
Abstract
Background
Increases in maximal strength and muscle volume represent central aims of training interventions. Recent research suggested that the chronic application of stretch may be effective in inducing hypertrophy. The present systematic review therefore aimed to syntheisize the evidence on changes of strength and muscle volume following chronic static stretching.
Methods
Three data bases were sceened to conduct a systematic review with meta-analysis. Studies using randomized, controlled trials with longitudinal (≥ 2 weeks) design, investigating strength and muscle volume following static stretching in humans, were included. Study quality was rated by two examiners using the PEDro scale.
Results
A total of 42 studies with 1318 cumulative participants were identified. Meta-analyses using robust variance estimation showed small stretch-mediated maximal strength increases (d = 0.30 p < 0.001) with stretching duration and intervention time as significant moderators. Including all studies, stretching induced small magnitude, but significant hypertrophy effects (d = 0.20). Longer stretching durations and intervention periods as well as higher training frequencies revealed small (d = 0.26–0.28), but significant effects (p < 0.001–0.005), while lower dosage did not reach the level of significance (p = 0.13–0.39).
Conclusions
While of minor effectiveness, chronic static stretching represents a possible alternative to resistance training when aiming to improve strength and increase muscle size. As a dose-response relationship may exist, higher stretch durations and frequencies as well as long program durations should be further elaborated.
Key Points
-
• While animal research consistently showed chronic stretch-mediated hypertrophy and strength increases, literature in humans draws an inconclusive picture, possibly due to lack of comparability of stretching parameters, such as duration and frequency.
-
• Our systematic review is the first that included studies using comparable stretching durations of up to two hours in humans, which showed small magnitude maximal strength increases and muscle hypertrophy.
-
• Even though less effective, high volume stretching might provide a sufficient alternative to strength training when aiming to induce muscle hypertrophy and strength increases. It must be noted that comparatively high training effort is opposed by comparatively small adaptations, suggesting a preference for the more efficient strength training if applicable.
Similar content being viewed by others

Background
Stretch training is commonly used to achieve improvements in flexibility [1, 2], with widespread applications in sports conditioning and orthopedic physical therapy [3, 4]. While it was widely accepted in the 1980s that static stretching should be included in warm-up routines [5,6,7], current evidence questions the implementation of (static) stretching during warm-up due to its detrimental impact on subsequent sports performance [8,9,10].
Despite adverse acute effects, static stretching may be beneficial for athletes if performed in the long-term [11, 12]. A recent systematic review with meta-analysis evaluating animal studies found chronic stretching of the anterior latissimus dorsi in chickens and quails (for up to 24 h per day, seven days per week) substantially increased muscle mass by up to 319% (d = 8.5) due to increases in muscle cross-sectional area (up to 142%; d = 7.9). Besides these structural changes, gains in maximal strength (up to 95%; d = 12.4) [13] were observed. Interestingly, investigations aiming to translate animals’ muscle adaptions to humans were requested as early as in 1983: “Thirty minutes of stretching per day is certainly within normal physiological limits, and as a result may be applied to human muscle with hopes that similar adaptations would occur” [14].
Stretching effects on hypertrophy [15, 16] and strength [17, 18] in humans were previously reviewed pointing out only small strength increases (under dynamic conditions [17]) while muscle hypertrophy was exclusively evident using high intensity stretching [16]. However, even though recent reviews were performed in 2023, they missed inclusion of new literature that – for the first time – applied static stretching with continuous stretching durations up to two hours [19,20,21,22,23,24,25,26], which might lead to an under- or overestimation of the current evidence.
Consequently, the aim of this systematic review with meta-analysis was to investigate changes in muscle size and maximum strength following chronic static stretching interventions in humans. We hypothesized that stretching programs, performed in the long-term, would lead to increases in both outcomes. Based on findings from animal research, we assumed that previous stretching volume was not sufficient. Therefore, we hypothesized longer stretching session durations and intervention periods, as well as high training frequencies would trigger improvements, while lower durations/frequencies would not elicit relevant changes.
Methods
A systematic review and meta-analysis using robust variance estimation was performed adhering to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The study was registered in the PROSPERO database (CRD42023411225).
Literature Search
Two independent investigators (KoW & LHL) conducted a systematic literature search using MEDLINE/PubMed, Web of Science and SPORTDiscus (March 2023) and updated in January 2024. The following inclusion criteria were applied: (1) randomized, controlled study design; (2) static stretching intervention with a duration of at least two weeks, performed in humans; (3) measurement of (a) maximal strength or related parameters such as active peak torque and/or (b) markers of muscle size (i.e., cross-sectional area, muscle thickness). Studies assessing acute effects, combining static stretch training with other (active) training protocols such as resistance training or neuromuscular facilitation, or including patients were excluded. The search terms (Online Supplemental Material) were created based on the requirements of each database. As an example, the terms for PubMed were as follows:
((stretch*) AND (performance OR strength OR 1RM OR force OR MVC OR (maxim* AND “voluntary contraction”) OR hypertrophy OR “muscle cross-sectional area” OR CSA OR “muscle thickness” OR “muscle mass” OR “muscle volume”) NOT (acute OR postural OR pnf OR “proprioceptive neuromuscular facilitation” OR “stretch shortening”)).
In addition to database searches, the reference lists of all included studies were screened for further eligible articles [27].
Methodological Study Quality and Risk of Bias
The assessment of study quality was performed by two independent investigators (KW1 & LHL) using the PEDro scale for randomized, controlled trials [28, 29]. If consensus could not be reached, a third rater casting the decisive vote was consulted (MK). The PEDro scale (Table A in Supplemental Material) was used in previous reviews with meta-analysis on exercise and exercise therapy [30, 31].
Risk of publication bias was examined using visual inspection of funnel plots [32], which were created using the method of Fernandez-Castilla et al. [33]. Additionally, Egger’s regression tests incorporating robust variance estimation for funnel plot asymmetry were applied [34]. The certainty about the evidence was rated as very low, low, moderate or high using the criteria proposed by the GRADE working group [35]. Generally, the quality of evidence of randomized trials is considered high and thereafter adjusted within the GRADE framework. In case of limitations in study design or execution, inconsistency of results, indirectness of evidence, imprecision or publication bias, one point is subtracted for each weakness. Conversely, large-magnitude effects or a dose-response gradient each lead to addition of one point to the quality of evidence rating.
Data Processing and Statistics
The means (M) and standard deviations (SD) from pre- and post-intervention tests were extracted for all parameters and study arms (stretching and inactive control). In case of missing data, the authors of the primary studies were contacted. Changes from pre to post were computed as M(posttest) – M(pretest) and standard deviations were pooled as
To account for multiple within-study outcome dependency with unknown origin of covariances, meta-analytical calculation was performed using robust variance estimation [36]. Standardized mean differences (SMD) and 95% confidence intervals (CI) for maximal strength capacity and muscle size changes (including both muscle thickness and muscle cross-sectional area) were pooled from fitting parameters from all included studies. We used R (R Foundation for Statistical Computing, Vienna, Austria) with the robumeta, version 2.0 [36] and metapackages. Obtained effect sizes (ES) were interpreted as 0 ≤ d < 0.2 trivial, 0.2 ≤ d < 0.5 small, 0.5 ≤ d < 0.8 moderate, or d ≥ 0.8 large [37], while τ² was used to explore study outcome heterogeneity, with classifications equal to effect sizes.
Meta-regression was performed using the robumeta package for dependent study outcomes, as described by Fisher & Tipton [36]. Furthermore, to quantify the influence of quantifable outcome moderators (stretching duration, intervention period and training frequency) when aiming to enhance maximal strength and muscle size, sub-analyses were performed for three variables: intervention duration, session duration and exercise frequency. For moderating variables (duration, intervention period and training frequency), we used the median-split for cut-off determination (intervention duration: small: <6 weeks vs. high: ≥ 6 weeks, frequency: low: <5 sessions vs. high: ≥5 sessions, stretching duration: short: <15 min vs. long: ≥15 min. To test for significant differences in mean effect size of sub-groups, the Welsh test was performed due to violation of normal distribution. If several study effects were presented mean effects for each study were calculated to account for within-study dependency in effect size comparsions.
Results
Search Results
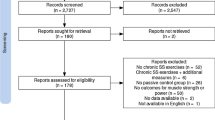
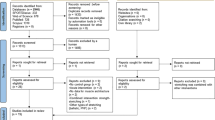
Figure 1 displays the flow of the literature search.

Flow chart of literature search
Collectively, the queries in the three databases returned 10,427 hits. After application of inclusion and exclusion criteria, a total of 42 eligible studies with 1318 participants were identified. Among these, 36 studies with 85 ES [19,20,21,22,23,24,25,26, 38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65] investigated strength parameters. Nineteen (19) studies [21,22,23,24, 26, 39, 66,67,68, 51, 52, 55, 57, 58, 69,70,71, 63, 65] with 45 ES examined markers of muscle size.
Methodological Quality, Risk of Bias and Quality of Evidence
Per average, the methodological quality of the included studies was rated as fair [72] (mean 4.17 ± 1.4 out of 10 points; range 2 to 8 points; see Table A in Supplemental Material). For both outcomes (muscle volume and maximal strength), the quality of evidence was downgraded by 2 levels (high to low) due to high risk of bias (limitations in study quality: fair PEDro score and heterogeneity in study designs). In case of the sub-analyses for session and intervention duration (outcomes of maximal strength), the quality of evidence was upgraded by one level due to moderate to strong associations (low to moderate effect sizes, mostly on same side effect).
Quantitative Synthesis
Table 1 provides the study characteristics of included articles, while Table 2 summarizes the quantitative analysis results for overall and different subgroups.
Maximal Strength Capacity
Static stretching showed a small positive effect on maximal strength (d = 0.30, p < 0.001, 95% CI 0.14 to 0.46, τ²=0.01, 36 studies with 85 ES, Table 1). The certainty about the evidence is low. Meta-regression showed stretching duration positively influenced maximal strength (p = 0.04, estimate: 0.005), while a tendency was reported for intervention period (p = 0.06, estimate: 0.06). No significant result could be found for training frequency (p = 0.64).
Accordingly, higher stretch durations (≥ 15 min) induced small strength increases (d = 0.45, p < 0.001, 95% CI 0.29 to 0.62, τ²=0.0, 14 studies, 30 ES, Fig. 2) which were opposed to shorter durations (< 15 min) which revealed a small-magnitude, not significant effect (d = 0.21, p = 0.06, 95% CI -0.06 to 0.44, 22 studies, 55 ES, Fig. 3) with a significant mean ES difference (p = 0.01). The certainty about the evidence is moderate.

Illustrates the meta-analytical results of long stretching durations. Legend: 1RM = one repetition maximum, EL = extended leg, FL = flexed leg

Illustrates the meta-analytical results of short stretching durations. Legend: HI = high intensity group, LI = low intensity group, 1RM = one repetition maximum
Similar to stretch duration, longer program durations (> 6 weeks) achieved small strength increases (d = 0.36, p = 0.003, 95%CI 0.13 to 0.59, τ²=0.04, 24 studies with 51 ES) while shorter durations yielded only trivial improvements (d = 0.16, p = 0.006, 95%CI 0.05 to 0.26, τ²=0.0, 12 studies, 34 ES), with a significantly higher mean effect for longer intervention periods (p = 0.03). The certainty about the evidence is moderate. High training frequencies (more than five stretching sessions per week) led to small-magnitude strength increases (d = 0.32, p = 0.025, 95% CI 0.05 to 0.6, τ²=0.04, 16 studies, 40 ES). Less than five sessions per week yielded only a small effect size (d = 0.26, p < 0.001, 95%CI 0.14 to 0.38, τ²=0, 20 studies with 45 ES), without a significant difference in group mean effects (p = 0.39). The certainty about the evidence is low.
Hypertrophy
For hypertrophy, a trivial positive effect of stretching was found (d = 0.20, p = 0.003, 95% CI 0.08 to 0.32, τ²=0.0, 19 studies, 45 ES) (see Fig. 4). The certainty about the evidence is low. While the meta regression (p = 0.23–0.88) revealed no significant influence of any included moderator, long-duration stretching (≥ 15 min) had a small effect size (d = 0.28, p = 0.005, 95% CI 0.12 to 0.44, τ²=0.0, 7 studies, 17 ES) without a significant difference compared to shorter durations (p = 0.29) that, in turn, failed reaching a significant effect (d = 0.13, p = 0.14, 95%CI -0.05 to 0.30, τ²=0.0, 12 studies with 28 ES). Similarly, studies that performed stretching for more than 6 weeks revealed d = 0.26, p < 0.001 extracted from 16 studies with 35 ES, while shorter training periods failed to reach the level of significance (d= -0.05, p = 0.13 from 3 studies and 10 ES) with higher effects for longer periods (p = 0.006). If stretching was performed more than 5 times per week, there were significant small magnitude increases in muscle size (d = 0.27, p = 0.002, from 11 studies with 28 ES), opposed by no significant effect for lower training frequencies (d = 0.09, p = 0.39), without a significantly higher mean effect size for higher frequencies (p = 0.31). The certainty about the evidence is low for all effects.

Forest plot for all included studies on stretch-mediated hypertrophy
Publication Bias
Visual inspection of funnel plots (Fig. 5) revealed no indication of a publication bias for maximal strength as well as for muscle volume. Consistently, for both outcomes, Egger’s regression tests showed no publication bias p = 0.23–0.31.

Shows funnel plots for visual publication bias inspection, with (a) for maximal strength studies and (b) for hypertrophy studies. Plot size illustrates the number of outcomes in the respective study that were pooled and weighted in the meta-analytical calculation
Discussion
In accordance with previous research, the present systematic review found chronic static stretching to increase (a) maximum strength [11, 12, 17, 18], and (b) muscle size [16]. With stretching duration and a tendency for intervention time as moderating training parameters for maximal strength, our results indicate longer stretching durations to be of superior effectiveness. While overall stretch-induced hypertrophy showed small effects (d = 0.2), these effects seem attributable to stretching durations of ≥ 15 min, intervention periods of > 6 weeks and training frequencies of ≥ 5 times as lower dosage did not reach the level of significance in subgroup calculations (p = 0.14–0.39). The possible necessity of high stretching volumes with regard to improvements in strength and muscle volume is in line with results from animal studies [73, 74].
As pointed out, early evidence had mostly suggested that stretching does not modify morphological and functional muscle parameters in humans [11, 12, 15]. However, this assumption was based on a lack of studies using high to very high stretch durations. Even the most recent review of Arntz et al. [18] did not include long duration studies [19,20,21, 25, 26, 75, 76], while Panidi et al. [16] included only one long-duration study [26]. Since animal research indicated a potential dose-reponse relationship [14, 77], a meta-regression was performed that confirmed stretching duration to significantly moderate strength adaptations. While in contrast, the regression did not reveal such a relationship for muscle hypertrophy, significant muscle size enhancements were only obtained in higher dosage in subgroup analyses (≥ 15 min stretching, ≥6 weeks intervention period, ≥5x stretching per week). Compared to animals with reported muscle mass increases of up to 300% [78], human hypertrophy effects must be considered small. These differences could be attributed to diverse factors. Compared to animals, human muscle protein synthesis is slower [79,80,81]. This may be one explanation for a lack of hypertrophy in response to 30 min of stretch reported by Yahata [65]. Nevertheless, by using stretching durations of accumulated 15 min per session, Wohlann et al. [20] obtained significant muscle hypertrophy. There were differences in the intervened muscle groups, Wohlann used 4x weekly pectoralis stretching, while calf muscle stretching performed by Yahata and colleagues [65] was applied only twice per week. The potential role of training frequency is supported by consistent hypertrophy effects in all Warneke et al. studies [23, 24, 26], who used daily stretching. The results of the meta-analysis partly confirm this assumption, although meta regression did not reach the level of significance for both, maximal strength and hypertrophy. However, subgroup analysis for hypertrophy showed only more frequent training application to produce significant effects, while no significant influence of frequency was observed for strength increases.
Several mechanisms could explain the stretch-induced increases in muscle size or strength. First and foremost, it may be speculated that time under tension is not only paramount for gains in muscle volume following resistance training [82] but also following stretching [83], which would be in agreement with our results, showing the stretching duration to be important for strength (meta regression: p = 0.038), but also for hypertrophy, as only with ≥ 15 min muscle size did increases occur. Accordingly, the literature shows high mechanical tension imposed on the sarcomere could trigger protein synthesis [84, 85]. In quails and chickens, progressive stretching induced fast hypertrophy alongside serial sarcomereogenesis during the first days of the intervention [78]. However, when the stretching stimulus remained unmodified during such a program, initial increases in muscle cross-sectional area started to disappear [86]. Ashmore [87] suggested that the mechanical tension caused by stretching would lead to high stresses and compensatory adaptations in the sarcomere. It has, furthermore, been hypothesized that an increased total amount of sarcomeres reduces tension and with this stress on the individual sarcomere [86]. Thus, to increase training intensity and to ensure continuously strong tensioning of the sarcomere, the stretching stimulus needs to be re-adjusted. Indeed, Antonio & Gonyea [78] achieved the highest gains in muscle mass and hypertrophy by increasing the stretch intensity, starting with 10% of the body weight up to 35% after 5 weeks of chronic stretch in quails.
Another theory postulates that chronic stretch creates hypoxic conditions which are similar to those during blood flow restriction. Reducing arterial perfusion has been demonstrated to increase lactate levels, growth hormone concentrations, and inflammatory cytokines such as interleukin-6 [88, 89]. Such metabolic milieu may represent a potent stimulus for mTOR signaling [90,91,92]. Interestingly, Jessee et al. [93] showed that blood flow restriction induces hypertrophy, however, it seems of minor relevance for maximum strength increases. Hotta et al. [94] observed acute decreases of blood flow during 30 min of stretching in animals. Studies measuring the metabolic muscle response to stretching would thus be warranted in order to further delineate the potential relevance of the abovementioned factors.
In sum, irrespective of initial processes, muscle hypertrophy requires an increase in muscle protein synthesis. Suzuki & Takeda [95] and Kremer [96] described the activation of stretch-activated channels and thus, the stimulation of the mTOR/p70S6K/PI3K pathway [97,98,99]. The literature emphasizes the importance of mechanical tension (e.g., through stretching) to trigger anabolic signaling pathways, with the stimulation of protein synthesis [100,101,102,103] as an underlying mechanism of hypertrophy (and maximal strength) [104,105,106]. Van der Pjil et al. [107, 108] indicated the relevance of titin unfolding in hypertrophy (in parallel and longitudinal), supporting the hypothesis of high intensities [109]. Conversely, Fowles et al. [110] were not able to show acute increases in protein synthesis after 33-minutes of stretching in humans, although significant increases in protein synthesis rates had been reported in animals [100, 102, 103, 111]. The stronger response in animals could hence be explained by a higher protein synthesis rate [80, 81].
With regard to the increases in maximum strength, it may be expected that the increases in muscle volume would drive the strength gains. This would require hypertrophy to precede enhanced strength. However, no study has investigated the temporal association of both factors. In addition, effect sizes were trivial to small for muscle volume but moderate for strength. Another theory may attribute the improvements to neural adaptations [112, 113]. The studies by Warneke et al. [19, 26] and Nelson et al. [60], on the one hand, provide support for this assumption as they detected strength increases in the non-stretched contralateral leg. However, on the other hand, Holly et al. [114] and Barnett et al. [115] showed no significant increase in EMG activity during stretching in animals. Furthermore, Sola et al. [116] found stretch-mediated hypertrophy in denervated muscles, indicating a minor role of neural aspects. Therefore, to clarify the role of neural aspects in stretch-mediated adaptations, further research seems necessary.
Even though muscle hypertrophy only occurs using higher dosage stretching, our work has significant clinical implications. In general, stretching may represent an alternative to conventional resistance training interventions inducing muscle size- and strength increases. Nevertheless, several aspects must be considered. While Currier et al. [117] showed moderate to large magnitude maximal strength and muscle size increases of ES = 0.51 and ES = 1.60, respectively, when using resistance training, the present study’s small magnitude effect sizes of ES = 0.28 and ES = 0.45, respectively, showed that even long stretching durations were less effective. Assuming about one hour of stretching on one isolated muscle to achieve meaningful muscle hypertrophy [83] seems, on the one hand, of limited practical relevance [85]. On the other hand, passively induced mechanical tension via stretch training could be included into daily life, with for example using splints/ortheses during sitting in the office or while watching television [118]. A further benefit might be the potential applicability for people lacking motivation or ability to perform resistance training (e.g., patients with unstable cardiovascular diseases), if heavy resistance training is contraindicated, or after muscle, ligament or bone injuries leading to prolonged times of immobilization. Thus, (probably only) for conditioned populations, stretching could provide a sufficient alternative, especially since no training supervision is necessary to ensure safe exercise execution. Although stretching could be a valuable training intervention, it should only temporarily substitute or, even better, supplement classical training regimes. This is of importance because although stretching has been shown to be beneficial for cardiovascular health [119], it may not add as efficiently to the recommended levels of physical activity (e.g. by the World Health Organization, 150 min of moderate or 75 min of vigorous activity per week) as other activities such as walking, running, team sports, or resistance training.
Several aspects call for further research. Even though significant stretch-induced muscle hypertrophy in response to stretching durations of ≥ 15 min was identified, this was based on only 7 studies with a range of 3 × 5 min to one hour of stretching, with the highest effects originating from one research group [19,20,21, 23,24,25,26, 76]. Thus, further studies are requested to confirm or disconfirm the results. Furthermore, all long-lasting stretch interventions (more than one hour) were performed with high stretching frequency and intervention periods (≥ 6 weeks), increases in maximal strength and muscle volume cannot be clearly ascribed to one of these parameters. Further studies should hence examine long-lasting stretch interventions of < 6 weeks and/or ≤ 5 sessions per week. Moreover, the role of stretch intensity merits further investigation. Reporting stretch intensity using individual pain perception seems of questionable validity [120]. However, it is well known from strength training that training intensity seems to be of crucial importance for adaptations, especially with regard to maximum strength increases [121]. Considering the importance of titin unfolding, which is assumed to occur exclusively in maximally stretched sarcomeres, reaching high degrees of stretch could be hypothesized to be of paramount importance [109, 122].
Despite some plausible theories [83], the underlying mechanisms remain speculative. While many physiological parameters were assessed in animals, no studies examined signaling pathways and possible alterations of protein synthesis in humans. Furthermore, research has almost exclusively focused on skeletal muscle. Interestingly, it has been shown that the connective tissue can exert significant force transmission effects [123]. Therefore, it may be prudent for future trials to consider multiple tissues.
Some increases in the examined parameters were surprisingly high in studies included in our review. Nelson et al. [60] reported an improvement in maximal strength of 29% (d = 1.48) in the stretched leg and a gain of about 11% (d = 0.46) in the contralateral control leg following 4 × 30 s stretching three times per week for ten weeks. Mizuno [55] found increases of 24% using static stretching three times per week for eight weeks, while Panidi et al. [69] detected hypertrophy effects of up to 23%. When these short duration stretching results are compared to those from strength training [124], the listed stretch-induced adaptations seem unreasonably high, even though participants are partially classified untrained to recreationally active. Against this background, it will be of interest to further identify moderator variables determining strong and weak stretch responders.
Lastly, testing for significant differences of mean effects to provide a valuable statement of subgroup differences was performed using the Welsh test. This testing procedure must be considered a supplementation of the main statistics and must be interpreted with caution, as no specific pooling for dependent outcomes was possible. If one study provided multiple outcomes, effect size means were calculated, meaning each study corresponded to one outcome, which reduced this limitation.
Conclusions
The present systematic review provides low- to moderate-certainty evidence that chronic static stretching increases maximum strength and muscle size. While the overall effects are small if existent, comparatively high effort seems necessary with longer stretching- and intervention periods (≥ 15 min, ≥ 6 weeks) and greater frequencies (≥ 5x/week) seem particularly effective. The exact physiological mechanisms causing potential effects remain a matter of debate. Nevertheless, even though less effective compared to resistance training, high volume stretching might provide a valuable alternative under special circumstances, e.g., if traditional resistance training is contraindicated.
Data Availability
Data can be provided on reasonable request. Supplemental materal associated with this article can be found in the online version.
Abbreviations
- CI:
-
confidence interval
- ES:
-
effect size
- M:
-
mean
- SD:
-
standard deviation
- SMD:
-
standardized mean differences
References
Konrad A, Alizadeh S, Daneshjoo A, Hadjizadeh AS, Graham S, Zahiri A et al. Chronic effects of stretching on range of motion with consideration of potential moderating variables: a systematic review with meta-analysis. J Sport Health Sci. 2023.
Medeiros DM, Martini TF. Chronic effect of different types of stretching on Ankle Dorsiflexion Range of Motion: systematic review and Meta-analysis. Foot(Edinb). 2018;34:28–35.
Malliaropoulos N, Papalexandris S, Papalada A, Papacostas E. The role of stretching in Rehabilitation of Hamstring injuries: 80 athletes Follow-Up. Med Sci Sports Exerc. 2004;36:756–9.
Tunwattanapong P, Kongkasuwan R, Kupniratsaikul V. The effectiveness of a Neck and Shoulder stretching Exercise Program among Office Workers with Neck Pain: a Randomized Controlled Trial. Clin Rehabil. 2016;30:64–72.
Shellock FG, Prentice WE. Warming-up and stretching for Improved Physical Performance and Prevention of sports-related injuries. Sports med. 1985;2:267–78.
Gremion G. Is stretching for sports Performance still useful? A review of the literature. Rev Med Suisse. 2005;1:1830–4.
Williford HN, East JB, Smith FH, Burry LA. Evaluation of warm-up for improvement in flexibility. Am J Sports Med. 1986;14:316–9.
Ebadi LA, Çetin E. Duration dependent effect of static stretching on quadriceps and hamstring muscle force. Sports. 2018;6.
Kay AD, Blazevich AJ. Effect of acute static stretch on maximal muscle performance: a systematic review. Med Sci Sports Exerc. 2012;44:154–64.
Simic L, Sarabon N, Markovic G. Does pre-exercise static stretching inhibit maximal muscular performance? A meta-analytical review. Scand J Med Sci Sports. 2013;23:131–48.
Medeiros DM, Lima CS. Influence of chronic stretching on muscle performance: systematic review. Hum Mov Sci. 2017;54:220–9.
Shrier I. Does stretching improve performance? A systematic and critical review of the literature. Clin J Sport Med. 2004;14:267–73.
Warneke K, Freund PA, Schiemann S. Long-lasting stretching induced muscle hypertrophy - a Meta-analysis of Animal studies. J Sci Sport Exerc. 2022.
Frankeny JR, Holly GR, Ashmore CR. Effects of graded duration of Stretch on normal and dystrophic skeletal muscle. Muscle Nerve. 1983;6:269–77.
Nunes JP, Schoenfeld BJ, Nakamura M, Ribeiro AS, Cunha PM, Cyrino ES. Does stretch training induce muscle hypertrophy in humans? A review of the literature. Clin Physiol Funct Imaging. 2020;40:148–56.
Panidi I, Donti O, Konrad A, Petros CD, Terzis G, Mouratidis A et al. Muscle architecture adaptations to static stretching training: a systematic review with meta-analysis. Sports Med Open. 2023;9.
Thomas E, Ficarra S, Nunes JP, Paoli A, Bellafiore M, Palma A, et al. Does stretching training influence muscular strength? A systematic review with Meta-analysis and Meta-regression. J Strength Cond Res. 2023;37:1145–56.
Arntz F, Markov A, Behm DG, Behrens M, Negra Y, Nakamura M, et al. Chronic effects of Static stretching exercises on muscle strength and power in Healthy Individuals across the Lifespan: a systematic review with multi-level Meta-analysis. Sports Med. 2023;53:723–45.
Warneke K, Keiner M, Hillebrecht M, Schiemann S. Influence of one hour versus two hours of Daily Static stretching for six weeks using a calf-muscle-stretching orthosis on maximal strength. Int J Environ Res Public Health. 2022;19.
Wohlann T, Warneke K, Kalder V, Behm DG, Schmidt T, Schiemann S. Influence of 8-weeks of supervised static stretching or resistance training of pectoral major muscles on maximal strength, muscle thickness and range of motion. Eur J Appl Physiol. 2024.
Wohlann T, Warneke K, Hillebrecht M, Petersmann A, Ferrauti A, Schiemann S. Effects of daily static stretch training over 6 weeks on maximal strength, muscle thickness, contraction properties and flexibility. Front Sports Act Living. 2023;5.
Warneke K, Hillebrecht M, Claassen-Helmers E, Wohlann T, Keiner M, Behm DG. Effects of a home-based stretching program on Bench Press Maximum Strength and Shoulder Flexibility. J Sports Sci Med. 2023;597–604.
Warneke K, Wirth K, Keiner M, Lohmann LH, Hillebrecht M, Brinkmann A, et al. Comparison of the effects of long-lasting static stretching and hypertrophy training on maximal strength, muscle thickness and flexibility in the plantar flexors. Eur J Appl Physiol. 2023;123:1773–87.
Warneke K, Keiner M, Wohlann T, Lohmann LH, Schmitt T, Hillebrecht M, et al. Influence of long-lasting static stretching intervention on functional and morphological parameters in the plantar flexors: a randomized controlled trial. J Strength Cond Res. 2023;37(10):1993-2001. https://doi.org/10.1519/JSC.0000000000004513. Epub 2023 Jun 5. PMID: 37318350.
Warneke K, Konrad A, Keiner M, Zech A, Nakamura M, Hillebrecht M, et al. Using Daily stretching to Counteract Performance decreases as a result of reduced physical Activity—A controlled trial. Int J Environ Res Public Health. 2022;19:15571.
Warneke K, Brinkmann A, Hillebrecht M, Schiemann S. Influence of long-lasting Static stretching on maximal strength, muscle thickness and flexibility. Front Physiol. 2022;13.
Horsley T, Dingwall O, Sampson M. Checking reference lists to find additional studies for systematic reviews. Cochrane Database Syst Rev. 2011;2011.
de Morton NA. The PEDro Scale is a valid measure of the Methodological Quality of clinical trials: a demographic study. Aust J Physiother. 2009;55:129–33.
Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83:713–21.
Van Duijnhoven HJR, Heeren A, Peters MAM, Veerbeek JM, Kwakkel G, Geurts ACH, et al. Effects of Exercise Therapy on Balance Capacity in Chronic Stroke: systematic review and Meta-analysis. Stroke. 2016;47:2603–10.
Stojanović E, Ristić V, McMaster DT, Milanović Z. Effect of Plyometric Training on Vertical Jump performance in female athletes: a systematic review and Meta-analysis. Sports Med. 2017;47:975–86.
Mavridis D, Salanti G. Exploring and accounting for publication bias in mental health: a brief overview of methods. Evid Based Ment Health. 2014;17:11–5.
Fernández-Castilla B, Declercq L, Jamshidi L, Beretvas SN, Onghena P, van den Noortgate W. Visual representations of meta-analyses of multiple outcomes: extensions to forest plots, funnel plots, and caterpillar plots. Methodology. 2020;16:299–315.
Pustejovsky J. [R-meta] egger’s test for funnel plot symmetry of a ’robu()’model. https://stat.ethz.ch/pipermail/r-sig-meta-analysis/2019-November/001876.html. 2019.
Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004;328:1490.
Fisher Z, Tipton E, Robumeta. An R-package for robust variance estimation in meta analysis. arXiv:1503.02220. 2015.
Faraone SV. Interpreting estimates of treatment effects: implications for managed care. P T. 2008;33:700–3.
Abdel-aziem AA, Mohammad WS. Plantar-flexor static stretch training effect on eccentric and concentric peak torque – a comparative study of trained versus untrained subjects. J Hum Kinet. 2012;34:49–58.
Akagi R, Takahashi H. Effect of a 5-week static stretching program on hardness of the gastrocnemius muscle. Scand J Med Sci Sports. 2014;24:950–7.
Barbosa GM, Trajano GS, Dantas GAF, Silva BR, Vieira WHB. Chronic effects of Static and Dynamic stretching on Hamstrings eccentric strength and functional performance: a Randomized Controlled Trial. J Strength Cond Res. 2020;34:2031–9.
Brusco CM, Blazevich AJ, Pinto RS. The effects of 6 weeks of constant-angle muscle stretching training on flexibility and muscle function in men with limited hamstrings’ flexibility. Eur J Appl Physiol [Internet]. 2019;119:1691–700. https://doi.org/10.1007/s00421-019-04159-w.
Caldwell SL, Bilodeau RLS, Cox MJ, Behm DG. Cross education training effects are evident with twice daily, self-administered band stretch training. J Sports Sci Med. 2019;18:544–51.
Chen CH, Nosaka K, Chen HL, Lin MJ, Tseng KW, Chen TC. Effects of flexibility training on eccentric exercise-induced muscle damage. Med Sci Sports Exerc. 2011;43:491–500.
Cini A, de Vasconcelos GS, Soligo MC, Felappi C, Rodrigues R, Aurélio Vaz M, et al. Comparison between 4 weeks passive static stretching and proprioceptive neuromuscular facilitation programmes on neuromuscular properties of hamstring muscles: a randomised clinical trial. Int J Ther Rehabil. 2020;27:1–11.
Ikeda N, Ryushi T. Effects of 6-Week Static stretching of knee extensors on flexibility, muscle strength, Jump Performance, and muscle endurance. J Strength Cond Res. 2021;35:715–23.
Kokkonen J, Nelson AG, Eldredge C, Winchester JB. Chronic static stretching improves exercise performance. Med Sci Sports Exerc. 2007;39:1825–31.
Konrad A, Tilp M. Increased range of motion after static stretching is not due to changes in muscle and tendon structures. Clin Biomech Elsevier Ltd. 2014;29:636–42.
Kubo K, Kanehisa H, Fukunaga T. Effect of stretching training on the viscoelastic properties of human tendon structures in vivo. J Appl Physiol. 2002;92:595–601.
LaRoche DP, Lussier MV, Roy SJ. Chronic stretching and Voluntary muscle force. J Strength Cond Res. 2008;22:589–96.
Leslie AW, Lanovaz JL, Andrushko JW, Farthing JP. Flexibility training and the repeated-bout effect: priming interventions prior to eccentric training of the knee flexors. Appl Physiol Nutr Metab. 2017;42:1044–53.
e Lima KMM, Carneiro SP, de Alves S, Peixinho D, de Oliveira CC. Assessment of muscle Architecture of the biceps femoris and Vastus Lateralis by Ultrasound after a chronic stretching program. Clin J Sport Med. 2015;25:55–60.
Longo S, Cè E, Valentina Bisconti A, Rampichini S, Doria C, Borrelli M, et al. The effects of 12 weeks of static stretch training on the functional, mechanical, and architectural characteristics of the triceps surae muscle-tendon complex. Eur J Appl Physil. 2021;121:1743–58.
Marshall PWM, Cashman A, Cheema BS. A Randomized Controlled Trial for the Effect of Passive stretching on measures of Hamtring Extensibility, Passive Stiffness, Strength and Stretch Tolerance. J Sci Med Sport. 2011;14:535–40.
Minshull C, Eston R, Bailey A, Rees D, Gleeson N. The differential effects of PNF versus passive stretch conditioning on neuromuscular performance. Eur J Sport Sci. 2014;14:233–41.
Mizuno T. Combined effects of Static stretching and Electrical Stimulation on Joint Range of Motion and muscle strength. J Strength Cond Res. 2019;33:2694–703.
Morton SK, Whitehead JR, Brinkert RH, Caine DJ. Resistance training vs. static stretching: effects on flexibility and strength. J Strength Cond Res. 2011;25:3391–8.
Moltubakk MM, Villars FO, Magulas MM, Magnusson SP, Seynnes OR, Bojsen-Møller J. Altered triceps Surae muscle-Tendon Unit properties after 6 months of Static stretching. Med Sci Sports Exerc. 2021;53:1975–86.
Nakamura M, Yoshida R, Sato S, Yahata K, Murakami Y, Kasahara K et al. Comparison between high- and Low-Intensity Static Stretching Training Program on active and Passive properties of Plantar Flexors. Front Physiol. 2021;12.
Nakao S, Ikezoe T, Nakamura M, Umegaki H, Fujita K, Umehara J, et al. Chronic effects of a Static stretching Program on Hamstring Strength. J Strength Cond Res. 2019;35:1924–9.
Nelson AG, Kokkonen J, Winchester JB, Kalani W, Peterson K, Kenly MS, et al. A 10-Week stretching program increases strength in the contralateral muscle. J Cond Res. 2012;26:832–6.
Nóbrega ACL, Paula KC, Carvalho ACG. Interaction between Resistance Training and Flexibility Training in healthy young adults. J Strength Conditioning Res. 2005;19:842.
Reiner M, Gabriel A, Sommer D, Bernsteiner D, Tilp M, Konrad A. Effects of a high-7-Week Pectoralis muscle stretching training on muscle function and muscle stiffness. Sports Med Open. 2023;9:40.
Simpson CL, Kim BDH, Bourcet MR, Jones GR, Jakobi JM. Stretch training induces unequal adaptation in muscle fascicles and thickness in medial and lateral gastrocnemii. Scand J Med Sci Sports. 2017;27:1597–604.
Wilson SJ, Christensen B, Gange K, Todden C, Hatterman-Valenti H, Albrecht JM. Chronic stretching during 2 weeks of immobilization decreases loss of girth, peak torque, and dorsiflexion range of motion. J Sport Rehabil. 2019;28:67–71.
Yahata K, Konrad A, Sato S, Kiyono R, Yoshida R, Fukaya T, et al. Effects of a high-volume static stretching programme on plantar-flexor muscle strength and architecture. Eur J Appl Physiol. 2021;121:1159–66.
Andrade RJ, Freitas SR, Hug F, Le Sant G, Lacourpaille L, Gross R, et al. Chronic effects of muscle and nerve-directed stretching on tissue mechanics. J Appl Physiol. 2020;129:1011–23.
Freitas SR, Mil-Homens P. Effect of 8-week high-intensity stretching training on biceps femoris architecture. J Strength Cond Res. 2015;29:1737–40.
Kay AD, Rubley B, Talbot C, Mina M, Baross AW, Blazevich AJ. Stretch imposed on active muscle elicits positive adaptations in strain risk factors and exercise-induced muscle damage. Scand J Med Sci Sports. 2018;28:2299–309.
Panidi I, Bogdanis GC, Terzis G, Donti A, Konrad A, Gaspari V et al. Muscle architectural and functional adaptations following 12-Weeks of stretching in adolescent female athletes. Front Physiol. 2021;12.
Peixinho CC, Silva GA, Brandão MCA, Menegaldo LL, de Oliveira LF. Effect of a 10-Week stretching program of the triceps Surae muscle Architecture and Tendon Mechanical properties. J Sci Sport Exerc. 2021;3:107–14.
Sekir U, Arslan G, Ilhan O, Akova B. Effects of Static and Dynamic stretching on muscle Architecture. Turkish J Sports Med. 2019;54:158–68.
Cashin AG, McAuley JH. Clinimetrics: Physiotherapy evidence database (PEDro) scale. J Physiother. 2020;66:59.
Warneke K, Freund PA, Schiemann S. Long-lasting stretching induces muscle hypertrophy: a Meta-analysis of Animal studies. J Sci Sport Exerc. 2022.
Kelley G. Mechanical overload and skeletal muscle Fiber hyperplasia: a Meta-analysis. J Appl Physiol. 1996;81:1584–8.
Warneke K, Zech A, Wagner CM, Konrad A, Nakamura M, Keiner M, et al. Sex diffeences in stretch-induced hypertrophy, maximal strength and flexibility gains. Front Physiol. 2022;13:1078301.
Warneke K, Lohmann LH, Keiner M, Wagner C, Schmidt T, Wirth K, et al. Using Long-Duration Static Stretch Training to counteract strength and flexibility deficits in moderately trained participants. Int J Environ Res Public Health. 2022;1:15.
Bates GP. The relationship between duration of stimulus per day and the extend of hypertrophy of slow-tonic skeletal muscle in the fowles, Gallus gallus. Comp Biochem Physiol. 1993;106A:755–8.
Antonio J, Gonyea WJ, Progressive WJG. Progressive stretch overload of skeletal muscle results in hypertrophy before hyperplasia. J Appl Physiol. 1993;75:1263–71.
Sayegh JF, Lajtha A. In vivo rates of protein synthesis in brain, muscle, and liver of five vertebrate species. Neurochem Res. 1989;11:1165–8.
Garibotto G, Tessari P, Robaudo C, Zanetti M, Saffioti S, Vettore M, et al. Protein turnover in the kidney and the whole body in humans. Min Electrolyte Metab. 1997;23:185–8.
Tessari P, Garibotto G, Inchiostro S, Robaudo C, Saffioti S, Vettore M, et al. Kidney, splanchnic, and leg protein turnover in humans. Inside from leucine and phenylalanine kinetics. J Clin Invest. 1996;98:1481–92.
Martins-Costa HC, Lacerda LT, Diniz RCR, Lima FV, Andrade AGP, Peixoto GH, et al. Equalization of training protocols by Time under Tension determines the magnitude of changes in strength and muscular hypertrophy. J Strength Cond Res. 2022;36:1770–80.
Warneke K, Lohmann LH, Lima CD, Hollander K, Konrad A, Zech A et al. Physiology of stretch-mediated hypertrophy and strength increases: a narrative review. Sports Med. 2023.
Wackerhage H, Schoenfeld BJ, Hamilton DL, Lehti M, Hulmi JJ. Stimuli and sensors that initiate muscle hypertrophy following resistance exercise. J Appl Physiol. 2019;126:30–43.
Schoenfeld BJ, Wackerhage H, De Souza E. Inter-set stretch: a potential time-efficient strategy for enhancing skeletal muscle adaptations. Front Sports Act Living. 2022;4.
Devol DL, Novakofski J, Fernando R, Bechtel PJ. Varying amounts of Stretch stimulus regulate Stretch-Induced muscle hypertrophy in the chicken. Biochem Physiol. 1991;100A:55–61.
Ashmore CR. Stretch-induced growth in chicken wing muscles: effects on hereditary muscular dystrophy. Am J Physiol. 1982;242:C178–83.
Hughes L, Rosenblatt B, Haddad F, Gissane C, McCarthy D, Clarke T, et al. Comparing the effectiveness of blood Flow Restriction and Traditional Heavy load resistance training in the Post-surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction patients: a UK National Health Service Randomised Controlled Trial. Sports Med. 2019;49:1787–805.
Krzysztofik M, Wilk M, Wojdała G, Gołaś A. Maximizing muscle hypertrophy: A systematic review of advanced resistance training techniques and methods. Int J Environ Res Public Health. MDPI AG; 2019.
Loenneke JP, Wilson JM, Marín PJ, Zourdos MC, Bemben MG. Low intensity blood flow restriction training: a meta-analysis. Eur J Appl Physiol. 2012;112:1849–59.
Horiuchi M, Okita K. Blood Flow Restricted Exercise and vascular function. Int J Vasc Med. 2012;2012:1–17.
Fry CS, Glynn EL, Drummond MJ, Timmerman KL, Fujita S, Abe T, et al. Blood flow restriction exercise stimulates mTORC1 signaling and muscle protein synthesis in older men. J Appl Physiol. 2010;108:1199–209.
Jessee MB, Buckner SL, Mouser JG, Mattocks KT, Dankel SJ, Abe T, et al. Muscle adaptations to High-Load Training and very low-load training with and without blood Flow Restriction. Front Physiol. 2018;9:1–10.
Hotta K, Behnke BJ, Arjmandi B, Ghosh P, Chen B, Brooks R, et al. Daily muscle stretching enhances blood flow, endothelial function, capillarity, vascular volume and connectivity in aged skeletal muscle. J Physiol. 2018;596:1903–17.
Suzuki YM, Takeda S. Mechanobiology in skeletal muscle. Mech Biology. 2011;51–62.
Kremer B. Dehnungsinterventionen im Spannungsfeld historischer Entwicklung, ritualisierter Anwendung, Meisterlehre und Wissenschaft; Eine Bestandsanalyse. Karlsruher Sportwissenschaftliche Beiträge. 2017. pp. 188–92.
Mousavizadeh R, Hojabrpour P, Eltit F, McDonald PC, Dedhar S, McCormack RG, et al. β1 integrin, ILK and mTOR regulate collagen synthesis in mechanically loaded tendon cells. Sci Rep. 2020;10:1–12.
Bradley JMB, Kelley MJ, Rose A, Acott TS. Signaling pathways used in trabecular matrix metalloproteinase response to Mechanical Stretch. Investig Ophthalmol Vis Sci. 2003;44:5174–81.
Aoki MS, Miyabara EH, Soares AG, Saito ET, Moriscot AS. mTOR pathway inhibition attenuates skeletal muscle growth induced by stretching. Cell Tissue Res. 2006;324:149–56.
Czerwinski SM, Martin JM, Bechtel PJ. Modulation of IGF mRNA abundance during stretch-induced skeletal muscle hypertrophy and regression. J Appl Physiol. 1994;76:2026–30.
Goldspink G. Changes in muscle mass and phenotype and the expression of autocrine and systemic growth factors by muscle in response to stretch and overload. J Anat. 1999;194:323–34.
Sparrow MP. Regression of Skeletal Muscle of Chicken Wing after Stretch-Induced Hypertrophy. Am J Physiol. 1982;242:C333–8.
Laurent GJ, Sparrow MP, Millward DJ. Turnover of muscle protein in Fowl: changes in Rates of protein synthesis and breakdown during hypertrophy of the anterior and posterior latissimus dorsi muscles. Biochem J. 1978;176:407–14.
Aguilar-Agon KW, Capel AJ, Martin NRW, Player DJ, Lewis MP. Mechanical loading stimulates hypertrophy in tissue-engineered skeletal muscle: Molecular and phenotypic responses. J Cell Physiol. 2019;234:23547–58.
Boppart MD, Mahmassani ZS. Integrine signaling: linking mechanical stimulation to skeletal muscle hypertrophy. Am J Physiol Cell Physiol. 2019;317:C629–41.
Sasai N, Agata N, Inoue-Miyazu M, Kawakami K, Kobayashi K, Sokabe M, et al. Involvement of PI3K/Akt/TOR pathway in stretch-induced hypertrophy of myotubes. Muscle Nerve. 2010;41:100–6.
van der Pijl R, Strom J, Conijn S, Lindqvist J, Labeit S, Granzier H, et al. Titin-based mechanosensing modulates muscle hypertrophy. J Cachexia Sarcopenia Muscle. 2018;9:947–61.
van der Pijl RJ, Hudson B, Granzier-Nakajima T, Li F, Knottnerus AM, Smith J et al. Deleting Titin’s C-Terminal PEVK exons increases Passive Stiffness, alters splicing, and induces cross-sectional and longitudinal hypertrophy in skeletal muscle. Front Physiol. 2020;11.
Apostolopoulos N, Metsios GS, Flouris AD, Koutedakis Y, Wyon MA. The relevance of stretch intensity and position—a systematic review. Front Psych. 2015;6.
Fowles JR, MacDougall JD, Tarnopolsky MA, Sale DG, Roy BD, Yarascheski KE. The effects of acute passiv stretch on muscle protein synthesis in humans. Can J Appl Physiol. 2000;25:165–80.
Laurent GJ, Sparrow MP. Changes in RNA, DNA and protein content and the Rates of protein synthesis and degradation durting hypertrophy of the Anterior Latissimus Dorsi muscle of the adult fowl (Gallus Domesticus). Growth. 1977;41:249–62.
Del Vecchio A, Casolo A, Negro F, Scorcelletti M, Bazzucchi I, Enoka R, et al. The increase in muscle force after 4 weeks of strength training is mediated by adaptations in motor unit recruitment and rate coding. J Physiol. 2019;597:1873–87.
Kim EH, Hassan AS, Heckman CJ. Changes in motor unit discharge patterns following strength training. J Physiol. 2019;597:3509–10.
Holly RG, Barnett JG, Ashmore CR, Taylor RG, Molti PA. Stretch-induced growth in chicken wing muscles: a new model of stretch hypertrophy. Am J Physiol. 1980;238:C62–71.
Barnett JG, Holly RG, Ashmore CR. Stretch-induced growth in chicken wing muscles: biochemical and morphological characterization. Am J Physiol. 1980;239:C39–46.
Sola M, Christensen DL, Martin AW. Hypertrophy and Hyperplasia of Adult Chicken Anterior Latissimus Dorsi muscles following Stretch with and without Denervation 0. Exp Neurol. 1973;41:76–100.
Currier BS, Mcleod JC, Banfield L, Beyene J, Welton NJ, D’Souza AC, et al. Resistance training prescription for muscle strength and hypertrophy in healthy adults: a systematic review and bayesian network meta-analysis. Br J Sports Med. 2023;57:1211–20.
Behm DG, Granacher U, Warneke K, Aragão-Santos JC, Da Silva-Grigoletto ME, Konrad A. Minimalist training: is lower dosage or intensity resistance training effective to improve physical fitness? A narrative review. Sports Med. 2023.
Thomas E, Bellafiore M, Gentile A, Paoli A, Palma A, Bianco A. Cardiovascular responses to muscle stretching: a systematic review and Meta-analysis. Int J Sports Med. 2021.
Lim W, Park H. No significant correlation between the intensity of static stretching and subject’s perception of pain. J Phys Ther Sci. 2017;29:1856–9.
Schoenfeld BJ, Peterson MD, Ogborn D, Contreras B, Sonmez GT. Effects of Low- vs. high-load resistance training on muscle strength and hypertrophy in Well-trained men. J Strength Cond Res. 2015;29:2954–63.
Freundt JK, Linke WA. Titin as a force-generating muscle protein under regulatory control. J Appl Physiol. 2019;126:1474–82.
Wilke J, Debelle H, Tenberg S, Dilley A, Maganaris C. Ankle motion is Associated with Soft tissue displacement in the dorsal thigh: an in vivo investigation suggesting Myofascial Force Transmission across the knee Joint. Front Physiol. 2020;11.
Schoenfeld BJ, Grgic J, Ogborn D, Krieger JW. Strength and hypertrophy adaptations between Low- vs. high-load resistance training: a systematic review and Meta analysis. J Strength Cond Res. 2017;31:3508–23.
Acknowledgements
Not applicable.
Registration of the Study
The study was registered in the PROSPERO data base using the number CRD42023411225 and the title “Effects of Chronic Static Stretching on Maximal Strength and Muscle Hypertrophy: A Systematic Review with Meta-Analysis”.
Funding
The authors acknowledge the financial support by the University of Graz.
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
KoW wrote the first draft, contributed to the screening of studies, performed the meta-analytic procedure with the help of JW, and performed the graphical illustration with the help of LHL. LHL contributed to study screening, assisted in the writing and helped with the graphical illustration. JW supervised the project, included critical feedback and advised on statistical procedures. MK, KlW, SS and AK included their critical feedback and expertise in the fields to the manuscript. All authors contributed to the manuscript and discussed the final version.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Competing Interests
The authors declare that they have no competing interests. There were no sponsors included.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Warneke, K., Lohmann, L.H., Behm, D.G. et al. Effects of Chronic Static Stretching on Maximal Strength and Muscle Hypertrophy: A Systematic Review and Meta-Analysis with Meta-Regression. Sports Med - Open 10, 45 (2024). https://doi.org/10.1186/s40798-024-00706-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-024-00706-8