
Abstract
Purpose
We aimed to histologically evaluate the influence of bone materials used during guided bone regeneration (GBR) on subsequent peri-implantitis in an experimental ligature-induced peri-implantitis model in beagle dogs.
Methods
Bilateral mandibular premolars (PM2-4) were extracted from six beagle dogs. After 3 months, standardized bone defects (3 mm [mesio-distal width] × 2 mm [bucco-lingual width] × 3 mm [depth]) were created in the experimental group, with simultaneous dental implant placement at the center of the defects. The defects were randomly filled with either autograft (AG) or deproteinized bovine bone mineral (DBBM) and covered with a collagen membrane. In the control group, implant fixtures were placed without creating an intrabony defect. After 3 months, a healing abutment was placed. Four weeks later, a 3–0 silk thread was ligated around the implants to induce peri-implantitis. After 4 weeks, the specimens were dissected and histologically examined.
Results
There were no clinical findings of inflammation until silk thread ligation. Four weeks after the onset of peri-implantitis, gingival redness and swelling were seen with mild resorption of the peri-implant bone on dental radiographs. There were no significant differences between the AG, DBBM, and control groups for the following parameters: bone-to-implant contact, distance from the implant shoulder to the base of the bone defect, area of bone defect, and area of new bone.
Conclusions
Within the limitations of this study, it can be concluded that peri-implant tissues after GBR using AG and DBBM underwent the same degree of bone resorption by peri-implantitis as the no defect group.
Similar content being viewed by others

Background
Placement of dental implants in the ideal three-dimensional position is important to achieve predictable functional and esthetic restoration [1, 2]. Following tooth extraction as a pre-procedure to implant treatment, the volume of the residual bone decreases, as is represented by buccal bone loss, due to alveolar bone remodeling [3, 4]. Horizontal and vertical bone resorption of up to 29–63% and 11–22%, respectively, has been reported within 6 months after tooth extraction [5]. Bone loss at the implant site is a risk factor for bone resorption after implant placement [6, 7].
Various bone regenerative techniques are effective in improving implant survival rates and have been used to achieve long-term success [8, 9]. Guided bone regeneration (GBR) is an established technique for the horizontal and vertical augmentation of the ridge volume with long-term stability [10].
Bone graft materials, including autograft (AG), deproteinized bovine bone mineral (DBBM), allograft, and alloplast, have been applied in GBR [11]. Among them, only AG possesses all three properties of osteogenesis, osteoinduction, and osteoconduction, and is therefore considered the gold standard [7, 12, 13]. However, the use of other bone grafts is increasing in clinical practice due to the problems associated with autografts, including greater invasiveness of the procedure to obtain the graft from the donor site and the limited quantity of the graft that can be harvested [12]. The effectiveness of DBBM for vertical and horizontal bone augmentation due to its osteoconductive property, has been reported. However, it is not osteoinductive [14] and resorbs poorly in tissues, with an unknown rate of resorption [15].
Peri-implantitis is one of the complications of implant therapy. According to the 2008 consensus report by the 6th European Workshop on Periodontology, 28–56% of patients treated with implants develop peri-implantitis in 1 year of implant placement [16]. In 2017, Ogata et al. reported the development of peri-implantitis in 9.7% of 267 Japanese patients 3 years after implant placement [17].
Therefore, prevention of peri-implantitis is important, and plaque control is an effective method to reduce its incidence [18]. However, since there are concerns that reduced plaque control is a result of decreased salivary volume and function associated with physical conditions, such as aging [19, 20], the risk of peri-implantitis may be considered unavoidable. In addition, this risk persists even after treatment of the peri-implant tissues by GBR.
Although the use of various bone grafts has been reported for the treatment of peri-implantitis, it remains unclear whether the bone graft material used for ridge augmentation influences the development of subsequent peri-implantitis.
Kim et al. demonstrated the usefulness of a three-walled GBR experimental model in dogs as a reproducible model for periodontal regeneration [21], and the ligature-induced peri-implantitis model became the standard model for the study of the treatment and pathogenesis of peri-implantitis following the research by Schwarz et al. [22, 23, 24]. Nevertheless, an experimental model to study the influence of the bone graft on subsequently occurring peri-implant inflammation has not been established. Therefore, we adapted the established experimental models for this study. We performed histological examinations to determine if the bone graft material used for augmentation altered the progression and extent of subsequent peri-implant inflammation.
Methods
All procedures and protocols in this study were approved by the Institutional Animal Care and Use Committee of Tokyo Medical and Dental University (A2018-322A) (Fig. 1). Six healthy 1-year-old male beagle dogs were used in this experiment. All surgical procedures were performed under general and local anesthesia. Medetomidine hydrochloride (0.05 mL/kg, Domitor®; Orion Corporation, Espoo, Finland) was administered intramuscularly as premedication. Spontaneous respiration was maintained by intravenous injection of sodium thiopental (0.005 mL/kg, Ravonal®; Mitsubishi Tanabe Seiyaku Co., Osaka, Japan). Lidocaine hydrochloride (2%, 1:80,000 epinephrine, Xylocaine; Fujisawa Pharmaceutical Co., Osaka, Japan) was administered as local anesthesia.

Diagram of experimental design protocol
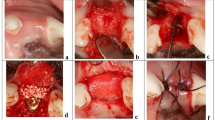
Bilateral mandibular second, third, and fourth premolars in the beagles were extracted to provide sufficient space for dental implant placement. After 12 weeks of spontaneous healing, mucoperiosteal flaps extending from the first premolar to the first molar were elevated along the crest of the alveolar ridge. The alveolar crest was flattened by a periodontal chisel (Jovanovic; Hu-Friedy, Chicago, IL, USA) to obtain sufficient bone width for the experiment. The bone harvested during this process was collected for use as an AG. In the experimental group, standardized bone defects (2 mm buccal-lingual width × 3 mm mesio-distal width × 3 mm depth) were surgically created on the planned implant site. After the creation of these defects, bone-level implant fixtures (Straumann φ3.3 mmNC, SLA®8 mm, Roxolid®) were placed at the center of the defects (Fig. 2a). The intrabony defects were filled with either AG or DBBM (Bio-Oss®; Geistlich Pharma., Switzerland) (Fig. 2b). In the control group, implant fixtures were placed without creating an intrabony defect first. The experimental groups and the control group were designated randomly by random function (Microsoft Excel 2011; Microsoft Corporation, Redmond, WA, USA). After placing the cover screw (Straumann NC Closure cap φ2.8 mm, H 0 mm), an absorbable collagen membrane (Bio-Gide®; Geistlich Pharma., Switzerland) was placed in the experimental groups. The flaps were repositioned and immobilized using sutures (Gore-Tex® CV-6 Suture; W.L. Gore & Associates, Inc., Newark, DE, USA). After the surgical procedures, an antibiotic (Penicillin G; Meiji Seika Pharma Co., Ltd, Tokyo, Japan) and an analgesic agent (Vetorphale; Meiji Seika Pharma Co., Ltd, Tokyo, Japan) were administered intramuscularly. After 2 weeks of healing, the sutures were removed. The surgical site was rinsed with a 2% solution of chlorhexidine (HiBiTane® concentrate; Sumitomo Seiyaku Co., Ltd., Osaka, Japan) three times a week for 12 weeks.

Surgical procedures. a Intrabony defects (3 mm [mesio-distal width] × 2 mm [bucco-lingual width] × 3 mm [depth]) were created and implants were placed at their center. b Left-sided defects were filled with deproteinized bovine bone minerals. Right-sided defects were filled with autograft. cTwelve weeks after implant placement, the cover screw was removed and the healing abutment was placed. d Four weeks after placing the healing abutment, a 3–0 silk ligature was placed. e Four weeks after placing the ligature to induce peri-implantitis, plaque accumulation and gingival redness were observed
Twelve weeks after implant placement, the position of each implant fixture was confirmed by bone sounding, and the gingiva over the cover screw was removed. The cover screw was replaced by the healing abutment (Straumann NC conical shape, φ4.8 3.5 mm) (Figs. 2c).
After 4 weeks of healing, 3–0 silk ligatures (Blade silk; Hashimoto Co., Ltd., Tokyo, Japan) were placed in the peri-implant sulcus (Fig. 2d). The remaining ligature thread was checked, and dental radiographs were taken once a week to confirm bone resorption around the implant. Four weeks after ligation, the beagles were euthanized by an overdose of intravenous thiopental. The mandibules containing all surgical sites were dissected into blocks and fixed in 10% neutral buffered formaldehyde (Mild form® 10 N; Wako Pure Chemical industries) for morphological and histological evaluation. One experienced surgeon (T.M.) performed all surgical procedures in this experiment.
Radiographic analysis
The height of the alveolar bone around the implant fixture at the time of ligature placement and 4 weeks after ligation was compared on radiographs. The difference in the height was defined as the length of bone loss. In all groups, the length of bone loss was represented the average of the mesial and distal measurements. The ratio of the length of bone loss to the length of the implant fixture was calculated.
Histological analysis
The tissue blocks containing the implant were fixed in 10% formaldehyde solution (Mildform® 10 N; Wako Pure Chemical Industries, Ltd.), followed by dehydration with ethanol solutions of different concentrations, which were replaced with acetone. After further treatment with methylmethacrylate (MMA) solution, the specimens were embedded in MMA resin, polished into 30–40 μm thick non-demineralized sections, and stained with toluidine blue.
Histological examination was done using an optical microscope (ECLIPSE Ni-U; Nikon Corporation, Tokyo, Japan). Histological measurements were performed using a computerized imaging system consisting of a high-definition color camera head (DS-Fi2; Nikon Corporation, Tokyo, Japan). The following parameters were measured by the same experienced and blinded examiner (T.A.). Intra-examiner reproducibility was ensured by the examiner reading 18 sections from all sites and repeating the same procedure 24 h later. Calibration was accepted at 90% level.
Bone-to-implant contact (BIC) was calculated as the percentage of implant-bone contact within the region of interest (ROI). An ROI was defined as the same area of the bone defect (3 mm mesio-distal width × 3 mm depth). The percentage of new bone and bone defect areas in the ROI were calculated. All reported parameters represented the average of the mesial and distal measurements. These items were measured using image analysis software (ImageJ v.1.43u; National Institutes of Health, Bethesda, MD, USA).
The following parameters were evaluated for all specimens:
-
BIC (%): bone contact percentage of the implant body length in the ROI
-
First BIC (fBIC, mm): distance from IS to first bone-to-implant contact
-
Area of bone loss (mm2): the area from the implant shoulder (IS) to the base of the defect
-
Area of new bone (mm2): amount of new bone formation calculated from the base of the defect.
Statistical analysis
Means and standard deviations for each parameter were calculated for each group, and statistical analysis for each group was performed using analysis of variance (Microsoft Excel 2011; Microsoft Corporation, Redmond, WA, USA). The level of significance was set at P < 0.05. The data are expressed as mean ± SD.
Difference in the area of new bone between the AG and DBBM groups was assessed with the paired t-test, and a p-value < 0.05 was considered statistically significant.
Results
Clinical observations
No flap necrosis or wound dehiscence was observed during the 12 weeks after implant placement. The residual bone grafts were not exposed at any of the experimental sites. Healing occurred uneventfully at all sites in all groups. All implants achieved good primary stability at the time of installation. There was no loss of implants during the experiment. Four weeks after ligation, plaque deposition and gingival redness were observed around the implants (Fig. 2e).
Radiographic observations
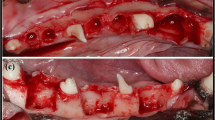
At the time of insertion of the 3–0 silk thread, the heights of the alveolar bone and IS were comparable in all groups (Fig. 3a). There was no continuous radiolucency around the implants. No bone graft was identified in the AG and DBBM groups. Four weeks later, the bone level of the alveolar ridge in all groups was below IS (Fig. 3b). The average bone loss relative to the implants was 14.3 ± 0.9% in the control group, 13.6 ± 1.9% in the AG group, and 14.8 ± 2.1% in the DBBM group, and there was no statistically significant difference (Fig. 3c).

Dental radiographs and graphics representing the average bone loss relative to the implants on the radiographs. a Four weeks after placing the healing abutment. Yellow arrows represent the bottom of bone loss. b Four weeks after insertion of the ligature. Yellow arrows represent the bottom of bone loss. c Graphic about the average bone loss in all groups. There was no statistically significant difference used by the analysis of variance
Histological observations
Shallow circumferential bone loss around implants was observed in all groups. No fibrous tissue intervention was found around the implants (Fig. 4).

Photomicrograph of a region of interest (Toluidine blue). a–c Original magnification view (Scale bar = 500 μm). The area inside the yellow box indicates the region of interest. d–f The white boxed depicts the tissue under high magnification (× 20, Scale bar = 50 μm). a, d Control, b, e autograft, and c, f deproteinized bovine bone mineral groups. *Residual bone graft
Compared to the control group, the bone distribution around the implants in the AG group was sparse. The boundary between new bone, AG, and original bone was unclear. (Fig. 4a, b).
In the AG group, residual bone graft was not observed. The AG had been replaced by alveolar bone (Fig. 4b, e). Residual bone grafts of DBBM were found within the ROI and encased in bone tissue (Fig. 4c, f).
Histometric analyses
No significant differences in bone defect area, new bone area, BIC, and fBIC were observed between the control, AG, and DBBM groups (Table 1). Although there was no statistically significant difference, there was a tendency for the DBBM group to have a lower BIC and a higher fBIC.
The area of bone loss was greater in the AG and DBBM groups than in the control group.
The area of new bone area was greater in the AG group than in the DBBM group. But there was no statistically significant difference (P = 0.056) (Table 2).
Discussion
This study histologically investigated the influence of different bone grafts (AG and DBBM) on peri-implant inflammation after GBR. Schwarz et al. demonstrated that peri-implantitis progresses faster than periodontitis because of the structural differences between the periodontal and peri-implant tissues [25]. Hämmerle et al. reported that the survival rate of implants placed at grafted sites was similar to that of implants not requiring guided bone regeneration [26]. However, it is unclear if the graft used for ridge augmentation with GBR can influence subsequent peri-implant inflammation.
To our knowledge, this is the first study to histologically evaluate the inflammation in peri-implant tissues regenerated by GBR; therefore, we combined the previous GBR model with the experimental peri-implantitis model.
This study compared the effect of inflammation on the AG and DBBM grafted concomitantly as implant placement in comparison with that in the control group. Therefore, no bone defect was created in the control group. The size of the bone defect to be fabricated was small because the bone height needed to be comparable in all groups before induction of peri-implantitis. In fact, the dental radiographs acquired before peri-implantitis induction showed that the bone levels were similar in height in all the groups.
In previous studies, active breakdown of ligature-induced peri-implantitis has been reported over a mean period of 12.0 ± 5.0 weeks, with a mean bone loss of 41.6 ± 16.1% relative to the implant length [22, 27]. Compared to these previous reports, the ligation period in the present study was shorter and the amount of bone resorption observed was lesser. In this study, a bone resorption of 40% of the 8-mm-long implant could result in a greater extent of resorption than that with the original 3-mm-deep bone defect. As a result, it could be difficult to assess the effect of inflammation-induced bone resorption on the area where the bone substitute was implanted. Therefore, in this study, the ligation period was scheduled to be shorter than that in previous studies to ensure that the extent of bone resorption would not exceed the implanted bone substitute [22, 27].
Some studies reported that DBBM particles can induce the expression of multinucleated giant cells, or stimulate the formation of fibrous tissue [28,29,30]. In other studies, DBBM particles were not absorbed under inflammatory conditions [28, 31]. In the present study, residual DBBM granules were observed in the DBBM group, confirming the insolubility of DBBM, as reported by Handschel et al. [15] (Fig. 4). Multinucleate giant cells were not observed around the DBBM granules in the histological sections.
Encapsulation by fiber tissue occurs in response to foreign bodies [29]. If the graft is not encapsulated in soft tissue, GBR is considered successful [29, 32]. In this study, since encapsulation was not observed, we considered GBR to be successful. After DBBM was surrounded by new bone, the progress of bone resorption was same as that of the native bone.
Comparing the BIC in the control and AG groups, there was lower BIC in the DBBM group. However, the difference was not statistically significant. Santis et al. reported that BIC tended to be lower in the DBBM group than the AG group, but there was no significant difference [33]. Other studies reported that bone resorption in areas augmented by AG was unpredictable and could vary between 12 and 80% [34]. Since DBBM particles are stable and induce bone formation in the long term, DBBM may be more advantageous for the long-term prognosis [35]. It was suggested that the use of DBBM in combination with AG may improve the stability of the graft [34]. However, it has been reported that bone at the bone-implant interface has weak mechanical properties due to its low mineral content [36]. Compared to the control and AG groups, the DBBM group tended to have a larger area of bone loss and fBIC, which could be influenced by the mineral content. GBR using AG or DBBM may be an effective treatment in terms of resistance of peri-implantitis.
The DBBM group showed a tendency to show lower results for all parameters compared to the other groups; however, the difference was not significant. It is thought that the residual granules of DBBM did not influence the degree of bone resorption due to inflammation as a sufficient healing period was provided after GBR. This suggests that the long-term prognosis of inflammation is not dependent on the bone graft used for GBR. In this study, peri-implantitis was not induced immediately after GBR, so it is unclear whether inflammation generated during bone regeneration affects DBBM. To investigate the influence of inflammation on bone graft materials, further research is needed to determine the short-term prognosis.
Further investigation of the inflammation in peri-implant tissues after GBR using different bone grafts, such as allografts and alloplasts, is needed.
In this study, there was no difference in the bone resorption by the inflammation occurring in the AG and DBBM groups compared to control group, indicating the usefulness of DBBM with regard to good availability of the graft without requiring invasive procedures.
Conclusion
Within the limitations of this study, it can be concluded that peri-implant tissues after GBR using AG and DBBM underwent the same degree of bone resorption by peri-implantitis as the no defect group.
Availability of data and materials
All data generated or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AG:
-
Autograft
- DBBM:
-
Deproteinized bovine bone mineral
- BIC:
-
Bone-to-implant contact
- fBIC:
-
First BIC
- GBR:
-
Guided bone regeneration
- ROI:
-
Region of interest
References
Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004;19(Suppl):43–61.
Howell TH, Fiorellini J, Jones A, et al. A feasibility study evaluating rhBMP-2/absorbable collagen sponge device for local alveolar ridge preservation or augmentation. Int J Periodont Restor Dent. 1997;17:124–39.
De Santis E, Botticelli D, Pantani F, et al. Bone regeneration at implants placed into extraction sockets of maxillary incisors in dogs. Clin Oral Implants Res. 2011;22:430–7.
Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005;32:212–8.
Tan WL, Wong TL, Wong MC, et al. A systematic review of post-extractional alveolar hard and soft tissue dimensional changes in humans. Clin Oral Implants Res. 2012;23(Suppl 5):1–21.
French D, Grandin HM, Ofec R. Retrospective cohort study of 4,591 dental implants: analysis of risk indicators for bone loss and prevalence of peri-implant mucositis and peri-implantitis. J Periodontol. 2019;90:691–700.
Sudarsan S, Arun KV, Priya MS, et al. Clinical and histological evaluation of alloderm GBR and BioOss in the treatment of Siebert’s class I ridge deficiency. J Indian Soc Periodontol. 2008;12:73–8.
Wang HL, Al-Shammari K. HVC ridge deficiency classification: a therapeutically oriented classification. Int J Periodont Restor Dent. 2002;22:335–43.
Mellonig JT, Nevins M. Guided bone regeneration of bone defects associated with implants: an evidence-based outcome assessment. Int J Periodont Restor Dent. 1995;15:168–85.
Li H, Zheng J, Zhang S, et al. Experiment of GBR for repair of peri-implant alveolar defects in beagle dogs. Sci Rep. 2018;8:16532.
Mittal Y, Jindal G, Garg S. Bone manipulation procedures in dental implants. Indian J Dent. 2016;7:86–94.
Sheikh Z, Najeeb S, Khurshid Z, et al. Biodegradable materials for bone repair and tissue engineering applications. Materials (Basel). 2015;8:5744–94.
Sheikh Z, Hamdan N, Ikeda Y, et al. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: a review. Biomater Res. 2017;21:9.
Hämmerle CH, Chiantella GC, Karring T, et al. The effect of a deproteinized bovine bone mineral on bone regeneration around titanium dental implants. Clin Oral Implants Res. 1998;9:151–62.
Handschel J, Simonowska M, Naujoks C, et al. A histomorphometric meta-analysis of sinus elevation with various grafting materials. Head Face Med. 2009;5:12.
Lindhe J, Meyle J. Periodontology GDoEWo. Peri-implant diseases: consensus report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008;35:282–5.
Ogata Y, Nakayama Y, Tatsumi J, et al. Prevalence and risk factors for peri-implant diseases in Japanese adult dental patients. J Oral Sci. 2017;59:1–11.
Jepsen S, Berglundh T, Genco R, et al. Primary prevention of peri-implantitis: managing peri-implant mucositis. J Clin Periodontol. 2015;42(Suppl 16):S152-157.
Pedersen W, Schubert M, Izutsu K, et al. Age-dependent decreases in human submandibular gland flow rates as measured under resting and post-stimulation conditions. J Dent Res. 1985;64:822–5.
Wilkinson DJ, Piasecki M, Atherton PJ. The age-related loss of skeletal muscle mass and function: measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res Rev. 2018;47:123–32.
Kim CS, Choi SH, Chai JK, et al. Periodontal repair in surgically created intrabony defects in dogs: influence of the number of bone walls on healing response. J Periodontol. 2004;75:229–35.
Schwarz F, Sculean A, Engebretson SP, et al. Animal models for peri-implant mucositis and peri-implantitis. Periodontol. 2000;2015(68):168–81.
de Molon RS, Park CH, Jin Q, et al. Characterization of ligature-induced experimental periodontitis. Microsc Res Tech. 2018;81:1412–21.
Martins O, Ramos JC, Baptista IP, et al. The dog as a model for peri-implantitis: a review. J Invest Surg. 2014;27:50–6.
Schwarz F, Herten M, Sager M, et al. Comparison of naturally occurring and ligature-induced peri-implantitis bone defects in humans and dogs. Clin Oral Implants Res. 2007;18:161–70.
Hämmerle CH, Jung RE, Feloutzis A. A systematic review of the survival of implants in bone sites augmented with barrier membranes (guided bone regeneration) in partially edentulous patients. J Clin Periodontol. 2002;29(Suppl 3):226–31 (discussion 232-223).
Schwarz F, Sager M, Becker J. Peri-implantitis defect model. In: Giannobile WV, Nevins M, editors. Osteology guidelines for oral and maxillofacial regeneration: preclinical models for translational research. Quintessenz: Schweizerland; 2012. p. 197–224.
Carmagnola D, Berglundh T, Araújo M, et al. Bone healing around implants placed in a jaw defect augmented with Bio-Oss. An experimental study in dogs. J Clin Periodontol. 2000;27:799–805.
Busenlechner D, Tangl S, Arnhart C, et al. Resorption of deproteinized bovine bone mineral in a porcine calvaria augmentation model. Clin Oral Implants Res. 2012;23:95–9.
Barbeck M, Udeabor SE, Lorenz J, et al. Induction of multinucleated giant cells in response to small sized bovine bone substitute (Bio-Oss™) results in an enhanced early implantation bed vascularization. Ann Maxillofac Surg. 2014;4:150–7.
Kuchler U, Dos Santos GM, Heimel P, et al. DBBM shows no signs of resorption under inflammatory conditions. An experimental study in the mouse calvaria. Clin Oral Implants Res. 2020;31:10–7.
Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials. Semin Immunol. 2008;20:86–100.
De Santis E, Lang NP, Cesaretti G, et al. Healing outcomes at implants installed in sites augmented with particulate autologous bone and xenografts. An experimental study in dogs. Clin Oral Implants Res. 2013;24:77–86.
Mordenfeld A, Johansson CB, Albrektsson T, et al. A randomized and controlled clinical trial of two different compositions of deproteinized bovine bone and autogenous bone used for lateral ridge augmentation. Clin Oral Implants Res. 2014;25:310–20.
Aludden HC, Mordenfeld A, Hallman M, et al. Lateral ridge augmentation with Bio-Oss alone or Bio-Oss mixed with particulate autogenous bone graft: a systematic review. Int J Oral Maxillofac Surg. 2017;46:1030–8.
Johnson TB, Siderits B, Nye S, et al. Effect of guided bone regeneration on bone quality surrounding dental implants. J Biomech. 2018;80:166–70.
Acknowledgements
The data were fully controlled by the authors, and no commercial input was obtained during study preparation. The authors report no conflicts of interest related to this study.
Funding
This research was supported by JSPS KAKENHI Grant Numbers JP18K17095, JP 19K19046, JP19K24063, JP20K18571.
Author information
Authors and Affiliations
Contributions
T. M. conceived the study design. R.S., T.M., T.A., S.F., M.O., K.N., S.T., S.H., W.O. and K.M. did the animal experiment. R.S., T.M., S.F., M.O. performed data acquisition and analysis. R.S. drafted the manuscript. R.S., T.M., S.F., M.O., Y.I. and T.I. revised the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This animal experiment was approved by the Bioethics Committee of Tokyo Medical and Dental University(A2018-322A).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sato, R., Matsuura, T., Akizuki, T. et al. Influence of the bone graft materials used for guided bone regeneration on subsequent peri-implant inflammation: an experimental ligature-induced peri-implantitis model in Beagle dogs. Int J Implant Dent 8, 3 (2022). https://doi.org/10.1186/s40729-022-00403-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40729-022-00403-9