
Abstract
Background
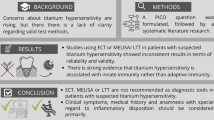
There is currently a lack of guidelines for clinicians regarding titanium hypersensitivity in implant dentistry. Diagnostic tests such as the epicutaneous test or the lymphocyte transformation test showed inconsistent results regarding reliability and validity and thus, evidence-based consensus recommendations regarding diagnostic and therapeutic options may be helpful in clinical decision-making. Therefore, the German S3 guideline on titanium hypersensitivity in implant dentistry was developed.
Findings
In the objectives, procedure, voting method and venue were defined and the consensus participants were invited. A systematic literature research was performed, and the overall quality of the evidence was rated according to the GRADE working group. Eight recommendations were formulated within the framework of a structured consensus conference under independent moderation and could be voted on with strong consensus (> 95% agreement). The formulated statements and recommendations were developed in small groups according to the guidelines of the Association of the Scientific Medical Societies in Germany (AWMF) and were discussed and agreed upon in the plenum.
Conclusions
For reasonable decision-making, a patient’s clinical symptoms should be regarded as leading parameters, which are usually expressed by a local inflammatory reaction with subsequent disturbed osseous integration. Allergy tests, such as the epicutaneous test or the lymphocyte transformation test are not helpful in titanium intolerance assessments, since these tests indicate T cell-mediated allergies, which are not observed in titanium intolerance reactions. Other metals and impurities that might be present in superstructures or alloys also need to be considered as the cause of an intolerance reaction and a trigger for contact sensitization. In the case of a suspected titanium particle-related, local immunologically induced inflammatory reaction with subsequent impaired osseous integration, dental ceramic implants can be considered as a therapeutic option.
Graphical Abstract

Similar content being viewed by others


Background
The demand for dental implants is continuously increasing due to the demographic change and an increasing esthetic and masticatory awareness within the population. However, with the increase in implantations, the number of cases with peri-implantitis is also increasing. With the development of the German S3 guideline on titanium hypersensitivity in implant dentistry, necessary recommendations regarding diagnostic and therapeutic options for patients with clinically suspicious intolerance reactions prior to and after implant insertion are provided as an evidence- and consensus-based decision support for dentists for the first time. The aim of this guideline was to determine in which cases patients would benefit from extended dermatological or laboratory-based diagnostics and how the clinical relevance of individual diagnostic findings and symptoms should be evaluated. The following PICO design was used: which effect does the insertion of a titanium dental implant (I) have in patients with and without metal allergy (P) compared to patients with ceramic implants or without implants (C) in terms of the development of a hypersensitivity reaction (O). A systematic literature search was performed, and the overall quality of the evidence was rated according to the GRADE working group. Randomized controlled trials were assessed according to the Cochrane Risk of Bias Tool I [1], cohort studies according to the Newcastle–Ottawa scale [2], and case series according to Moga et al. 2012 [3].
A total of eight recommendations were discussed and formulated in a structured consensus conference with an independent moderation. Strong consensus agreement was reached by > 95% of participants, consensus agreement by 75 to 95% of the participants, majority consensus agreement by 50 to 75% of participants and no consensus agreement by < 50% of the participants.
The formulated statements and recommendations were developed in small groups according to the guidelines of the Association of the Scientific Medical Societies in Germany (AWMF) and were afterwards discussed and agreed upon in the plenum.
A systematic review regarding diagnostic tests for titanium hypersensitivity was published by the authors and may be accessed for further background information regarding this topic [4].
Consensus statements
Predictive epicutaneous test (ECT) for titanium hypersensitivity
The ECT for the clarification of a potentially existing sensitization (referred to in the literature as prophetic testing) should not be performed (strong consensus/literature: [5, 6]/quality of evidence: moderate).
Background: The ECT, with which contact sensitization can be detected, plays a subordinate role for the question of titanium implant tolerance, due to its divergent pathophysiology compared to an allergy.
Predictive ECT for titanium hypersensitivity in patients with anamnestic allergic symptoms
The ECT should also not be performed in patients with a history of relevant previous diseases (strong consensus/literature: [5,6,7,8]/quality of evidence: low).
The ECT, which detects contact sensitizations, plays a subordinate role for the question of titanium implant tolerance, due to differences in pathophysiology compared to an allergy.
ECT in patients with clinical symptoms and suspected titanium hypersensitivity
The ECT should also not be performed in patients with suspected clinical intolerance (strong consensus/literature: [6, 7, 9]/quality of evidence: low).
The ECT, which can detect contact sensitization, plays a subordinate role for the question of titanium implant tolerance, since differences in the pathophysiology compared to an allergy are present.
Predictive lymphocyte transformation test (LTT) with regard to titanium
The LTT for the clarification of a potentially existing sensitization to titanium (referred to in the literature as prophetic testing) should not be performed (strong consensus/literature [10]/quality of evidence: low).
The LTT, which can detect an allergic reaction in vitro, plays a subordinate role for the question of titanium implant tolerance, since this is not an allergy in the classical sense from a pathophysiological point of view.
Predictive LTT regarding titanium in patients with anamnestic allergic symptoms
The LTT in relation to titanium should also not be performed in patients with a medical history of relevant previous diseases (strong consensus, literature: [10]/quality of evidence: low).
The LTT, which can detect an allergic reaction in vitro, plays a subordinate role for the question of titanium implant tolerance, due to differences in pathophysiology compared to an allergy.
LTT in patients with clinical symptoms and suspected titanium hypersensitivity
LTT should also not be performed in patients with suspected clinical intolerance to titanium (strong consensus/literature [10]/quality of evidence: low).
The LTT, which can detect an allergic reaction in vitro, plays a subordinate role for the question of titanium implant tolerance, since differences in the pathophysiology compared to an allergy are present.
Superstructures
Regarding hypersensitivity reactions in implant dentistry, it should be kept in mind that superstructures may cause hypersensitivity reactions or allergies. Other alloy components and impurities as well as adhesives should be considered as well (strong consensus/literature [11]/quality of evidence: low).
When discussing a metal allergy or titanium intolerance reaction, it must be kept in mind that endosseous implants are predominantly made of pure titanium (grade 4), but grade 5 titanium alloys and other alloys (metals) are also used, particularly in superstructures. An omission test can point the way to incompatibilities or allergies related to materials in superstructures. In the event of an allergic contact dermatitis of the oral mucosa to other prosthetic materials in implant alloys or superstructures (such as aluminum, vanadium, palladium or niobium, as well as nickel contamination) or other prosthetic materials in superstructures, such as cements or adhesives, LTT or ECT may be useful for differential diagnosis.
In vitro test methods should be considered, if epicutaneous testing is not possible for technical reasons (e.g., chronic generalized eczema) or if this would be too dangerous due to the toxicity of the substance, which should be taken into account for chemical substances (e.g., acrylates) that have been little investigated in this regard. In addition, the LTT has the advantage that an iatrogenic sensitization of the patient cannot take place, since the provocation with the allergen takes place in vitro and not within the patients skin [12].
Treatment options for patients with suspected titanium hypersensitivity reaction
For patients with suspected titanium intolerance, dental ceramic implants may be considered as a treatment option (strong consensus/literature: [9, 13, 14]/quality of evidence: low).
The indication for an explantation of a titanium implant should only be determined very strictly. The treatment of peri-implant biofilm-associated infections should initially be carried out in accordance with national guidelines. Since no ceramic products are available for orthodontic anchorage screws, conventional anchorage tools should be used and tissue contact should be kept as short as possible.
To date, titanium intolerance has not been adequately documented in the literature and valid diagnostic evidence is questionable. However, studies show evidence that the inflamed environment (peri-implantitis/mucositis) is associated with a higher peri-implant titanium particle load. Macrophage stimulation tests attempt to analyze this individual immune response in vitro. It has also been shown that patients have genetic predispositions with regard to their individual inflammatory reaction, which can be detected in genetic tests. Currently available tests can therefore only be regarded as useful indicative diagnostic tools. The clinical differentiation between a triggering bacterial inflammation and possible immunological inflammation due to titanium particles is not yet distinguishable with strong evidence.
Conclusion
For reasonable therapeutic decisions, clinical symptoms should be regarded as leading parameters, which are expressed by a local inflammatory reaction with subsequent disturbed osseous integration. Tests for the detection of type IV sensitizations, such as the ECT or the LTT, are not recommended since these tests indicate T cell-mediated allergies, which titanium intolerance does not represent. Furthermore, these tests are not target-specific in implant dentistry since titanium particle-induced peri-implant inflammation is a nonspecific immune activation. However, a specific immunological reaction in the sense of sensitization can be triggered by other metals used in titanium alloys, by impurities of the implant surface or in metal alloys of abutments and superstructures.
According to national guidelines, peri-implantitis treatment should be performed and the explantation of a dental implant should be regarded as ultimate option. Dental ceramic implants can be considered as a therapeutic option.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Change history
11 February 2023
Missing Open Access funding information has been added in the Funding Note
References
Higgins JPT, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928.
Wells G, Shea B, O'Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle–Ottawa Scale (NOS) for assessing the quality of non-randomized studies in meta-analysis. 2000.
Carmen Moga BG, Schopflocher D, Harstall C. Development of a quality appraisal tool for case series studies using a modified Delphi technique. 2012.
Müller-Heupt LK, Schiegnitz E, Kaya S, Jacobi-Gresser E, Kämmerer PW, Al-Nawas B. Diagnostic tests for titanium hypersensitivity in implant dentistry: a systematic review of the literature. Int J Implant Dent. 2022;8(1):29.
Sicilia A, Cuesta S, Coma G, Arregui I, Guisasola C, Ruiz E, et al. Titanium allergy in dental implant patients: a clinical study on 1500 consecutive patients. Clin Oral Implants Res. 2008;19(8):823–35.
Sun Y, Hu Y, Yuan Q, Yu J, Wu X, Du Z, et al. Association between metal hypersensitivity and implant failure in patients who underwent titanium cranioplasty. J Neurosurg. 2018;131(1):40–6.
Muller K, Valentine-Thon E. Hypersensitivity to titanium: clinical and laboratory evidence. Neuro Endocrinol Lett. 2006;27(Suppl 1):31–5.
Hosoki M, Nishigawa K, Tajima T, Ueda M, Matsuka Y. Cross-sectional observational study exploring clinical risk of titanium allergy caused by dental implants. J Prosthodont Res. 2018;62(4):426–31.
Vrbova R, Podzimek S, Himmlova L, Roubickova A, Janovska M, Janatova T, et al. Titanium and other metal hypersensitivity diagnosed by MELISA® test: follow-up study. Biomed Res Int. 2021;2021:5512091.
Jacobi-Gresser E, Huesker K, Schütt S. Genetic and immunological markers predict titanium implant failure: a retrospective study. Int J Oral Maxillofac Surg. 2013;42(4):537–43.
Syed M, Chopra R, Sachdev V. Allergic reactions to dental materials-a systematic review. J Clin Diagn Res. 2015;9(10):Ze04-9.
Lochmatter P, Zawodniak A, Pichler WJ. In vitro tests in drug hypersensitivity diagnosis. Immunol Allergy Clin N Am. 2009;29(3):537–54.
Osman RB, Swain MV, Atieh M, Ma S, Duncan W. Ceramic implants (Y-TZP): are they a viable alternative to titanium implants for the support of overdentures? A randomized clinical trial. Clin Oral Implant Res. 2014;25(12):1366–77.
Siddiqi A, Payne AGT, De Silva RK, Duncan WJ. Titanium allergy: could it affect dental implant integration? Clin Oral Implants Res. 2011;22(7):673–80.
Acknowledgements
Not applicable.
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
LKM-H, ES, SK, EJ-G, PWK and BA-N: drafting the work or revising it critically for important intellectual content, final approval of the version to be published: LKM-H, ES, SK, EJ-G, PWK and BA-N. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
There are no commercial or other associations that might create a duality of interests in connection with the short communication. Lena Katharina Müller-Heupt declares that she has no conflict of interest. Eik Schiegnitz reports lectures, personal fees, and/or grants from Dentsply, Geistlich, Medartis, Septodont, and Straumann not related to the present work. Sebahat Kaya declares no conflict of interest. Elisabeth Jacobi-Gresser declares no conflict of interest. Bilal Al-Nawas reports lectures, personal fees, and/or grants from Camlog, Dentsply, Geistlich, Medartis, Straumann, and Zimmer not related to the present work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Müller-Heupt, L.K., Schiegnitz, E., Kaya, S. et al. The German S3 guideline on titanium hypersensitivity in implant dentistry: consensus statements and recommendations. Int J Implant Dent 8, 51 (2022). https://doi.org/10.1186/s40729-022-00451-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40729-022-00451-1