
Abstract
Background
Given the severe economic and performance implications of hamstring injuries, there are different attempts to identify their risk factors for subsequently developing injury prevention strategies to reduce the risk of these injuries. One of the strategies reported in the scientific literature is the application of interventions with eccentric exercises. To verify the effectiveness of these interventions, different eccentric strength measurements have been used with low-cost devices as alternatives to the widespread used isokinetic dynamometers and the technically limited handheld dynamometers. Therefore, the purpose of the present systematic review was to summarize the findings of the scientific literature related to the evaluation of eccentric strength of hamstring muscles with these new technologies.
Methods
Systematic searches through the PubMed, Scopus, and Web of Science databases, from inception up to April 2020, were conducted for peer reviewed articles written in English, reporting eccentric strength of hamstrings assessed by devices, different to isokinetic and handheld dynamometers, in athletes.
Results
Seventeen studies were finally included in the review with 4 different devices used and 18 parameters identified. The pooled sample consisted of 2893 participants (97% male and 3% female: 22 ± 4 years). The parameters most used were peak force (highest and average), peak torque (average and highest), and between-limb imbalance (left-to-right limb ratio). There is inconsistency regarding the association between eccentric hamstrings strength and both injury risk and athletic performance. There is no standardized definition or standardization of the calculation of the used parameters.
Conclusions
The current evidence is insufficient to recommend a practical guide for sports professionals to use these new technologies in their daily routine, due to the need for standardized definitions and calculations. Furthermore, more studies with female athletes are warranted. Despite these limitations, the eccentric strength of hamstring muscles assessed by different devices may be recommended for monitoring the neuromuscular status of athletes.
Similar content being viewed by others


Key Points
-
Eccentric hamstrings strength using 4 different devices was evaluated with 18 different parameters after 3-to-6 trials performed unilaterally or bilaterally. Peak force, peak torque, and between-limb imbalance were the most used parameters.
-
Eccentric strength hamstring assessed by different devices can be a useful tool for monitoring neuromuscular status of athletes in laboratory and field settings. The assessments should be performed bilaterally with the average of 6 trials.
-
There is a need of consensus for identifying the best procedures, definitions, and calculations for evaluation of the eccentric strength of hamstrings in different sport settings.
Background
Despite the constant evolution of applied sport training tools and technologies, including 24-h monitoring [1] and artificial intelligence [2], hamstring strain injuries are still the most common injuries in sports involving high-speed running activities [3]. A longitudinal analysis between 2001 and 2013 found that hamstring injuries had annually increased by 4% in professional soccer [4]. In addition to soccer [5], hamstring injuries are common in other team sports as American Football [6], Australian Rules Football [7], basketball [8], cricket [9], rugby [10], and in individual sports as track and field [11].
Eccentric exercises are one of the most popular strategies with strong evidence supporting their use for injury prevention [3]. Given the severe economic and performance implications of hamstring strain injuries, there are attempts to identify the main risk factors associated with these injuries and to develop efficient prevention strategies [3]. In this context, new alternative tools to isokinetic and handheld dynamometers [12, 13], with requirements of minimal equipment and easy-to-use in the field, have been developed to verify the effect of eccentric exercises on different eccentric strength measures [14, 15]. Previously, Tous-Fajardo et al. [14] tested an instrumented flywheel leg-curl machine that offered eccentric overload for hamstring development. Opar et al. [15] developed a novel field-testing device, the NordBord, for assessing hamstring eccentric strength, based on the commonly employed Nordic hamstring exercise. These devices have received an increasing interest from practitioners and researchers [16] and many other interesting field applications to reduce hamstring injuries are currently being published [15,16,17,18].
However, there is no evidence to support the decision-making process of practitioners for using these new devices. Therefore, the purpose of the present systematic review was to search, analyze, and summarize the current findings of the scientific literature related to the evaluation of eccentric strength of hamstring muscles with these new technologies.
Methods
We adopted the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19].
Sources and Study Selection Process
Three electronic databases (PubMed, Scopus and Web of Science) were systematically searched from inception up to April 2020. The command line (“eccentric strength” OR “Nordic exercise” OR “hamstring”) AND (“equipment” OR “device”) was used during the electronic searches. Titles and abstracts were reviewed and screened by the first author (JGC) for the potential eligible studies based on inclusion criteria. Two authors (CACF and NFNB) retrieved and independently assessed the full text of the potential eligible studies. If any doubt arose during this process, a fourth author (JCS) was involved for the final decision by consensus.
Eligibility Criteria
-
(1)
The study was written in English.
-
(2)
The study was published as original research in a peer-reviewed journal as a full text article.
-
(3)
Data were reported from team or individual sport athletes.
-
(4)
The participants were competitive athletes (defined as Olympic, international, professional, semi-professional, national, regional, youth academy or division I collegiate);
-
(5)
Eccentric knee flexors strength was assessed by devices different to isokinetic and handheld dynamometers.
Data Extraction
Three review authors (JGC, CACF, and NFNB) independently extracted information from the included full-text publications, such as authors, year, population information (mean age, sex ratio, sample size, sport, competitive level), study design, devices used to assess eccentric hamstrings strength, data collection procedures (number of repetitions, performed bilaterally or unilaterally), and the main findings of these studies about injury risk or sports performance. Discrepancies were resolved through discussion until consensus was reached. A narrative synthesis of data was performed.
Quality Assessment
The quality of all studies was evaluated by two authors (LGG and CRC) using evaluation criteria (Table 1) based on a study by Saw et al. [20]. Scores were allocated based on how well each criterion was met, assuming a maximum possible score of 8 (low risk of bias). Studies with a risk of bias score of 4 or less were considered poor and were subsequently excluded. Once the studies to be included had been defined, we performed an additional review, checking reference lists [21] to identify additional peer reviewed studies that met the inclusion criteria. One study which met inclusion criteria was also included during the peer review process following a reviewer suggestion.
Results
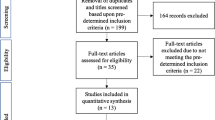
The initial search returned 1759 articles (see Fig. 1). After the removal of duplicates (n = 563), a total of 1196 studies were retained for full text screening. Following the eligibility assessment, 1180 studies were excluded as they did not meet the inclusion criteria. Finally, after considering one study suggested by one of the reviewers, 17 studies were included in this systematic review [14,15,16, 22,23,24,25,26,27,28,29,30,31,32,33,34,35].

Study selection PRISMA flow diagram
Characteristics of the Studies and Risk of Bias
The pooled sample size and age included 2893 participants with 22 ± 4 years, being composed mostly by male athletes (97%). The athletes were involved in only seven sports: soccer (70%), Australian Rules Football (12%), rugby (7%), alpine skiing (6%), cricket (1%), and track and field (sprinters) (1%). Three studies did not report the sport of the athletes (3%). All the studies included had a low risk of bias, with a score > 4 (see online supplementary Table 1). The average bias score for the studies was 7.6 (range 5–8).
There were 16 observational studies, with 9 cross-sectional studies [14, 16, 22, 24,25,26,27, 34, 35], 6 prospective cohort studies [23, 28,29,30,31,32] and one reliability and case-control study [15]. The follow-up period of these prospective cohort studies ranged between one preseason period [30] to four seasons [23]. An interventional cross-over study [33] was also included.
Main Findings
The summary of the 17 studies included in the systematic review is provided in Table 2. Four different devices were found to assess eccentric strength of hamstrings: an instrumented flywheel leg-curl machine (6%) [14], the NordBord (82%) [15, 16, 22,23,24, 26, 28,29,30,31,32,33,34,35], a custom-made device based on the prototype validated by Opar et al. [13] with two commercially-available load cells (6%) [25], and a custom-made device with load cells fixed in the dominant leg with a built-in potentiometer to measure sagittal knee angle (6%) [27].
The selected studies were related to hamstring (n = 10) and anterior cruciate ligament injuries risks (n = 1), previous experience effect (n = 1), device reliability (n = 1), body mass effect (n = 2), augmented feedback (n = 1), sprint performance (n = 1), variability and correlation with isokinetic strength testing (n = 1), and body positioning during the test (n = 1). In addition, 18 parameters related to eccentric hamstring strength were obtained from the devices using 3-to-6 unilateral or bilateral trials: peak force (average or highest, and absolute or relative), peak torque (average or highest, and absolute or relative), average force (N), average power (W), peak power (W), average velocity (m/s), peak velocity (m/s), and between-limb imbalance. The between-limb imbalance included 5 different equations: (1) left-right limb ratio, 2) stronger leg peak force − weaker leg peak force (× 100); (3) 1 − (dominant leg strength/non-dominant leg strength) × 100; (4) stronger limb minus the weaker limb, with the stronger limb being used as the reference value, i.e., 100%; and (5) (strongest limb − weakest limb)/(sum of both limbs)]. However, the same parameters were calculated in different ways in different studies (see details in Table 2).
Discussion
The purpose of this systematic review was to analyze the findings related to the evaluation of hamstrings eccentric strength with alternative devices. Thus, we described the instruments used to assess eccentric hamstring strength and the clinical outcomes related. There are four different devices used to evaluate eccentric knee flexors strength data. Eccentric hamstring strength using these devices was evaluated from 18 different parameters obtained in 3–6 trials. There is inconsistent evidence correlating eccentric knee flexor strength with an increased risk of sustaining hamstring strain injuries, as well as limited evidence associating eccentric knee flexors strength and sports performance.
The first study found in the literature reported that athletes using an instrumented flywheel leg-curl machine showed greater eccentric strength performances [14]. However, this finding may also suggest an influence of the learning effect [37, 38]. Therefore, a previous execution of the test procedures to reduce the intra-subject variability, which is called familiarization, is therefore necessary and constitutes an important factor to be considered in this context [39, 40]. Augmented feedback, with its effects well recognized in the scientific literature [41, 42], was tested in another study using a single session of real-time visual feedback during the Nordic hamstring testing. With this procedure, the mean peak force was increased [33]. Thus, researchers and practitioners should pay attention to the importance of familiarization sessions and whether augmented feedback is being used by athletes, to guarantee higher levels of reliability of the measures obtained with these devices.
The NordBord device [15, 16, 22,23,24, 26, 28,29,30,31,32,33,34,35] and another similar device [25] were the most common instruments used for assessing eccentric hamstring strength. These devices have been developed as low-cost alternatives to the widespread used isokinetic dynamometers [12] and the technically limited handheld dynamometers [13]. The NordBord device for bilateral assessment of Nordic hamstring exercise showed a high to moderate test-retest reliability, i.e., intraclass correlation coefficient (ICC) = 0.83–0.90 and standard error of measurement (SEM) = 6–9%. However, a lower reliability was found during unilateral testing (ICC = 0.56–0.73 and SEM = 10–11%) [15]. Also, for between-limb imbalance, it was found that only the ratios based on the peak force averaged across 6 trials had acceptable reliability values (ICC = 0.85; 95% CI 0.71–0.93; SEM = 5%, 95% CI 4–6%) [15]. Despite the good reliability of some NordBord measures, a poor correlation was found between peak isokinetic hamstring eccentric torque (60°/s) and forces measured with the NordBord device (r = 0.35; r2 = 12%) [23]. Besides, there was no correlation between bilateral imbalances in isokinetic eccentric contraction strength (60°/s) and eccentric strength measured during the Nordic hamstring exercise [23], despite the former being considered the gold standard [43] and its use to determine quadriceps-to-hamstring ratios aiming to identify risk profiles [44]. The authors also reported a substantial variability for isokinetic measures between different seasons with the SEM ranging 15–19% [23]. Additionally, during the Nordic hamstring exercise with the hip in neutral position, there was a higher semitendinosus activity in the early phase of the movement and a higher biceps femoral long head activity during the final phase. This behavior was changed with hip flexed at 90°, where a higher semitendinosus activity was found in the final phase of the movement [27]. During the Nordic hamstring exercise, the athlete is required to resist via forceful eccentric knee flexor contractions, thus increasing the external torque around the knee joint as the athlete progresses toward the ground. In contrast, isokinetic testing imposes maximal effort throughout the full range of motion [28]. The poor correlation of imbalance measures between both tests may be justified by the fact that the Nordic hamstring exercise only measures the imbalance when both legs are tested at the same time [45]. In contrast, during isokinetic testing, each leg is evaluated separately. Therefore, bilateral testing should be preferred when evaluating the Nordic hamstring exercise with these devices.
It has been previously suggested that athletes with a history of hamstring injuries present knee flexor weakness in their injured limb when compared to their uninjured limb and to uninjured athletes [15, 25]. In the same manner, players with hamstring injury lasting more than 3 weeks, exhibited a ~ 9% lower knee flexor eccentric strength than uninjured players during the preseason [24]. Contrary to this, it has been also observed no difference in eccentric hamstring strength between previously injured and uninjured athletes [26]. Furthermore, previously hamstring injured and uninjured athletes have displayed similar between-limb asymmetries on eccentric knee flexors strength, with half of the previously injured athletes and 37% of the uninjured athletes presenting between-limb asymmetries above ~ 10% [25]. In this regard, players with previous lower extremity injuries had shown similar eccentric strength imbalances in comparison to non-injured players, with athletes’ body masses being positively correlated to bilateral eccentric strength imbalances [34]. This conflicting evidence was also found in prospective cohort studies. Previously, some authors have suggested that levels of eccentric knee flexors strength below 256 N at the start of pre-season, 279 N at the end of pre-season in Australian Rules footballers [28], and 337 N for the whole season in soccer players [31] may increase the risk of a hamstring strain injury by ~ 4.4 times [31]. Furthermore, higher levels of between-limb imbalance (> 15%) were also associated with an increased risk of hamstring strain injury [29]. Conversely, others did not find any association between eccentric hamstring strength or between-limb imbalances and an increased risk of hamstring strain injuries [28, 29, 31, 32]. However, it is noteworthy that these previous studies evaluated players from different sports. Therefore, it is possible that the differences between physical characteristics of these athletes [46, 47] and the specific demands of each sport could explain the inconsistencies observed in these previous studies [29, 48, 49]. Moreover, these previous studies looked for this association in a linear fashion while isolating specific parameters. Since hamstring injuries have a multifactorial nature, it may be suggested for future studies to better test this association through the combination of different risk factors, including sports performance, running demands, and hamstrings strength [50].
Another reason for the inconsistencies observed in previous literature could be the different characteristics between hamstring demands during running activities and the Nordic hamstring exercise. Although the exact mechanisms for hamstring injuries are not fully understood [50, 51], it is suggested to occur mainly during the late swing phase or the early stance phase, in which hamstrings are highly activated at longer lengths [51,52,53,54,55]. Hamstrings are required to contract eccentrically during the terminal swing phase of a running gait cycle to decelerate the forward swinging shank and to oppose the external hip-flexor and knee extensor torques developed [56,57,58]. In addition, they are required to contract concentrically during early stance to absorb the high ground reaction forces [59]. Further, hamstrings demands increase with higher running speeds, such as sprinting at maximal or close to maximal speeds [54, 59, 60], which is the situation at which the hamstrings strain injuries frequently occur [53, 61]. However, eccentric hamstring strength assessment with these devices occurs at the slowest possible knee angular velocity [15, 31], with trials performed at very low angular velocities of − 30°s−1 [62]. Furthermore, it has been also shown that when running at ~ 75% of the maximal running speed, there was approximately a 15% higher hamstrings electromyographic (EMG) activity than during a maximum voluntary isometric contraction [63] and higher EMG amplitudes when compared to the Nordic hamstring exercise [63, 64]. Therefore, the strength measures assessed during the Nordic hamstring exercise do not elicit the same demands as during running activities. In addition, some evidence have pointed out that low levels of eccentric strength may reduce the hamstring ability to perform well during the gait cycle, potentially increasing the hamstring strain injury risk [52, 65]. While we are not questioning the well-established effects of the Nordic hamstring exercise on reducing hamstring strain injury risk [66,67,68,69], it is important to consider that hamstring strain injuries are multifactorial and complex [51, 70,71,72], and therefore, caution should be taken by practitioners when using some isolated measurements, such as peak forces or between-limb imbalances during this test in an attempt to estimate a hamstring strain injury risk.
The horizontal component of the ground reaction forces is suggested to be the key mechanical feature of sprint acceleration performance [73,74,75,76,77], with subjects who are able to produce the greatest amounts of horizontal force in sprint running presenting higher eccentric hamstring peak torque capability and also being able to activate to a greater extent their hamstring muscles before initial ground contact [75]. Of note, this parameter can be monitored with other new technologies not included in the current review (i.e., mobile app and sports radar system) [77, 78]. In addition, the contributions of horizontal and vertical components of ground reaction forces on sprint performance have been described in the literature to be 17– 61% and 17–23%, respectively [73, 76, 79, 80]. In this regard, limited evidence indicated that eccentric hamstring strength measured with the NordBord device was largely correlated to 20-m sprint performance (r = − 0.52; r2 = 27%, p < 0.05) [22]. Therefore, all this information suggests that higher levels of eccentric hamstring strength could be an important component of an athlete’s neuromuscular capabilities to achieve higher speeds and thus a better sprint performance [22, 75]. Notably, the 20-m sprint time and the eccentric hamstring strength measured in the Nordic hamstring exercise share a common variance of 27% in youth soccer players [22]. Thus, sports practitioners interested in monitoring the neuromuscular status during the training process could use these tools to evaluate the eccentric strength of hamstring muscles in the same manner as vertical jump evaluations. This suggestion is based on the association levels observed between sprint performances and vertical jump height in elite sprinters (r2 = 47 to 76%) [81], collegiate soccer players (r2 = 22 to 46%) [82], and elite young basketball players (r2 = 37%) [83]. Therefore, these devices may serve as an appealing option for neuromuscular status monitoring, as occurs with vertical jump performance evaluations [84].
Attention should be given to how the eccentric hamstring strength parameters evaluated by these devices were calculated in the articles included. In an instrumented flywheel leg-curl device, the parameters were calculated from 6 coupled concentric-eccentric actions [14]. During Nordic hamstring exercises, some studies adopted the peak force averaged from 3 [23, 24, 26, 28,29,30,31,32,33] or 6 [15] bilateral maximal repetitions in absolute values (N) [15, 23, 26, 28,29,30,31,32,33], while others reported these values normalized by body mass (N/kg) [24, 26, 28, 31, 32]. There were also reports on these values relative to moment of the season, expressed as the late preseason/early preseason ratio [30]. Some researchers used the highest peak force of 3 repetitions in absolute values (N) [16, 22, 23, 25, 26, 29, 32, 35] or normalized by body mass [22, 26, 29, 32], while others adopted the highest peak force of 6 repetitions in absolute terms (N) [15]. Some authors measured eccentric hamstring torque through the product of mean peak force data (N) [27, 31] or the highest peak force data (N) [22, 26] by the lever arm of shank length, with this measure reported in absolute terms (Nm) [22, 26, 27, 31] or normalized by body mass (Nm/kg) [22, 26, 31]. All these inconsistencies were also presented for between-limb imbalance measures, calculated as percentage differences of left/right limb force ratio for uninjured players and uninjured/injured limbs force ratio in the injured group [28, 29, 31]. In other studies, it was calculated as the left-right limb force ratio [32], converted to the percentage difference using log-transformed raw data followed by back transformation [15, 33], as the stronger leg peak force minus weaker leg [25, 34, 35], as the stronger limb being used as the reference value (i.e., 100%) [25], or by dividing torque or force of the right limb by the measures of left limb [26]. There was also one study that calculated Eq. 1 [24]:
and another that adopted Eq. 2 [22]:
All this variety makes it difficult to compare the different results observed in studies examining lower limbs imbalance with regard to hamstring strain injury or sports performance.
Lastly, although with a limited number of athletes for sex comparisons, male athletes were found to produce greater absolute force levels compared to female athletes, but the relative force (normalized to body mass) was similar between sexes [26]. This is important as eccentric hamstring strength assessed by these devices is suggested to be body mass dependent [16, 22]. Additionally, Nordic hamstring strength increases with the player’s age, and body size has been reported to be largely related to the increase in absolute Nordic hamstring strength [22]. Therefore, adopting absolute units (i.e., N and Nm) or simply dividing eccentric hamstring strength by body mass (i.e., N/Kg; Nm/kg) may not be optimal strategies. In this regard, future studies may use allometric scaling for solving this issue. An alternative method could be to apply a correction factor, as previously suggested [16] with the following Eq. (3):
Finally, it is worth noting that in the first studies found in the scientific literature, 6 repetitions were performed for the hamstring assessments [14, 15]. Among these studies, in a single reliability study, the authors reported that, when peak force was averaged across the 6 trials, the results were more reliable [15]. This finding agrees with previous studies that verified greater sensitivity for the averaged results than for the highest performance in trials for detecting trained related changes in countermovement jumps [84, 85]. Future studies should consider a standard method to assess eccentric knee flexors strength during the Nordic hamstring exercise, including 6 trials and body mass normalization. On the other hand, from a clinical perspective, these measures should be used over the season thus allowing the management of training loads and also as criteria before returning to play. This information could guide sports professionals during the training and rehabilitation processes to decrease injury and re-injury risks.
Conclusions
There is a growing scientific evidence suggesting the use of new devices to evaluate the eccentric hamstring strength of athletes. These devices have been developed as low-cost alternatives to the widespread used isokinetic dynamometers and the technically limited handheld dynamometers. There is inconsistent evidence correlating eccentric knee flexor strength with an increased injury risk of hamstrings, and very limited evidence about its relationship with athletic performance. The parameters most widely used during these evaluations were peak force (average or highest), peak torque (average or highest), and between-limb imbalance (left-right limb ratio). Due to the variety of strength measurements observed in the current literature, there is an urgent need for better defining the procedures and the parameters to be used with these devices. The eccentric strength of hamstrings assessed by these devices may be useful as a tool for monitoring the neuromuscular status of athletes during a whole season.
Availability of Data and Materials
After publication, all data necessary to understand and assess the conclusions of the manuscript are available to any reader of Sports Medicine-Open.
Abbreviations
- BM:
-
Body mass
- EMG:
-
Electromyography
- F:
-
Female
- HSI:
-
Hamstring strain injury
- ICC:
-
Intraclass correlation coefficient
- M:
-
Male
- n :
-
Sample size
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- r 2 :
-
Coefficient of determination
- SEM:
-
Standard error of measurement
- y:
-
Years old
References
Duking P, Achtzehn S, Holmberg H-CC, Sperlich B, Dueking P, Achtzehn S, et al. Integrated framework of load monitoring by a combination of smartphone applications, wearables and point-of-care testing provides feedback that allows individual responsive adjustments to activities of daily living. Sensors. 2018;18:1–11.
Claudino JG, de Oliveira Capanema D, de Souza TV, Serrão JC, Machado Pereira AC, Nassis GP. Current approaches to the use of artificial intelligence for injury risk assessment and performance prediction in team sports: a systematic review. Sport Med Open. 2019;5(1):28.
Shield AJ, Bourne MN. Hamstring injury prevention practices in elite sport: evidence for eccentric strength vs. lumbo-pelvic training. Sport Med. 2018;48:513–24.
Ekstrand J, Waldén M, Hägglund M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: a 13-year longitudinal analysis of the UEFA Elite Club injury study. Br J Sports Med. 2016;50:731–7.
van Dyk N, Farooq A, Bahr R, Witvrouw E. Hamstring and ankle flexibility deficits are weak risk factors for hamstring injury in professional soccer players: a prospective cohort study of 438 players including 78 injuries. Am J Sports Med. 2018;46:2203–10.
Werner BC, Belkin NS, Kennelly S, Weiss L, Barnes RP, Potter HG, et al. Acute gastrocnemius-soleus complex injuries in national football league athletes. Orthop J Sport Med. 2017;5:1–6.
Watsford ML, Murphy AJ, McLachlan KA, Bryant AL, Cameron ML, Crossley KM, et al. A prospective study of the relationship between lower body stiffness and hamstring injury in professional Australian rules footballers. Am J Sports Med. 2010;38:2058–64.
Drakos MC, Domb B, Starkey C, Callahan L, Allen AA. Injury in the National Basketball Association: a 17-year overview. Sports Health. 2010;2:284–90.
Orchard JW, Kountouris A, Sims K. Risk factors for hamstring injuries in Australian male professional cricket players. J Sport Health Sci. 2017;6:271–4.
Whitehouse T, Orr R, Fitzgerald E, Harries S, McLellan CP. The epidemiology of injuries in Australian Professional Rugby Union 2014 Super Rugby Competition. Orthop J Sport Med. 2016;4:1–10.
Sugiura Y, Sakuma K, Sakuraba K, Sato Y. Prevention of hamstring injuries in collegiate sprinters. Orthop J Sport Med. 2017;5:1–6.
Aagaard P, Simonsen EB, Magnusson SP, Larsson B, Dyhre-Poulsen P. A new concept for isokinetic hamstring: quadriceps muscle strength ratio. Am J Sports Med. 1998;26:231–7.
Whiteley R, Jacobsen P, Prior S, Skazalski C, Otten R, Johnson A. Correlation of isokinetic and novel hand-held dynamometry measures of knee flexion and extension strength testing. J Sci Med Sport. 2012;15:444–50.
Tous-Fajardo J, Maldonado RA, Quintana JM, Pozzo M, Tesch PA. The flywheel leg-curl machine: offering eccentric overload for hamstring development. Int J Sports Physiol Perform. 2006;1:293–8.
Opar DA, Piatkowski T, Williams MD, Shield AJ. A novel device using the Nordic hamstring exercise to assess eccentric knee flexor strength: a reliability and retrospective injury study. J Orthop Sports Phys Ther. 2013;43:636–40.
Buchheit M, Cholley Y, Nagel M, Poulos N. The effect of body mass on eccentric knee-flexor strength assessed with an instrumented Nordic hamstring device (Nordbord) in football players. Int J Sports Physiol Perform. 2016;11:721–6.
Macdonald B. An investigation into the immediate effects of pelvic taping on hamstring eccentric force in an elite male sprinter – a case report. Phys Ther Sport. 2017;28:15–22.
Wik EH, Auliffe SM, Read PJ. Examination of physical characteristics and positional differences in professional soccer players in Qatar. Sports. 2018;7(1):9.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097.
Saw AE, Main LC, Gastin PB. Monitoring the athlete training response: subjective self-reported measures trump commonly used objective measures: a systematic review. Br J Sports Med. 2016;50:281–91.
Horsley T, Dingwall O, Sampson M. Checking reference lists to find additional studies for systematic reviews. Cochrane Database Syst Rev. 2011;(8):MR000026. https://doi.org/10.1002/14651858.MR000026.pub2. Accessed 10 Jan 2021.
Markovic G, Sarabon N, Boban F, Zoric I, Jelcic M, Sos K, et al. Nordic hamstring strength of highly trained youth football players and its relation to sprint performance. J Strength Cond Res. 2020;34:800–7.
van Dyk N, Witvrouw E, Bahr R. Interseason variability in isokinetic strength and poor correlation with Nordic hamstring eccentric strength in football players. Scand J Med Sci Sports. 2018;28:1878–87.
Vicens-Bordas J, Esteve E, Fort-Vanmeerhaeghe A, Bandholm T, Clausen MB, Opar DA, et al. Eccentric hamstring strength is associated with age and duration of previous season hamstring injury in male soccer players. Int J Sports Phys Ther. 2020;15:246–53.
Ribeiro-Alvares JB, Oliveira GDS, De Lima-E-Silva FX, Baroni BM. Eccentric knee flexor strength of professional football players with and without hamstring injury in the prior season. Eur J Sport Sci. 2020;1-9. https://doi.org/10.1080/17461391.2020.1743766 [published online ahead of print, 2020 Mar 26].
Giakoumis M, Pollock N, Mias E, McAleer S, Kelly S, Brown F, et al. Eccentric hamstring strength in elite track and field athletes on the British Athletics world class performance program. Phys Ther Sport. 2020;43:217–23.
Hegyi A, Lahti J, Giacomo J-P, Gerus P, Cronin NJ, Morin J-B. Impact of hip flexion angle on unilateral and bilateral Nordic hamstring exercise torque and high-density electromyography activity. J Orthop Sport Phys Ther. 2019;49:584–92.
Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. Eccentric hamstring strength and hamstring injury risk in Australian footballers. Med Sci Sports Exerc. 2015;47:857–65.
Bourne MN, Opar DA, Williams MD, Shield AJ. Eccentric knee flexor strength and risk of hamstring injuries in rugby union. Am J Sports Med. 2015;43:2663–70.
Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. The effect of previous hamstring strain injuries on the change in eccentric hamstring strength during preseason training in elite Australian footballers. Am J Sports Med. 2015;43:377–84.
Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. 2016;50:1524–35.
van Dyk N, Bahr R, Burnett AF, Whiteley R, Bakken A, Mosler A, et al. A comprehensive strength testing protocol offers no clinical value in predicting risk of hamstring injury: a prospective cohort study of 413 professional football players. Br J Sports Med. 2017;51:1695–702.
Chalker WJ, Shield AJ, Opar DA, Rathbone EN, Keogh JWL. Effect of acute augmented feedback on between limb asymmetries and eccentric knee flexor strength during the Nordic hamstring exercise. PeerJ. 2018;6:e4972.
Isik A, Unlu G, Gozubuyuk OB, Aslanyurek T, Bereceli C. The relationship between previous lower extremity injury, body weight and bilateral eccentric hamstring strength imbalance in young soccer players. Montenegrin J Sport Sci Med. 2018;7:23–8.
Franchi MV, Ellenberger L, Javet M, Bruhin B, Romann M, Frey WO, Spörri J. Maximal eccentric hamstrings strength in competitive alpine skiers: cross-sectional observations from youth to elite level. Front Physiol. 2019;10:88.
Thiese MS. Observational and interventional study design types; an overview. Biochem Med. 2014;24:199–210.
Wulf G, Shea CH. Principles derived from the study of simple skills do not generalize to complex skill learning. Psychon Bull Rev. 2002;9:185–211.
Magill R, Anderson D. Motor learning and control: concepts and applications. 11th ed. New York City: McGraw-Hill Higher Education; 2016.
Currell K, Jeukendrup AE. Validity, reliability and sensitivity of measures of sporting performance. Sport Med. 2008;38:297–316.
Claudino JG, Mezêncio B, Soncin R, Ferreira JC, Valadão PF, Takao PP, et al. Development of an individualized familiarization method for vertical jumps. Rev Bras Med Esporte. 2013;19:359–62.
Bonnette S, Dicesare CA, Kiefer AW, Riley MA, Foss KDB, Thomas S, et al. A technical report on the development of a real-time visual biofeedback system to optimize motor learning and movement deficit correction. J Sport Sci Med. 2020;19:84–94.
Myer GD, Stroube BW, Dicesare CA, Brent JL, Ford KR, Heidt RS, et al. Augmented feedback supports skill transfer and reduces high-risk injury landing mechanics: a double-blind, randomized controlled laboratory study. Am J Sports Med. 2013;41:669–77.
Croisier JL, Ganteaume S, Binet J, Genty M, Ferret JM. Strength imbalances and prevention of hamstring injury in professional soccer players: a prospective study. Am J Sports Med. 2008;36:1469–75.
van Dyk N, Bahr R, Whiteley R, Tol JL, Kumar BD, Hamilton B, Farooq A, Witvrouw E. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: a 4-year cohort study. Am J Sports Med. 2016;44:1789–95.
Jakobi JM, Chilibeck PD. Bilateral and unilateral contractions: possible differences in maximal voluntary force. Can J Appl Physiol. 2001;26:12–33.
Zemski AJ, Slater GJ, Broad EM. Body composition characteristics of elite Australian rugby union athletes according to playing position and ethnicity. J Sports Sci. 2015;33:970–8.
Bilsborough JC, Greenway KG, Opar DA, Livingstone SG, Cordy JT, Bird SR, et al. Comparison of anthropometry, upper-body strength, and lower-body power characteristics in different levels of Australian Football Players. J Strength Cond Res. 2015;29:826–34.
Grant D, David P, Sue H. Applied physiology and game analysis of Rugby Union. Sport Med. 2003;33:973–91.
Orchard JW, Seward H, Orchard JJ. Results of 2 decades of injury surveillance and public release of data in the Australian Football League. Am J Sports Med. 2013;41:734–41.
Green B, Bourne MN, van Dyk N, Pizzari T. Recalibrating the risk of hamstring strain injury (HSI): a 2020 systematic review and meta-analysis of risk factors for index and recurrent hamstring strain injury in sport. Br J Sports Med. 2020;54:1081–8.
Kenneally-Dabrowski CJB, Brown NAT, Lai AKM, Perriman D, Spratford W, Serpell BG. Late swing or early stance? A narrative review of hamstring injury mechanisms during high-speed running. Scand J Med Sci Sport. 2019;29:1083–91.
Chumanov ES, Schache AG, Heiderscheit BC, Thelen DG. Hamstrings are most susceptible to injury during the late swing phase of sprinting. Br J Sports Med. 2012;46(2):90.
Schache AG, Dorn TW, Blanch PD, Brown NAT, Pandy MG. Mechanics of the human hamstring muscles during sprinting. Med Sci Sports Exerc. 2012;44:647–58.
Schache AG, Dorn TW, Wrigley TV, Brown NATT, Pandy MG. Stretch and activation of the human biarticular hamstrings across a range of running speeds. Eur J Appl Physiol. 2013;113:2813–28.
Schimitt B, Tyler T, McHugh M. Hamstring injury rehabilitation and prevention of reinjury using lengthened state eccentric training: a new concept. J Sci Med Sport. 2012;7:333–41.
Novacheck TF. The biomechanics of running. Gait Posture. 1998;7:77–95.
Mann RA, Hagy J. Biomechanics of walking, running, and sprinting. Am J Sports Med. 1980;8:345–50.
Schache AG, Dorn TW, Williams GP, Brown NAT, Pandy MG. Lower-limb muscular strategies for increasing running speed. J Orthop Sports Phys Ther. 2014;44:813–24.
Orchard JW. Hamstrings are most susceptible to injury during the early stance phase of sprinting. Br J Sports Med. 2012;46:88–9.
Kyröläinen H, Avela J, Komi PV. Changes in muscle activity with increasing running speed. J Sports Sci. 2005;23:1101–9.
Askling C, Saartok T, Thorstensson A. Type of acute hamstring strain affects flexibility, strength, and time to return to pre-injury level. Br J Sports Med. 2006;40:40–4.
Wiesinger H-P, Gressenbauer C, Kosters A, Scharinger M, Muller E. Device and method matter: a critical evaluation of eccentric hamstring muscle strength assessments. Scand J Med Sci Sports. 2020;30:217–26.
Hegyi A, Gonçalves BAM, Finni T, Cronin NJ. Individual region- and muscle-specific hamstring activity at different running speeds. Med Sci Sports Exerc. 2019;51:2274–85.
Hegyi A, Péter A, Finni T, Cronin NJ. Region-dependent hamstrings activity in Nordic hamstring exercise and stiff-leg deadlift defined with high-density electromyography. Scand J Med Sci Sport. 2018;28:992–1000.
Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sport Med. 2012;42:209–26.
Al Attar WSA, Soomro N, Sinclair PJ, Pappas E, Sanders RH. Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players: a systematic review and meta-analysis. Sport Med. 2017;47:907–16.
Petersen J, Thorborg K, Nielsen MB, Budtz-Jørgensen E, Hölmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer: a cluster-randomized controlled trial. Am J Sports Med. 2011;39:2296–303.
Van Dyk N, Behan FP, Whiteley R. Including the Nordic hamstring exercise in injury prevention programmes halves the rate of hamstring injuries: a systematic review and meta-analysis of 8459 athletes. Br J Sports Med. 2019;53:1362–70.
Van Der Horst N, Smits DW, Petersen J, Goedhart EA, Backx FJG. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. Am J Sports Med. 2015;43:1316–23.
Freckleton G, Pizzari T. Risk factors for hamstring muscle strain injury in sport: a systematic review and meta-analysis. Br J Sports Med. 2013;47:351–8.
Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition - narrative review and new concept. Br J Sports Med. 2016;50:1309–14.
Bourne MN, Timmins RG, Opar DA, Pizzari T, Ruddy JD, Sims C, et al. An evidence-based framework for strengthening exercises to prevent hamstring injury. Sport Med. 2018;48:251–67.
Hunter JP, Marshall RN, McNair PJ. Relationships between ground reaction force impulse and kinematics of sprint-running acceleration. J Appl Biomech. 2005;21:31–43.
Kawamori N, Nosaka K, Newton RU. Relationships between ground reaction impulse and sprint acceleration performance in team sport athletes. J Strength Cond Res. 2013;27:568–73.
Morin JB, Gimenez P, Edouard P, Arnal P, Jiménez-Reyes P, Samozino P, et al. Sprint acceleration mechanics: the major role of hamstrings in horizontal force production. Front Physiol. 2015;6:1–14.
Ishøi L, Aagaard P, Nielsen MF, Thornton KB, Krommes KK, Hölmich P, Thorborg K. The influence of hamstring muscle peak torque and rate of torque development for sprinting performance in football players: a cross-sectional study. Int J Sports Physiol Perform. 2019;14:665–73.
Romero-Franco N, Jiménez-Reyes P, Castaño-Zambudio A, Capelo-Ramírez F, Rodríguez-Juan JJ, González-Hernández J, Toscano-Bendala FJ, Cuadrado-Peñafiel V, Balsalobre-Fernández C. Sprint performance and mechanical outputs computed with an iPhone app: comparison with existing reference methods. Eur J Sport Sci. 2017;17:386–92.
Mendiguchia J, Edouard P, Samozino P, Brughelli M, Cross M, Ross A, Gill N, Morin JB. Field monitoring of sprinting power-force-velocity profile before, during and after hamstring injury: two case reports. J Sports Sci. 2016;34:535–41.
Nagahara R, Mizutani M, Matsuo A, Kanehisa H, Fukunaga T. Association of sprint performance with ground reaction forces during acceleration and maximal speed phases in a single sprint. J Appl Biomech. 2018;34:104–10.
Wdowski MM, Gittoes MJR. First-stance phase force contributions to acceleration sprint performance in semi-professional soccer players. Eur J Sport Sci. 2020;20:366–74.
Loturco I, DʼAngelo RA, Fernandes V, et al. Relationship between sprint ability and loaded/unloaded jump tests in elite sprinters. J Strength Cond Res. 2015;29(3):758–64.
McFarland I, Dawes JJ, Elder C, Lockie R. Relationship of two vertical jumping tests to sprint and change of direction speed among male and female collegiate soccer players. Sports. 2016;4:11.
Asadi A. Relationship between jumping ability, agility and sprint performance of elite young basketball players: a field-test approach. Brazilian J Kinanthropometry Hum Perform. 2016;18:177–86.
Claudino JG, Cronin J, Mezêncio B, McMaster DT, McGuigan M, Tricoli V, et al. The countermovement jump to monitor neuromuscular status: a meta-analysis. J Sci Med Sport. 2017;20:397–402.
Claudino JG, Cronin JB, Amadio AC, Serrão JC. How can the training load be adjusted individually in athletes with an applied statistical approach? J Athl Enhanc. 2016;5:6.
Acknowledgements
We would like to thank for the authors of cited articles who collaborated to obtain the data.
Funding
No sources of funding were used to assist in the design, collection, analysis, and interpretation of data or in writing of this manuscript.
Author information
Authors and Affiliations
Contributions
JGC: design, collection, analysis, interpretation of data, and writing up of the paper. CACF: design, collection, analysis, interpretation of data, and writing up of the paper. NFNB: design, collection, analysis, interpretation of data, and writing up of the paper. LGG: interpretation of data and writing up of the paper. CRC: design, collection, analysis, interpretation of data, and writing up of the paper. RCQ: interpretation of data and writing up of the paper. GFR: interpretation of data and writing up of the paper. OOJ: design, interpretation of data, and writing up of the paper: ACMP: interpretation of data and writing up of the paper. DB: interpretation of data and writing up of the paper. JCS: design, collection, analysis, interpretation of data and writing up of the paper. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
All authors consent to the publication of the manuscript.
Competing Interests
João Gustavo Claudino, Carlos Alberto Cardoso Filho, Natália Franco Netto Bittencourt, Luiz Guilherme Gonçalves, Crislaine Rangel Couto, Roberto Chiari Quintão, Guilherme Fialho Reis, Otaviano de Oliveira Júnior, Alberto Carlos Amadio, Daniel Boullosa, and Júlio Cerca Serrão declare that they have no conflicts of interest relevant to the content of this review.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Claudino, J.G., Cardoso Filho, C.A., Bittencourt, N.F.N. et al. Eccentric Strength Assessment of Hamstring Muscles with New Technologies: a Systematic Review of Current Methods and Clinical Implications. Sports Med - Open 7, 10 (2021). https://doi.org/10.1186/s40798-021-00298-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-021-00298-7