
Abstract
Background
Immune checkpoint inhibitor (ICI) myocarditis is associated with significant mortality risk. Electrocardiogram (ECG) changes in ICI myocarditis have strong prognostic value. However the impact of complete heart block (CHB) is not well defined. This study sought to evaluate the impact of CHB on mortality in ICI myocarditis, and to identify clinical predictors of mortality and CHB incidence.
Methods
We conducted a retrospective cohort study of patients with ICI myocarditis at three Mayo Clinic sites from 1st January 2010 to 31st September 2022 to evaluate mortality rates at 180 days. Clinical, laboratory, ECG, echocardiographic, and cardiac magnetic resonance imaging (CMR) characteristics were assessed. Cox and logistic regression were performed for associations with mortality and CHB respectively.
Results
Of 34 identified cases of ICI myocarditis, 7 (20.6%) had CHB. CHB was associated with higher mortality (HR 7.41, p = 0.03, attributable fraction 86.5%). Among those with CHB, troponin T (TnT) < 1000 ng/dL, low white blood cell count and high ventricular rate at admission were protective. There was trend towards increased survival among patients who underwent permanent pacemaker insertion (p = 0.051), although most experienced device lead complications. Factors associated with development of CHB included prolonged PR and QRS intervals and low Sokolow Lyon Index. Where these were normal and TnT was < 1000 ng/dL, no deaths occurred. Impaired myocardial longitudinal strain was sensitive for ICI myocarditis but was not prognostically significant.
Conclusion
There is a strong temporal association between CHB and early mortality in people with ICI myocarditis. Focusing on arrhythmogenic complications can be helpful in predicting outcomes for this group of critically ill individuals.
Similar content being viewed by others


Introduction
Immune Checkpoint Inhibitor (ICI) therapy for cancer has increased substantially in the last decade with its ability to improve prognosis in a number of cancers [1]. ICI Myocarditis is a rare form of drug-induced myocardial injury characterized by infiltration of myocardial and skeletal muscle tissue with CD4 + and CD8 + T-cells [2]. Although increasingly recognized, the true incidence among those receiving ICI therapy is unclear [2, 3]. However, it is generally accepted to occur in < 1% of ICI therapy recipients. Mortality risk is high and has been estimated at 27% [2, 4].
A broad constellation of clinical data, biomarkers, electrocardiogram (ECG) and imaging parameters are used for diagnosis of myocarditis, and in some cases myocardial biopsy is undertaken [5]. ECG abnormalities in ICI myocarditis may include ventricular tachycardia and high-degree atrioventricular block, with conduction abnormalities carrying significant prognostic importance [4, 6, 7]. Other important characteristics include development of prolonged QRS, decrease in Sokolow-Lyon index, and development of pathologic Q waves [7]. The higher rates of arrhythmogenic fatality and conduction disorders are in keeping with histopathological involvement in the sinoatrial and atrioventricular nodes [2, 7]. Imaging characteristics of ICI myocarditis may differ from those in idiopathic or viral myocarditis. Cardiac magnetic resonance (CMR) has a high false negative value for ICI myocarditis compared to other types of acute myocarditis [4, 8, 9].
In the setting of suggested high mortality, and the need for a clear framework to guide clinical decision making, this study sought to examine the association between complete heart block (CHB) and mortality among patients with ICI myocarditis. Clinical demographics, biochemical and imaging characteristics were assessed for association with mortality rates and development of CHB among those with ICI myocarditis.
Methods
Study population
This study was approved by the Mayo Clinic Institutional Review Board (Application # 22–009077). Patients with ICI myocarditis were identified retrospectively from medical records using the Mayo Clinic Data Explorer system across all three Mayo Clinic Sites (Arizona, Florida and Minnesota). Patients who received ICI therapy and subsequently were diagnosed with myocarditis were identified between January 1st 2010 and September 30th 2023. Three Physician independent review with majority consensus was conducted to determine if a case met the criteria for possible, probable or definite myocarditis as defined by Bonaca et al., [5]. Patients who didn’t meet these criteria, or who had myocarditis prior to receiving ICI therapy, were excluded.
Definitions
Case definition was the presence of acute ICI myocarditis, with associated complete heart block (CHB) during inpatient hospitalization on ECG or cardiac telemetry [5]. Controls were patients with ICI myocarditis who did not have CHB during hospitalization. The primary outcome was the mortality rate within 180 days of first administration of ICI. Secondary outcome was the development of CHB.
Clinical characteristics
Clinical data were collected through review of electronic medical records. These included demographic information (age and sex), as well as pertinent co-morbidities (diabetes, hypertension, coronary artery disease, chronic obstructive lung disease, obstructive sleep apnea, prior stroke or transient ischemic attack, prior smoking, family history of premature coronary artery disease, hyperlipidemia, pericarditis, heart failure, acute coronary syndrome, prior conduction issues, prior atrial fibrillation, cancer type). Medications at admission were recorded, including anticoagulant, antihypertensive, statin, and antiplatelet agent use. Baseline and admission laboratory data were collected, including white blood cell count, 5th generation Troponin T, creatine kinase (CK), aspartate aminotransferase (AST), alanine aminotransferase (ALT), albumin and N-terminal pro-brain natriuretic peptide (NT-Pro BNP).
Baseline and admission ECG data were collected. Sokolow Lyon Index (SLI) and T-wave inversion were calculated by single physician review (SAK, YA, MOS), while other measurements were based on machine calculated readings (ventricular rate, PR interval, QRS duration, QT interval, QTc interval, P/QRS/T axis). Data for transthoracic echocardiography (TTE) was collected, where available, prior to and after ICI myocarditis, and available CMR imaging reports were reviewed. Left ventricular longitudinal strain analysis was conducted retrospectively by a single operator (TB) on admission/post-admission TTEs using the same Echo Insight software for all patients. Global, apical, mid and basal strain were assessed. For key data-points relating to ICI diagnosis (biomarkers, CMR, TTE, and presence of CHB), independent dual-entry of data was performed to ensure accurate data entry.
Analysis
Statistical analysis was performed using StataIC 16. Univariate cox regression was used to calculate and compare mortality rates among all people with ICI myocarditis. Attributable fraction was calculated using mortality rates. Nelson Aalen graphs were examined to assess validity of the proportional hazard assumption. Bivariate logistic regression was used to identify variables associated with development of CHB. Where significant data sparsity existed, Fisher’s exact test was used to assess for association between diagnostic testing and mortality risk at 180 days. Sensitivity was calculated for diagnostic testing. Associations with mortality risk and survival time among people with CHB were quantified using nonparametric methods, with the exception of use of linear regression and Pearson’s correlation coefficient where linear trend was identified on two-way scatter plot. Qualitative review was conducted among participants with ICI myocarditis with associated complete heart block (CHB).
Results
A total of 51 charts were identified on initial screening, from 8522 patients who received at least one ICI during the study period. Following three-physician independent review, 34 patients met inclusion criteria for ICI myocarditis. Of these, 7 had complete heart block (CHB). Schoenfeld residual test demonstrated no evidence of violation of the proportional hazard assumption (χ2 = 0, p = 0.95). Mortality rate for all patients with ICI myocarditis in the 180 days following ICI administration was 0.176 deaths per 100 person-days (95% confidence interval [CI]: 0.091 to 0.338). Incidence risk for ICI myocarditis was 3.99 per 1000 patients treated. Incidence risk for ICI myocarditis with CHB was 0.82 per 1000 patients treated.
Mortality with CHB
Patients with CHB had substantially higher short-term mortality compared to those without CHB. Mortality rate among those with CHB was 0.74 deaths per 100 person-days (95% CI 0.31 to 1.78), while it was 0.09 (95% CI 0.03 to 0.24) for those without CHB (Fig. 1). Hazard ratio for presence of CHB was 7.41 (95% CI 1.96 to 28.04, p = 0.03, retrospective power ≅ 100%) [10]. The population attributable fraction of CHB to overall mortality rates in people with ICI myocarditis at 180 days was 86.5%. Nonparametric testing verified a strong association between CHB and mortality risk (Fisher’s exact p = 0.007) and survival time (Rank sum p = 0.0023) at 180 days.

Kaplan Meyer Curve demonstrating cumulative survival among patients with ICI myocarditis, stratified by presence of CHB
Characteristics of patients with CHB
All 7 patients who had CHB associated with ICI myocarditis had metastatic disease. Median survival 180 days after ICI administration was 91 days (Tables 1 and 2). All patients had elevated 5th generation TnT, CK, WBC count and transaminases (AST and ALT). Shortness of breath, low TnT and WBC count and high HR were associated with reduced survival time (Tables 2 and 3), while ECG characteristic were otherwise not prognostic.
There was a trend towards association between use of a permanent pacemaker and survival (Tables 1 and 3), however this was not statistically significant (p = 0.051). Two patients declined permanent pacemaker (PPM) insertion and died shortly thereafter. Five patients underwent PPM insertion, one of whom received a leadless pacemaker. Device lead complications were present in 3 of 4 patients. One patient developed bradycardic arrest secondary to ventricular lead failure to capture (exit block), however was successfully resuscitated and the lead was replaced, after which device function appeared normal. One patient had atrial under-sensing and atrial sensing was disabled. Another patient developed atrial lead dislodgement immediately following the procedure. These two patients were transitioned to ventricular pacing, but did not develop apparent long-term structural sequelae of lead malfunction. No patient underwent magnetic resonance imaging (MRI) following pacemaker insertion.
All-cause mortality in ICI myocarditis
Several ECG characteristics were strongly associated with reduced mortality, including SLI < 13 mV (p = 0.01) and QRS duration > 120 ms (p = 0.04). TnT was also strongly associated with increased mortality rate (p = 0.01) (Table 3).
Predicting development of CHB
Baseline ECG characteristics, include first degree AV block and low SLI, were strongly associated with development of CHB (Table 4). All patients who developed CHB had QRS > 120 ms (p = 0.003). There was no significant association between laboratory findings and CHB development, however there was a non-significant trend towards increasing incidence of CHB with increasing AST level (OR for 1-unit increase 1.006, p = 0.058).
Cardiac imaging features
There was little evidence of association between TTE assessment of left ventricle systolic function and regional wall motion abnormalities (Table 5). TTE was performed in 31 cases. Twenty-four TTEs were included in analysis of strain imaging. Of the 7 patients with TTE following ICI administration where strain was not performed, one was permanently paced, one TTE was of insufficient quality, and the other 5 TTEs were not processed due to technical issues. There was no strong rank association between global or segmental longitudinal strain and CHB or mortality rates (Table 6). The median values of global, mid and basal longitudinal strain were significantly greater than -18% (> -18% defined as normal). The basal, mid and global strain values were significantly lower than the apical median strain value.
CMR was associated with modest sensitivity of 65% for diagnosis of ICI myocarditis; however, it was not prognostically significant and there was suggestion of selection bias (Table 5). CMR evidence of myocarditis (definite myocarditis) was available for 41.18% (14/34) of cases. There was no association between mortality and CMR results (Exact p = 0.35). Lack of CMR during or after index hospitalization was associated with a 16-fold increase in mortality rate at 180 days (HR for lack of CMR 16.15, 95% CI 2.01 to 129.75, p < 0.01). Failure or inability to undergo completed CMR was strongly associated with CHB incidence (Exact p = 0.012). There was a strong linear trend towards increasing mortality with increasing diagnostic certainty (Wald test p-value 0.016 for difference in HR, p = 0.69 for test for departure from linear trend, see Table 5).
Myocarditis prognostic approach
Taking into account parameters identified as being associated with increased mortality, a prognostication scale of ICI myocarditis was proposed based on the presence of the following prognostic characteristics during admission for ICI myocarditis: 1) Troponin T > 1000 ng/dL, 2) ECG PR interval > 200 ms, 3) ECG QRS interval > 120 ms, and 4) ECG Sokolow Lyon Index > 14 mV. Patients without any of these characteristics were classified as mild ICI myocarditis, those with one or more characteristics as having moderate ICI myocarditis, and those with complete heart block as having severe myocarditis. There were no deaths in the group with mild myocarditis (Table 7). For each increase in severity grade, there was a sixfold increase in mortality rate, and this difference was statistically significant (p < 0.001) (Fig. 2).

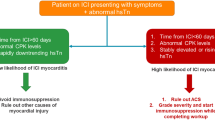
Central Illustration
Discussion
Diagnosis and prognostication in ICI myocarditis is a significant challenge. This study demonstrates the clinically important finding that the development of CHB is strongly associated with early mortality in ICI myocarditis. At 6 months, 86.5% of all-cause mortality was attributed to CHB. The remaining deaths occurred almost exclusively in patients with risk factors for development of CHB, such as prolonged QRS and reduced SLI. These findings are consistent with the initial case series of ICI myocarditis, which demonstrated infiltration of myocardium and conduction system, including the sinoatrial and atrioventricular nodes, with T-cells and macrophages [2].
This large study reviewing of over 8,500 patients receiving ICI across three states in a tertiary referral medical institution, lends additional perspective into the overall low incidence of ICI myocarditis, and insight into the predominantly conduction related mechanism for mortality. There is a range of previously reported incidences of CHB in the literature, with incidence rates of 42% (15/36 cases) in Cautela et al., [11], 15.2% (19/125) in Power et al., [7], and 8.6% (3/35) cases identified in Mahmood et al. [12]; this comes to a cumulative prevalence of 18.88% (37/196 cases) which is similar to our study’s estimate of 20.58%. The total effect of CHB on mortality however appears higher, likely due to the use of survival time analysis. This is due to this study’s unique cohort design, using mortality rate rather than risk to estimate attributable fraction and hazard ratio. Mortality risk is comparable to other ICI myocarditis cohorts, indicating good external validity [2,3,4].
Through this cohort study, we illustrate a framework for prognostication in ICI myocarditis which is dependent on more readily available troponin and ECG data, with a focus on prediction of CHB incidence. This framework is in keeping with existing evidence that both troponin and ECG measurements have significant prognostic value in ICI myocarditis [4, 7, 11, 13, 14]. In a condition where more advanced diagnostics are difficult to obtain, and where prognostic value of other investigations is limited, a focus on arrhythmogenic complications of this condition can help determine the appropriate level of care for these critically ill individuals.
Myocardial strain has been proposed as an early marker for ICI myocarditis, and is associated with elevated troponin levels [15]. It has also been suggested as a predictor of mortality [16, 17]. Although our numbers are small in the present study, we observe that despite high sensitivity, GLS did not have significant prognostic value. There are significant difficulties in obtaining CMR in this cohort in addition to limitations of low sensitivity [8, 9, 13]. There was potential bias in results of CMR testing, as CMR and echo strain data were frequently not performed in assessment of ICI myocarditis. Failure or inability to complete these studies was strongly associated with high mortality rates. The most recent guidelines relating to ICI myocarditis have removed CMR from diagnostic criteria, likely due to limited sensitivity [13, 14]. Studies examining CMR in ICI myocarditis rely on patient registries for data [8, 9]. This study demonstrates that such patients who have a CMR are much less likely to die from myocarditis. They therefore may have different (and less severe) disease on imaging than those who cannot tolerate the procedure, resulting in selection bias.
Further research including a focus on prevention and management of CHB in ICI myocarditis is required. Research to date has focused on use of immunosuppression [11]. Despite the small sample size, this study provides some data to support use of permanent pacemakers in treatment of ICI myocarditis with CHB. There may be a role for empiric device insertion in patients with high-risk features for CHB development. Given the high burden of device lead complications, use of leadless devices may be a consideration in this cohort, provided it is in line with overall patient goals of care. Early recognition of patients who are at high risk of progression to this often-fatal arrhythmia should be the focus of initial clinical evaluation.
Study limitations
There are limitations to this study. ICI myocarditis is a rare condition, and this is reflected in the small study size. This prevents use of multivariate analysis; however statistical power is retained. This is due to the high mortality rate in ICI myocarditis in general and the relatively large difference in mortality rate between those with and without CHB. This paper doesn’t examine cause-specific analysis due to the high number of out-of-hospital deaths in this cohort, as many patients were discharged to hospice care. It is challenging to adjudicate cause of death in a manner which would avoid differential misclassification, so all-cause mortality rate was used. The study cohort was limited to hospitalized patients, so results may not be generalized to the outpatient setting. Information bias was minimized by applying a standardized definition, and use of three physician majority consensus. It is possible that cases were missed where diagnosis of myocarditis was not captured in coding. The approach to severity stratification presented in Table 6 will require external validation. For associations with CHB, there were fewer than 7 cases, which introduces a risk of unstable regression analysis. This doesn’t appear to be the case, as results of the primary association can be verified with non-parametric methods.
Conclusion
Mortality in ICI myocarditis is strongly associated with CHB. ECG parameters and troponin level may help identify those who may be higher risk of development of CHB.
Availability of data and materials
Irrevocably anonymized is available upon reasonable request via email to osheam12@tcd.ie.
Abbreviations
- ICI:
-
Immune checkpoint inhibitors
- CHB:
-
Complete heart block
- TnT:
-
5Th generation troponin T
- ECG:
-
Electrocardiogram
- CMR:
-
Cardiac magnetic resonance imaging
- TTE:
-
Transthoracic echocardiogram
- SLI:
-
Sokolow Lyon Index
References
Puri P, Cortese D, Baliga S. A time series analysis of immune checkpoint inhibitor use in the United States Medicare population: 2014–2019. J Dermatolog Treat. 2022;33(4):2004–7.
Johnson DB, Balko JM, Compton ML, Chalkias S, Gorham J, Xu Y, Hicks M, Puzanov I, Alexander MR, Bloomer TL, et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N Engl J Med. 2016;375(18):1749–55.
Salem JE, Manouchehri A, Moey M, Lebrun-Vignes B, Bastarache L, Pariente A, Gobert A, Spano JP, Balko JM, Bonaca MP, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol. 2018;19(12):1579–89.
Escudier M, Cautela J, Malissen N, Ancedy Y, Orabona M, Pinto J, Monestier S, Grob JJ, Scemama U, Jacquier A, et al. Clinical Features, Management, and Outcomes of Immune Checkpoint Inhibitor-Related Cardiotoxicity. Circulation. 2017;136(21):2085–7.
Bonaca MP, Olenchock BA, Salem J-E, Wiviott SD, Ederhy S, Cohen A, Stewart GC, Choueiri TK, Carli MD, Allenbach Y, et al. Myocarditis in the Setting of Cancer Therapeutics. Circulation. 2019;140(1):80–91.
Power JR, Alexandre J, Choudhary A, Ozbay B, Hayek S, Asnani A, Tamura Y, Aras M, Cautela J, Thuny F, et al. Electrocardiographic Manifestations of Immune Checkpoint Inhibitor Myocarditis. Circulation. 2021;144(18):1521–3.
Power JR, Alexandre J, Choudhary A, Ozbay B, Hayek SS, Asnani A, Tamura Y, Aras M, Cautela J, Thuny F, et al. Association of early electrical changes with cardiovascular outcomes in immune checkpoint inhibitor myocarditis. Arch Cardiovasc Dis. 2022;115(5):315–30.
Zhang L, Awadalla M, Mahmood SS, Nohria A, Hassan MZO, Thuny F, Zlotoff DA, Murphy SP, Stone JR, Golden DLA, et al. Cardiovascular magnetic resonance in immune checkpoint inhibitor-associated myocarditis. Eur Heart J. 2020;41(18):1733–43.
Thavendiranathan P, Zhang L, Zafar A, Drobni ZD, Mahmood SS, Cabral M, Awadalla M, Nohria A, Zlotoff DA, Thuny F, et al. Myocardial T1 and T2 Mapping by Magnetic Resonance in Patients With Immune Checkpoint Inhibitor-Associated Myocarditis. J Am Coll Cardiol. 2021;77(12):1503–16.
Sterne BKJ. Essential Medical Statistics. (2nd Edition). United Kingdom: Wiley Global Research (STMS); 2003.
Cautela J, Zeriouh S, Gaubert M, et al. Intensified immunosuppressive therapy in patients with immune checkpoint inhibitor-induced myocarditis. J Immuno Ther Cancer. 2020;8:e001887. https://doi.org/10.1136/jitc-2020-001887.
Mahmood SS, Fradley MG, Cohen JV, Nohria A, Reynolds KL, Heinzerling LM, Sullivan RJ, Damrongwatanasuk R, Chen CL, Gupta D, et al. Myocarditis in Patients Treated With Immune Checkpoint Inhibitors. J Am Coll Cardiol. 2018;71(16):1755–64.
Thuny F, Bonaca MP, Cautela J. What Is the Evidence of the Diagnostic Criteria and Screening of Immune Checkpoint Inhibitor-Induced Myocarditis? CardioOncology. 2022;4(5):624–8.
Herrmann J, Lenihan D, Armenian S, Barac A, Blaes A, Cardinale D, Carver J, Dent S, Ky B, Lyon AR, et al. Defining cardiovascular toxicities of cancer therapies: an International Cardio-Oncology Society (IC-OS) consensus statement. Eur Heart J. 2022;43(4):280–99.
Tamura Y, Tamura Y, Takemura R, Yamada K, Taniguchi H, Iwasawa J, Yada H, Kawamura A. Longitudinal Strain and Troponin I Elevation in Patients Undergoing Immune Checkpoint Inhibitor Therapy. JACC:CardioOncology. 2022;4(5):673–85.
Awadalla M, Mahmood SS, Groarke JD, Hassan MZO, Nohria A, Rokicki A, Murphy SP, Mercaldo ND, Zhang L, Zlotoff DA, et al. Global Longitudinal Strain and Cardiac Events in Patients With Immune Checkpoint Inhibitor-Related Myocarditis. J Am Coll Cardiol. 2020;75(5):467–78.
Quinaglia T, Gongora C, Awadalla M, Hassan MZO, Zafar A, Drobni ZD, Mahmood SS, Zhang L, Coelho-Filho OR, Suero-Abreu GA, et al. Global Circumferential and Radial Strain Among Patients With Immune Checkpoint Inhibitor Myocarditis. JACC Cardiovasc Imaging. 2022;15(11):1883–96.
Acknowledgements
The authors gratefully acknowledge Scott A. Sheffield MS and GetBodySmart for permission to use their illustrations.
Funding
This project did not receive funding.
Author information
Authors and Affiliations
Contributions
Michael P O’Shea – Assisted with study conception and took primary responsibility for the conduct of the study, collected and analyzed data, contributed to three physician review of cases, wrote and re-drafted the final manuscript and approved the final manuscript. Suganya Arunachalam Karikalan – Assisted with study conception and developed the data collection protocol, collected data, assisted with re-drafting article and approved the manuscript submitted. Ali Yusuf – Assisted with study conception, collected data, assisted with re-drafting the article and approved the manuscript submitted. Timothy Barry – Assisted with study conception, conducted retrospective strain analysis on transthoracic echocardiography data, assisted with re-drafting the article, approved the manuscript submitted. Eiad Habib – Assisted with study conception, collected data, contributed to three physician review of cases, assisted with re-drafting the article, approved the final manuscript. John O’Shea – Assisted with interpretation of data, obtained approval for secondary use of illustration used in study primary illustration, interpretation of data, development of key figures for study, assisted with re-drafting, approved the final manuscript. Michael Killian – Assisted with interpretation of data, assisted with data collection and figure design, assisted with re-drafting, approved the final manuscript. Eman Baqal – Assisted with data collection and interpretation, assisted with manuscript revision, final approval of the manuscript submitted. Srishti Nayak – Assisted with data collection and interpretation, assisted with manuscript revision, final approval of the manuscript submitted. Joerg Hermann – Contributed data from Mayo Clinic Rochester, contributions to critical review of manuscript, final approval of manuscript submitted. Rajeev Masson – Assisted with data interpretation and data collection protocol, assisted with manuscript revision, final approval of the manuscript submitted. Shimoli Shah – Assisted with study conception and design, major contributions to critical review of manuscript, final approval of the manuscript submitted. Chadi Ayoub – Assisted with study conception and design, assisted with cardiac imaging data collection and interpretation, major contributions to critical review of the manuscript, final approval of the manuscript submitted. Hicham El Masry – Primary supervising consultant and research mentor to the primary author, assisted in study conception and design, obtained IRB ethical approval, major contributions to critical review of the manuscript, final approval of the manuscript submitted.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Mayo Clinic Institutional Review Board (Application # 22–009077).
Consent for publication
Participant approval for data to be used for research and publication was obtained prior to inclusion in the Mayo Data Explorer Database.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
O’Shea, M.P., Karikalan, S.A., Yusuf, A. et al. Complete heart block is a significant predictor of mortality in immune checkpoint inhibitor myocarditis. Cardio-Oncology 9, 34 (2023). https://doi.org/10.1186/s40959-023-00185-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40959-023-00185-y