
Abstract
Soccer is the most popular sport in the world. Expectedly, the incidence of soccer-related injuries is high and these injuries exert a significant burden on individuals and families, including health and financial burdens, and on the socioeconomic and healthcare systems. Using established injury prevention frameworks, we present a concise synthesis of the most recent scientific evidence regarding injury rates, characteristics, mechanisms, risk and protective factors, interventions for prevention, and implementation of interventions in soccer. In this umbrella review, we elucidate the most recent available evidence gleaned primarily from systematic reviews and meta-analyses. Further, we express the exigent need to move current soccer injury prevention research evidence into action for improved player outcomes and widespread impact through increased attention to dissemination and implementation research. Additionally, we highlight the importance of an enabling context and effective implementation strategies for the successful integration of evidence-based injury prevention programs into real-world soccer settings. This narrative umbrella review provides guidance to inform future research, practice, and policy towards reducing injuries among soccer players.
Similar content being viewed by others


Key Points
-
This review provides a one-stop evidence reference regarding the prevention of soccer injuries, including evidence and perspectives on the implementation of proven interventions.
-
Overall evidence supports the use of the 11+ neuromuscular training warm-up and focused strength training, and there is emerging evidence for load management programs to mitigate injury risk among soccer players.
-
Theory-driven dissemination and implementation studies are needed to improve the adoption, adherence, appropriate adaptation, scale-up, and sustainment of evidence-based injury prevention interventions in soccer.
-
The findings from this review provide guidance to inform future research, practice, and policy towards reducing injuries among soccer players.
Background
Soccer (football) is the most popular sport in the world [1], with some 270 million involved in the sport worldwide in 2006 [2]. For approximately 110,000, it is a profession and thus a source of income; for some 38 million registered players, it is a team game organized within leagues and competitions; and for about 226 million others, it is an enjoyable exercise surrogate for fitness and health [2]. The health benefits of soccer as “medicinal exercise” are well documented, for example, improved cardiovascular health, mental health, and bone health [3]. However, there is a paradoxical negative effect of soccer on health when players get injured (e.g., obesity or post-traumatic osteoarthritis after an anterior cruciate ligament injury) [4, 5]. Furthermore, soccer injuries exert a significant burden on socioeconomic and healthcare systems [6]. Founded on established epidemiological frameworks describing the sequence of research steps to effective injury prevention practice [7, 8]—from identifying injury rates to the implementation of effective interventions—we present a narrative umbrella review that articulates best available evidence to inform guidelines, practice, and policy towards mitigating the risk of injuries in soccer, and in turn maximizing the benefits of participation among individuals.
Methods
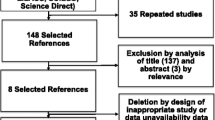
To achieve the above-mentioned purpose, we conducted methodical searches across five databases (MEDLINE, SPORTDiscus, PsycINFO, CINAHL, and Cochrane Database of Systematic Reviews) from January 2010 to January 2020 to identify all systematic reviews, meta-analyses, reviews, and original research (where limited or no reviews were available) across soccer injury studies that investigated injury incidence, characteristics, mechanisms, risk and protective factors, interventions for prevention, and implementation and evaluation of interventions. A summary of the search records for our primary source of data (systematic and narrative reviews) is presented in Table 1, and details of the search terms used—key concepts and search words—are presented in an additional file (Supplementary File). Our search strategy involved the use of relevant search descriptors of “OR” and “AND” to combine search/key words and key concepts, respectively, after each search word was exploded (exp) to capture all literature possible. Search records were limited to articles with full text, written in the English language, and relating to humans. The same methodology was used to obtain primary research articles where no reviews were available.
Results
Injury Rates
Injury incidence among soccer players differs across levels of participation, age, type of exposure, and sex. The incidence of injuries in soccer is mostly significant during games/matches, ranging from 9.5 to 48.7 injuries/1000 h among competitive male youth players, 2.5 to 8.7 injuries/1000 h among male professional players, and 12.5 to 30.3 injuries/1000 h among female players [9,10,11,12] (Table 2). The incidence of injuries appears higher among males vs. females, and injury incidence is higher during games/matches vs. practice/training for all participation categories, among both male and female players [10,11,12]. Soccer players younger than 12 years of age have a lower injury rate (1.0–1.6 injuries per 1000 h) compared to older players [9].
Injury Location and Type
Most soccer injuries occur in the lower limbs (60–90%), especially the ankle, knee, and thigh [10,11,12,13,14]. Among male players, the most common injuries affect the hamstring muscles followed by the ankle, knee, and groin [11, 13]. Comparably, among female players, knee and ankle injuries are the most common, followed by thigh/hamstring injuries [10, 13].
Thigh, Knee, and Ankle Injuries
Most thigh injuries result from strains with a high proportion of hamstring injuries, despite quadriceps injuries leading to longer absence from play [15]. The prevalence and history of hamstring injury is greater among adult professional players (40%) compared to under-20 players (18%) [16]. Up to 18% of severe soccer injuries presenting at hospital emergency departments involve the knee [17]. One such injury involves the anterior cruciate ligament (ACL). The ACL injury rate among females (2.0/10,000 athlete exposures) is 2.2 times higher than that of males (0.9/10,000 athlete exposures), independent of participation level [18]. Ankle injuries account for up to 20% of all soccer injuries with ankle sprains constituting 77% of all ankle injuries [14, 19].
Concussion
The prevalence of concussion in youth soccer appears to be relatively low with an incidence of 0.19 (95% CI 0.16–0.21) concussions per 1000 athletic exposures and 0.27 (95% CI 0.24–0.30) concussions per 1000 athletic exposures among male and female players, respectively [20]. A higher concussion incidence has been consistently reported among females [10, 20].
Injury Mechanisms
Overall, about two-thirds of soccer injuries are traumatic and the other one-third (27–33%) are caused by overuse [11, 12, 21]. These findings are based on a medical attention/time-loss injury definition, and emerging evidence from studies using an all-complaint injury definition suggests that overuse onset injuries may be as prevalent as acute onset injuries [22]. About two-thirds of traumatic injuries are contact injuries, of which 12–28% are caused by foul play. Notably, non-contact injuries account for 26–58% of all injuries [13, 21]. Injuries occur primarily during the initial or final 15 min of the match, indicating the significance of an appropriate warm-up and the effects of fatigue on players [23].
Risk and Protective Factors
Non-modifiable Risk Factors
Player Position
Goalkeepers are at a lower overall risk of injury compared to outfield players in the male game [24]. Independent of goalkeepers, current evidence is inconsistent regarding the association between player position and injury risk; however, it appears that strikers may be at a greater risk as compared with other outfield players during matches [24].
Previous Injury
A history of previous injury continues to be the most consistent and strongest risk factor for future injury, and this also holds true for specific injuries [9, 25,26,27,28,29]. For example, a history of previous hamstring injury is associated with future hamstring injury among male players [25, 28], previous ACL injury is associated with risk of future ACL injury [29], and previous ankle sprain injury is related to the emergence of new ankle sprain injuries [27].
Age
Current evidence regarding age as a risk factor for soccer injury is limited. One systematic review suggested that increasing age was a risk factor for future hamstring injury among male players [25]. Another systematic review concluded that existing literature was insufficient to infer any relationship between age and the risk of ACL injury among soccer players [29]. In a single prospective study, age > 14 years was a significant risk factor for future acute knee injury among female players [30].
Genetics
Familial predisposition for ACL injury is associated with increased risk of ACL injury and acute knee injury [29, 30].
Sex
Overall, the incidence of injuries is higher among males vs. females [10, 11]; however, female sex is associated with increased ACL injury risk [29].
Competitive Setting
Game exposure demonstrated increased injury risk compared to practice for both male and female soccer players [29, 31]. Furthermore, within the practice setting, the risk of injury is higher for scrimmage compared to normal practice and walk-through [29].
Shoe-Surface Interaction
Current research suggests there is an association between higher shoe-surface interaction and increased ACL injury risk [29].
Pre-season Knee Complaints
Females presenting with pre-season knee complaints appear to be at increased risk for acute knee injury during the season [30].
Early Sport Specialization
Though there is a lack of substantive evidence for soccer specifically, early sport specialization has been found to be associated with a greater risk for overuse injuries across multiple youth sports [9]. One study showed that female soccer players 12–15 years of age playing on more than one team had increased risk for lower extremity overuse injuries [32].
Growth and Leg Length
Elite male youth soccer players are at greater risk for traumatic injury in the year of peak height velocity [33]. A recent prospective study of male soccer players aged 10–12 years shows an association between an increase in leg length throughout the season and risk for overuse injury [34]. The same study suggests an association between longer leg length and risk of overuse injury among male soccer players aged 13–15 years. Additionally, they found a higher weight and a decreased growth rate to be associated with an increased risk of acute injury.
Modifiable Risk Factors
Load
Evidence regarding load-injury relationships among soccer players is still emerging as reviews remain sparse in this area of inquiry. Current evidence across team sports indicates that load, in terms of player exposure and/or exertion, could either be an independent protective or risk factor for injury, depending on whether load administration is optimal and progressive or suboptimal (e.g., load spike), respectively, and that this relationship is likely moderated by other risk factors for injury [35,36,37,38,39,40]. Prospective studies showed that a high amount of absolute (accumulated or cumulative) load, based on different calculations of load measures (e.g., 1-weekly, 2-weekly), was associated with greater risk of injury among elite youth and professional soccer players [39,40,41]. These findings suggest that it may be expedient to have an absolute load threshold, for example, weekly load threshold, to further mitigate injury risk in soccer, especially youth soccer [39, 40]. Altogether, available evidence suggests that avoiding a spike in load (e.g., the acute to chronic workload ratio) is associated with less soccer injuries [39,40,41].
Neuromuscular Factors
Hamstring/quadriceps strength ratio imbalance is a key risk factor for hamstring muscle injury; specifically, decreased hamstring strength relative to quadriceps strength is a risk factor for knee ligamentous injuries in both male and female youth soccer players [29, 42]. Decreased single leg hop distance is also associated with increased hamstring injury risk [43]. While current evidence is inconclusive for muscle strength asymmetry (i.e., right vs. left) as a risk factor, eccentric hamstring strength asymmetry is specifically indicated as a key predictor of injury among male youth soccer players [26]. Furthermore, eccentric hamstring strength (< 256 N) and single leg hamstring bridge scores of less than 20 reps on the right leg are associated with increased risk of hamstring strain [43]. Poor landing mechanics, specifically, increased dynamic knee valgus, is associated with increased risk for lower limb injury, including ACL injury [9, 42, 43]. Leg dominance and leg asymmetry also relates to increased risk of injury; a difference of 15% or greater, between an individual’s dominant and non-dominant limb, has been shown to predict future injury [42]. An asymmetry of greater than 4 cm on the anterior reach portion of the Y-balance test places athletes at 2.5 times greater risk for injury among male youth soccer players [42, 43]. Hip external rotation strength scores using handheld dynamometry of less than 18% of the individual’s body weight is associated with lower extremity and back injuries [43]. Additionally, the literature suggests that the risk of injury may increase with altered neuromuscular firing during dynamic movements like cutting or landing, and dynamic stability deficits may increase lower extremity injury risk for male youth soccer players [42].
Protective Factors
Although mention of protective factors in review level evidence did not exist at the time of this evidence review, findings from original research previously described (under modifiable risk factors) signify load management as a viable target for mitigating injury risk in soccer. For example, an in-season relative load measure of acute to chronic workload ratio of 1 to 1.25 significantly reduced injuries among youth players [40], and a reduced absolute load significantly reduced injuries among youth and adult professional players [39, 40]. Additionally, current evidence suggests that improved neuromuscular capacity and control, including increased quadriceps, hamstring, hip flexor strength, and movement control are protective against injuries among soccer players [9, 26, 29, 42, 43].
Opportunities for Prevention
Effective Interventions
Drawing from available evidence regarding modifiable risk factors and protective factors for soccer injuries, injury prevention experts have developed and tested interventions for reducing musculoskeletal injuries in soccer. There is extensive high-quality evidence (including two reviews of systematic reviews) showing the clinical effectiveness of exercise-based interventions in the form of neuromuscular training (NMT) warm-up programs in reducing all soccer-related injuries across sex, ages, and skill levels. Specifically, the 11+ (formerly called the FIFA 11+) warm-up program reduces overall injury rate (i.e., all injuries) by 30 to 47% [23, 44,45,46], lower limb injury rate by 39 to 44% [44, 45], overuse injury rate by 55%, and knee injury rate by 52% [47]. Emerging evidence also suggests that the 11+ Kids (a version for children under 12 years old) is efficacious (48% reduction for all injuries) for reducing injuries in younger players [48]. Additionally, the “Knee Injury Prevention Program” (KIPP) has the potential to significantly reduce non-contact lower limb injury and overuse injury among young female soccer players by 50% and 56%, respectively [47].
In a recent systematic review, the application of a variety of exercise-based injury prevention programs for youth players was found to reduce injury rates by up to 46% [49]. Furthermore, the risk of hamstring injuries can be reduced by up to 51% when the Nordic Hamstring exercise is implemented in isolation [50]. A recent meta-analysis showed that ankle injuries can be reduced by as much as 40% [51] and a meta-analysis of meta-analyses [52] demonstrated that a 50% reduction can be achieved for all ACL injuries in a heterogeneous sample of athletes, including soccer players, when NMT warm-up is implemented.
Specific instructions on how to perform aforementioned NMT warm-up programs can be found in the International Olympic Committee’s “Get Set” app, an innovative and accessible mobile app that provides continued access to illustrative and video information regarding effective sport- and body-specific NMT warm-up programs, including the 11+ program. The 11+ program can also be accessed from the following website: https://www.youtube.com/watch?v=RSJIp7e7fyY
Although concussions are not frequent in soccer, sustaining a concussion may present severe and lasting negative health consequences [53]. It is important for coaches, parents, and administrators to be aware of concussion signs and symptoms and know what to do if concussion is suspected. For concussion prevention, there is evidence that education about concussion among key stakeholders, e.g., coaches, referees, and parents, can reduce the incidence of concussion and facilitate improved outcomes [54]. Interventions for primary (e.g., rule change and avoiding a slippery playing surface) and secondary (e.g., concussion recognition and decision on return to playtime) prevention are mainly informational for coaches and parents/guardians. A popular evidence-based educational tool is the Concussion Awareness Training Tool, available at https://cattonline.com.
Cost-Effectiveness of Interventions
Literature regarding the cost-effectiveness of injury prevention interventions in soccer is limited. A reduction of 43% was reported in healthcare costs in the training group that underwent an NMT warm-up similar to the 11+ program with additional use of a wobble-board, when compared to a standard practice control group [55]. Similarly, the “11+ Kids” program showed a 51% reduction in healthcare costs when compared with a regular warm-up [56].
Implementation and Evaluation
Literature regarding the evaluation of the implementation of efficacious/effective interventions such as the 11+ and other NMT warm-up programs is advancing despite the lack of reviews [57,58,59,60,61,62,63,64,65,66,67]. However, of all the studies currently available, only two reported using an implementation framework to evaluate a preventative program. The Reach Effectiveness Adoption Implementation Maintenance Framework was used in both studies: one to evaluate an NMT warm-up program for knee/ACL prevention, and the other to evaluate the Adductor Strengthening Program for groin injury prevention [57, 59]. Overall, the execution of NMT warm-up programs when implemented ranged between low and moderate [60, 68].
To improve the spread and implementation of evidence-based injury prevention intervention in soccer, an understanding of implementation contexts is imperative. Although more rigorous theory-driven studies are needed to further understand potential contextual moderators of successful/unsuccessful implementation, a small number of studies have investigated perceived facilitators and barriers to NMT programs across levels of soccer participation (Table 3).
Current Best Practices for Implementation
Literature regarding best practices for onward translation of evidence-based injury prevention programs into routine practice in community and professional soccer remains sparse, and the urgent need for research in this field of inquiry has been identified [70]. The following conclusions have been reached in existing literature:
-
(1)
Preseason structured coaching workshops have the potential to effectively increase coach attitudes, perceived behavioral control, self-efficacy, and intention and subsequent implementation of NMT programs [64, 71, 72]. However, it remains unclear whether high levels of behavioral determinants, i.e., cognitive and psychosocial factors, would ultimately result in high levels of program adherence and maintenance over time [57].
-
(2)
Coach-led delivery of the 11+ appears to be relatively sufficient in implementing the program; evidence on the advantage of having additional support or supervision from research or team staff, e.g., strength and conditioning coach, an athletic trainer, or physiotherapist, is mixed [57, 60, 71].
-
(3)
For maximum effectiveness, coaches need to ensure quality delivery to their teams by performing NMT warm-up exercises with proper technique and adhering to the program guidelines, while adapting it to fit their local setting. A minimum of 2× weekly appears to be optimal and thereby recommended [58, 61].
-
(4)
Quality implementation requires soccer associations and organizations at the federal, provincial, and community levels to enact policies that enforce injury prevention programs and education and policies that require coaches to use proven NMT warm-up programs such as the 11+ [60, 73, 74].
Conclusions and Call to Action
This review provides guidance to inform future research, policy, and practice towards reducing injuries among soccer players. It presents a one-stop evidence reference regarding the burden, etiology, and prevention of soccer injuries, including current opportunities for evidence-based interventions and their implementation. To achieve desired outcomes and population-level impact from injury prevention research evidence, evidence-based interventions need enabling contexts and effective implementation strategies for a successful integration into real-world settings. Consequently, innovators (e.g., researchers) and implementation actors at the organizational (e.g., football associations, government/public health agencies, non-profit organizations, football clubs) and individual (e.g., coaches, strength and conditioning personnel, medical staff) levels have critical roles to play and are urged to rise to the occasion.
Researchers need to acquire an appreciable level of proficiency in dissemination and implementation research designs to build upon current literature to advance dissemination and implementation science in soccer injury prevention. Specifically, theory-driven dissemination and implementation studies are needed to improve the adoption, adherence, appropriate adaptation, delivery, scale-up, and sustainment of evidence-based injury prevention interventions such as the 11+ in soccer. Researchers should move beyond randomized controlled trials evaluating efficacy in NMT programs (considering that there is extensive evidence supporting NMT efficacy ) to evaluating strategies for implementation in randomized controlled and pragmatic (e.g., quasi-experimental) trials. Further, researchers should use current information on implementation barriers to and facilitators of evidence-based interventions and knowledge from implementation science to conceptualize and test potential implementation strategies. In addition, soccer organizations and their staff, especially coaches, have the obligation of ensuring safety among their players. Collectively, researchers, knowledge brokers, policymakers, leaders, and administrators in soccer and other related organizations need to work collaboratively to move current injury prevention evidence into action in order to protect players’ current and future health.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated during the current study.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- NMT:
-
Neuromuscular training
References
Top-10 trending most popular sports in America 2019 | SportyTell [Internet].
FIFA Big Count 2006: 270 million people active in football [Internet]. 2007 [accessed 2020 Apr 1]. https://www.fifa.com/mm/document/fifafacts/bcoffsurv/bigcount.statspackage_7024.pdf.
Krustrup P, Dvorak J, Junge A, Bangsbo J. Executive summary: the health and fitness benefits of regular participation in small-sided football games. Scand J Med Sci Sports. 2010.
Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007.
Toomey CM, Whittaker JL, Nettel-Aguirre A, Reimer RA, Woodhouse LJ, Ghali B, et al. Higher fat mass is associated with a history of knee injury in youth sport. J Orthop Sports Phys Ther. 2017;.
Fuller CW. Assessing the return on investment of injury prevention procedures in professional football. Sports Med. 2019.
van Mechelen W, Hlobil H, Kemper HCG. Incidence, severity, aetiology and prevention of sports injuries: a review of concepts. Vol. 14, Sports Medicine: An International Journal of Applied Medicine and Science in Sport and Exercise. 1992. p. 82–99.
Finch C. A new framework for research leading to sports injury prevention. J Sci Med Sport. 2006;9(1–2):3–9.
Watson A, Mjaanes JM. Soccer injuries in children and adolescents. Pediatrics. 2019.
Junge A. Epidemiology in female football players. In: Football traumatology: new trends: Second Edition. 2015.
Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of injury incidences in male professional adult and elite youth soccer players: a systematic review. J Athl Train (Allen Press. 2016 May;51(5):410–424.
López-Valenciano A, Ruiz-Pérez I, Garcia-Gómez A, Vera-Garcia FJ, De Ste CM, Myer GD, et al. Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br J Sports Med. 2020.
Junge A, Dvorak J. Soccer injuries: a review on incidence and prevention. Sports Med. 2004;34(13):929–38.
Feria-Arias E, Boukhemis K, Kreulen C, Giza E. Foot and ankle injuries in soccer. Am J Orthop (Belle Mead NJ). 2018;.
Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of injury incidences in male professional adult and elite youth soccer players: a systematic review. J Athl Train. 2016.
Ribeiro-Alvares JB, Dornelles MP, Fritsch CG, de Lima-e-Silva FX, Medeiros TM, Severo-Silveira L, et al. Prevalence of hamstring strain injury risk factors in professional and under-20 male football (soccer) players. J Sport Rehabil. 2019.
Roth TS, Osbahr DC. Knee injuries in elite level soccer players. American journal of orthopedics (Belle Mead, N.J.). 2018.
Montalvo AM, Schneider DK, Silva PL, Yut L, Webster KE, Riley MA, et al. “What’s my risk of sustaining an ACL injury while playing football (soccer)?” A systematic review with meta-analysis. British Journal of Sports Medicine. 2019.
Fong DT-P, Hong Y, Chan L-K, Yung PS-H, Chan K-M. A systematic review on ankle injury and ankle sprain in sports. Sports Med. 2007;37(1):73–94.
Pfister T, Pfister K, Hagel B, Ghali WA, Ronksley PE. The incidence of concussion in youth sports: a systematic review and meta-analysis. Br J Sports Med. 2016 Mar;50(5):292–7.
Bizzini M, Dvorak J. FIFA 11+: an effective programme to prevent football injuries in various player groups worldwide-a narrative review. Br J Sports Med. 2015;49(9).
Harøy J, Clarsen B, Thorborg K, Hölmich P, Bahr R, Andersen TE. Groin problems in male soccer players are more common than previously reported. Am J Sports Med. 2017;45(6):1304–8.
Sadigursky D, Braid JA, De Lira DNL, Machado BAB, Carneiro RJF, Colavolpe PO. The FIFA 11+ injury prevention program for soccer players: a systematic review. BMC Sports Sci Med Rehabil. 2017.
Della Villa F, Mandelbaum BR, Lemak LJ. The effect of playing position on injury risk in male soccer players: systematic review of the literature and risk considerations for each playing position. American journal of orthopedics (Belle Mead, N.J.). 2018.
Hughes T, Sergeant JC, Parkes MJ, Callaghan MJ. Prognostic factors for specific lower extremity and spinal musculoskeletal injuries identified through medical screening and training load monitoring in professional football (soccer): a systematic review. BMJ Open Sport Exerc Med. 2017.
McCall A, Carling C, Davison M, Nedelec M, Le Gall F, Berthoin S, et al. Injury risk factors, screening tests and preventative strategies: a systematic review of the evidence that underpins the perceptions and practices of 44 football (soccer) teams from various premier leagues. Br J Sports Med. 2015 May;49(9):583–9.
Owoeye OBA, Palacios-Derflingher LM, Emery CA. Prevention of ankle sprain injuries in youth soccer and basketball: effectiveness of a neuromuscular training program and examining risk factors. Clin J Sport Med. 2018;28(4):325–31.
van Beijsterveldt AMC, van de Port IGL, Vereijken AJ, Backx FJG. Risk factors for hamstring injuries in male soccer players: a systematic review of prospective studies. Scand J Med Sci Sports. 2013;23(3):253–62.
Volpi P, Bisciotti GN, Chamari K, Cena E, Carimati G, Bragazzi NL. Risk factors of anterior cruciate ligament injury in football players: a systematic review of the literature. Muscles, Ligaments and Tendons Journal. 2016.
Hägglund M, Waldén M. Risk factors for acute knee injury in female youth football. Knee Surgery, Sport Traumatol Arthrosc. 2016;24(3):737–46.
Emery CA, Meeuwisse WH, Hartmann SE. Evaluation of risk factors for injury in adolescent soccer: implementation and validation of an injury surveillance system. Am J Sports Med. 2005;33(12):1882–91.
O’Kane JW, Neradilek M, Polissar N, Sabado L, Tencer A, Schiff MA. Risk factors for lower extremity overuse injuries in female youth soccer players. Orthop J Sport Med. 2017.
Read P, Oliver JL, De Ste Croix MBA, Myer GD, Lloyd RS. Injury risk factors in male youth soccer players. Strength Cond J (Lippincott Williams Wilkins). 2015 Oct;37(5):1–7.
Rommers N, Rössler R, Goossens L, Vaeyens R, Lenoir M, Witvrouw E, et al. Risk of acute and overuse injuries in youth elite soccer players: body size and growth matter. J Sci Med Sport. 2020.
Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;.
Malone S, Hughes B, Doran DA, Collins K, Gabbett TJ. Can the workload–injury relationship be moderated by improved strength, speed and repeated-sprint qualities? J Sci Med Sport. 2019;22(1).
Gabbett TJ, Hulin BT, Blanch P, Whiteley R. High training workloads alone do not cause sports injuries: how you get there is the real issue. Br J Sports Med. 2016;50(8):444–5.
Owoeye OBA. Digging deep into the etiology of basketball injuries: a complex systems approach for risk mitigation. In: Lavar L, Kocaoglu B, Bytomski J, Cole B, Arundale A AN, editor. The basketball sports medicine and science book. Springer; 2020.
Watson A, Brickson S, Brooks A, Dunn W. Subjective well-being and training load predict in-season injury and illness risk in female youth soccer players. Br J Sports Med. 2017.
Bowen L, Gross AS, Gimpel M, Li F-X. Accumulated workloads and the acute:chronic workload ratio relate to injury risk in elite youth football players. Br J Sports Med. 2016;bjsports-2015-095820.
Malone S, Owen A, Newton M, Mendes B, Collins KD, Gabbett TJ, et al. The acute:chonic workload ratio in relation to injury risk in professional soccer. J Sci Med Sport. 2016;0(0):646–8.
Read PJ, Oliver JL, De Ste Croix MBA, Myer GD, Lloyd RS. Neuromuscular risk factors for knee and ankle ligament injuries in male youth soccer players. Sports Medicine. 2016.
Read PJ, Oliver JL, De Ste Croix MBA, Myer GD, Lloyd RS. A review of field-based assessments of neuromuscular control and their utility in male youth soccer players. Journal of Strength and Conditioning Research. 2019.
Al Attar WSA, Alshehri MA. A meta-analysis of meta-analyses of the effectiveness of FIFA injury prevention programs in soccer. Scand J Med Sci Sports. 2019.
Al Attar WSA, Soomro N, Pappas E, Sinclair PJ, Sanders RH. How effective are F-MARC injury prevention programs for soccer players? A systematic review and meta-analysis. Sports Med. 2016;46(2):205–17.
Thorborg K, Krommes KK, Esteve E, Clausen MB, Bartels EM, Rathleff MS. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: a systematic review and meta-analysis of the FIFA 11 and 11+ programmes. Br J Sports Med. 2017;bjsports-2016-097066.
Herman K, Barton C, Malliaras P, Morrissey D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: a systematic review. BMC Med. 2012.
Rössler R, Junge A, Bizzini M, Verhagen E, Chomiak J, aus der Fünten K, et al. A multinational cluster randomised controlled trial to assess the efficacy of ‘11+ Kids’: a warm-up programme to prevent injuries in children’s football. Sport Med. 2018;.
Hanlon C, Krzak JJ, Prodoehl J, Hall KD. Effect of injury prevention programs on lower extremity performance in youth athletes: a systematic review. Sport Heal A Multidiscip Approach. 2020;12(1):12–22.
Al Attar WSA, Soomro N, Sinclair PJ, Pappas E, Sanders RH. Effect of injury prevention programs that include the Nordic hamstring exercise on hamstring injury rates in soccer players: a systematic review and meta-analysis. Sports Med. 2017;47(5):907–16.
Grimm NL, Jacobs JC, Kim J, Amendola A, Shea KG. Ankle injury prevention programs for soccer athletes are protective: a level-I meta-analysis. J Bone Joint Surg (Am Vol). 2016.
Webster KE, Hewett TE. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J Orthop Res. 2018.
Gardner RC, Yaffe K. Epidemiology of mild traumatic brain injury and neurodegenerative disease. Molecular and Cellular Neuroscience. 2015.
Tator CH. Sport concussion education and prevention. J Clin Sport Psychol. 2012.
Marshall DA, Lopatina E, Lacny S, Emery CA. Economic impact study: neuromuscular training reduces the burden of injuries and costs compared to standard warm-up in youth soccer. Br J Sports Med. 2016;bjsports-2015-095666-.
Rossler R, Verhagen E, Rommers N, Dvorak J, Junge A, Lichtenstein E, et al. Comparison of the “11+ Kids” injury prevention programme and a regular warmup in children’s football (soccer): a cost effectiveness analysis. Br J Sports Med. 2019.
Frank BS, Register-Mihalik J, Padua DA. High levels of coach intent to integrate a ACL injury prevention program into training does not translate to effective implementation. J Sci Med Sport. 2015;18(4):400–6.
Hägglund M, Atroshi I, Wagner P, Waldén M, Hagglund M, Atroshi I, et al. Superior compliance with a neuromuscular training programme is associated with fewer ACL injuries and fewer acute knee injuries in female adolescent football players: secondary analysis of an RCT. Br J Sports Med. 2013;47(15):974–9.
Harøy J, Wiger EG, Bahr R, Andersen TE. Implementation of the adductor strengthening programme: players primed for adoption but reluctant to maintain — a cross-sectional study. Scand J Med Sci Sports. 2019.
Joy EA, Taylor JR, Novak MA, Chen M, Fink BP, Porucznik CA. Factors influencing the implementation of anterior cruciate ligament injury prevention strategies by girls soccer coaches. J Strength Cond Res. 2013;27(8):2263–9.
Soligard T, Nilstad A, Steffen K, Myklebust G, Holme I, Dvorak J, et al. Compliance with a comprehensive warm-up programme to prevent injuries in youth football. Br J Sports Med. 2010;44(11):787–93.
Steffen K, Emery CA, Romiti M, Kang J, Bizzini M, Dvorak J, et al. High adherence to a neuromuscular injury prevention programme (FIFA 11+) improves functional balance and reduces injury risk in Canadian youth female football players: a cluster randomised trial. Br J Sports Med. 2013;47(12):794–802.
Lindblom H, Carlfjord S, Hägglund M. Adoption and use of an injury prevention exercise program in female football: a qualitative study among coaches. Scand J Med Sci Sports. 2018;28(3):1295–303.
McKay CD, Merrett CK, Emery CA. Predictors of FIFA 11+ implementation intention in female adolescent soccer: an application of the health action process approach (HAPA) model. Int J Environ Res Public Health. 2016;13(7).
O’Brien J, Finch CF. Injury prevention exercise programs for professional soccer: understanding the perceptions of the end-users. Clin J Sport Med. 2017.
Norcross MF, Johnson ST, Bovbjerg VE, Koester MC, Hoffman Marc F.; ORCID: http://orcid.org/0000-0001-5329-3925 MAAI-O http://orcid. org/Norcros. Factors influencing high school coaches’ adoption of injury prevention programs. [Internet]. Ardern Comstock, Donaldson, Finch, Finch, Finch, Finch, Frank, Gilchrist, Glasgow, Glasgow, Hagglund, Joy, Kamath, LaBella, Lindblom, McKay, Morrissey, Orr, Pate, Rogers, Rogers, Sadoghi, Sawyer, Soligard, Twomey, Van Tiggelen, White B, editor. Vol. 19, Journal of Science and Medicine in Sport. Norcross, Marc F., marc.norcross@oregonstate.edu: Elsevier Science; 2016. p. 299–304.
Donaldson A, Callaghan A, Bizzini M, Jowett A, Keyzer P, Nicholson M. Awareness and use of the 11+ injury prevention program among coaches of adolescent female football teams. Int J Sports Sci Coach. 2018;13(6):929–38.
Junge A, Lamprecht M, Stamm H, Hasler H, Bizzini M, Tschopp M, et al. Countrywide campaign to prevent soccer injuries in Swiss amateur players. Am J Sports Med. 2011.
O’Brien J, Young W, Finch CF. The use and modification of injury prevention exercises by professional youth soccer teams. Scand J Med Sci Sports. 2017.
Owoeye OBA, McKay CD, Verhagen EALM, Emery CA. Advancing adherence research in sport injury prevention [Internet]. Vol. 52, British Journal of Sports Medicine. 2018. p. 1078–9.
Steffen K, Meeuwisse WH, Romiti M, Kang J, McKay C, Bizzini M, et al. Evaluation of how different implementation strategies of an injury prevention programme (FIFA 11+) impact team adherence and injury risk in Canadian female youth football players: a cluster-randomised trial. Br J Sports Med. 2013;47(8):480–7.
Pryor JL, Root HJ, Vandermark LW, Pryor RR, Martinez JC, Trojian TH, et al. Coach-led preventive training program in youth soccer players improves movement technique. J Sci Med Sport. 2017;.
Bizzini M, Dvorak J. FIFA 11+: an effective programme to prevent football injuries in various player groups worldwide-a narrative review. Br J Sports Med. 2015;49(9):577–9.
Bizzini M, Junge A, Dvorak J. Implementation of the FIFA 11+ football warm up program: How to approach and convince the Football associations to invest in prevention. Br J Sport Med. 2013;47(12).
Acknowledgements
The funding for this review was managed by Pike, I. and Babul, S. of the British Columbia (BC) Injury Research and Prevention Unit and BC Children’s Hospital Research Institute and coordinated by Richmond, S. of the Canadian Injury Prevention Trainee Network.
Funding
Provided by the British Columbia Alliance for Healthy Living Society, Canada, and supported by the Saint Louis University, MO, USA.
Author information
Authors and Affiliations
Contributions
OO conceived the study and did the initial systematic literature search. MV did the updated literature search. OO and MV drafted the manuscript, and OO and IP substantially revised it. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
The authors, Oluwatoyosi Owoeye, Mitchell VanderWey, and Ian Pike, declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Additional file 1:.
Search terms
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Owoeye, O.B.A., VanderWey, M.J. & Pike, I. Reducing Injuries in Soccer (Football): an Umbrella Review of Best Evidence Across the Epidemiological Framework for Prevention. Sports Med - Open 6, 46 (2020). https://doi.org/10.1186/s40798-020-00274-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40798-020-00274-7