
Abstract
Background
Due to the increased prevalence of eating outside-the-home, alongside high rates of childhood obesity, the objective of this study was to analyze the nutritional quality of kids’ meals (including main entrées with accompanying side dishes, desserts and beverages) from Canadian fast-food (FFR) and sit-down restaurant (SDR) chains.
Methods
Data (serving size, calories, fat, saturated fat, trans fat, sodium and fibre) for 3,235 meals were obtained in 2010 from the websites of 7 SDRs and 10 FFRs of the 35 chains with more than 20 outlets in Canada and offering kids’ meals. T-tests were used to compare nutrient levels from SDR and FFR.
Results
On average, SDR meals had larger serving sizes compared to FFR meals (628 g vs. 562 g). As a result, SDR meals contained significantly higher amounts of calories (846 kcal vs. 737 kcal) and saturated fat (12 g vs. 8 g) (p < 0.0001). More than 50 % of kids’ meals from SDR and 35 % of meals from FFR exceeded 1,200 mg of sodium – the daily Adequate Intake for children aged 4-8 years. SDR meals had 41 % and 13 % of total calories coming from fat and saturated fat, while FFR had 37 % and 10 %, respectively. However, standardized comparisons of meals calculated per 100 g showed that FFR had significantly higher (p < 0.001) amounts of calories (244 vs 185 kcal/100 g) and sodium (538 vs 381 mg/100 g) compared to SDR.
Conclusion
These results illustrate that addressing the poor nutritional quality of restaurant kids’ meals should be a major public health priority.
Similar content being viewed by others

Background
In the past thirty years, the prevalence of childhood obesity has nearly doubled—presently, one in every four Canadian youth is considered overweight or obese [1]. Studies have shown that consumption of outside-the-home prepared foods significantly increases the net energy, total fat and sodium intake compared to at-home foods [2, 3]. Thus, eating outside-the-home may be a potential factor promoting the increased prevalence of obesity [4, 5].
According to the Canadian Community Health Survey, 19 % of children aged four to eight ate something prepared in a fast-food outlet on the day they were surveyed, and this number was even higher (23 %) among boys aged nine to thirteen [6]. Studies investigating the nutritional quality of kids’ meals at restaurants have consistently shown overall low nutritional quality. A study comparing the ‘healthiness’ of kids’ meals offered at major fast food restaurant chains (FFR) across the United States demonstrated that four of the five chains scored below 60 on the Healthy Eating Index-2005– a measure of diet quality [7]. Furthermore, studies investigating the nutritional quality of kids’ meals at both FFR and sit down chain restaurants (SDR) in the United States have shown that 99 % had a low nutritional quality due to excessive calories, sodium and/or fat [8], while only 3 % of meals met National School Lunch Program criteria for healthy food [9]. Similar findings were observed in kids’ meals offered in other countries. In Australia, only 16 and 22 % of FFR met the current industry’s nutritional criteria for children aged four to eight and nine to thirteen years, respectively [10]. Likewise, kids’ meals from FFR and SDR in the United Kingdom contained high calories, fat and sodium – either meeting or exceeding the nutrient-based standards established for children [11].
Although studies have consistently shown that outside-the-home meals targeted to children are not meeting current nutritional standards, more extensive research is needed. Multinational chain restaurants may share similar menu items but research has shown that that nutrient levels for similar menu items from the same multinational restaurant chain can vary significantly between countries [12, 13]. To date, research on the nutritional quality of restaurant foods in Canada have demonstrated unacceptably high levels of calories, sodium and saturated fat [14]. Addressing the excessive sodium content in restaurant foods needs to be a high priority, as many meals contain sodium levels, well in excess of daily recommendations. However, with the exception of one study that reported on the sodium level in kids’ meal items [15], there is no data on the nutritional quality of kids’ meals from Canadian chain restaurants. In addition, FFR are often targeted as the main culprit contributing to poor nutrition, however, research has shown that menu items from SDR often contain calories and sodium compared to menu items from FFR [16]. To date, Canadian FFR and SDR kids’ meals have not previously been compared. Therefore, the objectives of this study were to:
-
1)
Analyze the nutritional quality of kids’ meals (including serving size, calories, saturated fat, trans fat, sodium and fibre) from Canadian chain restaurants.
-
2)
Compare the nutritional quality of kids’ meals from fast-food restaurants (FFR) with those from sit-down restaurants (SDR).
-
3)
Assess sodium levels in kids’ meals relative to current recommendations for children.
Methods
Data were derived from the University of Toronto Restaurant Database, created in 2010. The database contains nutrition information (calories, serving size and the thirteen nutrients commonly found on the Nutrition Facts table) obtained from the websites of 85 Canadian chain restaurants that had more than 20 outlets nationally. Details pertaining to the construction of the database have been described elsewhere [16].
Using the database, 35 restaurant chains that provided nutrition information for kids’ menu items were identified. Online menus and nutritional information for kids’ menu items from these restaurants were downloaded in autumn 2012 and compared to original database. Sixteen restaurant chains were excluded because data was unavailable for >50 % of their kids’ menu offerings. Two were excluded because they did not include serving size data. In total, 7 SDR and 10 FFR chains were included in the study and included a wide variety from pizza, burger, Mexican, and breakfast restaurant chains etc. Figure 1 shows the methodology for restaurant chain selection. Five-percent of the meal combinations and nutrition composition data were double-checked by an independent coder to ensure accuracy. There was high agreement between coders, with only a 1 % discrepancy; any errors were recalculated and adjusted accordingly.

Overview of methodology used to identify FFR and SDR chains included in this study
Kids’ meals typically contained an entrée, along with a side dish, a drink and often a dessert. Nutrition information from all possible combinations of each entrée with various accompanying sides, drinks and desserts were calculated. For example, if a hamburger entrée came with a choice of two side dishes and a choice of two drinks, four possible meal combinations were derived (hamburger + side 1 + drink 1, hamburger + side1 + drink2, hamburger + side2 + drink1, and hamburger + side2 + drink 2). Diet drinks (containing no sugar) and meal “add-ons/up-grades” were excluded. Three standard beverages (based on the average serving size and nutrient levels in cola soft drinks, 2 % milk and orange juice) were assigned when restaurants did not provide details about their kids’ beverages. For this study, serving size, calories, fat, saturated fat, trans fat, sodium and fibre were assessed.
Statistical analysis
Data were weighted to ensure that each restaurant and each meal was equally represented in the sample, irrespective of the number of combinations derived from each entrée and the number of meals offered at each restaurant. Descriptive statistics and tests of normality were calculated both per serving and per 100 g for complete meals (entrée + side dish + dessert + beverage), as well as meals excluding beverages (entrée + side dish + dessert) and meals excluding beverages and dessert (entrée + side dish). Measures of variance were reported as standard errors because the data was weighted. T-tests were used to compare nutrient levels in SDR, versus FFR. The proportion of meals exceeding the children’s AI (Adequate Intake, the recommended daily nutrient level to maintain health) for sodium of 1,200 mg/day and 1,500 mg/day, and UL (Tolerable Upper Intake Level, highest value of acceptable daily nutrient intake; exceeding UL can negatively impact health) of 1,900 mg/day and 2,200 mg/day for ages 4 to 8 years and 9 to 13 years, respectively, were also calculated [17, 18]. Other nutrients, such as saturated fat and total fat, were not compared to IOM recommendations because there is no recommended AI for these nutrients. Statistical analyses were conducted using SAS version 9.3 software (SAS Institute Inc.).
Results
Comparing nutrient levels in kids’ meals from FFR and SDR
Table 1 shows the average nutrient levels in 3,235 kids’ meals (comprised of an entrée, side dish, beverage and dessert) from Canadian SDR and FFR. Kids’ meals from SDR contained significantly higher calories, fat, saturated fat and trans fat content compared to FFR. Fibre was higher in FFR compared to SDR (p <0.01). Sodium content was consistently high in both SDR and FFR.
SDR meals had a significantly larger serving size (p < 0.001) when compared to FFR meals (Table 2). Standardized analyses per 100 g showed that; FFR had significantly higher amounts of calories, fat and sodium (p < 0.001), with no significant difference in saturated fat levels (p = 0.48). Analyses including dessert (Additional file 1: Table S1) showed similar trends.
Percentage of total calories from fat and saturated fat
In SDR, 41 % of total calories were derived from fat, while 13 % was derived from saturated fat (Table 2). In FFR, the distributions were 37 and 10 %, respectively. Saturated fat as a percentage of total fat was 31 and 27 % for SDR and FFR, respectively.
Sodium levels in comparison to the children’s’ recommendations
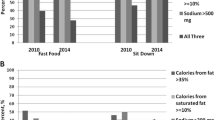
More than 50 % of the kids’ meals from SDR and 32 % of meals from FFR exceeded the daily AI (1,200 mg) for children aged 4-8 years (Fig. 2), while 27 % and over 11 % respectively exceeded the AI for children 9–13 years old. Approximately 1 % of meals exceeded the UL.

Percent comparison of kids’ meals exceeding the Institute of Medicine’s daily sodium recommendations AI* for children. N = 3235. Kids’ meals consist of an entrée, side dish, beverage and when applicable, dessert. *AI = Adequate Intake, the recommended daily nutrient level to maintain health, for sodium of 1,200 mg/day and 1,500 mg/day, for children ages 4 to 8 years and 9 to 13 years, respectively
Fibre levels in relation to children’s’ recommendations
Restaurant kids’ meals on average contained 5–6 grams per serving. This is approximately 25 % of the AI for fibre for 4–8 years old children, and 19 % of the AI for children 9–13 years old.
Discussion
The results of this study showed that kids’ meals from FFR and SDR were high in calories, and also alarmingly high sodium and saturated fat when compared to the Institute of Medicine (IOM) recommendations. Mean sodium levels exceeded the AI for children 4–8 years old, and mean saturated fat levels ranged from 31 to 36 % of total fats, or 10–13 % of total calories from fat. Although there is no specific AI for saturated fat, the American Heart Association recommends aiming for a dietary pattern that achieves 5 to 6 % of calories from saturated fat [19]. Due to larger portion sizes, kids’ meals from SDRs had significantly higher amounts of calories and saturated fat when compared to FFRs. However, when nutrient levels were standardized per 100 g, SDRs had a significantly lower calorie and sodium density compared to FFRs.
The data showing that SDR meals had significantly higher levels of unhealthy nutrients when compared to FFR is not a novel finding. Two previous studies have also found that SDR meals have higher amounts of calories, fat and saturated fat [20, 21]. However, our study expanded upon this research by demonstrating that among kids’ meals, this discrepancy was largely due to larger portion sizes in SDR. Furthermore, when comparisons were standardized, FFR often had higher densities of unhealthy nutrients. Therefore, our results indicate that kids’ meals from SDR are not necessarily less healthful in terms of their nutrient composition, when compared to kids’ meals from FFR, rather they are simply larger.
These results were consistent with similar studies conducted in other countries that have investigated the nutrient levels in kids’ meals from chain restaurants. In comparison to Batada et al.’s findings in the United States [8], calorie levels were similar (740 kcal in the US, versus 737–846 kcal in the Canadian data in this study). The observed differences in sodium levels (1,448 mg in the US versus 1,230–1,248 mg in this study) may be due to the fact that, unlike Batada’s study, the data presented here was weighted to ensure that each restaurant and meal was equally represented.
Similar to our findings, previous research has shown that 1 % of FFR kids’ meals in Australia exceeded the sodium UL for children [10]. However, kids’ meals from Australia on average had fewer calories (532 kcal versus 737 in our study), less saturated fat (6.4 g versus 8 g), and less sodium (702 mg versus 1230 mg) compared to the Canadian results in this study. The higher levels observed in Canada compared to Australia may be due to the variation in the number of meals assessed (199 meals in Australian study, versus 815 FFR meals in our Canadian study). Consistent with our findings, research in the United Kingdom demonstrated that SDR had higher calories compared to FFR and similar to our findings, this difference was due to larger portion sizes [11]. In addition, the FFR kids’ meals in the United Kingdom also had a higher calorie density compared to SDR meals (1.6 kcal/g and 1.2 kcal/g).
The differences seen when comparing nutrient levels per serving and per 100 g illustrate the importance of setting nutrition standards to assess nutrient levels both per serving and per 100 g. The standards set in the US according to the National Restaurant Association’s criteria, assess calories, sodium and trans fat per serving, and assess fats as a percentage of total calories. Currently, the US National Restaurant Association’s criteria does not assess any nutrient levels on a per 100 g basis. Therefore, the large differences seen in this study, when comparing nutrient levels per 100 g, illustrate that standardized comparisons are an important factor when developing criteria to define healthy restaurant meals.
In the United States, efforts are being made to improve the nutritional quality of kids’ restaurant meals and to encourage healthier choices for children when eating-out. For example, two counties in California have banned the distribution of toys with meals that do not meet specific nutritional criteria [22]. In addition, the US National Restaurant Association has launched the “Kids Live Well” program which encourages restaurants to offer and promote healthy kids’ meals that meet specific nutritional criteria [23]. Despite these efforts elsewhere, to date, none of these policies or initiatives exist in Canada. Therefore, the results of this study illustrate that there is a need for programs and/or policies in Canada to encourage restaurants to improve the nutritional quality of their kids’ meals. Preliminary research in the United States has shown that menu-labeling in restaurants may be one way to encourage restaurants to improve the nutritional quality of their meals [24]. Additionally, providing sodium targets for restaurant foods, as was done by Health Canada for packaged foods in Canada would further support such efforts.
Limitations of this study are that many restaurants did not provide data for their kids’ meals; therefore our data represent only a sample of the restaurant sector. Furthermore, the integrity of the results are reliant upon the validity of the data provided online by the restaurants. While this data was collected in 2010, studies to date have shown no major changes in sodium [25], or calorie levels in restaurants [26], therefore, these conclusions are likely still relevant.
Conclusion
Overall, these results show that kids’ meals from Canadian chain restaurants contain alarmingly high amounts of calories, fats and sodium. Therefore, considering the prevalence of eating outside-the-home, alongside the increased rates of childhood obesity, these data suggest that addressing the poor nutritional quality of kids’ meals at restaurants should be an important public health priority.
Abbreviations
- FFR:
-
fast-food restaurants
- SDR:
-
sit-down restaurants
References
Public Health Agency of Canada-Canadian Institute for Health Information, Obesity in Canada - A joint report from the Public Health Agency of Canada and the Canadian Institute for Health Information. 2011.
Bowman SA, Gortmaker SL, Ebbeling CB, Pereira MA, Ludwig DS. Effects of fast-food consumption on energy intake and diet quality among children in a national household survey. Pediatrics. 2004;113(1 Pt 1):112–8.
Powell LM, Nguyen BT. Fast-food and full-service restaurant consumption among children and adolescents: effect on energy, beverage, and nutrient intake. JAMA Pediatr. 2013;167(1):14–20.
Garcia G, Sunil TS, Hinojosa P. The fast food and obesity link: consumption patterns and severity of obesity. Obes Surg. 2012;22(5):810–8.
Fleischhacker SE, Evenson KR, Rodriguez DA, Ammerman AS. A systematic review of fast food access studies. Obes Rev. 2011;12(5):e460–71.
Garriguet D: Nutrition: Findings from the Canadian Community Health Survey Overview of Canadians' Eating Habits. In. Edited by Division HS, vol. Catalogue no. 82-620-MIE — No. 2. Ottawa: Statistics Canada; 2004.
Kirkpatrick SI, Reedy J, Kahle LL, Harris JL, Ohri-Vachaspati P, Krebs-Smith SM. Fast-food menu offerings vary in dietary quality, but are consistently poor. Public Health Nutr. 2014;17(4):924–31.
Batada A, Bruening M, Marchlewicz EH, Story M, Wootan MG. Poor nutrition on the menu: children’s meals at America’s top chain restaurants. Childhood obesity (Print). 2012;8(3):251–4.
O’Donnell SI, Hoer SL, Mendoza JA, Goh ET. Nutrient quality of fast food kids meals. Am J Clin Nutr. 2008;88:1388–95.
Wellard L, Glasson C, Chapman K. Fries or a fruit bag? Investigating the nutritional composition of fast food children’s meals. Appetite. 2012;58(1):105–10.
Reeves S, Wake Y, Zick A. Nutrition labeling and portion size information on children’s menus in fast-food and table-service chain restaurants in London, UK. J Nutr Educ Behav. 2011;43(6):543–7.
Hobin E, White C, Li Y, Chiu M, O’Brien MF, Hammond D. Nutritional quality of food items on fast-food ‘kids’ menus’: comparisons across countries and companies. Public Health Nutr. 2014;17(10):2263–9.
Dunford E, Webster J, Woodward M, Czernichow S, Yuan WL, Jenner K, Ni Mhurchu C, Jacobson M, Campbell N, Neal B. The variability of reported salt levels in fast foods across six countries: opportunities for salt reduction. CMAJ. 2012;184(9):1023–8.
Scourboutakos MJ, Semnani-Azad Z, L’Abbe MR. Restaurant Meals: Almost a Full Day’s Worth of Calories, Fats, and Sodium. JAMA Intern Med. 2013;173(14):1373–4.
Scourboutakos MJ, L’Abbe MR. Sodium levels in Canadian fast-food and sit-down restaurants. Can J Public Health. 2013;104(1):e2–8.
Scourboutakos MJ, L’Abbe MR. Restaurant menus: calories, caloric density, and serving size. Am J Prev Med. 2012;43(3):249–55.
Canada H. Food and Nutrition. In. Health Canada; 2006.
Dietary Reference Intakes: Water, Potassium, Sodium, Chloride, and Sulfate - See more at: http://iom.nationalacademies.org/Reports/2004/Dietary-Reference-Intakes-Water-Potassium-Sodium-Chloride-and-Sulfate.aspx#sthash.FDayAJrw.dpuf. In. Institude of Medicine; 2004.
American Heart Association Nutrition C, Lichtenstein AH, Appel LJ, Brands M, Carnethon M, Daniels S, Franch HA, Franklin B, Kris-Etherton P, Harris WS, et al. Diet and lifestyle recommendations revision 2006: a scientific statement from the American Heart Association Nutrition Committee. Circulation. 2006;114(1):82–96.
Serrano EL, Jedda VB. Comparison of fast-food and non-fast-food children’s menu items. J Nutr Educ Behav. 2009;41(2):132–7.
Wu HW. What’s on the menu? A review of the energy and nutritional content of US chain restaurant menus. 2012:1-10
Ordinance amending Article 8 of the San Francisco Health Code by adding Sections 471.1 through 479.9 to set nutritional standards for restaurant food sold accompanied by toys of other youth focused incentive items [http://www.sfbos.org/ftp/uploadedfiles/bdsupvrs/committees/materials/lu092710_101096.pdf]
Kids Live Well Program - About, [http://www.restaurant.org/Industry-Impact/Food-Healthy-Living/Kids-LiveWell/About]
Bruemmer B, Krieger J, Saelens BE, Chan N. Energy, Saturated Fat, and Sodium Were Lower in Entrées at Chain Restaurants at 18 Months Compared with 6 Months Following the Implementation of Mandatory Menu Labeling Regulation in King County, Washington. Journal of the Academy of Nutrition and Dietetics. 2012;112(8):1169–76.
Scourboutakos M LAM. A longitudinal study of changes in sodium levels in a sample of Canadian chain restaurant foods from 2010 to 2013. Canadian Medical Association Journal Open 2014, Accepted.
Jacobson MF, Havas S, McCarter R. Changes in sodium levels in processed and restaurant foods, 2005 to 2011. JAMA Intern Med. 2013;173(14):1285–91.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that they have no competing interest.
Authors’ contributions
ZSA was involved with the conception and design, acquisition of data, analysis/interpretation and drafting of the manuscript. MJS was involved with the conception and design, acquisition of data and critical revision of the manuscript for important intellectual content. MRL guided the conception and design and critical revision of the manuscript for important intellectual content. All authors have read and approved the final submitted manuscript.
Additional file
Additional file 1: Table S1.
Comparison of nutrient levels in sit-down and fast-food restaurant kids’ meals (excluding beverages). (DOCX 13 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Semnani-Azad, Z., Scourboutakos, M.J. & L’Abbé, M.R. Kids’ meals from Canadian chain restaurants are exceedingly high in calories, fats, and sodium: a cross-sectional study. BMC Nutr 2, 16 (2016). https://doi.org/10.1186/s40795-016-0056-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40795-016-0056-8