38], this study has declared higher MDD supply for children, respectively.
According to the country's profile, the possible gap is caused by poor food production, consumption, living standard of the people, countries commitment to their policy, sociocultural and attitudes as well as maternal and child health services coverage, and people's ability to purchase a range of food items in Gambia. The recent rise in the cost of consumable goods and a lack of knowledge about how to make complementary foods may be factors in the lack of dietary diversity among Gambian youngsters.
The results of this study suggest that children between the ages of 6 and 23 months require a diet that is a little more varied than is typical for their age. When compared to a kid aged 6–11 months, a child between the ages of 12 and 17 and 18 and 23 months had around a four to five times greater likelihood of receiving the minimum amount of diverse food. We can support this with solid evidences we have in hand. Several studies done in Ethiopia [37, 39], Indonesia [40], Bangladesh [40], and Nepal [36] have declared similar findings with this study at hand. An evidence from the UNICEF found that whereas nearly half of the young children aged 18–23 months received four or more food categories each day, less than a quarter of infants aged 6–11 months did [41]. There is a significant age gap between the children in this. This can be a result of mothers' attitudes about IYCF. According to research on Gambia's eating habits and beliefs, many mothers do not consider starting supplemental feeding for their children at a young age [42]. Mothers' socioeconomic position, culture, and customs have been observed to affect the early introduction of supplemental foods in the Gambia and Nepal [42, 43]; furthermore, the study highlighted that this could be difficult without the help of their friends, families, and community. Therefore, it is vital to implement national initiatives and program aimed at mums of young children to encourage healthy eating and feeding habits.
We discovered beneficial relationships between the children's MDD and the rich home wealth index. Compared to women from households with the lowest wealth index, those from wealthy households had increased probabilities of seeking to give their children MDD. Other favorable research works from the Gambia [44], Burkina Faso [45], Rwanda [34], and Ethiopia [24]. The lack of resources in poor homes to offer a balanced diet for the family members may account for the link between a low wealth index and under adequate MDD in children. Such households frequently experience poor environmental conditions, a higher risk of disease exposure, and limited access to essential medical services, less ability to purchase household goods to their families as a whole might facilitate the inadequate MDD. Additionally, this study discovered that media exposure, access, and use—including reading newspapers, magazines, and other publications—were all positively related to attaining a sufficient MDD. This outcome was consistent with earlier research done in Ethiopia [24], Spain [46], and Rwanda [34]. This demonstrates the effectiveness of mass media exposure in modifying mothers' knowledge, attitudes, and health-seeking behaviors as well as their interactions with their families and the larger community.
The minimum dietary diversity of infants aged 6–23 months was similarly related to local government districts. Compared to mothers who had lived in Banjul, mothers who had lived in Kanifing, Janjanbureh, and Basse were 49%, 38%, and 51% less likely to provide their kids the necessary variety of meals. Although the author could not find other previous literatures to support this figure, we can have a solid evidence at hand to justify it according to the profiles of these local governmental areas. Evidence indicated that there are also regional differences in the distribution of health professionals. The Greater Banjul Area (GBA), which includes the Kanifing and Banjul City Councils, is home to the majority of health professionals in both the public and private sectors. Actually, of all the cadres, GBA has the highest percentage. The GBA contains more than half of the physician specialists, dentists, pharmacists, and laboratory workers. According to sector HR statistics, most (79%) of salaried professional health employees are working in the public sector, and majority of the urban residence found in Banjul, this population might have higher access of health-related practices [47, 48]. From this vantage point, most mums who reside in GBA may have a higher likelihood of receiving expert guidance concerning their children from these persons. Mothers that are knowledgeable and educated may be found here as well.
This study had a number of advantages. First of all, because the study was based on sizable datasets that were nationally representative, it has enough statistical power to generalize findings to Gambia children between the ages of 6 and 23 months. Second, to guarantee that the findings were representative at the national and regional levels, the estimates for the study were finished after the data had been weighted to account for probability sampling and nonresponse. Additionally, a suitable multilevel analytical technique was employed to study the determinants of changes in MDD over time. This will be the first national study in the Gambia and will provide insight for upcoming researchers and programmers. When analyzing the findings, it is important to consider the current study's several limitations. Because of the cross-sectional nature of the study, it is hard to determine whether the independent and dependent variables are causally related. Additionally, this study did not consider a number of unobserved variables, such as soil restrictions and altitude, which were not examined as part of the survey. The restrictions mentioned above should be taken into consideration when interpreting the survey's results. However, we think that our discoveries and suggestions will significantly advance knowledge about Gambian children's feeding practices.
Conclusions
Although the MDD value may be marginally higher than certain countries' figures, the WHO dietary evaluation tool recommends that it is very low. The nation may require aggressive action to combat child malnutrition. After controlling confounders and other possible biases, mass media exposure, age of the child, wealth index and regions were the prominent factors that have been revealed a statistically significant value. The government of the Gambia may reap significant benefits if it supports local and national media, supports economically disadvantaged households, and collaborates with local states, community-based campaign implementers, and other stakeholders.
Availability of data and materials
Data for this analysis came from the DHS Program on Gambian 2019/20 DHS data files, which are open to the public. The DHS program repository has the datasets created and/or analyzed during the current investigation at www.dhsprogram.com.
References
Habte T-Y, Krawinkel M. Dietary diversity score: a measure of nutritional adequacy or an indicator of healthy diet? 2016.
Rathnayake KM, Madushani P, Silva K. Use of dietary diversity score as a proxy indicator of nutrient adequacy of rural elderly people in Sri Lanka. BMC Res Notes. 2012;5:1–6.
WHO Guidelines Approved by the Guidelines Review Committee. Infant and young child feeding: model chapter for textbooks for medical students and allied health professionals. Geneva: World Health Organization; 2009. (Copyright © 2009, World Health Organization).
World Health Organization. Global nutrition monitoring framework: operational guidance for tracking progress in meeting targets for 2025. 2017.
World Health Organization. Global action plan on physical activity 2018–2030: more active people for a healthier world. Geneva: World Health Organization; 2019.
World Health Organization. Nutrition in the WHO African region. 2017.
Estimates: WHOUWTWBGJCM. Levels and trends in child malnutrition: key findings of the 2020 edition. Geneva, Switzerland: WHO; 2020.
International Food Policy Research Institute. Global nutrition report 2015: actions and accountability to advance nutrition and sustainable development. Washington, DC; 2015. https://www.un.org/nutrition/sites/www.un.org.nutrition/files/global_nutrition_report_2015.pdf.
World Health Organization. Guiding principles for complementary feeding of the breastfed child 2023. Switzerland, Geneva; 2023. https://www.who.int/publications/i/item/9275124604.
World Health Organization. Malnutrition. 2021. https://www.who.int/news-room/fact-sheets/detail/malnutrition. 2021.
Infant and young child feeding [Internet]. http://www.who.int/mediacentre/factsheets/fs342/en/. 2021.
Solomon D, Aderaw Z, Tegegne TK. Minimum dietary diversity and associated factors among children aged 6–23 months in Addis Ababa, Ethiopia. Int J Equity Health. 2017;16(1):1–9.
World Health Organization. Indicators for assessing infant and young child feeding practices: part 2: measurement; 2010.
World Health Organization. Indicators for assessing infant and young child feeding practices: part 1: definitions: conclusions of a consensus meeting held 6–8 November 2007 in Washington DC. USA: World Health Organization; 2008.
Anin SK, Saaka M, Fischer F, Kraemer A. Association between infant and young child feeding (IYCF) indicators and the nutritional status of children (6–23 months) in northern Ghana. Nutrients. 2020;12(9):2565.
Saaka M, Wemakor A, Abizari A-R, Aryee P. How well do WHO complementary feeding indicators relate to nutritional status of children aged 6–23 months in rural Northern Ghana? BMC Public Health. 2015;15(1):1–12.
Dafursa K, Gebremedhin S. Dietary diversity among children aged 6–23 months in Aleta Wondo District, Southern Ethiopia. J Nutr Metab. 2019;2019:1–10.
Mekonnen TC, Workie SB, Yimer TM, Mersha WF. Meal frequency and dietary diversity feeding practices among children 6–23 months of age in Wolaita Sodo town, Southern Ethiopia. J Health Popul Nutr. 2017;36(1):1–8.
Temesgen H, Yeneabat T, Teshome M. Dietary diversity and associated factors among children aged 6–23 months in Sinan Woreda, Northwest Ethiopia: a cross-sectional study. BMC Nutr. 2018;4(1):1–8.
Khamis AG, Mwanri AW, Ntwenya JE, Kreppel K. The influence of dietary diversity on the nutritional status of children between 6 and 23 months of age in Tanzania. BMC Pediatr. 2019;19(1):1–9.
Agrawal S, Kim R, Gausman J, Sharma S, Sankar R, Joe W, et al. Socio-economic patterning of food consumption and dietary diversity among Indian children: evidence from NFHS-4. Eur J Clin Nutr. 2019;73(10):1361–72.
Ali NB, Tahsina T, Hoque DME, Hasan MM, Iqbal A, Huda TM, et al. Association of food security and other socio-economic factors with dietary diversity and nutritional statuses of children aged 6–59 months in rural Bangladesh. PLoS ONE. 2019;14(8):e0221929.
Abizari A-R, Azupogo F, Nagasu M, Creemers N, Brouwer ID. Seasonality affects dietary diversity of school-age children in northern Ghana. PLoS ONE. 2017;12(8):e0183206.
Seboka BT, Hailegebreal S, Yehualashet DE, Gilano G, Kabthymer RH, Ewune HA, et al. Exploring spatial variations and determinants of dietary diversity among children in Ethiopia: spatial and multilevel analysis using EDHS (2011–2016). J Multidiscip Healthc. 2021;14:2633.
Rakotonirainy NH, Razafindratovo V, Remonja CR, Rasoloarijaona R, Piola P, Raharintsoa C, et al. Dietary diversity of 6-to 59-month-old children in rural areas of Moramanga and Morondava districts, Madagascar. PLoS ONE. 2018;13(7):e0200235.
United Nations. United Nations sustainable development goals. New York: UN; 2015.
Gatica-Domínguez G, Neves PA, Barros AJ, Victora CG. Complementary feeding practices in 80 low-and middle-income countries: prevalence of and socioeconomic inequalities in dietary diversity, meal frequency, and dietary adequacy. J Nutr. 2021;151(7):1956–64.
UNICEF. The Gambia multiple indicator cluster survey 2018: survey findings report. The Gambia multiple indicator cluster survey 2018: survey findings report 2019, p. 694.
2021 GNR. Country nutrition profiles Gambia: the burden of malnutrition at a glance, 2021.
Gambia Bureau of Statistics - GBoS, ICF. The Gambia demographic and health survey 2019–20. Banjul, The Gambia: GBoS/ICF; 2021.
Croft TN, Marshall AM, Allen CK, Arnold F, Assaf S, Balian S. Guide to DHS statistics. Rockville: ICF; 2018. p. 645.
Collin M. Lining up to eat: birth order and nutritional status in rural Ethiopia. Oxford: St Antony’s College; 2006.
Merlo J, Chaix B, Ohlsson H, Beckman A, Johnell K, Hjerpe P, et al. A brief conceptual tutorial of multilevel analysis in social epidemiology: using measures of clustering in multilevel logistic regression to investigate contextual phenomena. J Epidemiol Community Health. 2006;60(4):290–7.
Custodio E, Herrador Z, Nkunzimana T, Węziak-Białowolska D, Perez-Hoyos A, Kayitakire F. Children’s dietary diversity and related factors in Rwanda and Burundi: a multilevel analysis using 2010 Demographic and Health Surveys. PLoS ONE. 2019;14(10):e0223237.
Kabir I, Khanam M, Agho KE, Mihrshahi S, Dibley MJ, Roy SK. Determinants of inappropriate complementary feeding practices in infant and young children in Bangladesh: secondary data analysis of Demographic Health Survey 2007. Matern Child Nutr. 2012;8:11–27.
Baek Y, Chitekwe S. Sociodemographic factors associated with inadequate food group consumption and dietary diversity among infants and young children in Nepal. PLoS ONE. 2019;14(3):e0213610.
Alemu TG, Techane MA, Wubneh CA, Assimamaw NT, Belay GM, Tamir TT, et al. Spatial variation and determinates of dietary diversity among children aged 6–23 months in Ethiopia: spatial and multilevel analysis using Ethiopian Demography Health Survey (EDHS) 2019. Arch Public Health. 2022;80(1):1–13.
Belay DG, Aragaw FM, Teklu RE, Fetene SM, Negash WD, Asmamaw DB, et al. Determinants of inadequate minimum dietary diversity intake among children aged 6–23 months in sub-Saharan Africa: pooled prevalence and multilevel analysis of demographic and health survey in 33 sub-Saharan African Countries. Front Nutr. 2022;9:894552.
Beyene M, Worku AG, Wassie MM. Dietary diversity, meal frequency and associated factors among infant and young children in Northwest Ethiopia: a cross-sectional study. BMC Public Health. 2015;15(1):1–9.
Sekartaji R, Suza DE, Fauziningtyas R, Almutairi WM, Susanti IA, Astutik E, et al. Dietary diversity and associated factors among children aged 6–23 months in Indonesia. J Pediatr Nurs. 2021;56:30–4.
UNICEF. UNICEF. From the first hour of life: making the case for improved infant and young child feeding everywhere; 2008. http://data.unicef.org/topic/nutrition/infant-and-young-child-feeding/. 2016.
Njai M, Dixey R. A study investigating infant and young child feeding practices in Foni Kansala district, western region, Gambia. J Clin Med Res. 2013;5(6):71–9.
Adhikari R. Food utilization practices, beliefs and taboos in Nepal: an overview. Washington: United States Agency for International Development; 2010.
Sey-Sawo J, Sarr F, Bah HT, Senghore T. Women’s empowerment and nutritional status of children in the Gambia: further analysis of the 2020 Gambia demographic and health survey. BMC Public Health. 2023;23(1):1–13.
Poda GG, Hsu C-Y, Chao JC-J. Factors associated with malnutrition among children <5 years old in Burkina Faso: evidence from the Demographic and Health Surveys IV 2010. Int J Qual Health Care. 2017;29(7):901–8.
Pérez-Rodrigo C, Escauriaza BA, Bartrina JA, Allúe IP. Dietary assessment in children and adolescents: issues and recommendations. Nutr Hosp. 2015;31(3):76–83.
African Health Workforce Observatory aWHO. Human resources for health country profile The Gambia. https://chwcentral.org/wp-content/uploads/2016/04/gambia_country_profile.pdf. 2009.
Harpham T. Urban health in the Gambia: a review. Health Place. 1996;2(1):45–9.
Acknowledgements
The study's ethical consideration was acknowledged by the authors as being handled by the DHS program office.
Funding
No specific grant for this research was provided by funding organizations in the public, private, or nonprofit sectors.
Author information
Authors and Affiliations
Contributions
BT was involved in conceptualization, data curation, formal analysis, research, methodology, tools, software, validation, visualization, original draft writing, review, and editing. Data collection, formal analysis, research, methodology, tools, software, validation, visualization, and writing, review, and editing are all services provided by MMJ and NTA. The final manuscript was read and approved by all writers.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Online at www.dhsprogram.com, ethical approval and a letter of permission were requested, and the DHS program was given permission with permission letter number 183913 through email to access the data for this study. This study made use of freely accessible data that was completely devoid of any personal information. The GDHS provided the secondary data used in the study. Concerns about informed consent, confidentiality, anonymity, and privacy of the study sample were ethically addressed by the GDHS authorities, and we did not alter or utilize the data in any other way. Both participants and the general public were excluded from this investigation. The study's data set was publicly accessible and devoid of any private information. The study is conducted using secondary data from the GDHS. We didn't alter the data and utilized it for other purposes. Both patients and the general public were not involved in this investigation.
Consents for publication
Not applicable.
Competing interest
The authors declare no competing interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Terefe, B., Jembere, M.M. & Assimamaw, N.T. The prevalence and multilevel analysis of minimum dietary diversity intake and its determinants among 6–23 months old infants in The Gambia: further analysis of the Gambian demographic and health survey data. J Health Popul Nutr 42, 98 (2023). https://doi.org/10.1186/s41043-023-00442-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s41043-023-00442-x