
Abstract
Purpose
The risk of breast cancer (BC) and related mortality have increased in Middle-East countries during recent decades. The relationship between several nutrient intakes and the risk of BC has been investigated in several studies. However, few studies have estimated the effects of patterns of different nutrient intake on the risk of BC in this region.
Methods
A total of 453 patients who were recently diagnosed with breast cancer and 516 healthy women participated in the current case–control study. To evaluate the dietary intakes, we used a validated 168-item food frequency questionnaire (FFQ) during the last year. Nutrient Patterns (NPs) were extracted through factor analysis (FA) of energy-adjusted twenty-six nutrients. The relationship between nutrient patterns and the risk of breast cancer in pre and post-menopausal women was estimated by multivariable regression.
Results
Four major nutrient patterns were identified in the current study. The first nutrient pattern was rich in animal protein, retinol, riboflavin, pantothenic acid, cobalamin, and calcium. Higher saturated fatty acids (SFAs), mono-unsaturated fatty acids (MUFAs), polyunsaturated fatty acids (PUFAs), and trans fatty acids (TFAs), and lower intakes of niacin were observed in nutrient pattern 2. The third nutrient pattern was rich in fiber, potassium, and vitamin C. Nutrient pattern 4, was associated with higher intakes of vegetable protein, alpha-tocopherol, and magnesium. A significant inverse relationship was observed between adherence to nutrient pattern 3 and the risk of BC in all participants [odds ratio (OR) = 0.70, 95% confidence interval (CI): 0.50, 0.97, P = 0.03) and pre-menopausal women (OR = 0.59 (0.39–0.89), P = 0.01).
Conclusion
Decreasing odds of breast cancer were observed by adherence to a nutrient pattern high in dietary fiber, vitamin C, and potassium. Future prospective investigations are recommended to confirm these findings.
Similar content being viewed by others


Introduction
Breast cancer is the most extensive cancer among women worldwide [1]. Breast cancer has been known as the cause of approximately 11.7 percent of all new cancer cases in 2020 [2]. In Iran, breast cancer is the most common malignancy in women and the fifth most fatal disease in the general population [3]. Almost 6,160 people are suffering from breast cancer annually, and 17 percent of them are not able to survive [4]. The average age of its onset has also changed from 40 to 30 years in recent years [5].
As a multifactorial disease, breast cancer can result from a combination of unmanageable risk factors such as genetics, sex, and estrogen [6] and modifiable ones like smoking, low physical activity, obesity, and alcohol drinking [7]. A healthy diet has also been considered a determinative factor in modifying breast cancer [8]. For example, it has been claimed that a healthy dietary pattern, rich in fruits, vegetables, and whole grains, with lower amounts of red meat and refined foods, can have a preventive role in breast cancer among women [9]. Adherence to a Mediterranean dietary pattern has also been shown to decrease the risk of breast cancer [10]. However, the synergistic effects of nutrients can challenge the accuracy of results in studies assessing the effects of different dietary patterns on the risk of diseases [11]. For example, a meta-analysis of 54 observational studies has observed reduced odds of breast cancer in higher categories of vitamin C consumption [12]. The combined intakes of vitamins C and E did not show any significant relationship with the risk of breast cancer in a prospective cohort investigation [13]. Therefore, different patterns of nutrients might be associated with the risk of breast cancer in several ways, which makes it critical to investigate this field.
Various nutrients might act synergically both in foods and the human body. Moreover, a single food is usually a combination of several nutrients with different functions [14]. Therefore, studying the effects of different patterns of nutrients on the risk of breast cancer might be much more helpful. The relationship between various nutrient patterns and the risk of cancers has been evaluated in previous studies. For instance, it has been shown that adherence to a “vitamins and fiber” nutrient pattern can significantly decrease the odds of lung cancer [15]. In addition, a significant reduction in the risk of colorectal cancer has been observed in the highest scores of “the antioxidants” nutrient pattern [16]. Yet, few studies have assessed the relationship between nutrient patterns and the risk of breast cancer [17,18,19,20,21]. The conflicting results of these studies might be associated with the difference between food sources and cooking methods in Middle Eastern countries in comparison with European countries [22]. For example, while one investigation suggested an increase in the risk of breast cancer adhering to a nutrient pattern rich in vitamin C in Jordan [17], others showed lower risks of breast cancer in higher tertiles of following a pattern with high values of vitamin C [18, 19]. Plus, although following an animal meat-based pattern was associated with a decrease in breast cancer risk in a study among the Italian population [20], a direct association was observed between adhering to a high-meat pattern and the risk of breast cancer in Uruguay [21]. Moreover, the early onset of an advanced stage of breast cancer can make it necessary to assess the effects of different nutrient patterns on breast cancer in this region [22].
A recent case–control study has examined the relationship between various nutrient patterns and the risk of breast cancer in Iran [18]. This study has shown an inverse relationship between a pattern high in B vitamins, vitamin C, magnesium, fiber, and carbohydrate, and the risk of breast cancer. However, this relationship was not adjusted for total energy intake which can make the results challenging. The small sample size of the mentioned study might also not bring accurate insight. Therefore, further assessments of the effects of different nutrient patterns on breast cancer can be necessary in Iran. The current study investigates the association between dietary nutrient patterns and the risk of breast cancer. This relationship was also investigated in pre and post-menopausal status, separately.
Subjects and methods
Study design and population
This case–control study was carried out on a population of 969 women aged 19 to 80 years old. Patients newly diagnosed with breast cancer (BC), who were referred to the cancer institute of Imam Khomeini Complex in Tehran, and had no previous history of cancer or long-term dietary restriction, were selected as the case group (n = 490). Healthy women (n = 509) were also recruited as the control group. These women were visitors, relatives, and friends of non-cancer patients who were hospitalized for other chronic diseases in the same hospital. They were matched to the case group by the city of residence and age group and enrolled into the study at the same time. Convenience sampling was used for choosing case and control groups. Participants who had not answered more than 70 questions of the food frequency questionnaire (FFQ) and subjects with a total energy intake higher than 5500 or lower than 800 kcal (n = 28) were excluded from the study. The total sample size considering the mentioned exclusions was 974 (n case = 473, n control = 501). All participants have signed a written informed consent form. The protocol of the current study was approved by the Bioethics Committee of Tehran University of Medical Science.
Dietary assessments
Common dietary intakes were assessed by applying a 168-item semi-quantitative FFQ. Trained researchers interviewed the participants about how often they have consumed specific foods in the last year. They could respond to the questions in terms of daily, weekly, or monthly. Specific portion sizes were also considered for reporting different food consumption. Subjects could represent their portion sizes if they were unable to use determinate ones. The validity of this FFQ was examined by comparing the reported amounts with two FFQs filled one year apart and 12 dietary recalls were answered every month [23, 24]. All reported values were converted to grams per day using household measurements [25]. The modified United States Department of Agriculture (USDA) for Iranian foods was used for computing total energy and nutrient intakes [26].
Assessment of other variables
Weight and height measurements were performed using a digital scale and a tape meter, respectively. Participants were shoeless, wore light clothes for weight measurements (to the nearest 100 g), and had a standing position to measure their height (to the nearest 0.5 cm). Body Mass Index (BMI) was calculated by dividing weight in kilograms (kg) by height in meters (m) squared. A 16-item Global Physical Activity Questionnaire (GPAQ) was applied to estimate subjects’ activity during the last year. This questionnaire consists of four domains that can evaluate activity levels in a normal week: activities related to a job, transportation activities, entertainment and exercise, and sedentary lifestyle. The obtained data were analyzed according to the GPAQ guidelines to assess metabolic equivalent hours during a typical week (MET-h/wk) [27]. Additional data on age, marital status, educational level, smoking habits, family history of breast cancer, pregnancy, onset age of menopause and menarche, hormone therapy, infertility history, and contraceptive usage were collected by performing a face-to-face interview.
Statistical analysis
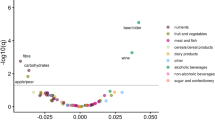
The nutrient intakes of participants were adjusted for energy and computed as the regression model’s residuals [28]. Factor analysis was conducted to identify major nutrient patterns among twenty-six macro and micro-nutrients. Considering the low amounts of vitamin D in Iranian food, it was not included in the factor analysis [29]. Kaiser–Meyer–Olkin (KMO) values higher than 0.70 were firmed as the required distribution of nutrients for conducting factor analysis (FA). Factors with eigenvalues higher than 0.2 and scree plot were applied to extract these patterns (Fig. 1). Factor loadings of nutrients have shown the relationship between every single nutrient and major nutrient patterns (Fig. 2). Following a special nutrient pattern is associated with lower intakes of nutrients with negative factor loadings and higher intakes of nutrients with positive factor loadings. The scores for each nutrient pattern were calculated by summing up the result of multiplying factor loadings of nutrient intakes by the amount of each nutrient intake. Participants were categorized based on the control group’s tertile scores. Continuous and categorical properties of participants across tertiles of each nutrient pattern were assessed by performing One-way ANOVA and chi-square tests, respectively. Mean intakes of macro and micro-nutrients of participants in the categories of each nutrient pattern were evaluated through the analysis of variance (ANOVA). Logistic regression was then performed to estimate odds Ratios (ORs) and 95% confidence intervals (95% CI) of breast cancer across tertiles of major nutrient patterns in crude and two multivariable-adjusted models. This relationship was adjusted for age and energy intake in model A. Additional adjustments for physical activity (PA), education, family history of breast cancer, smoking, marriage status, parity and Body Mass Index (BMI) were conducted in model B. The choice of confounders was done via literature review and LR test. P-values higher than 0.05 were considered significant. The relationship between nutrient patterns and the odds of breast cancer was also assessed separately among pre and post-menopausal women. Also, the interaction effect between nutrient patterns and menopausal status for risk of BC was assessed. These analyses were carried out by STATA version 14 (State Corp., College Station, TX). To create a radar chart visualizing nutrition patterns factor loadings, the Python package Plotly was utilized.

Scree plot

Nutrition patterns factor loadings showing the nutrients driving the nutrient patterns among Iranian women, including; Anim F: animal fat, Anim P: Animal protein, Calcium, CHO: carbohydrate, Chol: cholesterol, Fiber, Iron, Magnesium, MUFA: mono unsaturated fat, potassium, PUFA: poly unsaturated fat, Retinol, SFA: saturated fat, Selenium, Trans F: Trans-fat, veg F: vegetable fat, veg P: vegetable protein, vit B1: vitamin B1, vit B2: vitamin B2, vit B5: vitamin B5, vit B6: vitamin B6, vit B9: vitamin B9, vit B12:vitamin B12, vit C: vitamin C, Zinc, α-tocopherol, β-carotene
Results
This case–control study was carried out on a total population of 969 women (453 patients and 516 controls) aged 19 to 80 (mean age: 44.8 ± 10.8). Comparing the characteristics between case and control was previously shown [30]. Four dietary patterns were derived using the FA. Four major nutrient patterns were extracted through factor analysis which could explain 66.49% of participants’ overall intakes. The factor loadings of each nutrient across the main nutrient patterns are reported in Table 1. The first nutrient pattern, associated with higher values of animal protein, retinol, riboflavin, pantothenic acid, cobalamin, and calcium was characterized as “dairy, eggs, and fatty fish”. This pattern has described 21.53% of overall nutrient intakes. The second nutrient pattern, full of SFA, MUFA, PUFA, and TFA and correlated with a lower intake of niacin, was named “animal protein”. 17.57% of all nutrient intakes were explained by this nutrient pattern. Higher intakes of fiber, vitamin C, and potassium have been reported in the third nutrient pattern. So, it was characterized as “vegetables” and includes 16.25% of overall nutrient intakes. Nutrient pattern 4, correlated with higher amounts of vegetable protein, alpha-tocopherol, and magnesium was considered a “nuts and seeds” nutrient pattern.
The general characteristics of participants across tertiles of nutrient patterns have been described in Table 2. Educational level was higher in subjects in the highest tertile versus the lowest tertile of the first nutrient pattern (P < 0.01). Women in the third tertile of nutrient pattern 2 were younger (P = 0.005) and had lower BMI levels (P = 0.007) in comparison with the first tertile. On the other hand, the mean age (P = 0.007) and physical activity (P = < 0.01) of participants were higher in the highest tertile compared with the lowest tertile of the nutrient pattern 3. People in the highest tertiles of nutrient pattern 4 were also more physically active (P < 0.01) and had higher educational levels (P = 0.03).
The energy-adjusted dietary intakes of participants across tertiles of nutrient patterns have been shown in Table 3. Consumption of animal protein, carbohydrate, saturated fatty acids (SFAs), fiber, cholesterol, retinol, beta-carotene, calcium, magnesium, iron, zinc, selenium, potassium, vitamins B1, B2, B5, B6, B12, folate and vitamin C were significantly higher in the third tertile compared with the first tertile of nutrient pattern 1 (P < 0.01). However, significantly lower intakes of niacin, monounsaturated fatty acid (MUFA), polyunsaturated fatty acids (PUFAs), and trans fatty acids (TFAs) have been observed in highest versus lowest tertile of this nutrient pattern. Intakes of vegetable protein, cholesterol, retinol, cobalamin, alpha-tocopherol, SFA, mono-unsaturated fatty acids (MUFAs), PUFAs, and TFAs were significantly higher in the third tertile compared with the first tertile of nutrient pattern 2. While the overall consumption of animal protein, carbohydrate, fiber, beta carotene, thiamin, riboflavin, niacin, pantothenic acid, folate, vitamin C, calcium, magnesium, iron, zinc, selenium and potassium significantly reduced in highest tertile in comparison with the lowest tertile of the second nutrient pattern. The highest tertile of nutrient pattern 3, compared to the lowest tertile, was significantly associated with higher intakes of carbohydrate, fiber, beta carotene, vitamins B1, B2, B5, B12, C, and folate, alpha-tocopherol, calcium, magnesium, iron, and potassium, and lower intakes of cholesterol, retinol, niacin, zinc, selenium, SFA, PUFA, MUFAs, and TFAs. Higher, statistically significant consumption of animal protein, vegetable protein, carbohydrate, fiber, cholesterol, beta carotene, thiamin, riboflavin, pantothenic acid, folate, cobalamin, vitamin C, alpha-tocopherol, calcium, magnesium, iron, zinc, selenium, PUFAs, and potassium was observed in the highest tertile of nutrient pattern 4 compared to the lowest tertile. However, the third tertile of this nutrient pattern compared to the first tertile was significantly associated with lower intakes of niacin, SFA, MUFA, and TFA.
Crude and adjusted Odds Ratios and 95% CIs of breast cancer across tertiles of each nutrient pattern have been shown in Table 4. No significant association was observed between the first nutrient pattern and the risk of breast cancer either in crude or adjusted models. A significant direct relationship has been shown between the second nutrient pattern and the risk of breast cancer after controlling for age and energy intake in model A (OR = 1.41, 95% CI: 1.03,1.95, P = 0.03). However, no increase in the risk of breast cancer was observed by adherence to the second pattern after further adjustments for physical activity, educational level, family history of breast cancer, smoking, marriage status, and BMI in model B. Adherence to the third nutrient pattern has been associated with a reduction in the risk of breast cancer after adjusting for age and energy intake in the first model (OR = 0.69, 95% CI: 0.50, 0.95, P = 0.02). This relationship was also significant after further adjustments for other potential covariates in model B (OR = 0.70, 95% CI: 0.50, 0.97, P = 0.03). The relationship between nutrient pattern 4 and the risk of breast cancer was not significant in crude or adjusted models. There was no significant interaction effect between nutrient patterns and menopausal status for risk of BC in whole population after controlling for confounders.
Table 5 shows the stratified association between nutrient pattern and the risk of breast cancer among pre and post-menopause subjects. Adhering to the third nutrient pattern was indirectly associated with breast cancer risk in crude and adjusted models among premenopausal women (OR = 0.59, 95%CI: 0.39–0.89, P = 0.01). However, the relationship between other nutrient patterns and the odds of breast cancer was not significant. On the other hand, A significant inverse relationship was estimated between the first nutrient pattern and the risk of breast cancer after adjusting for age and total energy intake in the first model among post-menopausal women. This association was not significant in the model B after further controls for physical activity, BMI, marital status, education, previous history of breast cancer, smoking, and parity. Moreover, following the second nutrient pattern (animal protein pattern) was correlated with an increase in the risk of breast cancer in crude and partial adjustment models for age and energy intake. However, this relationship was no longer significant in the fully adjusted model among this population. No significant association was observed between other nutrient patterns and the risk of breast cancer among post-menopausal participants.
Discussion
In the current study, we evaluated the relationship between nutrient patterns and the risk of breast cancer in the context of a large case–control study. Four major nutrient patterns were diagnosed. The third nutrient pattern which was high in dietary fiber, potassium, and vitamin C was associated with a significant reduction in the risk of breast cancer in partial and fully adjusted models. This relationship was also significant in pre-menopausal but not post-menopausal women.
Few studies have examined the correlation between several nutrient patterns and the risk of breast cancer, previously. For example, a case–control study was carried out on a population of 401 healthy and patient Iranian women in 2018. In line with our results, this study has found an inverse relationship between following a nutrient pattern, characterized by higher intakes of B vitamins, potassium vitamin C, fiber, magnesium, iron, selenium, zinc, protein, carbohydrate, and calcium, and the risk of breast cancer. However, this relationship was not adjusted for energy intake in this study [18]. Despite these results, another case–control study conducted on 400 Jordanian women has shown a direct association between following the “vitamin C and beta-carotene” nutrient pattern and the risk of breast cancer [17]. This pattern was characterized by higher intakes of vitamin C, fiber, iron, folic acid, SFA, and cholesterol. However, this study has also demonstrated that adherence to the “high fat” nutrient pattern, with higher values of MUFA, PUFA, vegetable fat, and vegetable protein was correlated with an increase in the risk of breast cancer. This association might support the results of the current study. A reduction in the risk of BC was also observed by following the “calcium, phosphorus, and vitamin D” nutrient pattern in this investigation. Contrary to our results, a case–control study in Italy, found an inverse association between following the patterns named “animal product” and “unsaturated fatty acid” and the risk of breast cancer. These nutrient patterns were rich in animal protein, SFA, cholesterol, PUFA, MUFA, vitamin E, and animal and vegetable fats [20]. However, aligned with our results, a case–control study has shown an increase in the risk of breast cancer by following the “high meat” nutrient pattern (rich in SFA, MUFA, protein, and cholesterol). A significant inverse relationship was also observed by adherence to the “antioxidant” pattern (rich in vitamin C, vitamin E, flavonoids, glucose, and fructose) [21]. A prospective cohort study on 334,850 European women (EPIC study) has also suggested lower risks of breast cancer in correlation with following the “vegetables, fruits, and cereals” nutrient pattern (full of beta-carotene, fiber, vitamin C, and folate) [19].
In the present study, we found an inverse relationship between following a nutrient pattern, rich in vitamin C, potassium, and dietary fiber, and the risk of breast cancer. The protective role of these nutrients in the management of breast cancer has been assessed in several studies. For example, a meta-analysis of 69 observational studies has suggested a significant decrease in breast cancer incidence and mortality through higher vitamin C intakes [12]. Moreover, greater dietary vitamin C intakes before BC diagnosis have also been found to diminish BC death cases in a prospective cohort study [31]. On the other hand, a significant increase in the survival and recovery of BC was also observed through consuming vitamin C supplements in the first 6 months after BC diagnosis in a four-year longitudinal study [32]. Potassium has also been shown to be able to potentiate the antitumor effects of vitamin C in an in-vitro investigation [33]. the preventive effects of dietary fiber on the risk of breast cancer in both pre and post-menopause women have also been confirmed in a meta-analysis of 17 prospective longitudinal studies [34]. Enhancing the dietary intake of fruits and vegetables, which are rich in fiber, vitamin C, and potassium has also been reported to reduce the odds of breast cancer [35]. The risk of breast cancer has also been stated to be decreased by consuming fruits and vegetables in a meta-analysis of 15 observational studies [36].
Several mechanisms might explain the relationship between the third nutrient pattern and the odds of breast cancer. First, vitamin C might be able to suppress hydrogen peroxide (H2O2) secretion which is an important factor in cancer cell proliferation [37,38,39]. Dietary fiber, on the other hand, might have a decreasing function in estrogen enterohepatic circulation [40]. Fiber fermentation might lead to the production of short-chain fatty acids (SCFA) [41] with anti-inflammatory effects [42]. It has also been claimed that a combination of soluble and insoluble dietary fibers might play a protective role in breast tumorigenesis in rats [43].
The current study has some limitations. First, as a case–control study, selection and recall biases might not be avoidable. We tried to decrease these biases by choosing a control group among the patients’ families with almost similar properties to the case group. Collecting the patients who have been referred to the hospital might also help to reduce selection biases in the case group. Second, using FFQ to assess the individuals’ intake might lead to some amounts of misclassification. Moreover, it might not be possible to define the causality due to the case–control design. This study has also some strengths. For example, applying validated FFQs along with twelve dietary recalls might limit the possible recall biases of case–control studies. Moreover, a wide age range of the participants (19 to 80) can increase our results’ validity. Finally, assessing the relationship between nutrient patterns and the risk of breast cancer in both pre and post-menopausal situations separately has provided the possibility to reduce the effects of this status on our results.
In conclusion, we investigated that the third nutrient pattern, which was rich in dietary fiber, potassium, and vitamin C, and was characterized as the “vegetables” nutrient pattern, might reduce the risk of breast cancer both in general and pre-menopausal women.
Availability of data and materials
Data from this study are available on a reasonable request by the corresponding author.
References
Arnold M, Morgan E, Rumgay H, Mafra A, Singh D, Laversanne M, et al. Current and future burden of breast cancer: Global statistics for 2020 and 2040. The Breast. 2022;66:15–23.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49.
Taghavi A, Fazeli Z, Vahedi M, Baghestani AR, Pourhoseingholi A, Barzegar F, et al. Increased trend of breast cancer mortality in Iran. Asian Pac J Cancer Prev. 2012;13(1):367–70.
AlizadehOtaghvar H, Hosseini M, Tizmaghz A, Shabestanipour G, Noori H. A review on metastatic breast cancer in Iran. Asian Pac J Trop Biomed. 2015;5(6):429–33.
Naderimagham S, Alipour S, Djalalinia S, Kasaeian A, Noori A, Rahimzadeh S, et al. National and sub-national burden of breast cancer in Iran; 1990–2013. Arch Iran Med. 2014;17(12):794–9.
Majeed W, Aslam B, Javed I, Khaliq T, Muhammad F, Ali A, et al. Breast cancer: major risk factors and recent developments in treatment. Asian Pac J Cancer Prev. 2014;15(8):3353–8.
Maas P, Barrdahl M, Joshi AD, Auer PL, Gaudet MM, Milne RL, et al. Breast cancer risk from modifiable and nonmodifiable risk factors among white women in the United States. JAMA Oncol. 2016;2(10):1295–302.
Mourouti N, Kontogianni MD, Papavagelis C, Panagiotakos DB. Diet and breast cancer: a systematic review. Int J Food Sci Nutr. 2015;66(1):1–42.
Kwan ML, Weltzien E, Kushi LH, Castillo A, Slattery ML, Caan BJ. Dietary patterns and breast cancer recurrence and survival among women with early-stage breast cancer. J Clin Oncol. 2009;27(6):919–26.
Turati F, Carioli G, Bravi F, Ferraroni M, Serraino D, Montella M, et al. Mediterranean diet and breast cancer risk. Nutrients. 2018;10(3):326–36.
Malmir H, Shayanfar M, Mohammad-Shirazi M, Tabibi H, Sharifi G, Esmaillzadeh A. Patterns of nutrients intakes in relation to glioma: A case-control study. Clin Nutr. 2019;38(3):1406–13.
Zhang D, Xu P, Li Y, Wei B, Yang S, Zheng Y, et al. Association of vitamin C intake with breast cancer risk and mortality: a meta-analysis of observational studies. Aging. 2020;12(18):18415–35.
Nagel G, Linseisen J, van Gils CH, Peeters PH, Boutron-Ruault MC, Clavel-Chapelon F, et al. Dietary beta-carotene, vitamin C and E intake and breast cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). Breast Cancer Res Treat. 2010;119(3):753–65.
Johnson RK, Vanderlinden LA, DeFelice BC, Uusitalo U, Seifert J, Fan S, et al. Metabolomics-related nutrient patterns at seroconversion and risk of progression to type 1 diabetes. Pediatr Diabetes. 2020;21(7):1202–9.
Gnagnarella P, Maisonneuve P, Bellomi M, Rampinelli C, Bertolotti R, Spaggiari L, et al. Nutrient intake and nutrient patterns and risk of lung cancer among heavy smokers: results from the COSMOS screening study with annual low-dose CT. Eur J Epidemiol. 2013;28(6):503–11.
JafariNasab S, Ghanavati M, Bahrami A, Rafiee P, Sadeghi A, Clark CCT, et al. Dietary nutrient patterns and the risk of colorectal cancer and colorectal adenomas: a case-control study. Eur J Cancer Prev. 2021;30(1):46–52.
Tayyem RF, Mahmoud RI, Shareef MH, Marei LS. Nutrient intake patterns and breast cancer risk among Jordanian women: a case-control study. Epidemiol Health. 2019;41:e2019010.
Fereidani SS, Eini-Zinab H, Heidari Z, Jalali S, Sedaghat F, Rashidkhani B. Nutrient Patterns and Risk of Breast Cancer among Iranian Women: a Case- Control Study. Asian Pac J Cancer Prev. 2018;19(9):2619–24.
Assi N, Moskal A, Slimani N, Viallon V, Chajes V, Freisling H, et al. A treelet transform analysis to relate nutrient patterns to the risk of hormonal receptor-defined breast cancer in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2016;19(2):242–54.
Edefonti V, Decarli A, La Vecchia C, Bosetti C, Randi G, Franceschi S, et al. Nutrient dietary patterns and the risk of breast and ovarian cancers. Int J Cancer. 2008;122(3):609–13.
Ronco AL, de Stefani E, Aune D, Boffetta P, Deneo-Pellegrini H, Acosta G, et al. Nutrient patterns and risk of breast cancer in Uruguay. Asian Pac J Cancer Prev. 2010;11(2):519–24.
Vahid F, Hatami M, Sadeghi M, Ameri F, Faghfoori Z, Davoodi SH. The association between the Index of Nutritional Quality (INQ) and breast cancer and the evaluation of nutrient intake of breast cancer patients: A case-control study. Nutrition (Burbank, Los Angeles County, Calif). 2018;45:11–6.
Mirmiran P, Esfahani FH, Mehrabi Y, Hedayati M, Azizi F. Reliability and relative validity of an FFQ for nutrients in the Tehran lipid and glucose study. Public Health Nutr. 2010;13(5):654–62.
Esfahani FH, Asghari G, Mirmiran P, Azizi F. Reproducibility and relative validity of food group intake in a food frequency questionnaire developed for the Tehran Lipid and Glucose Study. J Epidemiol. 2010;20(2):150–8.
Ghaffarpour M, Houshiar-Rad A, Kianfar H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran: Nashre Olume Keshavarzy. 1999;7(213):42–58.
Haytowitz D, Lemar L, Pehrsson P, Exler J, Patterson K, Thomas R, et al. USDA national nutrient database for standard reference, release 24. US Department of Agriculture: Washington, DC, USA. 2011.
WHO. Global physical activity questionnaire (GPAQ) analysis guide. Geneva; 2012. p. 1–22.
Kim J, Mueller CW. Factor analysis - statistical methods and practical issues. Office of justice programs. United States of America; 1978. p. 88.
Tabrizi R, Moosazadeh M, Akbari M, Dabbaghmanesh MH, Mohamadkhani M, Asemi Z, et al. High prevalence of vitamin D deficiency among Iranian population: a systematic review and meta-analysis. Iran J Med Sci. 2018;43(2):125–39.
Mozafarinia M, Sasanfar B, Toorang F, Salehi-Abargouei A, Zendehdel K. Association between dietary fat and fat subtypes with the risk of breast cancer in an Iranian population: a case-control study. Lipids Health Dis. 2021;20:1–11.
Harris HR, Bergkvist L, Wolk A. Vitamin C intake and breast cancer mortality in a cohort of Swedish women. Br J Cancer. 2013;109(1):257–64.
Nechuta S, Lu W, Chen Z, Zheng Y, Gu K, Cai H, et al. Vitamin supplement use during breast cancer treatment and survival: a prospective cohort study. Cancer Epidemiol Biomarkers Prev. 2011;20(2):262–71.
Frajese GV, Benvenuto M, Fantini M, Ambrosin E, Sacchetti P, Masuelli L, et al. Potassium increases the antitumor effects of ascorbic acid in breast cancer cell lines in vitro. Oncol Lett. 2016;11(6):4224–34.
Farvid MS, Spence ND, Holmes MD, Barnett JB. Fiber consumption and breast cancer incidence: A systematic review and meta-analysis of prospective studies. Cancer. 2020;126(13):3061–75.
Marzbani B, Nazari J, Najafi F, Marzbani B, Shahabadi S, Amini M, et al. Dietary patterns, nutrition, and risk of breast cancer: a case-control study in the west of Iran. Epidemiol Health. 2019;41:e2019003.
Aune D, Chan DS, Vieira AR, Rosenblatt DA, Vieira R, Greenwood DC, et al. Fruits, vegetables and breast cancer risk: a systematic review and meta-analysis of prospective studies. Breast Cancer Res Treat. 2012;134(2):479–93.
Loo G. Redox-sensitive mechanisms of phytochemical-mediated inhibition of cancer cell proliferation (review). J Nutr Biochem. 2003;14(2):64–73.
Willcox JK, Ash SL, Catignani GL. Antioxidants and prevention of chronic disease. Crit Rev Food Sci Nutr. 2004;44(4):275–95.
Frei B. Reactive oxygen species and antioxidant vitamins: mechanisms of action. Am J Med. 1994;97(3a):5S-13S; discussion 22S-8S.
Aubertin-Leheudre M, Gorbach S, Woods M, Dwyer JT, Goldin B, Adlercreutz H. Fat/fiber intakes and sex hormones in healthy premenopausal women in USA. J Steroid Biochem Mol Biol. 2008;112(1–3):32–9.
Topping DL, Clifton PM. Short-chain fatty acids and human colonic function: roles of resistant starch and nonstarch polysaccharides. Physiol Rev. 2001;81(3):1031–64.
Manning PJ, Sutherland WH, McGrath MM, de Jong SA, Walker RJ, Williams MJ. Postprandial cytokine concentrations and meal composition in obese and lean women. Obesity (Silver Spring, Md). 2008;16(9):2046–52.
Cohen LA, Zhao Z, Zang EA, Wynn TT, Simi B, Rivenson A. Wheat bran and psyllium diets: effects on N-methylnitrosourea-induced mammary tumorigenesis in F344 rats. J Natl Cancer Inst. 1996;88(13):899–907.
Acknowledgements
Our Sincere thanks go to all participants.
Funding
This study was supported by a fund from the cancer research institute at Tehran University of Medical Science (no. 93–03-51–27113).
Author information
Authors and Affiliations
Contributions
FD developed the initial draft. BS and FT participated in the study design and analysis. FD implemented comments and suggestions of the co-authors. KZ and ASA contributed to conception, design, and data analysis. All authors reviewed the final version of the manuscript. KZ and AS supervised the study.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects/patients were approved by the Ethics Committee of Cancer Research Center, Tehran University of Medical Sciences (no. 93–03-51–27113). Written informed consent was obtained from all subjects.
Consent for publication
No data has been published by the names of the participants.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Dehghani, F., Sasanfar, B., Toorang, F. et al. Association between empirically derived nutrient patterns and breast cancer: a case–control study in a Middle Eastern country. BMC Nutr 10, 124 (2024). https://doi.org/10.1186/s40795-024-00934-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40795-024-00934-x