
Abstract
Background
Burn injuries remain a consistent challenge for providers of medical care worldwide and thus the current focus of medical professionals is on improving treatments and reducing the incidence of burns altogether. We conducted a literature search to summarize worldwide promoted burn prevention strategies.
Methods
A review of the Medline database was conducted using PubMed interface. Abstract screening and full-text analysis of eligible article was performed. Burn prevention strategies were summarized and sorted by origin.
Results
Between 2005 and now, 34 articles regarding burn prevention have been published. Seventy four percent of the articles were published in high income countries, followed by middle income countries with 18 % and low income countries with 9 % of all the manuscripts. The United States published the most articles (n = 17), followed by the United Kingdom (n = 5), and Iran (n = 3).
Conclusions
Although many hardships and barriers need to be overcome, it is more than worthwhile that high income countries should invest a great amount of effort to help low and middle income countries to create strategies to prevent burn injuries, as those burns, which do not occur will always have the best outcome.
Similar content being viewed by others


Background
Burn injuries remain a consistent challenge for providers of medical care worldwide, with approximately 300,000 fatalities and millions of patients affected by long-term consequences of thermal injuries each year. Two general approaches are taken to tackle this problem: improve treatment and reduce the incidence of burns altogether. Means and modalities of burn care and their respective outcomes are continuously improving, resulting for instance in decreased mortality from 6.2 to 3.2 %, shortened length of hospitalization from 13 to 8.6 days and increasing survival rates even for most extensive total body surface area (TBSA) burns over the last two decades in the US [1, 2].
Keynote lectures at the European Burn Conference in 2015 have brought up the discrepancies in the causes of burns depending on the income of the country. Thus tailored burn prevention strategies are required for each geographical location to ensure a reduction of burns. The WHO, American Burn Association and others have designed burn prevention strategies to accomplish the individual needs of burn prevention.
However, there is no general summary of all those prevention strategies which shows similarities and controversies of each approach. We aimed to conduct a brief literature search to summarize currently available burn prevention strategies and show up which countries are developing those.
Methods
Medical literature was reviewed in order to identify all studies of burn prevention, and burn prevention strategies. A review of the Medline database was conducted using PubMed (accessed 03/01/2016) interface. We limited the search to only articles written in the English language and published between 2005 and now. In addition, the same terms were used for google.com searches to detect further not PubMed listed articles.
On the PubMed interface, we used the following search terms: (“prevention”[Title] OR “awareness”[Title] AND (“burns”[MeSH Terms] OR “burns”[MeSH Terms] OR “burn”[MeSH Terms] OR “thermal trauma”[MeSH Terms]).
Abstract screening and when appropriate full-text analysis of eligible article was performed and all burn prevention strategies were summarized in Table 1. Special focus on geographical differences based on the income [3] of the several countries were summarized.
Results
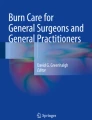
From 854 identified articles in PubMed, 34 were eligible for full-text analysis (Fig. 1). Most burn prevention strategies were published in the United States of America and Canada (50 %), followed by the European Union (21 %) and the Middle East (18 %, Fig. 2). Asia was the origin of 6 % of the manuscripts, and 3 % came from Africa as well as Australia. 74 % of the articles were published in high income countries. Whereas middle income countries published 18 % and low income countries 9 % of all the manuscripts. The United States was the country with the most articles published (n = 17), followed by the United Kingdom (n = 5), and Iran (n = 3, Table 1).

Flow chart

Map showing the distribution of the income classes and percent of prevention articles published between 2005 and now
Discussion
Our study showed that most of the burn prevention strategies were published in high income countries, which did not necessarily mean that they described burn prevention of those countries. A handful of those studies described prevention strategies for Africa and the Middle East. No prevention strategies were published in South America as well as Russia, which both can be graded as middle income countries [3]. Interestingly, all of the published strategies can be found in the strategies developed by the WHO (Table 2). Thus we assume that a general approach to prevent burns in LMIC must be provided high income countries, which have already established low incidences of burns and thus can provide knowledge to LMIC.
Prevention efforts have been accompanying these positive developments for decades: by means of education, changes in engineering, adapting and enforcing protective legislature and environmental modifications, the overall incidence of burn injury could be lowered substantially in the US. Limiting water heater temperatures and installment of smoke detectors are two widespread examples of primary prevention [4]. Furthermore governmental and non-governmental agencies are enhancing secondary prevention through educating the public on how to respond to thermal injury ideally when it does occur. Leaflets, social media PSAs and safety instructions at the workplace are only few examples of undertaken measures [5].
For example this year in February, Shriners Hospitals for Children are launching a year-long campaign entitled “Burn Awareness” [6]. In an educational video for children and adults, two comic characters, Boots and Brewster, are leading children through several rooms in a household to point out dangers and to teach how to avoid them. The video can be downloaded for free. In addition, activity books, which are provided in several languages, focusing on burn prevention and awareness can also be ordered via the Shriners Hospitals for Children homepage.
As encouraging as these accomplishments are, one must be mindful that they have only been achieved for developed high-income countries (HIC) such as the US and most countries of Europe. However, 95 % of annual burn injuries occur in countries of low and middle income (LMIC), where mortality rates are up to 10 times higher than in their high income counterparts [7]. In a joint effort to improve this situation, the World Health Organization (WHO) and the International Society for Burn Injuries (ISBI) launched “A WHO plan for burn prevention and care” in 2008, a 10-year prospective program designed to reduce thermal injury risks and standardize fundamental principles of burn treatment in LMIC [7].
Key goals of the program are to raise awareness for burn related problems, influence policies, regulations, legislation and their enforcement and to develop prevention programs and national burn strategies. The potential of preventive measures cannot be overrated in terms of cost-effectiveness, as there has been convincing data from the US which demonstrated manifold savings in health expenditure for every dollar spent on preventive measures [8]. With this in mind, a great deal of WHO’s prevention measures for LMIC target the same objectives as in HIC (smoke detectors, hot water temperature regulation, safety regulations for electric wiring, etc.). On the contrary, other risk factors are unique to the conditions in underdeveloped regions such as cooking with open fire, pots on ground level, use of kerosene lamps and easily ignitable loose clothing and thus need to be addressed specifically.
Another important aim of the WHO plan is to improve and standardize treatment for burn injuries. This is not only limited to acute care in specialized hospitals, but also includes educating the public on how to correctly react immediately after a burn occurs. Measures that are already widely taught in HIC through government and non-government agencies, such as immediate cooling, removing all clothing from the burned area and applying dry cloth while avoiding any creams, ointments or home remedies, are supposed to be introduced in LMIC as well. An encouraging large cohort study was recently published out of Shanghai, where the percentage of patients who had been educated on these effective methods via traditional media, internet or workplace education had a significantly better outcome across all types of burn injuries [9].
The current research has several limitations. The timeframe, 2005 up to now, as well as the use of PubMed only are definitively limitations of the study. We further included articles which have been published in English and thus our calculations regarding the origin of the prevention strategies might have been biased.
Lastly, a key goal of the WHO plan is to collect research data in an organized and comprehensive manner in order to validate the effectiveness of the undertaken efforts, as well as to provide valuable insights for the research community and future improvement of treatment and prevention programs [7].
Conclusions
Although many hardships and barriers need to be overcome, it is more than worthwhile that high income countries should invest a great amount of effort to help LMIC to create strategies to prevent burn injuries, as those burns, which do not occur will always have the best outcome.
References
American Burn Association. 2015 National Burn Repository [http://www.ameriburn.org/2015NBRAnnualReport.pdf]
Miller SF et al. National Burn Repository 2005: a ten-year review. J Burn Care Res. 2006;27(4):411–36.
The World Bank Group. Grouping Countries by Their Level of Development [http://www.worldbank.org/depweb/beyond/global/chapter2_2.html]
Peck M, Molnar J, Swart D. A global plan for burn prevention and care. Bull World Health Organ. 2009;87(10):802–3.
The U.S. Fire Administration. Working for a fire-safe America [www.usfa.fema.gov/citizen/focus]
Shriners Hopsitals for Children. Be Burn Aware [www.burnawareness.org]
Mock C et al. A WHO plan for burn prevention and care. Geneva: World Health Organization; 2008.
Haddix AC et al. Cost effectiveness analysis of a smoke alarm giveaway program in Oklahoma City, Oklahoma. Injury Prevention. 2001;7(4):276–81.
Ji SZ et al. Pre-hospital emergency burn management in Shanghai: analysis of 1868 burn patients. Burns. 2012;38(8):1174–80.
World Health Organization. Success Stories, Lessons Learned [http://apps.who.int/iris/bitstream/10665/97938/1/9789241501187_eng.pdf]
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hundeshagen, G., Wurzer, P., Forbes, A.A. et al. Burn prevention in the face of global wealth inequality. Saf Health 2, 5 (2016). https://doi.org/10.1186/s40886-016-0016-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40886-016-0016-7