
Abstract
Sexual health is important to the self worth, emotional well being, and overall quality of life of women in midlife. However, urinary incontinence, which is prevalent in this population, has a negative impact on sexual function. The purpose of this article is to review the impact of urinary incontinence on female sexual dysfunction and discuss the impact of urinary incontinence treatment on sexual function. We carried out a literature review on the effect of stress urinary incontinence and urgency urinary incontinence on sexual health and physiological response, including coital incontinence, satisfaction, desire, orgasm, frequency, and partner relationships. We examined the literature regarding changes in sexual function related to non-surgical and surgical interventions for incontinence. Overall, though studies are lacking and of poor quality, treatment of incontinence has been shown to improve sexual function. Both pelvic muscle training and midurethral slings have been shown to improve sexual function in those with stress urinary incontinence. In urgency urinary incontinence, evidence indicates improvement in sexual function after treatment with anti-muscarinic medications. Coital incontinence commonly improves with treatment of the underlying incontinence subtype. Although problems related to sexual health are complex and involve both psychological and physical factors, it is important to consider treatment of urinary incontinence as part of management of sexual dysfunction.
Similar content being viewed by others


Introduction
Urinary incontinence (UI) is a common condition, with reported prevalence ranging from 28 to 47 % in women during midlife [1, 2]. The risk of incontinence increases incrementally from the age of 40 to 60, with prevalence nearly doubled by age 55 [3]. Common types of incontinence include stress incontinence (urinary leakage with activity that increase intra-abdominal pressure), urgency urinary incontinence (leakage related to urgency and irritative bladder symptoms associated with overactive bladder), and mixed incontinence (a combination of stress and urgency urinary incontinence). Stress urinary incontinence is the most common type of urinary incontinence, accounting for 52 - 65 % of urinary incontinence in women aged 30 to 60 [4]. Treatment of stress UI is primarily surgical, while urgency urinary incontinence, a common problem that may affect 20 % of middle-aged women [5], is mainly treated with non-surgical options. In those with mixed urinary incontinence, the most bothersome and dominant incontinence type is treated first. However, coital incontinence, the leakage of urine during sexual intercourse, may have the most impact on sexual health and commonly occurs in women with any type of incontinence, with an overall prevalence from 11 to 60 % in middle-aged women with UI [6].
UI, even when not directly associated with intercourse, plays an important role in altering behaviors of human sexual function. This is concerning, as sexual health is very important in the overall quality of life and is tied to a woman’s self worth, emotional well-being, and even cognitive function [7]. In a recent report, 86 % of women with urinary incontinence reported that sexual health was an important issue; however, few women with UI will discuss problems with sexual health unless directly asked [8]. Our aim is to review the impact of urinary incontinence on female sexual dysfunction and discuss the impact of urinary incontinence treatment on sexual health of women in midlife.
Given the rarity of major, high-level evidence with regards to UI, treatment, and its relationship to sexual health, we searched for any trials related to these topics, prioritizing randomized controlled trials and prospective studies. We conducted a wide and comprehensive literature search in Pubmed (up to December 2014) on any articles examining overall changes in sexual health (overall subject-described impact). Additionally, we looked for the impact of urinary incontinence and treatment on aspects of the sexual physiologic responses (frequency, libido, desire, arousal, lubrication, orgasm, satisfaction, pain). No date or language restriction was used. Questionnaires and questionnaire subdomains used by studies to evaluate changes in sexual health are briefly described in Table 1.
Review
Urinary incontinence and overall impact on sexual health
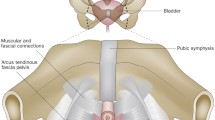
Because of the proximity of the bladder and urethra to the vagina and vulva, UI may have major effects on the sexual health of affected women. In clinic settings, incontinent middle-aged women commonly report disruption of sexual health with a median percentage of 28 % [9]. Complete abstinence from sex secondary to urinary incontinence can range from 5.9 to 38 %, a wide range owing to the diversity of the populations included in these studies [10–12]. Older women with urinary incontinence report decreased self-rated health and a greater incidence of depression [5], which may also affect sexual health. Women with UI show greater dysfunction on validated sexual function questionnaires compared to those without incontinence [13], regardless of menopausal status [14].
When examining sexual health in women with stress UI, older age, postmenopausal state, greater prolapse, and greater parity have been associated with worse sexual function scores [15]. The severity and duration of stress UI may not be associated with the level of sexual function [16, 17]. In patients with urgency UI, twenty-five percent of women with urgency UI report negative impacts on their sex life [18, 19]. Urgency UI is also significantly associated with lower self-esteem [20], which significantly influences sexual dysfunction [21].
Impact on the female sexual response
Severe UI has been found to be significantly associated with decreased libido and vaginal dryness [22], decreased interest, and decreased satisfaction with sexual intercourse, including orgasmic dysfunction [9].
In particular, women with stress UI have been noted to have problems with desire, arousal, and lubrication [23]. Decreased desire in these women may be related to unsatisfying partner relationship, worries about coital incontinence, and unsatisfying somatic health [21]. In spite of decreased sexual desire, a majority of women with stress UI (78 %) are able to achieve orgasm [16], and may not necessarily display decreased sexual activity [24]. Women with urgency UI similarly also report significant difficulty with hypoactive sexual desire, and arousal disorder; however, achieving orgasm is also difficult in this population [25–27]. In women with urgency UI, this results in decreased sexual activity [28] and decreased sexual satisfaction associated with urgency UI [2].
Dyspareunia, pain with intercourse, often accompanies UI and varies in prevalence from 8 to 42 % amongst middle-aged women with UI [9]. Studies have reported significantly greater rates of dyspareunia in women with UI and other lower urinary tract symptoms compared to controls [22, 25]. Dyspareunia has been noted more frequently in women with stress UI compared to those with overactive bladder [15]. However, dyspareunia does commonly accompany urgency UI [28, 29].
Impact on partners’ sexual health
UI also affects the sexual function of partners. Male partners of women with any type of UI report decreased overall sexual function, satisfaction, frequency of intercourse, and increased rates of erectile dysfunction as compared with partners of women without UI [30]. In spite of these negative effects, 42 % were unaware of the presence of coital incontinence. Of those who were aware, the majority (65 %) did not consider the UI to be the main problem affecting sexual health [21]. Negative effects on marital relationships have been correlated specifically with the presence of urgency UI [31].
Coital incontinence and impact on sexual health
Coital incontinence deserves particular focus as it is often directly associated with sexual dysfunction. Coital incontinence is prevalent in up to 56 % of middle-aged women with incontinence [9], and peaks around the age of 50, with subsequent decrease as women enter their sixth decade of life [32]. Risk factors for coital incontinence include severity of incontinence [33], obesity [34], parity [35], and anterior and posterior vaginal wall prolapse [35]. The severity of the coital incontinence may be associated with the degree of sexual dysfunction [35, 36].
The impact of coital incontinence on sexual function is multifold. Actual leakage during coitus can affect sexual satisfaction. However, worry about leakage also contributes, and is significantly associated with decreased sexual desire and sexual satisfaction [21]. Embarrassment, guilt and anxiety about sexual activities are highly prevalent in this population [37]. Arousal can be also compromised, as patients with coital incontinence have significantly greater issues with lubrication [37]. Dyspareunia may be increased in women with coital incontinence compared to those without urinary complaints [37]. Avoidance of intercourse specifically because of coital incontinence is common [37]. Among partners of women with coital incontinence, an association with increased ejaculation before reaching full erection was noted [37].
Coital incontinence may occur at any time during intercourse, but is most commonly noted during penetration and orgasm [21, 38], although it is also frequently reported during clitoral stimulation and arousal [21]. Coital incontinence during penetration is commonly associated with stress UI [35, 39–41], while detrusor spasms have been implicated in coital incontinence during orgasm [39, 42]. Coital incontinence resulting from stress UI during penetration may be due to the alteration of the urethrovesical angle and elevation of the bladder neck by the erect penis during moments of increased intra-abdominal pressure. The mechanism of urinary incontinence during orgasm is unclear. It is postulated that penile stimulation of the nerve rich area of the bladder base and trigone may trigger detrusor overactivity in those with severe overactive bladder [42]. Alternately, stimulation of the vanilloid receptors in this area, which are reportedly increased in density in patients with urgency, may trigger detrusor contractions [43]. However, other studies have found no relationship between timing of coital incontinence and stress UI, detrusor overactivity, or mixed urinary incontinence [38, 44]; and that regardless of timing of coital incontinence, stress UI was the most frequently diagnosed type of incontinence, while detrusor overactivity was uncommon [45].
The impact of treatment of urinary incontinence on sexual health
Treatment of incontinence includes both non-surgical and surgical modalities. Non-surgical treatment for stress UI includes pelvic muscle training (strengthening the levator ani muscles, the main support for the bladder during increased intra-abdominal pressure) [46], anti-incontinence pessaries, and transvaginal electrical stimulation. However, the treatment of stress UI is primarily surgical, and includes midurethral mesh slings, Burch colposuspension, and periurethral bulking injection (injection of bulking agents into the urethral wall to improve continence) [47]. Urgency UI is typically treated by non-surgical methods, including pelvic muscle training and biofeedback, transvaginal electrical stimulation, medication, percutaneous tibial nerve stimulation (involving stimulation of sacral plexus via the tibial nerve). Surgical therapies for urgency UI include botulinum toxin injection of the detrusor muscle and sacral neuromodulation (implantation of a device that stimulates the sacral nerve). Treatment of coital incontinence, like treatment for mixed urinary incontinence, is generally based on the treatment of the dominant incontinence type.
In the discussion below, we will address the effect of treatments for stress UI and urge UI on sexual function, the physiological female sexual response, and coital incontinence.
Non-surgical treatment of urinary incontinence
Table 2 summarizes the effect of non-surgical treatments for stress UI and urgency UI on sexual function.
In stress UI, several high level, large trials support the idea that pelvic floor muscle training can significantly decrease urinary-related sexual problems [48] as well as improve sexual physiological response in the areas of desire, arousal, lubrication, orgasm, and satisfaction [49]. These improvements may be correlated to increased pelvic muscle strength [49]. Coital incontinence was found to be improved with muscle training [48, 49]. Pelvic muscle training, in combination with biofeedback and occasionally transvaginal electrical stimulation, is also used to treat urgency UI. The effect on sexual function in this population has not been extensively studied, and involves mostly small case series. A small randomized controlled trial comparing traditional pelvic exercises to biofeedback-assisted exercises and transvaginal electrical stimulation found that biofeedback-assisted pelvic floor muscle training resulted in greatest improvement in the King’s Health Questionnaire Personal Relationship domain [50].
Transvaginal electrical stimulation can be used to treat stress and urgency UI through strengthening of the pelvic floor muscles. One case series that included 12 women with stress UI and sexual dysfunction prior to treatment reported statistically significant improvements in overall sexual health (as indicated by improvement in Female Sexual Function Index score) and most subscale domains related to physiological response after 3 months of transvaginal electrical stimulation therapy [51]. Likewise, this modality can be used to treat urgency UI. In the same case series, which included ten women with urgency UI, transvaginal electrical stimulation also led to improved scores in the subjects with urgency UI [51]. A small randomized controlled trial found that transvaginal electrical stimulation resulted to less improvement in the King’s Health Questionnaire Personal Relationship domain than pelvic muscle training [50].
Anti-incontinence pessaries are commonly used for stress UI. One randomized controlled trial comparing anti-incontinence pessaries, pelvic floor muscle training/continence strategies, or both found no difference in the rates of incontinence, overall sexual function improvement, or sexual response achieved by pessaries compared to pelvic muscle training. Pessary users who had improvement in urinary symptoms (58.8 %) had greater improvement in overall sexual health (as indicated by higher Pelvic Organ Prolapse/Incontinence Sexual Questionnaire scores) than those who did not (2.26 ± 3.24 versus 0.48 ± 3.76, p = 0.0007) [50]. However, pelvic muscle training may be potentially more effective alone or in combination with anti-incontinence pessaries than with pessaries alone [50].
Anticholinergic medications are one of the first-line treatments for urgency UI. Though these medications are well studied, many large trials do not include specific assessment of changes in sexual function. Oxybutynin and tolterodine are two anti-cholinergic medications with high-quality evidence supporting improvement in sexual function with use. In the Multicentre Assessment of Transdermal Therapy in Overactive Bladder with Oxybutynin (MATRIX), which included 2878 subjects, 19.1 % of women reported improvement in sex life while 11.2 % reported worsening following 6 months of treatment with oxybutnin [52]. Similar proportions of women reported improvement in partner relationships and sexual desire [52]. Treatment with tolterodine was found to improve overall sexual health (higher sexual function questionnaire scores) compared with baseline in two studies, with particular improvement in desire, arousal, orgasm, lubrication, and satisfaction subscales [53, 54]. Fesoterodine likewise was found to improve subjects’ Personal Relationship scores as compared to controls [55]. Other smaller prospective studies have reported some improvement in sexual health following treatment with solifenacin [56] and trospium [57]. Certain trials also found that anti-muscarinic medication may improve coital incontinence. In the MATRIX study, oxybutynin was found to decrease the incidence of coital incontinence from 22.8 to 19.3 %, a statistically significant change [52]. In a study with tolterodine, 59 % of patients with incontinence at orgasm had improvement in response to tolterodine, though they were less likely to respond to treatment compared to those without coital incontinence (41.2 % v 17 %, p = 0.023) [39].
There are currently no studies evaluating the effect of a newer class of medication, beta-3 agonists, on sexual health.
Two small, poor quality trials on percutaneous tibial nerve stimulation found mixed sexual health outcomes. In two studies that included middle-aged women, one found no improvement in Female Sexual Function Index scores [58], while the other noted improvement in the Nine Questions Regarding Sexual Functioning scores, particularly in satisfaction, frequency, and orgasm [59].
Overall, there is strong evidence that pelvic muscle training can significantly improve sexual health in women with stress and urgency UI respectively. Transvaginal electrical stimulation (for both stress and urgency UI), pelvic muscle training (urgency UI), and anti-cholinergic medication (urgency UI) may improve sexual health, but data is limited by quantity and quality. Literature on anti-incontinence pessaries (stress UI) and percutaneous tibial nerve stimulation (urgency UI) show mixed improvement in sexual health; more trials are needed.
Surgical treatment of urinary incontinence
Surgical treatment of stress and urgency UI differ, but both seem to result in overall improvement in sexual health. Table 3 summarizes the effect of surgical treatments of stress UI on sexual function as reported in prospective studies. Midurethral slings are the gold standard for treatment of stress UI in middle-aged women, making up the majority of incontinence procedures performed on women aged 18 to 64 [47]. The effect of midurethral slings on sexual health is supported by several large prospective trials and randomized controlled trials.
There is a trend towards improvement in sexual health after correction with a midurethral sling. A meta-analysis of 21 studies noted that the pooled chance of improvement of sexual health following sling placement was 33.9 %, with improvement ranging from 1.8 to 94 % (0.95, 95 % CI 0.34, 1.56) [44]. One study that included 133 middle-aged women reported that 40 % of non-sexually active women reestablished intercourse after surgery [60].
Several studies reported improvement in aspects of female sexual response. There was an association between midurethral sling and decreased anxiety [61], resulting in improvement in sexual spontaneity, arousal, and orgasm in certain patients [62]. However, when examining other specific subdomains, most studies found no changes in sexual desire [63, 64], orgasmic capabilities [63, 64], intercourse frequency [63, 65], or satisfaction [63, 64] following sling surgery. Zycynski et al reported improvement in dyspareunia rates in a group of 406 subjects aged 52.9 +/- 11.0 years following sling surgery for stress UI [66].
Anti-incontinence surgeries can be very effective in treating coital incontinence. In fact, improvement after surgery was primarily attributed to decreased urinary-related sexual complaints such as coital incontinence [32, 61]. Pooled data on midurethral slings from a meta-analysis showed a significant reduction in coital incontinence with an OR 0.12 (CI 0.08-0.17) [44]. Post-operatively, patients also reported decreased fear and embarrassment of coital incontinence [67]. Women with coital incontinence and stress UI at baseline were also more likely to display improvement in frequency and enjoyment of intercourse as compared to those without coital incontinence (32.5 % v 6.8 %) [68].
Worsening of sexual function after midurethral sling placement is less common but possible, approximately 13.1 % in a meta-analysis by Jha et al [44]. This can manifest as new-onset dyspareunia [67], loss of libido [67], and de novo anorgasmia [64, 69]. The mechanism is not understood, but may be attributed to mesh complications such as erosion [70], changes in clitoral blood flow after dissection in the periurethral area, narrowing of the vaginal opening, or potential injury to the pudendal nerve branches [70, 71]. Removal or revision of mesh may improve sexual dysfunction; one case series showed that use of vaginal estrogen or correction of erosion after mesh slings were found to have improvement in all Female Sexual Function Index scores except orgasm [72].
Burch colposuspension is less commonly used to treat stress UI given the availability of minimally invasive techniques. Evidence on the effect of Burch colposuspension on overall sexual health is poor in quality and contradictory. One retrospective study comparing tension-free vaginal tape to Burch found no significant difference in sexual improvement post-operatively, though there was a non-significant increase in worsening of intercourse after tension-free vaginal tape [73]. Another small prospective study found decreased sexual function in both groups, but to a greater degree in patients who underwent Burch colposuspension [74].
Periurethal bulking injections are useful for management of stress UI in women who are poor candidates for general anesthesia, as these procedures can be performed with local anesthetics. Data on the effect of bulking agents on sexual function is limited in number and quality. One small prospective study on 29 patients (mean age: 53 years old) treated with polyacrylamide hydrogel injections reported significant improvement in total Pelvic Organ Prolapse/Incontinence Sexual Questionnaire-12 scores, and 6 patients reestablished sexual activity post-operatively [75]. Sexual response (desire, excitement, and orgasm) likewise improved. Four patients who presented with coital incontinence prior to injections achieved resolution of their incontinence [75].
Table 4 shows the effect of surgical treatments of urgency UI on sexual function. Studies on onabotulinumtoxin A injection and sexual function have not been conducted, though an randomized controlled trial by Nitti et al did note a significant improvement in the King’s Health Questionnaire Personal Relationships domain score following treatment with Botox in women with urgency UI [76]. Data on sacral neuromodulation is mixed. Four low quality studies showed significant improvement in sexual function questionnaire scores [77–80], while one did not [81]. Subscale improvements were noted in lubrication, pain, arousal, satisfaction, and orgasm intensity [77–80]. One case series on sacral neuromodulation indicated decreased coital incontinence in 3 patients, and cured coital incontinence in 2 patients, as well as decreased fear of coital incontinence [79].
Overall, there is high quality data to support improvement of sexual function after treatment with midurethral slings. Periurethral injection may improve sexual health, though larger studies are needed. The effect of Burch colposuspension on sexual function is mixed, and more evidence is required. High quality, large studies examining the effect of surgical treatments of urgency UI on sexual function are needed, though sacral neuromodulation shows promise in a few low quality studies.
Conclusions
Urinary incontinence is a bothersome condition that is prevalent in middle age women. There is significant data to support that urinary incontinence is detrimental to sexual function, especially in women in midlife. While data on the effect of urinary incontinence treatments on sexual function is limited by the lack of large trials and high quality trials, treatment of any incontinence has been shown to improve sexual function. For stress UI, non-surgical and surgical treatments - pelvic muscle training and midurethral slings - have been shown to improve sexual function. For urgency UI, treatment with pelvic muscle training and anti-muscarinic medications has the most evidence of improvement in sexual function. Coital incontinence generally improves with treatment of the underlying incontinence subtype. Though problems with sexual health in middle-aged women with incontinence are admittedly complex, and involve both psychological and physical factors, evaluation and treatment of urinary incontinence is important in the management of this important issue.
Abbreviations
- ATLAS:
-
Ambulatory treatments for leakage associated with stress
- UI:
-
Urinary incontinence
References
Dooley Y, Kenton K, Cao G, Luke A, Durazo-Arvizu R, Kramer H, et al. Urinary incontinence prevalence: results from the National Health and Nutrition Examination Survey. J Urol. 2008;179(2):656–61.
Waetjen LE, Liao S, Johnson WO, Sampselle CM, Sternfield B, Harlow SD, et al. Factors associated with prevalent and incident urinary incontinence in a cohort of midlife women: a longitudinal analysis of data: study of women's health across the nation. Am J Epidemiol. 2007;165(3):309–18.
Moller LA, Lose G, Jorgensen T. The prevalence and bothersomeness of lower urinary tract symptoms in women 40 ± 60 years of age. Acta Obstet Gynecol Scand. 2000;79:298–305.
Hannestad YS, Rortveit G, Sandvik H, Hunskaar S, Norwegian EPINCONT study. Epidemiology of Incontinence in the County of Nord-Trondelag. A community-based epidemiological survey of female urinary incontinence: The norwegian EPINCONT study. epidemiology of incontinence in the county of nord-trondelag. J Clin Epidemiol. 2000;53(11):1150–7.
Stewart WF, Van Rooyen JB, Cundiff GW, Abrams P, Herzog AR, Corey R, et al. Prevalence and burden of overactive bladder in the united states. World J Urol. 2003;20(6):327–36.
Barber MD, Dowsett SA, Mullen KJ, Viktrup L. The impact of stress urinary incontinence on sexual activity in women. Cleve Clin J Med. 2005;72(3):225–32.
Ratner ES, Erekson EA, Minkin MJ, Foran-Tuller KA. Sexual satisfaction in the elderly female population: A special focus on women with gynecologic pathology. Maturitas. 2011;70(3):210–5.
Nilsson M, Lalos O, Lindkvist H, Lalos A. How do urinary incontinence and urgency affect women's sexual life? Acta Obstet Gynecol Scand. 2011;90(6):621–8.
Shaw C. A systematic review of the literature on the prevalence of sexual impairment in women with urinary incontinence and the prevalence of urinary leakage during sexual activity. Eur Urol. 2002;42(5):432–40.
Lam GW, Foldspang A, Elving LB, Mommsen S. Social context, social abstention, and problem recognition correlated with adult female urinary incontinence. Dan Med Bull. 1992;39(6):565–70.
Rizk DE, Shaheen H, Thomas L, Dunn E, Hassan MY. The prevalence and determinants of health care-seeking behavior for urinary incontinence in united arab emirates women. Int Urogynecol J Pelvic Floor Dysfunct. 1999;10(3):160–5.
Norton PA, MacDonald LD, Sedgwick PM, Stanton SL. Distress and delay associated with urinary incontinence, frequency, and urgency in women. BMJ. 1988;297(6657):1187–9.
Sen I, Onaran M, Aksakal N, Acar C, Tan MO, Acar A, et al. The impact of urinary incontinence on female sexual function. Adv Ther. 2006;23(6):999–1008.
Aslan G, Koseoglu H, Sadik O, Gimen S, Cihan A, Esen A. Sexual function in women with urinary incontinence. Int J Impot Res. 2005;17(3):248–51.
Oh SJ, Ku JH, Choo MS, Yun JM, Kim DY, Park WH. Health-related quality of life and sexual function in women with stress urinary incontinence and overactive bladder. Int J Urol. 2008;15(1):62–7.
Liebergall-Wischnitzer M, Paltiel O, Hochner-Celnikier D, Lavy Y, Manor O, Woloski Wruble AC. Sexual function and quality of life for women with mild-to-moderate stress urinary incontinence. J Midwifery Womens Health. 2011;56(5):461–7.
Berglund AL, Fugl-Meyer KS. Some sexological characteristics of stress incontinent women. Scand J Urol Nephrol. 1996;30(3):207–12.
Sand PK, Appell R. Disruptive effects of overactive bladder and urge urinary incontinence in younger women. Am J Med. 2006;119(3 Suppl 1):16–23.
Heidler S, Mert C, Wehrberger C, Temml C, Ponholzer A, Rauchenwald M, et al. Impact of overactive bladder symptoms on sexuality in both sexes. Urol Int. 2010;85(4):443–6.
Woods NF, Mitchell ES. Consequences of incontinence for women during the menopausal transition and early postmenopause: Observations from the seattle midlife women's health study. Menopause. 2013;20(9):915–21.
Nilsson M, Lalos O, Lindkvist H, Lalos A. Impact of female urinary incontinence and urgency on women's and their partners' sexual life. Neurourol Urodyn. 2011;30(7):1276–80.
Handa VL, Harvey L, Cundiff GW, Siddique SA, Kjerulff KH. Sexual function among women with urinary incontinence and pelvic organ prolapse. Am J Obstet Gynecol. 2004;191(3):751–6.
Sako T, Inoue M, Watanabe T, Ishii A, Yokoyama T, Kumon H. Impact of overactive bladder and lower urinary tract symptoms on sexual health in japanese women. Int Urogynecol J. 2011;22(2):165–9.
Lukacz ES, Whitcomb EL, Lawrence JM, Nager CW, Contreras R, Luber KM. Are sexual activity and satisfaction affected by pelvic floor disorders? analysis of a community-based survey. Am J Obstet Gynecol. 2007;197(1):88.e1–6.
Salonia A, Zanni G, Nappi RE, Briganti A, Dehò F, Fabbri F, et al. Sexual dysfunction is common in women with lower urinary tract symptoms and urinary incontinence: Results of a cross-sectional study. Eur Urol. 2004;45(5):642–8. discussion 648.
Cohen BL, Barboglio P, Gousse A. The impact of lower urinary tract symptoms and urinary incontinence on female sexual dysfunction using a validated instrument. J Sex Med. 2008;5(6):1418–23.
Del Rosso A, Pace G, Di Pierro ED, Masciovecchio S, Galatioto GP, Vicentini C. Impact of overactive bladder on sexual function in women. Urologia. 2011;78(3):200–2.
Coyne KS, Sexton CC, Thompson C, Kopp ZS, Milsom I, Kaplan SA. The impact of OAB on sexual health in men and women: Results from EpiLUTS. J Sex Med. 2011;8(6):1603–15.
Zahariou A, Karamouti M, Tyligada E, Papaioannou P. Sexual function in women with overactive bladder. Female Pelvic Med Reconstr Surg. 2010;16(1):31–6.
Bekker MD, Beck JJ, Putter H, Van Driel MF, Pelger RC, Weijmar Schultz WC, et al. Sexual experiences of men with incontinent partners. J Sex Med. 2010;7(5):1877–82.
Yip SK, Chan A, Pang S, Leung P, Tang C, Shek D, et al. The impact of urodynamic stress incontinence and detrusor overactivity on marital relationship and sexual function. Am J Obstet Gynecol. 2003;188(5):1244–8.
Moller LA, Lose G, Jorgensen T. The prevalence and bothersomeness of lower urinary tract symptoms in women 40-60 years of age. Acta Obstet Gynecol Scand. 2000;79(4):298–305.
Nygaard I, Milburn A. Urinary incontinence during sexual activity: Prevalence in a gynecologic practice. J Womens Health. 1995;4(1):83–6.
Melin I, Falconer C, Rössner S, Altman D. Sexual function in obese women: impact of lower urinary tract dysfunction. Int J Obes (Lond). 2008;32(8):1312–8.
El-Azab AS, Yousef HA, Seifeldein GS. Coital incontinence: relation to detrusor overactivity and stress incontinence. Neurourol Urodyn. 2011;30(4):520–4.
Hayder D. The effects of urinary incontinence on sexuality: seeking an intimate partnership. J Wound Ostomy Continence Nurs. 2012;39(5):539–44.
Kizilkaya Beji N, Yalcin O, Ayyildiz EH, Kayir A. Effect of urinary leakage on sexual function during sexual intercourse. Urol Int. 2005;74(3):250–5.
Vierhout ME, Gianotten WL. Mechanisms of urine loss during sexual activity. Eur J Obstet Gynecol Reprod Biol. 1993;52(1):45–7.
Serati M, Salvatore S, Uccella S, Nappi RE, Bolis P. Female urinary incontinence during intercourse: a review on an understudied problem for women's sexuality. J Sex Med. 2009;6(1):40–8.
Hilton P. Urinary incontinence during sexual intercourse: a common, but rarely volunteered, symptom. Br J Obstet Gynaecol. 1988;95(4):377–81.
Emery J, Book NM, Novi JM. The association between post-void leakage and coital incontinence and intrinsic sphincter deficiency among women with urinary incontinence. Female Pelvic Med Reconstr Surg. 2010;16(6):349–52.
Serati M, Salvatore S, Uccella S, Cromi A, Khullar V, Cardozo L, et al. Urinary incontinence at orgasm: relation to detrusor overactivity and treatment efficacy. Eur Urol. 2008;54(4):911–5.
Liu L, Mansfield KJ, Kristiana I, Vaux KJ, Millard RJ, Burcher E. The molecular basis of urgency: regional difference of vanilloid receptor expression in the human urinary bladder. Neurourol Urodyn. 2007;26(3):433–8.
Jha S, Ammenbal M, Metwally M. Impact of incontinence surgery on sexual function: a systematic review and meta-analysis. J Sex Med. 2012;9(1):34–43.
Moran PA, Dwyer PL, Ziccone SP. Urinary leakage during coitus in women. J Obstet Gynaecol. 1999;19(3):286–8.
Kegel AH. Stress incontinence of urine in women; physiologic treatment. J Int Coll Surg. 1956;25(4 Part 1):487–99.
Jonsson Funk M, Levin PJ, Wu JM. Trends in the surgical management of stress urinary incontinence. Obstet Gynecol. 2012;119(4):845–51.
Bo K, Talseth T, Vinsnes A. Randomized controlled trial on the effect of pelvic floor muscle training on quality of life and sexual problems in genuine stress incontinent women. Acta Obstet Gynecol Scand. 2000;79(7):598–603.
Zahariou AG, Karamouti MV, Papaioannou PD. Pelvic floor muscle training improves sexual function of women with stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(3):401–6.
Wang AC, Wang YY, Chen MC. Single-blind, randomized trial of pelvic floor muscle training, biofeedback-assisted pelvic floor muscle training, and electrical stimulation in the management of overactive bladder. Urology. 2004;63(1):61–6.
Giuseppe PG, Pace G, Vicentini C. Sexual function in women with urinary incontinence treated by pelvic floor transvaginal electrical stimulation. J Sex Med. 2007;4(3):702–7.
Sand PK, Goldberg RP, Dmochowski RR, McIlwain M, Dahl NV. The impact of the overactive bladder syndrome on sexual function: a preliminary report from the multicenter assessment of transdermal therapy in overactive bladder with oxybutynin trial. Am J Obstet Gynecol. 2006;195(6):1730–5.
Rogers RG, Omotosho T, Bachmann G, Sun F, Morrow JD. Continued symptom improvement in sexually active women with overactive bladder and urgency urinary incontinence treated with tolterodine ER for 6 months. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(4):381–5.
Hajebrahimi S, Azaripour A, Sadeghi-Bazargani H. Tolterodine immediate release improves sexual function in women with overactive bladder. J Sex Med. 2008;5(12):2880–5.
Chapple CR, Van Kerrebroeck PE, Junemann KP, Wang JT, Brodsky M. Comparison of fesoterodine and tolterodine in patients with overactive bladder. BJU Int. 2008;102(9):1128–32.
Capo Jr JP, Laramée C, Lucente V, Fakhoury A, Forero-Schwanhaeuser S. Solifenacin treatment for overactive bladder in Hispanic patients: patient-reported symptom bother and quality of life outcomes from the VESIcare Open-Label Trial. Int J Clin Pract. 2008;62(1):39–46.
Danilova TI, Danilov VV, Luchinskii SA, Danilov VV, Vasil'chenko AV. Sexual dysfunction in women with overactive bladder and their correction with m-cholinolytic spasmex. Urologiia. 2010;6(6):30–4.
Eftekhar T, Teimoory N, Miri E, Nikfallah A, Naeimi M, Ghajarzadeh M. Posterior tibial nerve stimulation for treating neurologic bladder in women: a randomized clinical trial. Acta Med Iran. 2014;52(11):816–21.
van Balken MR, Vergunst H, Bemelmans BL. Sexual functioning in patients with lower urinary tract dysfunction improves after percutaneous tibial nerve stimulation. Int J Impot Res. 2006;18(5):470–5.
Filocamo MT, Serati M, Frumenzio E, LiMarzi V, Cattoni E, Champagne A, et al. The impact of mid-urethral slings for the treatment of urodynamic stress incontinence on female sexual function: a multicenter prospective study. J Sex Med. 2011;8(7):2002–8.
Jha S, Radley S, Farkas A, Jones G. The impact of TVT on sexual function. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(2):165–9.
Roos A, Thakar R, Sultan A, de Leeuw J, Paulus A. The impact of pelvic floor surgery on female sexual function: a mixed quantitative and qualitative study. BJOG. 2013.
Jha S, Moran P, Greenham H, Ford C. Sexual function following surgery for urodynamic stress incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(8):845–50.
Yeni E, Unal D, Verit A, Kafali H, Ciftci H, Gulum M. The effect of tension-free vaginal tape (TVT) procedure on sexual function in women with stress urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct. 2003;14(6):390–4.
Berthier A, Sentilhes L, Taibi S, Loisel C, Grise P, Marpeau L. Sexual function in women following the transvaginal tension-free tape procedure for incontinence. Int J Gynaecol Obstet. 2008;102(2):105–9.
Zyczynski HM, Rickey L, Dyer KY, Wilson T, Stoddard AM, Gormley EA, et al. Sexual activity and function in women more than 2 years after midurethral sling placement. Am J Obstet Gynecol. 2012;207(5):421.e1–6.
Mazouni C, Karsenty G, Bretelle F, Bladou F, Gamerre M, Serment G. Urinary complications and sexual function after the tension-free vaginal tape procedure. Acta Obstet Gynecol Scand. 2004;83(10):955–61.
Bekker M, Beck J, Putter H, Venema P, Lycklama à Nijeholt A, Pelger R, et al. Sexual function improvement following surgery for stress incontinence: the relevance of coital incontinence. J Sex Med. 2009;6(11):3208–13.
Ghezzi F, Serati M, Cromi A, Uccella S, Triacca P, Bolis P. Impact of tension-free vaginal tape on sexual function: results of a prospective study. Int Urogynecol J Pelvic Floor Dysfunct. 2006;17(1):54–9.
Elzevier HW, Putter H, Delaere KP, Venema PL, Nijeholt AA L a, Pelger RC. Female sexual function after surgery for stress urinary incontinence: Transobturator suburethral tape vs. tension-free vaginal tape obturator. J Sex Med. 2008;5(2):400–6.
Mouritsen L. Pathophysiology of sexual dysfunction as related to pelvic floor disorders. Int Urogynecol J Pelvic Floor Dysfunct. 2009;20 Suppl 1:S19–25.
Kuhn A, Eggeman C, Burkhard F, Mueller MD. Correction of erosion after suburethral sling insertion for stress incontinence: results and related sexual function. Eur Urol. 2009;56(2):371–6.
Demirkesen O, Onal B, Tunc B, Alici B, Cetinele B. Does vaginal anti-incontinence surgery affect sexual satisfaction? A comparison of TVT and burch-colposuspension. Int Braz J Urol. 2008;34(2):214–9.
Cayan F, Dilek S, Akbay E, Cayan S. Sexual function after surgery for stress urinary incontinence: vaginal sling versus burch colposuspension. Arch Gynecol Obstet. 2008;277(1):31–6.
Leone Roberti Maggiore U, Alessandri F, Medica M, Gabelli M, Venturini PL, Ferrero S. Periurethral injection of polyacrylamide hydrogel for the treatment of stress urinary incontinence: the impact on female sexual function. J Sex Med. 2012;9(12):3255–63.
Nitti VW, Dmochowski R, Herschorn S, Sand P, Thompson C, Nardo C, et al. OnabotulinumtoxinA for the treatment of patients with overactive bladder and urinary incontinence: results of a phase 3, randomized, placebo controlled trial. J Urol. 2013;189(6):2186–93.
Zabihi N, Mourtzinos A, Maher MG, Raz S, Rodriguez LV. The effects of bilateral caudal epidural S2-4 neuromodulation on female sexual function. Int Urogynecol J Pelvic Floor Dysfunct. 2008;19(5):697–700.
Signorello D, Seitz CC, Berner L, Trenti E, Martini T, Galantini A, et al. Impact of sacral neuromodulation on female sexual function and his correlation with clinical outcome and quality of life indexes: A monocentric experience. J Sex Med. 2011;8(4):1147–55.
Gill BC, Swartz MA, Firoozi F, Rackley RR, Moore CK, Goldman HB, et al. Improved sexual and urinary function in women with sacral nerve stimulation. Neuromodulation. 2011;14(5):436–43. discussion 443.
Pauls RN, Marinkovic SP, Silva WA, Rooney CM, Kleeman SD, Karram MM. Effects of sacral neuromodulation on female sexual function. Int Urogynecol J Pelvic Floor Dysfunct. 2007;18(4):391–5.
Ingber MS, Ibrahim IA, Killinger KA, Diokno AC, Peters KM. Neuromodulation and female sexual function: does treatment for refractory voiding symptoms have an added benefit? Int Urogynecol J Pelvic Floor Dysfunct. 2009;20(9):1055–9.
Handa VL, Whitcomb E, Weidner AC, Nygaard I, Brubaker L, Bradley CS, et al. Sexual function before and after non-surgical treatment for stress urinary incontinence. Female Pelvic Med Reconstr Surg. 2011;17(1):30–5.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
CC conceived and designed the aims of this review, conducted literature searches, and drafted the manuscript. LA participated in study design and critical revisions of the manuscript. UA aided in the design and coordination of the review and data acquisition, and helped to draft the manuscript. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
About this article

Cite this article
Chu, C.M., Arya, L.A. & Andy, U.U. Impact of urinary incontinence on female sexual health in women during midlife. womens midlife health 1, 6 (2015). https://doi.org/10.1186/s40695-015-0007-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40695-015-0007-6