
Abstract
Background
Rice protein is proved to have hypocholesterolemic and anti-atherosclerotic effects, and a few experimental studies showed its renoprotective effects, using animal diabetic models. However, no clinical studies have investigated its benefits for human health. We aimed to clarify how the intake of rice endosperm protein affects markers correlating to lipid dysfunction in human.
Methods
We recruited 18 male volunteers, 26–64 years of age, with risk factors for metabolic syndrome and allocated randomly into two groups. Half of them were administered test food containing rice endosperm protein and other half were administered control food containing sodium caseinate for 4 weeks. The dose of supplemental protein was 10 g/day. After medical examinations, the study foods were switched and the intervention was continued for another 4 weeks. Lipid metabolism markers were evaluated as primary outcome measures. Cross-over analysis was performed for 18 subjects using physical and clinical values measured before and after each intervention period.
Results
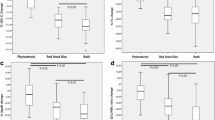
The serum high-density lipoprotein cholesterol (HDL-C) level was increased at 0.08 mmol/L [interquartile range (IQR) from −0.05 to 0.19 mmol/L] during the period when rice endosperm protein was administered (the rice endosperm protein period), whereas it was decreased at −0.04 mmol/L [IQR from −0.13 to 0.05 mmol/L] during the period when casein was administered (the casein period). Treatment effect was significant with P = 0.047. Changes in total cholesterol, low-density lipoprotein cholesterol and triglycerides were not different between treatments. Among the secondary outcome measures, decrease in serum uric acid (UA) during the rice endosperm protein period [−24 μmol/L (IQR from −39 to −6 μmol/L)] was greater than that during the casein period [0 (IQR from −6 to 13 μmol/L)] with a significant treatment effect (P = 0.030).
Conclusion
Supplemental intake of rice endosperm protein may elevate serum HDL-C level and lower serum UA level in male subjects with risk factors for metabolic syndrome.
Trial registration
Clinical Trials Registry: UMIN000008923.
Similar content being viewed by others


Background
Lifestyle habits, such as unhealthy eating, cause or exacerbate health problems, although predisposition to life style related diseases may be determined by genetic factors. A recent survey in Japan estimated that approximately 10.7 million patients suffer from the metabolic syndrome, and that 9.4 million people are at the risk of developing it. The prevalence of the metabolic syndrome is particularly striking in adult men aged 40–74 years. In this population, one in two men is either currently suffering from or is at the risk of developing metabolic syndrome [1]. Individuals suffering from metabolic syndrome have a 5-fold increased risk of developing diabetes, and those with diabetes have a 2- to 5-fold increased risk of developing cardiovascular disease [2]. Therefore, measures taken to reduce the risk of developing metabolic syndrome, such as the improvement of dietary habits, are considered to be important. The increased prevalence of metabolic syndrome and consequent higher risk for cardiovascular disease are thought to be due to obesity and insulin resistance influenced by lifestyle and western dietary pattern, such as increased energy, sugar, saturated fatty acid, less fiber, less physical activity, etc. Although rice remains the major nutrient source in Japanese diet, its consumption was halved between 2012 and peaked in 1962 [3]. The reduction in rice consumption in Japan is thought to be due at least a part to the westernization of dietary habit. However, Eshak et al. demonstrated the negative correlation between the amount of rice intake and the risk of cardiovascular disease in Japanese men [4]. Similarly, white rice intake in the way it is consumed in Southern Spain is reported to be negatively associated to the 6 years incidence of type 2 diabetes [5]. These findings suggest the beneficial effect of rice consumption under certain circumstances.
In animal trials, we and another group have shown that purified rice endosperm protein have hypocholesterolemic effects [6, 7]. Similarly, Tong et al. demonstrated that α-globulin, a component of rice endosperm protein, decreased serum cholesterol concentrations in rats fed a hypercholesterolemic diet and ameliorated atherosclerotic lesions in apolipoprotein (Apo) E-deficient mice [8]. These findings suggest the beneficial effects of rice endosperm protein intake in ameliorating lipid dysfunction such as decreasing total cholesterol (TC), low density lipoprotein cholesterol (LDL-C) and triglycerides (TG). Moreover, we reported that rice endosperm protein minimized the progression of diabetic nephropathy in Goto-Kakizaki rats on high-sucrose diet [9]. These findings encouraged us to clarify the effects of endosperm protein from white rice in humans with respect to risks for metabolic syndrome and cardiovascular disease.
In addition to rice protein, soy protein is another source of vegetable protein. Many studies have reported the health benefits of soy protein. The efficacy of soy protein intake on lowering the risk of coronary heart disease has been accepted by the US Food and Drug Administration [10]. Consumption of soy protein significantly lowers cardiovascular risks by affecting fasting plasma glucose, TC, LDL-C, serum TG, and C-reactive protein [11], and soy protein supplementation is thought to be an effective management strategy for metabolic and vascular diseases [12]. However, much less is known regarding the health benefits of rice protein. Using our method for the preparation of food grade purified rice endosperm protein from white rice, we aim to perform exploratory study to clarify how the intake of rice endosperm protein affects markers correlating to lipid dysfunction in humans as the primary clinical outcomes and those relating to metabolic syndrome risk factors. Our study is the first human trial of rice endosperm protein administration, which enrolled subjects with risk factors for metabolic syndrome.
Methods
Subjects
Adults were recruited among working people in Co-op Chemical Co., Ltd., Niigata, Japan who have the annual medical checkup based on the checked-up records obtained in April 2012. The study included subjects with at least two of the following criteria for the clinical diagnosis of metabolic syndrome according to the modified National Cholesterol Education Program’s Adult Treatment Panel III (NCEP): (i) visceral fat obesity defined as waist circumference ≥ 90 cm, (ii) serum TG ≥ 1.7 mmol/L or on drug treatment for elevated TG, (iii) serum high-density lipoprotein cholesterol (HDL-C) < 1.03 mmol/L or on drug treatment for reduced HDL-C, (iv) systolic-blood pressure (SBP) ≥ 130 mmHg, diastolic-blood pressure (DBP) ≥ 85 mmHg, or use of antihypertensive drugs, and (v) fasting plasma glucose ≥ 5.6 mmol/L or on drug treatment for elevated glucose [13]. Practically, among these criteria, “on drug treatment for reduced HDL-C” was not applicable for this study because such treatment is not permitted in the Japanese medical insurance system.
The exclusion criteria were as follows: 1) current treatment for diabetes mellitus, 2) severe heart, renal or liver disease, 3) perioperative stages, or severe infection or serious injury, 4) food allergies, and 5) those not eligible for the study due to any medical reason evaluated by a physician.
Study design and enrollment
The prospective, randomized, single blind, crossover study took place from September to December 2012. The subjects approved to participate in the trial were enrolled. Subjects were alternately assigned by the chief attending doctor according to the order of enrollment to any of the rice endosperm protein first group or the casein first group, respectively. Therefore, participants were blinded while chief attending doctor was not. During the pre-observation period, the subjects underwent physical examinations, including waist circumference, body mass index (BMI), SBP, DBP, and laboratory tests. Blood samples were obtained by venipuncture, reserved in collection tubes and centrifuged immediately at 1,700 × g for 15 min at 4 °C to recover serums. Biochemical analyses were performed by SRL, Inc. (Tokyo, Japan), a certified laboratory by the College of American Pathologists, an authoritative external organization, and the Japan Accreditation Board for Conformity Assessment started (ISO15189), an international standards for clinical testing laboratories. HDL-C levels were measured using the direct assay (Sekisui medical Inc., Japan). Uric acid (UA) levels were assayed by enzymatic methods (Sekisui medical Inc., Japan). Monocyte chemoattractant protein-1 (MCP-1) levels were measured using the ELISA assay (R&D SYSTEMS, Minneapolis). The mean coefficient of variation of HDL-C, UA, and MCP-1 measurements were inquired to be less than 5 %, less than 3 %, and 4.6–7.8 %, respectively. Waist circumference was measured at the umbilical level in the standing position after light expiration using a measuring tape, and BMI was calculated as weight divided by height squared. Blood pressure was measured once with an automatic sphygmomanometer while the patient was seated and after 5 min of rest. These examinations were performed in fasting condition.
Intervention
The test or control food, after being suspended in hot or cold water, was given twice a day to the subjects. The daily amount of supplemental protein to usual meal was calculated to be 10 g in total. No dietary habit restrictions were instructed during the trial period. The enrolled subjects were instructed to not change their lifestyle or physical activities during the study. After the second medical check at the end of week 4, the intervention foods were switched after 3 days of washout, and the test was pursued for another 4 weeks. Namely, the rice endosperm protein was administered for the rice endosperm protein first group during the first 4 weeks (period 1), and for the casein first group during the last 4 weeks (period 2), respectively (the rice endosperm protein period), whereas casein was administered for these groups during periods 2 and 1, respectively (the casein period).
Follow-up
Consumption of intervention food and occurrence of adverse events were examined by attending doctors based on the individuals’ study diary. Lifestyle and medicating situation of each subject was checked using a self-reporting sheet. Dietary habits were assessed using a validated, brief-type self-administered, diet history questionnaires (BDHQ), at the beginning and end of the interventional study [14]. Details of the BDHQ’s structure, calculation method of dietary intake, and validity for commonly studied macronutrients intake have been published [15]. Although the reliability of absolute values of energy intake has not been validated, we described the statistics of energy intake along with those of macronutrients to warrant that dietary habits of the subjects were not significantly altered during the study period. Subjects were followed-up for a month after the final medical investigation at the end of week 8, and the test was completed at the end of December 2012.
Preparation of test and control foods
Rice endosperm protein was extracted from rice flour of regular Japonica rice, Koshihikari by the alkaline extraction method described by Kumagai et al. [16]. The production was performed in a test plant set in Kameda Seika Co. Ltd. (Niigata, Japan) and was expanded to a 100-times larger scale than that described, and the protein was heated at 80 °C for 30 min before lyophilization. The rice endosperm protein powder with a 90.5 % protein content (calculated from the nitrogen content using a protein/nitrogen coefficient as 5.95) and Sodium Caseinate CW® (Nippon Shinyaku, Kyoto, Japan, 88.7 % protein content) were used as protein sources for test food and control food, respectively. Compositions of these dietary protein materials are summarized in Table 1. Their typical amino acid compositions quoted from Kubota et al. [9] are also shown in Table 1. Dextrin MAX 1000® was obtained from Matsutani Chemical Industry, Itami, Japan, and SK SWEET Z-3-15® (glucosylated stevia sweetener) was purchased from Nippon paper industries, Tokyo, Japan. The composition of the intervention food is shown in Table 2. These intervention foods were almost the same powder configurations, colors, tastes, and smells. They were packed in an aluminum bag and heat sealed.
Evaluation of outcome
Lipid metabolism markers such as serum TC, HDL-C, subfractions of HDL-C (HDL2 and HDL3), ApoA1, ApoA2, ApoB, ApoC2, ApoC3, ApoE, oxidized LDL (ox-LDL), remnant-like lipoprotein cholesterol (RLP-C), LDL-C, and TG were evaluated as primary outcome measures. Urea nitrogen (UN), UA, creatinine (CRE), insulin, adiponectin, glucose, high sensitive C-reactive protein (hsCRP), and MCP-1 of serum samples were measured as secondary outcomes. Fundamental values of hepatic and uric markers were also evaluated. These measurements were performed before and after each 4-week intervention period.
Evaluation of safety
Tolerability and safety were evaluated on the basis of the incidence and severity of the study of food-related adverse events experienced throughout the study. All adverse events occurring in both groups were analyzed for their frequency, severity, and association with intervention and efficacy outcome.
Statistics
Because many outcome measures were not normally distributed when the distribution was tested using the Kolmogolov–Smirnov test, we applied nonparametric analyses except for descriptive statistics for which values are expressed as means ± standard deviation (SD) for convenience. Change in values over time was tested using the Wilcoxon signed-rank test; change values were expressed in median [inter-quartile range]. Crossover analyses for treatment effect and treatment-period interaction were performed in accordance with the methods described in the textbook of Armitage and Berry [17]. Briefly, an absolute change in each outcome measure was calculated for each individual for each of period 1 and period 2 as d1 and d2, respectively. Then, the treatment effect was tested by comparing (d1 – d2) between the rice endosperm protein first and the casein first groups, and the treatment-period interaction was tested by comparing (d1 + d2) between the two groups. Although Student’s t-test is recommended to analyze these effects in the textbook, we applied Mann–Whitney U-test because we needed to consider non-parametric statistical procedures as mentioned above. Statistical analysis was performed using a statistical add-in software of Excel (Statcel 3, OMS Publishing, Saitama, Japan) for MS Excel (Microsoft, Redmond, WA, U.S.A.). Two-tailed P < 0.05 was regarded as statistically significant and 0.05 ≤ P < 0.1 was considered to be borderline level of statistical significance.
Results
Enrolled subjects and intervention
Twenty-four male subjects satisfying the inclusion criteria approved to be enrolled. No female subjects approved to participate in our study, although we wanted to recruit both men and women. Two subjects with extremely high serum TG levels (>9 mmol/L) were precluded. During the intervention, 2 subjects had changed their lifestyle drastically, i.e., transferred from shift work to office clerk work. Two subjects were found to have violated the instructions. Consequently, the analysis was conducted for the 18 remaining subjects as shown in Fig. 1. Eight subjects on a statin (HMG-CoA reductase inhibitor) for their elevated cholesterol and continued with the medication throughout the study.

Flow diagram of subjects
Characteristics of subjects
Baseline characteristics of the 18 subjects were as follows, age, 49.3 ± 10.6; height, 171.4 ± 6.6; body weight (BW), 74.8 ± 11.2; BMI, 25.3 ± 2.2; and waist circumference, 91.4 ± 6.6. Five out of 18 subjects were diagnosed with metabolic syndrome. Table 3 shows the dietary characteristics of the 18 subjects. No significant differences in dietary energy intake, percent energy of macronutrients, and ratio of plant-to-animal protein balance were observed between pre- and post-intervention values assessed using BDHQ. During the 8-week intervention and follow-up period, no adverse events were detected in any subjects enrolled.
Effects of rice endosperm protein intake
Effects of rice endosperm protein intake on physical measurements and clinical parameters were compared with those of casein intake. Results are shown in Table 4. Treatment-period interactions were checked and were not detected for any variables (data not shown).
Among the parameters related to the criteria for the clinical diagnosis of metabolic syndrome, no significant treatment effect was observed for waist circumference, SBP, DBP, glucose, and TG. On the other hand, HDL-C was influenced by the type of supplemental protein. HDL-C levels significantly increased during the rice endosperm protein period whereas it did not during the casein period; and this increase was considerably greater with a statistically significant treatment effect (P = 0.047). In contrast, no significant differences were observed in TC, LDL-C, HDL2, HDL3, ApoA1, ApoA2, ApoB, ApoC2, ApoC3, ApoE, ox-LDL, or RLP-C.
Serum UA was significantly reduced during the rice endosperm protein period, while this level did not change during the casein period. Presence of treatment effect was also confirmed by crossover analysis with P = 0.030. Slight increase in CRE, and slight decrease in ox-LDL were seen in both groups and these changes were statistically significant in the casein period. However, no significant treatment effects were found at all (Table 4). Serum MCP-1 levels were significantly reduced during the rice endosperm protein period (P < 0.01) while not during the casein period: the treatment effect was not significant but reached to the borderline significance level (P = 0.058). DBP was considerably increased during the intervention period irrespective of the type of supplemental protein. However, no significant treatment effect was observed. Hepatic and urinary parameters were also analyzed, but no significant changes were observed (data not shown).
Discussion
We conducted the first human trial to clarify the beneficial effect of rice endosperm protein intake in adult male subjects with risk factors for metabolic syndrome. Some animal experiments have been performed and the effect of rice endosperm protein in ameliorating lipid profile in humans was expected. Consequently biomarkers related to lipid metabolism were evaluated as main outcomes. The present study was performed as an exploratory one, consequently, variables somewhat different between the rice endosperm protein and the casein periods were also discussed even without statistical significance.
The administration of proteins (rice endosperm protein or casein) at a dose of 10 g protein/day during four consecutive weeks did not affect TG, LDL-C, HDL2, HDL3, ApoA1, ApoA2, ApoB, ApoC2, ApoC3, ApoE, ox-LDL, or RLP-C. However, HDL-C was significantly influenced by the type of ingested protein, particularly rice endosperm protein significantly increased HDL-C during the intervention (Table 4). Diet mediated increment of HDL-C is summarized in a review of Kapur et al. [18]. However, the effects of dietary proteins and a correlation with HDL-C levels are poorly investigated. Egg white is reported to elevate HDL-C in rodents [19] and humans [20]. Oda [21] mentioned in his review that sulfur-containing amino acids, especially methionine, were responsible for the increase in HDL-C and ApoA1. Rice endosperm protein is known to contain a higher level of sulfur-containing amino acids than casein and soy protein [7], at a level comparable to that of egg white. The human trial reporting the elevation of HDL-C levels with the administration of egg white [20] used a protein supply of 23 g daily, an amount of protein much greater than that in our study. However, elevation in HDL-C levels by rice endosperm protein intake might, at least in part, be explained by the stimulation of APOA1 by sulfur-containing amino acids in rice endosperm protein [21], although no significant differences other than HDL-C were observed.
We previously reported studies conducted in normal adult Wistar rats fed a normal diet, growing rats fed a cholesterol-enriched diet [7], or non-obese diabetic rats fed a high-sucrose diet showing a reduction of TC [9] by rice endosperm protein administration. The phenotypes of outcome of rice endosperm protein intake in humans and rodents were different in terms of changing lipid metabolism. Low levels of HDL-C are reported to increase the risk of coronary events in epidemiological [22] and clinical studies [23]. However, drugs increasing HDL-C levels such as fibrates, niacin, and cholesteryl ester transfer protein inhibitor have failed to reduce the risk of major cardiovascular events [24–28]. Further studies are needed to test whether increased ApoA1 and HDL-C by rice endosperm protein demonstrate cardiovascular protective properties.
Recent studies demonstrated that hyperuricemia is linked not only to gout but also to other important disorders including hypertension, chronic kidney disease, cardiovascular disease, and metabolic syndrome [29]. Prior to considering a drug treatment for symptoms, adopting a progressive life style change such as healthier eating habits is considered important for the prevention and treatment of hyperuricemia [30]. Along with such a trend, new food ingredients with hypouricemic effect are being researched. The methanol extract of a fruit [31], a flavonoid from a traditional herb [32], and onion [33] are demonstrated as hypouricemic substances by animal studies. The hypouricemic effect of fermented barley extract was shown in a human study reported by Hokazono et al. [34]. However, information on such effect in food and foodstuff remains limited. We have demonstrated in the present trial that rice endosperm protein intake significantly decreased serum UA levels compared with serum UA levels associated with casein intake. While ingested rice endosperm protein reduces serum UA, the responsible protein molecule remains to be identified and is currently investigated.
Intake of rice endosperm protein was found in the present study to decrease significantly the serum MCP-1 level, while casein intake did not change it. MCP-1, a secreted protein specifically attracting blood monocytes and tissue macrophages, is known to correlate with inflammation, and the increased level of serum MCP-1 is associated with markers of metabolic syndrome, obesity, insulin resistance, type 2 diabetes, hypertension, and hyperlipidemia [35]. Soy protein consumption is reported to down-regulate diet induced inflammation, i.e., dietary supplementation of soy protein significantly reduced plasma MCP-1, as well as insulin and TNF-α, in high fat diet-fed mice [36], although the isolate used was reported to contain isoflavones as well. Hence, synthetic peptides derived putatively from soy protein were found to inhibit MCP-1 expression when they were added to LPS-induced human vascular endothelial cells in vitro [37]. This suggests that such inhibition is mediated by peptides generated in vivo by protease/peptidases in the gut. Similarly, rice endosperm protein could possibly reduce MCP-1 levels in vivo in the same way as soy protein does. However, intergroup difference in MCP-1 was only tendency and further accumulation of evidence is required.
The tolerability of additional proteins in usual meals should be discussed. In the present study, the amount of rice endosperm protein added was 10 g/day, a dose much lower than the dose associated with harmful effects advocated by Pedersen et al. [38] and the 23 g of egg protein/day used in the study conducted by Asato et al. [20]. Recent clinical trials with soy protein were performed using doses of 15–56 g of protein/day [39–42]; however to date, no clinical reports have investigated rice protein intake. Consequently, in the present study, we used a smaller amount of protein, i.e., 10 g/day, to avoid potential health hazards. Based on the BDHQ results, the mean dietary protein intake was 1.05–1.11 g/kg BW/day (Table 3). When the additional protein intake from the intervention is taken into account, the resulting protein intake was 1.18–1.24 g/kg BW/day. The dose of 10 g/day of rice endosperm protein was found to be safe because no adverse event related to the intake of study foods was observed throughout the study.
A limitation of this study is that it included only men with a relatively wide range in age who had a risk of developing metabolic syndrome. In addition, the study included only 18 subjects and the intervention lasted only for 4 weeks. Although including a larger number of subjects that included women would have provided more robust results, due to the limitation of time and resources, only men were enrolled. Furthermore, no significant differences in SBP and DBP were observed between groups. DBP in both groups had a tendency to increase after 4 weeks, probably because of the environmental conditions. Indeed, the final medical investigation at week 8 was performed on a very cold day in December. Another limitation is the considerable short washout period of 3 days. Although no treatment-period interaction was detected as described before, carryover effects cannot be excluded. Finally, we assessed many outcome measures simultaneously since this study was as an exploratory one. Consequently, some statistical significance could have been observed by chance (type 1 error) and these results need to be further validated. The future validation studies should take into account the present obtained data for planning purposes. Despite these limitations, the present study provides an important insight into the beneficial effects of rice endosperm protein and a basis for future studies to examine long-term effects in a larger number of participants including both sexes.
Conclusion
Rice endosperm protein intake may increase HDL-C as well as reduce serum UA level in adult male subjects with risk factors for metabolic syndrome. These findings would suggest the beneficial effect of rice endosperm protein intake in prevention of incidence or suppression of deterioration of metabolic syndrome, and consequent reduction of risk for cardiovascular events, although further detailed study is required.
Data availability
All relevant data is contained in the manuscript.
Ethics
The study protocol was approved by the local ethics committee held in the School of Medicine, Niigata University, and was conducted in accordance with the principles of the amended Declaration of Helsinki, and Ethical Guideline for Epidemiological Research. Written informed consent was obtained from all participants prior to enrollment in the study.
Abbreviations
- Apo:
-
apolipoprotein
- BDHQ:
-
brief-type self-administered diet history questionnaire
- BMI:
-
body mass index
- BW:
-
body weight
- CRE:
-
creatinine
- DBP:
-
diastolic-blood pressure
- HDL-C:
-
high-density lipoprotein cholesterol
- hsCRP:
-
high sensitive C-reactive protein
- LDL-C:
-
low-density lipoprotein cholesterol
- MCP-1:
-
monocyte chemoattractant protein-1
- ox-LDL:
-
oxidized LDL
- RLP-C:
-
remnant-like lipoprotein cholesterol
- SBP:
-
systolic-blood pressure
- SD:
-
standard deviation
- TC:
-
total cholesterol
- TG:
-
triglyceride
- UA:
-
uric acid
- UN:
-
urea nitrogen
References
Status of patients and those having a high risk of contracting metabolic syndrome (visceral fat syndrome). In: Annual Health, Labour and Welfare Report 2009-2010. Ministry of Health, Labor and Welfare of Japan. http://www.mhlw.go.jp/english/wp/wp-hw4/dl/health_and_medical_services/P68.pdf. Accessed 3 Aug 2015.
Stern MP, Williams K, González-Villalpando C, Hunt KJ, Haffner SM. Does the metabolic syndrome improve identification of individuals at risk of type 2 diabetes and/or cardiovascular disease? Diabetes Care. 2004;27:2676–81.
Boosting demand for domestic agricultural products and promoting agricultural production based on demand. In: Annual report on food, agriculture and rural areas in Japan FY 2008 (Summary). Ministry of Agriculture, Forestry and Fisheries of Japan. www.maff.go.jp/e/annual_report/2008/pdf/e_1-2.pdf. Accessed 3 Oct 2015.
Eshak ES, Iso H, Date C, Yamagishi K, Kikuchi S, Watanabe Y, et al. Rice intake is associated with reduced risk of mortality from cardiovascular disease in Japanese men but not women. J Nutr. 2011;141:595–602. doi:10.3945/jn.110.132167.
Soriguer F, Colomo N, Olveira G, García-Fuentes E, Esteva I, Ruiz de Adana MS, et al. White rice consumption and risk of type 2 diabetes. Clin Nutr. 2013;32:481–4. doi:10.1016/j.clnu.2012.11.008.
Morita T, Oh-hashi A, Kasaoka S, Ikai M, Kiriyama S. Rice protein isolates produced by the two different methods lower serum cholesterol concentration in rats compared with casein. J Sci Food Agric. 1996;71:415–24. doi:10.1002/(SICI)1097-0010. (199608)71:4 < 415::AID-JSFA599 > 3.0.CO;2-6.
Yang L, Kumagai T, Kawamura H, Watanabe T, Kubota M, Fujimura S, et al. Effects of rice protein from two cultivars, Koshihikari and Shunyo, on cholesterol and triglyceride metabolism in growing and adult rats. Biosci Biotech Biochem. 2007;71:694–703.
Tong LT, Fujimoto Y, Shimizu N, Tsukino M, Akasaka T, Kato Y, et al. Rice α-globulin decreases serum cholesterol concentrations in rats fed a hypercholesterolemic diet and ameliorates atherosclerotic lesions in apolipoprotein E-deficient mice. Food Chem. 2012;132:194–200. doi:10.1016/j.foodchem.2011.10.056.
Kubota M, Watanabe R, Kabasawa H, Iino N, Saito A, Kumagai T, et al. Rice protein ameliorates the progression of diabetic nephropathy in Goto-Kakizaki rats with high-sucrose feeding. Br J Nutr. 2013;110:1211–9. doi:10.1017/S0007114513000354.
Food labeling: health claims; soy protein and coronary heart disease. Fed Regist. 1999;64:57700-33.
Azadbakht L, Atabak S, Esmailizadeh A. Soy protein intake, cardiorenal indices, and C-reactive protein in type 2 diabetes with nephropathy: a longitudinal randomized clinical trial. Diabetes Care. 2008;31:648–54. doi:10.2337/dc07-2065.
Matsuzawa Y. Adiponectin: Identification, physiology and clinical relevance in metabolic and vascular disease. Atheroscler Suppl. 2005;6:7–14.
Hata J, Doi Y, Ninomiya T, Tanizaki Y, Yonemoto K, Fukuhara M, et al. The effect of metabolic syndrome defined by various criteria on the development of ischemic stroke subtypes in a general Japanese population. Atherosclerosis. 2010;210:249–55. doi:10.1016/j.atherosclerosis.2009.10.044.
Kobayashi S, Murakami K, Sasaki S, Okubo H, Hirota N, Notsu A, et al. Comparison of relative validity of food group intakes estimated by comprehensive and brief-type self-administered diet history questionnaires against 16 d dietary records in Japanese adults. Public Health Nutr. 2011;14:1200–11. doi:10.1017/S1368980011000504.
Kobayashi S, Asakura K, Suga H, Sasaki S, Three-generation Study of Women on Diets and Health Study Group. High protein intake is associated with low prevalence of frailty among old Japanese women: a multicenter cross-sectional study. Nutr J. 2013;12:164. doi:10.1186/1475-2891-12-164.
Kumagai T, Kawamura H, Fuse T, Watanabe T, Saito Y, Masumura T, et al. Production of rice protein by alkaline extraction improves its digestibility. J Nutr Sci Vitaminol. 2006;52:467–72.
Armitage P, Berry G. The simple crossover design. In: Statistical methods in medical research. 3rd ed. Cambridge: Blackwell Science; 1994. p. 245–8.
Kapur NK, Ashen D, Blumenthal RS. High density lipoprotein cholesterol: an evolving target of therapy in the management of cardiovascular disease. Vasc Health Risk Manag. 2008;4:39–57.
Yamamoto S, Kina T, Yamagata N, Kokubo T, Shinjo S, Asato L. Favorable effects of egg white protein on lipid metabolism in rats and mice. Nutr Res. 1993;13:1453–7. doi:10.1016/S0271-5317(05)80794-8.
Asato L, Wang MF, Chan YC, Yeh SH, Chung HM, Chung SY, et al. Effect of egg white on serum cholesterol concentration in young women. J Nutr Sci Vitaminol. 1996;42:87–96.
Oda H. Functions of sulfur-containing amino acids in lipid metabolism. J Nutr. 2006;136:1666S–9.
Collaboration ERF, Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302:1993–2000. doi:10.1001/jama.2009.1619.
Barter P, Gotto AM, LaRosa JC, Maroni J, Szarek M, Grundy SM, et al. HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events. N Engl J Med. 2007;357:1301–10.
Schwartz GG, Olsson AG, Abt M, Ballantyne CM, Barter PJ, Brumm J, et al. Effects of dalcetrapib in patients with a recent acute coronary syndrome. N Engl J Med. 2012;367:2089–99. doi:10.1056/NEJMoa1206797.
Barter PJ, Caulfield M, Eriksson M, Grundy SM, Kastelein JJ, Komajda M. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med. 2007;357:2109–22.
Investigators AIM-HIGH, Boden WE, Probstfield JL, Anderson T, Chaitman BR, Desvignes-Nickens P, et al. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011;365:2255–67. doi:10.1056/NEJMoa1107579.
ACCORD Study Group, Ginsberg HN, Elam MB, Lovato LC, Crouse 3rd JR, Leiter LA, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med. 2010;362:1563–74. doi:10.1056/NEJMoa1001282.
Keech A, Simes RJ, Barter P, Best J, Scott R, Taskinen MR, et al. Effects of long-term fenofibrate therapy on cardiovascular events in 9795 people with type 2 diabetes mellitus (the FIELD study): randomised controlled trial. Lancet. 2005;366:1849–61.
Alvarez-Lario B, Macarrón-Vicente J. Is there anything good in uric acid? QJM. 2011;104:1015–24. doi:10.1093/qjmed/hcr159.
Pillinger MH, Keenan RT. Update on the management of hyperuricemia and gout. Bull NYU Hosp Jt Dis. 2008;66:231–9.
Yi LT, Li J, Su DX, Dong JF, Li CF. Hypouricemic effect of the methanol extract from Prunus mume fruit in mice. Pharm Biol. 2012;50:1423–7. doi:10.3109/13880209.2012.683115.
Kondo M, Hirano Y, Nishio M, Furuya Y, Nakamura H, Watanabe T. Xanthine oxidase inhibitory activity and hypouricemic effect of aspalathin from unfermented rooibos. J Food Sci. 2013;78:H1935–9. doi:10.1111/1750-3841.12304.
Haidari F, Rashidi MR, Keshavarz SA, Mahboob SA, Eshraghian MR, Shahi MM. Effects of onion on serum uric acid levels and hepatic xanthine dehydrogenase/xanthine oxidase activities in hyperuricemic rats. Pak J Biol Sci. 2008;11:1779–84.
Hokazono H, Omori T, Yamamoto T, Akaoka I, Ono K. Effects of a fermented barley extract on subjects with slightly high serum uric acid or mild hyperuricemia. Biosci Biotechnol Biochem. 2010;74:828–34.
Niu J, Kolattukudy PE. Role of MCP-1 in cardiovascular disease: molecular mechanisms and clinical implications. Clin Sci (Lond). 2009;117:95–109. doi:10.1042/CS20080581.
Yan L, Graef GL, Claycombe KJ, Johnson LK. Effects of voluntary running and soy supplementation on diet-induced metabolic disturbance and inflammation in mice. J Agric Food Chem. 2013;61:9373–9. doi:10.1021/jf401588h.
Burris RL, Ng HP, Nagarajan S. Soy protein inhibits inflammation-induced VCAM-1 and inflammatory cytokine induction by inhibiting the NF-κB and AKT signaling pathway in apolipoprotein E-deficient mice. Eur J Nutr. 2014;53:135–48. doi:10.1007/s00394-013-0509-7.
Pedersen AN, Kondrup J, Børsheim E. Health effects of protein intake in healthy adults: a systematic literature review. Food Nutr Res. 2013;30:57. doi:10.3402/fnr.v57i0.21245.
Liu ZM, Chen YM, Ho SC, Ho YP, Woo J. Effects of soy protein and isoflavones on glycemic control and insulin sensitivity: a 6-mo double-blind, randomized, placebo-controlled trial in postmenopausal Chinese women with prediabetes or untreated early diabetes. Am J Clin Nutr. 2010;91:1394–401. doi:10.3945/ajcn.2009.28813.
Baer DJ, Stote KS, Paul DR, Harris GK, Rumpler WV, Clevidence BA. Whey protein but not soy protein supplementation alters body weight and composition in free-living overweight and obese adults. J Nutr. 2011;141:1489–94. doi:10.3945/jn.111.139840.
Bosland MC, Kato I, Zeleniuch-Jacquotte A, Schmoll J, Enk Rueter E, Melamed J, et al. Effect of soy protein isolate supplementation on biochemical recurrence of prostate cancer after radical prostatectomy: a randomized trial. JAMA. 2013;310:170–8. doi:10.1001/jama.2013.7842.
Mangano KM, Hutchins-Wiese HL, Kenny AM, Walsh SJ, Abourizk RH, Bruno RS, et al. Soy proteins and isoflavones reduce interleukin-6 but not serum lipids in older women: a randomized controlled trial. Nutr Res. 2013;33:1026–33. doi:10.1016/j.nutres.2013.08.009.
Acknowledgements
The present study was supported by a Grant for Project Research (Development of Fundamental Technology for Analysis and Evaluation of Functional Agricultural Product and Functional Foods) from the Ministry of Agriculture, Forestry and Fisheries of Japan. The authors would like to thank Enago (www.enago.jp) for the English language review.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
MF, RW, MKa, and AS have received national research funding from the Ministry of Agriculture, Forestry and Fisheries of Japan and/or Japan Science and Technology Agency for the present research project. MH, RK, and MKa are receiving funding for research projects apart from the present study from Kameda Seika Co. Ltd. HK and MF are employees of Kameda. Although MH, HK, MF, MKu, MKa, and AS are joint inventors of a patent application related to this study, the right to obtain the patent has been assigned from Niigata University to Kameda.
Authors’ contributions
MH, RW, MKa, MKu, YS, and AS planned the study design. MH and AS performed clinical tests and were responsible for data collection. MF and HK developed and provided intervention foods. MH, RK, MF, RW, and AS analyzed and interpreted the data. NT supervised statistical analyses. All authors approved of the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Hosojima, M., Kaseda, R., Kondo, H. et al. Beneficial effects of rice endosperm protein intake in Japanese men with risk factors for metabolic syndrome: a randomized, crossover clinical trial. BMC Nutr 2, 25 (2016). https://doi.org/10.1186/s40795-016-0065-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40795-016-0065-7