
Abstract
Introduction
Intestinal parasite infections (IPIs) remain a significant public health concern, particularly in developing countries, where they disproportionately affect vulnerable populations such as prison inmates. Despite their high prevalence globally, many intestinal parasites are still neglected in research and control efforts. This study aimed to assess the prevalence and intensity of intestinal parasite infections, evaluate the performance of diagnostic methods, and identify associated factors of intestinal parasite infection among inmates of Hossana prison.
Method
An institution-based cross-sectional study was conducted at Hossana Prison from March to July 2023. A total of 421 inmates were enrolled using a systematic random sampling technique. Data on socio-demographics and determinants were collected using a semi-structured questionnaire. Faecal samples were examined using direct wet mount, Kato-Katz, and formol-ether concentration techniques. SPSS was used for data analysis. Logistic regression analysis with adjusted odds ratios (AOR) and 95% CI was used to assess the associations of independent variables with intestinal parasitic infections.
Results
The composite prevalence of intestinal parasitic infections among inmates was 35.6%, with most soil-transmitted helminth infections of light intensity. The frequently detected parasites were Entamoeba histolytica/dispar, Giardia lamblia, and the hookworms. The formol-ether concentration technique (FECT) demonstrated higher sensitivity for detecting soil-transmitted helminths compared to other techniques. Factors significantly associated with intestinal parasitic infections included informal education (AOR = 3.06; 95% CI: 1.01–8.17; p = 0.049), occasional handwashing after using the toilet (AOR = 3.65; 95% CI: 2.65–5.12; p = 0.001) or before eating (AOR = 6.72; 95% CI: 2.44–18.55; p = 0.001), not trimming fingernails (AOR = 3.24; 95% CI: 1.24–8.46; p = 0.016), sleeping in groups (AOR = 4.34; 95% CI: 2.16–9.18; p = 0.001), and lack of prior health education on intestinal parasitic infections (AOR = 6.21; 95% CI: 3.93–10.94; p = 0.001).
Conclusion
The moderate prevalence of intestinal parasitic infections among Hossana prison inmates is concerning, highlighting the need for targeted interventions. These should focus on improving sanitation and hygiene practices, providing regular health screenings and prompt treatment, modifying sleeping habits, maintaining personal hygiene, and offering health education on intestinal parasitic infection prevention strategies to reduce the spread of infections within the incarcerated population.
Similar content being viewed by others


Background
Intestinal parasitic infections (IPIs) remain a major global public health concern, affecting an estimated 3.5 billion people worldwide [1, 2]. Among these, soil-transmitted helminths (STHs) account for approximately 1.5 billion cases and are responsible for an estimated 4.98 million disability-adjusted life years (DALYs) [3,4,5,6]. Schistosoma species and STHs are classified as Neglected Tropical Diseases (NTDs) due to their high prevalence and limited attention in global health agendas [7]. In developing countries, more than half of the population is affected by IPIs, with protozoan infections occurring more frequently than helminthic infections [3, 7]. The burden of these infections varies depending on factors such as parasite species, climate, age, gender, and individuals’ immune and nutritional status [2]. Global estimates indicate that Entamoeba histolytica is responsible for over 55,000 deaths and 2.2 million DALYs annually [6], while Schistosoma species infect more than 240 million people worldwide [5, 8].
The impact of IPIs is particularly significant in prison populations, where living conditions often facilitate rapid transmission. Overcrowding, shared sanitation facilities, and limited access to healthcare services contribute to high infection rates among inmates [3, 4]. These infections can lead to chronic diarrhea, abdominal pain, malnutrition, and anemia, all of which impair physical health, cognitive function, and overall well-being [1, 9, 10]. These conditions are further exacerbated by inadequate sanitation, poor waste management, and insufficient healthcare infrastructure in many correctional facilities, particularly in low-resource settings, which increases inmates’ vulnerability to IPIs and elevates overall healthcare costs [4, 11, 12].
In Africa, favourable climatic conditions, persistent poverty, and poor socio-economic development significantly contribute to the higher prevalence of IPIs. On this continent, many individuals are affected by at least one parasitic species [10, 13]. The most common STH infections in Africa include ascariasis (Ascaris lumbricoides), hookworm infection (hookworms), strongyloidiasis (Strongyloides stercoralis), and trichuriasis (Trichuris trichiura) [10]. Schistosoma also causes approximately 200,000 deaths each year. Moreover, E. histolytica and Giardia lamblia are common causes of diarrhoea disease [6]. The prevalence of IPIs among African inmates is alarmingly high, often exceeding 70% [14, 15]. These infections worsen overall health, impact educational performance, and reduce productivity [16, 17].
In Ethiopia, IPIs are a major public health concern, often being among the top causes of outpatient morbidity. Millions of individuals are affected by STH infection and schistosomiasis in the country [18]. Addressing these issues has been prioritized in Ethiopia’s national master plan [19]. Prisoners in Ethiopia face severe challenges due to overcrowded facilities, poor sanitation, inadequate access to clean water, mobility issues, psychiatric conditions, stress, and limited medical care [15, 20]. Some research in Ethiopian prisons indicates the prevalence of IPIs ranges from 42.6 to 61.8% [15, 16, 21]. Determining the status of IPIs and their correlations is essential for developing effective control strategies. Existing data indicate that the issue varies by locality. Therefore, this study sought to assess the prevalence and intensity of IPIs, evaluate the performance of diagnostic methods, and identify associated factors of IPIs among inmates of Hossana prison, Central Ethiopia.
Methods and materials
Study design and area
An institution-based cross-sectional study was conducted from March 20 to July 17, 2023, in Hossana City prison. Hossana is the capital of the Central Ethiopia region, located 232 km south of Addis Ababa. Hossana spans 34 km² at an elevation of 2,177 m (7°34′60″N, 37°52′60″E), with a population of approximately 104,208 [22]. The city experiences an average annual temperature of 21.6 °C, average rainfall of 59 mm, and relative humidity of 64.8%. The local soil is composed of sand, alluvial sediment, and gravel [23]. Hossana City Prison is located 7 km from the town in an area called “Ajjo”. The institution occupies an estimated area of 10,000 square metres. According to the information obtained from the Hadiya Zone prison authority, the prison had 1,324 inmates during the study time. The prison has an on-site clinic offering diagnostic and treatment services; however, water supply and sanitation facilities are inadequate.
Population and eligibility criteria
The source population comprised all inmates at Hossana Prison, while the study population included those present during the study period. Eligible participants were inmates who had been incarcerated for at least one month. Inmates were excluded if they were mentally ill and unable to respond to questions or had been treated for IPIs within the month preceding the study.
Sample size calculation
The sample size was calculated using the single population proportion formula [15], based on a previously reported prevalence of 48.1% [20], a 95% confidence level, a 5% margin of error. After adjusting for a 10% non-response rate, the final sample size was 421.
Sampling technique
A systematic random sampling technique was employed to select study participants. The sampling frame was obtained from the information desk of Hossana prison. To compute the sampling interval (K-value), the total number of inmates was divided by the desired sample size of 421.
Then, after the first participant was selected randomly using a random number generator, the process was followed by systematic selection of every Kth interval.
Data collection
Before data collection, trained medical laboratory technologists obtained written informed consent/assent from participants in their preferred language (Hadiyya or Amharic). Face-to-face interviews were conducted using a semi-structured questionnaire to collect data on socio-demographics, medical history, hygiene, and other risk factors. The questionnaires were adapted from validated tools used in previous studies [4, 20, 21, 24]. Minor adjustments were made to suit the specific study needs. These questionnaires were initially developed in English, translated into the local language by bilingual experts, and back-translated to English to ensure linguistic and conceptual consistency. Direct observations were used to assess latrine availability, waste disposal facilities, and fingernail hygiene.
The participants were instructed on how to collect fecal samples properly. Approximately 5 g of fecal samples were collected in a wide-necked, dry, leak-proof, and grease-free container. Then, each sample was labelled using unique identification numbers. The specimens were examined immediately under a microscope using a direct wet mount (DWM), Kato-Katz technique, following the standard working procedure [1, 25]. The remaining samples were preserved with 10% formalin, placed in a triple packaging system, and transported to Hawassa University parasitology laboratory for examination using the formol-ether concentration Technique (FECT) [1, 25]. In the Kato-Katz technique, Eggs were counted and multiplied by a factor to calculate eggs per gram of feces, which helps quantify infection intensity [25]. To convert the egg count to eggs per gram, calculate how many such smears fit into 1 gram (1000 mg).
Therefore, to estimate EPG, the number of parasite eggs counted on the smear was multiplied by a factor of 24 [25]. This EPG value was then used to categorize the intensity of the infection into three levels: Light, Moderate, and Heavy, depending on the species of the parasite [1, 25].
Data quality assurance
A week before the survey, supervisors and data collectors received two days of training on the study objectives, procedures, and data collection methods, including interviews, questionnaire administration, participant approaching, and data quality assurance. The questionnaire was pre-tested on 5% of the sample at Hosana City Kebele 3 police office (temporary prison) and revised based on feedback. Its reliability was assessed using Cronbach’s alpha, which indicated good internal consistency (α = 0.82). All procedures adhered to the WHO standard operating procedures across pre-analytical, analytical, and post-analytical phases. Specimen collection and handling followed established quality control protocols, with reagents routinely checked for contamination. To minimize observer bias, two independent, blinded laboratory personnel conducted microscopic examinations separately, recording results on different sheets. Inconsistent findings were re-examined, and any discordant results were reviewed by a third independent microscopist.
Data analysis and interpretation
To ensure accuracy, data were entered twice using Epi-Data version 4.6 and then exported to Statistical Package for the Social Sciences (SPSS) version 26 (Armonk, NY: IBM Corp) for analysis. Descriptive statistics were summarized using means for continuous variables and frequencies (percentages) for categorical variables. The data were presented in tables and graphs/charts to clearly illustrate the findings. A binary logistic regression analysis model was conducted to examine the association between each independent variable and the prevalence of IPIs. Initially, bivariate analysis was performed to compute a crude odds ratio (COR) and to screen out potentially significant independent variables at a p-value ≤ 0.25. All variables below this threshold were included in a multivariable logistic regression analysis, which helps to control the effect of confounders. During multivariable logistic regression analyses, the adjusted odds ratio (AOR) with 95% confidence intervals (CIs) and a p-value < 0.05 were used to describe the strength of the association and statistical significance. Model adequacy was evaluated using the Hosmer-Lemeshow goodness-of-fit test (p > 0.05 indicating good fit). Multicollinearity was checked using the Variance Inflation Factor (VIF), with values ≤ 10 considered acceptable [26]. Variables were selected using the backward likelihood-ratio technique.
The intensity of infection was analyzed using the WHO assessment guideline [25]. The composite reference standard (CRS), which combined the results of three diagnostic methods (DWM, Kato-Katz, and FECT), was used as the gold standard for method performance comparisons, as recommended in the absence of a single definitive reference method. The inter-rater agreement among the diagnostic methods was evaluated using the Kappa statistic (κ), interpreted as follows: slight (0.01–0.20), fair (0.21–0.40), moderate (0.41–0.60), substantial (0.61–0.80), and almost perfect (0.81–0.99) [25].
Results
Socio-demographic characteristics of the study participants
A total of 421 participants were included in the study, achieving a 100% response rate. Among those examined for IPIs, 97.4% (n = 410) were male. The participants’ ages ranged from 15 to 86 years, with a mean age of 30.5 years. Regarding education, 30.6% (n = 129) of the inmates had only informal education, while 4.5% (n = 19) had attained a diploma or higher qualification. Nearly half of the participants (48.9%, n = 206) were married. Before incarceration, 44.9% (189) of the inmates were unemployed, and 53.2% (n = 224) lived in urban areas. Of the participants, 37.8% (n = 159) had been imprisoned for less than one year, while 24% (n = 101) had been incarcerated for two years or more. Approximately 52.7% (n = 222) of participants had no income before imprisonment (see Table 1).
Sanitation and hygienic practices of the inmates
Of the 421 inmates, 68.6% (n = 289) reported washing their hands after using the toilet, and 73.2% (n = 308) reported washing before meals. However, among those who practiced handwashing, only 54.4% (n = 229) used soap. About 76% (n = 320) of the inmates accessed drinking water from a tanker, while 56% (n = 236) received food from outside the prison, and 27.6% (n = 116) practiced “gursha” (feeding others). Additionally, 25.7% (n = 108) of the inmates did not trim their hand fingernails. Most rooms housed between 51 and 100 prisoners, and 46.6% (n = 196) of inmates slept in groups. Nearly half (47.7%, n = 201) of the inmates had not received health education on IPIs, and 66% (n = 278) had access to laboratory diagnosis services (see Table 2).
Prevalence of intestinal parasitic infections among inmates
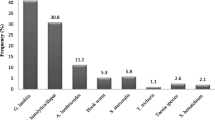
The composite prevalence, defined as the proportion of inmates positive by any of the three diagnostic methods, was 35.6% (n = 150) (95% CI: 31.03–40.17). A total of eight parasite species were identified, with varying prevalence rates among the surveyed population. E. histolytica/dispar showed the highest prevalence at 6.9% (n = 29), followed closely by G. lamblia at 6.2% (n = 26), and the hookworm species at 5.7% (n = 24). A. lumbricoides were present in 5.5% (n = 23) of the cases, while Entamoeba coli was found in 3.3% (n = 14) cases. Taenia species accounted for 2.6% (n = 11), S. mansoni for 1.4% (n = 6), and T. trichiura had the lowest prevalence at 1.0% (n = 4) (see Fig. 1a). In this study, the data showed that multiple protozoan infections account for 3.1% (n = 13) of all cases. The most frequent combination was E. histolytica/dispar with G. lamblia, found in 1.7% of all cases, or 53.8% (n = 7) of the multiple infection cases. Other detected co-infections included E. histolytica/dispar with E. coli (0.5% of all cases or 15.4% of multiple infections), E. histolytica/dispar with both G. lamblia and E. coli (0.7% of all cases or 23.1% of multiple infections, n = 3), and G. lamblia with E. coli (0.2% of all cases or 7.7% of multiple infections, n = 1) (see Fig. 1b).

Species-specific prevalence and co-infections of IPIs among inmates of Hossana Prison, Ethiopia, 2023
The prevalence of intestinal parasites varied across the three diagnostic methods used. The FECT method showed the highest overall detection rate (30.2%, n = 127), followed by DWM (23.8%, n = 100) and Kato-Katz (16.2%, n = 68). Protozoan parasites such as E. histolytica/dispar, G. lamblia, and E. coli were detected only by FECT and DWM, with comparable rates. Multiple parasitic infections were observed in 3.1% (n = 13) cases using both FECT and DWM. Some Helminth infections were detected by all three methods, though with varying sensitivity. Kato-Katz recorded the highest rates for Hookworm (5.7%, n = 24) and A. lumbricoides (5.5%, n = 23), followed by Taenia spp. (2.6%, n = 11), and S. mansoni (1.4%, n = 6). The FECT and DWM methods showed slightly lower detection rates for these helminths. However, the DWM failed to detect S. mansoni or T. trichiura (see Fig. 2).

Detection rate of IPIs by DWM, Kato-Katz, and FECT methods among inmates of Hossana Prison, Central Ethiopia, 2023
Diagnostic methods performance and testing agreement
The performance of the three diagnostic methods was assessed against CRS, considered the gold standard. FECT showed the highest sensitivity (84.7%) and NPV (92.2%), with near-perfect agreement (κ = 0.88). DWM demonstrated 66.7% sensitivity, 84.4% NPV, and substantial agreement (κ = 0.72). Kato-Katz had the lowest sensitivity (45.3%), NPV (76.8%), and moderate agreement (κ = 0.52) (see Table 3).
Intensity of infection with soil-transmitted helminths and Schistosoma mansoni
According to the WHO assessment guidelines [25], all STH infections (A. lumbricoides, T. trichiura, and hookworm) were of light intensity, while S. mansoni infections ranged from light to moderate intensity. The median egg counts per gram of stool (EPG) varied among species: Ascaris lumbricoides (1392 EPG), hookworm (936 EPG), Trichuris trichiura (432 EPG), and Schistosoma mansoni (72 EPG) (see Fig. 3).

Intensity of STHs and S. mansoni infections among prison inmates in Hossana, Central Ethiopia, 2023
Factors associated with intestinal parasitic infections
Multivariable logistic regression analysis identified several determinants significantly associated with intestinal parasitic infections (IPIs) among prison inmates. Inmates who attained informal education were more likely to be infected compared to those with diploma-level education or higher (AOR = 3.06; 95% CI: 1.01–8.17; p = 0.049). Inmates who sometimes washed their hands after using the toilet (AOR = 3.65; 95% CI: 2.65–5.12; p = 0.001) or before eating (AOR = 6.72; 95% CI: 2.44–18.55; p = 0.001) were more likely to have infections. Additionally, inmates who did not trim their fingernails (AOR = 3.24; 95% CI: 1.24–8.46; p = 0.016), those who slept in groups (AOR = 4.34; 95% CI: 2.16–9.18; p = 0.001), and those who had not received health education on IPIs (AOR = 6.21; 95% CI: 3.93–10.94; p = 0.001) were at significantly higher risk (see Table 4).
Discussion
The findings of this study indicate that IPIs have moderate public health significance among the inmate population. Although some preventive measures are in place, the observed prevalence highlights the need for strengthened interventions, including improved sanitation, health education on personal hygiene, routine screening, and targeted strategies for high-risk groups. Designing effective intervention strategies requires identifying the highest-risk communities through epidemiological surveys and intensity analysis, identifying potential contributing factors, and employing high-performance diagnostic methods. In line with these objectives, our study found a composite IPI prevalence of 35.6% among prison inmates, which is consistent with a study in Guinea [11]. This prevalence is lower than studies in Ethiopia [15, 20] and higher than studies in Nigeria [27], Nepal [17], and India [28]. Such differences may be attributed to the variation in the activities of the study populations (such as cleaning the compound or participating in outdoor labor activities that increase contact with contaminated soil or water), climatic and environmental conditions, sources of drinking water, and the number of inmates per cell. For instance, in a study conducted in Ethiopia [15], participants had frequent contact with soil, which may increase the risk of STH infections. In another study [20], a hotter, more humid climate, overcrowded conditions, and reliance on tanker-supplied water likely facilitate parasite transmission [29, 30].
In the present study, protozoan parasites were more prevalent (54.7%) than parasitic helminths, a pattern consistent with findings from Ethiopia [20, 21], Kenya [24], India [28], Nepal [17], and Nigeria [31]. This is because protozoa are more immediately contagious compared to helminth eggs, which require time to become infectious [1]. Entamoeba histolytica/dispar was the most common protozoan observed, which is similar to reports from Ethiopia [15, 21] and Kenya [24]. This may be due to the persistent nature of Entamoeba infections, which continue to propagate and spread unless treated, even with better hygienic conditions [15]. However, these findings contrast with a study in Malaysia [32], where Blastocystis species were the most common protozoa. Similarly, the most prevalent STHs were Hookworms. This is consistent with reports from Ethiopia [15] and Nigeria [31]. However, in another study in Ethiopia, A. lumbricoides was common [20]. This may be the cool climate in our study area may be less favorable for the embryonation of immature Ascaris lumbricoides ova. Similarly, the survival of hookworm larvae may be limited by extreme temperatures and desiccation, which could reduce their prevalence in other studies [33]. The higher prevalence of hookworm observed in our study could be attributed to frequent barefoot walking and soil contact during daily activities.
The most frequent co-infection observed was E. histolytica and G. lamblia, which aligns with findings from other studies [20, 21, 34]. However, this differs from a study in Kenya [24], where the most prevalent co-infections were A. lumbricoides and G. lamblia. Similarly, in Ethiopia, E. histolytica/dispar and A. lumbricoides were commonly found together. The differences in co-infection patterns may be attributed to geographical location, climatic conditions, and host-related factors, including immunity, age-related susceptibility, and the frequency of exposure to contaminated environments. Moreover, specific activities of the study populations, such as soil contact, may further contribute to variations in infection patterns across regions.
In our study, all detected cases of STH infections exhibited light intensity, which aligns with findings from previous research conducted in Ethiopia [16, 35]. This consistency could be beneficial for confirming the success of STH elimination efforts in our country. Typically, STH infections are unevenly distributed, meaning that while most people have low-intensity infections, only a small percentage of individuals carry infections of high intensity. S. mansoni infections range from light to moderate intensity, likely reflecting variations in exposure and the host’s immune response. These results underscore the importance of effective disease control measures and the need for tailored treatment strategies.
Accurate and reliable diagnostics are essential for effective disease monitoring and public health intervention in both community and endemic settings. This accuracy is defined by the sensitivity and specificity of the diagnostic methods used [36]. Although the Kato-Katz technique is widely endorsed for epidemiological studies of S. mansoni due to its simplicity and cost-effectiveness, our study reveals that it has comparable performance to CRS for detecting S. mansoni. Nonetheless, it exhibits lower sensitivity and negative predictive value compared to the FECT and the DWM methods for diagnosing STHs [9, 36, 37]. The FECT has demonstrated acceptable diagnostic performance, especially for detecting intestinal protozoa and STHs. This finding is consistent with results from other studies [36,37,38], which have reported that FECT provides reliable diagnostic accuracy for these infections. However, our results contradict findings from a study [39], which reported that the Kato-Katz technique has better performance outcomes. This discrepancy may be attributed to several factors, such as variations in study design, differences in the prevalence and intensity of infections in the study populations, or methodological differences in sample processing and analysis. Further investigation into these factors is necessary to understand the reasons behind the differing results and to refine diagnostic strategies.
This study also revealed that IPIs are a significant public health problem among prison inmates, strongly linked to poor hygiene practices and low educational attainment [10, 13]. This finding is supported by studies conducted in Kenya [24], Guinea [11], and Ethiopia [40]. This may be due to lower education levels are often linked to a lack of awareness about how parasitic infections are transmitted and prevented, which can increase the risk of acquiring IPIs [10]. This emphasizes the critical role of health literacy in adopting effective hygiene measures to interrupt transmission pathways within confined settings [5]. Besides, inmates with untrimmed fingernails are more prone to infections, a finding supported by studies across different areas of Ethiopia [16, 21, 41]. This is because untrimmed fingernails are difficult to clean and can harbours infective stages of parasites, serving as a reservoir for pathogens. The high prevalence of E. histolytica/dispar and G. lamblia among inmates may also be related to the high rate of untrimmed fingernails [21]. This underlines the importance of ensuring inmates have access to basic hygiene tools and receive education on personal grooming as part of infection control efforts.
Furthermore, this study shows that Inmates who slept in groups face a higher risk of IPIs. This increased risk is primarily due to crowded living conditions that facilitate close contact and environmental contamination, which promote parasite transmission [20]. Addressing overcrowding through improved prison infrastructure and management is therefore essential. Importantly, inmates with limited access to health education exhibited substantially higher odds of IPIs., This finding is consistent with studies in Cameroon [42] and Bolivia [43]. This highlights the crucial role of health education in managing and preventing parasitic infections. Lack of knowledge about transmission routes and preventive measures leads to poorer hygiene practices and increased susceptibility to infections. In environments like prisons, where access to information and resources is often restricted, the absence of health education can perpetuate the spread of parasites.
Limitations
A major limitation of this study was the inability to differentiate between E. histolytica (pathogenic) and E. dispar (non-pathogenic). Future studies should employ molecular techniques to clarify such distinctions. Additionally, the study had a low number of female participants, which may limit the generalizability of the findings. There is also potential for recall and information bias, as participants were interviewed about past experiences.
Conclusions and recommendations
The current moderate prevalence reveals that IPIs remain a significant health concern within prison settings, primarily associated with poor hygiene practices, low educational attainment, crowded living conditions, and limited access to health education. The predominant parasites identified in this study were E. histolytica, G. lamblia, Hookworm species, and A. lumbricoides.
IPIs can result in gastrointestinal illnesses, nutritional deficiencies, and a decline in overall health, potentially hindering their rehabilitation and quality of life. Therefore, empowering inmates through targeted health education programs is crucial to encourage better hygiene practices and reduce infection rates. These findings underscore the need to improve sanitation infrastructure by ensuring access to clean water and soap, promoting regular handwashing, and implementing regular health education tailored to inmates’ literacy levels. Additionally, adjusting sleeping arrangements to lessen crowding and establishing routine screening and treatment protocols are vital steps to mitigate the spread of infection effectively.
Multilateral collaboration among prison authorities, policymakers, and community organizations is essential for developing sustainable interventions and improving inmates’ health outcomes. Integrating prison health initiatives into national public health strategies will not only help manage IPIs within correctional facilities but also reduce their transmission to the wider community. Furthermore, employing a combination of diagnostic methods (FECT and Kato Katz) to improve infection detection and disease management. Future research should aim to validate these results in different settings.
Data availability
All data generated or analysed during this study are included in this published article.
Abbreviations
- AOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
- COR:
-
Crude odds ratio
- DWM:
-
Direct wet mount method
- EPG:
-
Egg per gram
- FECT:
-
Formol-ether concentration technique
- IPIs:
-
Intestinal parasite infection
- NPV:
-
Negative predictive value
- STHs:
-
Soil-transmitted helminths
- WHO:
-
World health organization
References
Cheesbrough M. District laboratory practice in tropical countries. Part 2. 2nd ed. Cambridge: Cambridge University Press; 2006.
Ahmed M. Intestinal parasitic infections in 2023. Gastroenterol Res. 2023;16:127.
Harp JA. Parasitic infections of the Gastrointestinal tract. Curr Opin Gastroenterol. 2003;19:31–6.
Muñoz-Antoli C, Irisarri-Gutiérrez MJ, Acosta L, Bonet MJ, Esteban JG, Toledo R. Intestinal parasitic infections and their potential risk factors among prison inmates in Valencia, Spain. BMC Infect Dis. 2023;23:616.
Gass K, Addiss DG, Freeman MC. Exploring the relationship between access to water, sanitation and hygiene and soil-transmitted helminth infection: a demonstration of two recursive partitioning tools. PLoS Negl Trop Dis. 2014;8:e2945.
Ghenghesh KS, Ghanghish K, BenDarif ET, Shembesh K, Franka E. Prevalence of Entamoeba histolytica, Giardia lamblia, and Cryptosporidium spp. in Libya: 2000–2015. Libyan J Med. 2016;11:1–6.
World Health Organization. Global distribution and prevalence of soil-transmitted helminth infections. Geneva: World Health Organization key fact sheet; 2020.
Dupouy-Camet J. In: Bruschi F, editor. Helminth infections and their impact on global public health. Vienna: Springer; 2014. pp. 229–79.
DiNardo A. Helminth infections and their impact on global public health. Clin Infect Dis. 2015;60:675–675.
Workineh L, Almaw A, Eyayu T. Trend analysis of intestinal parasitic infections at Debre Tabor comprehensive specialized Hospital, Northwest Ethiopia from 2017 to 2021: a five-year retrospective study. Infect Drug Resist. 2022;15:1009–18.
Kadio KJ, et al. Factors associated with intestinal parasites in the central prison of Conakry, Guinea. PAMJ-One Health. 2021;6:10.
Alves da Costa F, et al. The WHO prison health framework: a framework for assessment of prison health system performance. Eur J Public Health. 2022;32:565–70.
Karagiannis-Voules DA, et al. Spatial and Temporal distribution of soil-transmitted helminth infection in sub-Saharan africa: a systematic review and Geostatistical meta-analysis. Lancet Infect Dis. 2015;15:74–84.
Zida A, et al. Prevalence of intestinal parasitism in prisons in Ouagadougou. Burkina Faso Trop Med Health. 2014;24:383–7.
Mamo H. Intestinal parasitic infections among prison inmates and tobacco farm workers in Shewa Robit, North-Central Ethiopia. PLoS ONE. 2014;9:e99559.
Terefe B, Zemene E, Mohammed AE. Intestinal helminth infections among inmates in Bedele prison with emphasis on soil-transmitted helminths. BMC Res Notes. 2015;8:1.
Shrestha P, Shrestha D, Magar DT, Rai G, Rai KR, Rai SK. Intestinal parasitic infections among prison inmates in Kathmandu, Nepal. J Nepal Health Res Counc. 2019;17:382–7.
Liyih M, Damtie D, Tegen D. Prevalence and associated risk factors of human intestinal helminths parasitic infections in ethiopia: a systematic review and meta-analysis. Sci World J. 2022;1:3905963.
Federal Democratic Republic of Ethiopia Ministry of Health. National Neglected Tropical Diseases Master Plan, 2nd edn. Ethiopia. 2016.
Ameya G, et al. Intestinal parasite infections and associated factors among inmates of Arba minch prison, Southern ethiopia: cross sectional study. BMC Infect Dis. 2019;19:1.
Mardu F, Yohannes M, Tadesse D. Prevalence of intestinal parasites and associated risk factors among inmates of Mekelle prison, Tigrai Region, Northern Ethiopia, 2017. BMC Infect Dis. 2019;19:1.
Assefa M, Eshetu T, Biruksew A. Therapeutic efficacy of chloroquine for the treatment of plasmodium Vivax malaria among outpatients at Hossana health care Centre, Southern Ethiopia. Malar J. 2015;14:1–8.
Addise T, Bedadi B, Regassa A, Wogi L, Feyissa S. Spatial variability of soil organic carbon stock in Gurje Subwatershed, Hadiya Zone, Southern Ethiopia. Appl Environ Soil Sci. 2022;1:5274482.
Rop DC, et al. Risk factors associated with intestinal parasitic infections among inmates of Kisii Prison, Kisii County, Kenya. BMC Res Notes. 2016;9:1.
World Health Organization Expert Committee. Prevention and control of schistosomiasis and soil-transmitted helminthiasis. World Health Organ Tech Rep Ser. 2002;912:1–63.
Hosmer DW, Jr, Lemeshow S, Sturdivant RX. Applied logistic regression. 3rd ed. Hoboken: Wiley; 2013.
Ughava J, Robinson O, Edet P. Prevalence of intestinal helminthiasis among prison inmates in Jos, Nigeria. Afr J Biol. 2016;5:238–42.
Amit D, Kiran T, Shashwati N. Prevalence of intestinal parasites and urinary pathogens among prison inmates in central jail of Bhopal. Indian J Microbiol Res. 2016;3:47.
Dessie A, et al. Intestinal parasitic infections and determinant factors among school-age children in ethiopia: a cross-sectional study. BMC Res Notes. 2019;12:1.
Mulugeta M, Tolossa D, Abebe G. Description of long-term climate data in Eastern and southeastern Ethiopia. Data Brief. 2017;12:26–36.
Nadabo C, et al. Status of intestinal parasites in inmates of a correctional facility, Jos, Nigeria. Niger J Parasitol. 2020;41:1.
Angal L, et al. Determining intestinal parasitic infections (IPIs) in inmates from Kajang Prison, Selangor, Malaysia for improved prison management. BMC Infect Dis. 2015;15:1.
Schule SA, et al. Ascaris lumbricoides infection and its relation to environmental factors in the Mbeya region of Tanzania, a cross-sectional, population-based study. PLoS ONE. 2014;9:e92032.
Curval LG, et al. Prevalence of intestinal parasites among inmates in Midwest Brazil. PLoS ONE. 2017;12:e0182248.
Eyayu T, et al. Prevalence, intensity of infection, and associated risk factors of soil-transmitted helminth infections among school children at Tachgayint Woreda, northcentral Ethiopia. PLoS ONE. 2022;17:e0266000.
Hailu T, Abera B. Performance evaluation of direct saline stool microscopy, formol ether concentration, and Kato Katz diagnostic methods for intestinal parasitosis in the absence of gold standard methods. Trop Doct. 2015;45:178–82.
Taye S. Comparison of Kato-Katz and Formol-ether concentration methods for the diagnosis of intestinal helminthic infections among school children of Wonji Shoa town, Eastern ethiopia: a school-based cross-sectional study. Am J Health. 2014;2:271–4.
Aschale Y, Worku L, Addisu A, Alemu M, Alemu A. Comparison of direct wet mount, Kato-Katz, and formol ether sedimentation technique for the diagnosis of hookworm infection in Debre Elias Woreda, Northwest Ethiopia. Trop Doct. 2021;51:170–4.
Glinz D, et al. Comparing diagnostic accuracy of Kato-Katz, Koga agar plate, ether-concentration, and FLOTAC for Schistosoma mansoni and soil-transmitted helminths. PLoS Negl Trop Dis. 2010;4:e754.
Eyayu T, et al. Prevalence of intestinal parasitic infections and associated factors among patients attending Sanja primary Hospital, Northwest ethiopia: an institutional-based cross-sectional study. PLoS ONE. 2021;16:e0247636.
Belete YA, Kassa TY, Baye MF. Prevalence of intestinal parasite infections and associated risk factors among patients of Jimma health center requesting stool examination, Jimma, Ethiopia. PLoS ONE. 2021;16:e0248260.
Kamga HL, et al. The impact of health education on the prevalence of faecal-orally transmitted parasitic infections among school children in a rural community in Cameroon. Pan Afr Med J. 2011;8:1.
Lastrucci V, et al. Effect of a health education intervention on intestinal parasitic infections in Bolivian children. Eur J Public Health. 2020;30:690.
Acknowledgements
We extend our gratitude to the technical team from the Hawassa University Teaching and Referral Hospital’s parasitology laboratory, data collectors, as well as the staff and inmates of Hossana Prison, for their invaluable collaboration and support.
Funding
The research was funded by Hawassa University; however, the university had no role in the study design, data collection, analysis, interpretation, or manuscript preparation.
Author information
Authors and Affiliations
Contributions
J.N. generated the idea, wrote the proposal, and managed both field and laboratory work. TL, P.D., and Y.G. provided expertise in the study design, revised the proposal, and supervised the research project. P.D. and J.N. were responsible for data analysis, interpretation, and drafting of the manuscript. All authors revised the manuscript and approved it for submission.
Corresponding author
Ethics declarations
Ethical approval
Ethical approval for this study was obtained from Hawassa University’s Institutional Review Board (Ref. No: IRB/176/15). Written informed consent was obtained from all participants aged 18 years and older. For inmates under the age of 18, assents were obtained from the minors themselves, and written informed consent was secured from a designated cell representative acting in loco parentis (as a guardian). The study details were thoroughly explained to participants in their native language to ensure comprehension. All study procedures were conducted in compliance with the ethical and regulatory principles outlined in the Declaration of Helsinki. Participation was entirely voluntary, with the right to decline questions or not to provide samples without any penalty. All collected data were anonymized and kept confidential, accessible only to the principal investigator. Participants found to be infected with parasites received appropriate treatment following national treatment guidelines.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Nigus, J., Lambiyo, T., G/Silassie, Y. et al. Prevalence and determinants of intestinal parasitic infections among prison inmates in Central Ethiopia. Trop Dis Travel Med Vaccines 12, 4 (2026). https://doi.org/10.1186/s40794-025-00283-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1186/s40794-025-00283-y