
Abstract
Background
Myopia is the most common visual impairment in children and adolescents worldwide. This study described an economical and effective population-based screening pipeline and performed the project of a million scale children and adolescents myopia survey (CAMS), which will shed light on the further study of myopia from the level of epidemiology and precision medicine.
Methods
We developed a novel population-based screening pattern, an intelligent screening process and internet-based information transmission and analysis system to carry out the survey consisting of school children in Wenzhou, China. The examination items include unaided distance visual acuity, presenting distance visual acuity, and non-cycloplegic autorefraction. Myopia and high myopia were defined as spherical equivalent (SE) ≤ − 1.00 diopters (D) and SE ≤ − 6.00 D, respectively. Next, the reports of the vision checking were automatically sent to parents and the related departments. The CAMS project will be done two to four times annually with the support of the government. An online eyesight status information management system (OESIMS) was developed to construct comprehensive and efficient electronic vision health records (EVHRs) for myopia information inquiry, risk pre-warning, and further study.
Results
The CAMS completed the first-round of screening within 30 days for 99.41% of Wenzhou students from districts and counties, in June 2019. A total of 1,060,925 participants were eligible for CAMS and 1,054,251 (99.37% participation rate) were selected through data quality control, which comprised 1305 schools, and 580,609, 251,050 and 170,967 elementary, middle, and high school students. The mean age of participants was 12.21 ± 3.32 years (6–20 years), the female-to-male ratio was 0.82. The prevalence of myopia in elementary, middle, and high school students was 38.16%, 77.52%, and 84.00%, respectively, and the high myopia incidence was 0.95%, 6.90%, and 12.98%.
Conclusions
The CAMS standardized myopia screening model involves automating large-scale information collection, data transmission, data analysis and early warning, thereby supporting myopia prevention and control. The entire survey reduced 90% of staff, cost, and time consumption compared with previous surveys. This will provide new insights for decision support for public health intervention.
Similar content being viewed by others

Background
Refractive error is one of the most common eye ailments in the world [1]. In recent years, the prevalence of myopia is rising rapidly [2,3,4,5,6,7]. Individuals with high myopia have a higher risk of the development of permanent visual impairment or blindness due to retinal detachment, macular degeneration, cataract, and glaucoma [8,9,10,11,12,13,14,15]. The potential global productivity loss caused by vision impairment of uncorrected myopia was estimated at US$244,000 million in 2015 [16]. Based on existing trends, myopia is expected to affect about 49.8% of the world's population by the year 2050 [17].
In the last decade, a series of cross-sectional or prospective studies in refractive errors have been performed worldwide, such as in Asia [18,19,20,21,22,23,24,25,26,27,28,29,30,31], Europe [2, 32,33,34,35,36,37,38,39,40], America [41,42,43,44,45], Oceania [46,47,48,49], and Africa [50,51,52,53,54]. These studies provided essential information on the epidemiology of major ocular disorders and visual impairment among various countries and ethnic groups. In addition, these studies have indicated that the prevalence of refractive errors varies considerably depending on age, sex, ethnicity, and geographical environment. From a global perspective, myopia has a higher prevalence rate in East Asian countries (including China, Japan, South Korea, and Singapore) [55,56,57,58,59,60,61,62,63,64].
The myopia prevalence rate in China is higher than in other East Asian countries (for example, India and Nepal) [5, 27, 65,66,67]. A nationwide survey (2014) from China reported that the prevalence of myopia had reached 80% among students who had completed secondary education [68]. What is more disturbing is that vision impairment in children impacts their economic status and employment in adult life through influencing their psychological, social, and educational development [69]. Currently, there are vast numbers of cross-sectional refractive data for school-aged children, but longitudinal studies in this age group are relatively fewer and small-scale, even though investigating the incidence of myopia is of critical importance for formulating appropriate public health policies.
In the last year, the coronavirus disease (COVID-19) had led to an unprecedented global pandemic. To contain COVID-19, strict containment measures were imposed internationally, including social-distancing regulations, limited outdoor, school closures and switching in-person education to online home-based learning [70, 71]. With the implementation of these measures, citizens spent more time using digital devices for entertainment and education. This rapid increase in digital screen time may potentially lead to a rise of myopia rates worldwide, especially in Asia [72, 73]. Therefore, investigating the prevalence of myopia before and after the COVID-19 epidemic will help us understand the effect of factors such as digital devices and near activity on myopia prevalence.
The children and adolescents myopia survey (CAMS) is a population-based, city-wide, prospective cross-sectional survey undertaken to meet ocular health requirements of school-aged children and adolescents for the entire city of Wenzhou. This study screened 1.06 million students at over 1300 filtered schools. The initial cross-sectional survey was conducted in Jun 2019, while the subsequent follow-up study will last for ten years conducted at least twice annually. By December 2020, the follow-up survey had been performed four times. The main objective of this study was to determine the prevalence of myopia and high myopia. Secondary goals included recording the dynamic changes of myopia prevalence over the next decade and determining the prevalence of the other refractive errors. Furthermore, the CAMS includes a questionnaire survey to examine the living environment, eating habits, reading time, outdoor time and digital screen time, and the posture of near work. In addition, whole-exome sequencing and ophthalmic examination have been performed for high myopia students. The project results will contribute to public health intervention for eye health and clarify the molecular biological mechanism in myopia progression.
Methods
Ethics
The CAMS conformed to the principles of the Helsinki Declaration and has received ethics approval from the Eye Hospital of Wenzhou Medical University.
Study area and population
Wenzhou is located in southeast China (Fig. 1a), covering an area of nearly 11,613 km2, with 9.12 million permanent residents [74]. According to the demographic data (2019) released by the Wenzhou Statistical Bureau, about 6.55 million urban residents and 2.74 million rural residents have been living in the city [74]. There are four districts (Lucheng, Longwan, Ouhai, and Dongtou), two country-level cities (Ruian and Yueqing), and five counties (Yongjia, Pingyang, Cangnan, Wencheng, and Taishun). Wenzhou is one of the most developed cities in Zhejiang Province, whose gross domestic product (GDP) is 6606.1 billion RMB (in 2019), ranking 3rd in Zhejiang Province and placed 30th overall in China [75, 76].

Flowchart of the CAMS. a Location of the CAMS and regional population percentage of Wenzhou. b Framework of the CAMS. c Quality control, showing the participants available for analysis in the baseline
Study design and sampling process
The CAMS was a population-based, prospective cross-sectional survey initiated in May 2019, and funded by the Wenzhou government. This study aimed to enroll all school-aged children and adolescents from the elementary, middle, and high schools in the entire area of Wenzhou. Most notably, the CAMS is more than just vision screening; it is a combination of modernized vision screening, vision information management system, and electronic vison health records (EVHRs) (Fig. 1b). The study sought to attain four specific research objectives: (1) To determine the prevalence of myopia and other refractive errors in Wenzhou children and adolescents; (2) To record the dynamic changes of myopia prevalence over the next decade; (3) To publicize the knowledge of eye health care at the same time as the survey (such as playing a series of short cartoons about eye health knowledge in the waiting room, and handing out leaflets about eye health care); and (4) To delay the progress of myopia through early detection and intervention (CAMS provided the vision screening results and recommendations for participants on the EVHR, which is available for students and their parents to query). To date, the follow-up surveys have been completed four times, and the scale and intensity will remain the same as the initial vision screening in the coming 9 years.
Study committee
Led by the Wenzhou government and Wenzhou Education Bureau, a study committee was set up to organize, coordinate, and supervise the myopia survey. The office of the study committee was located at the Biomedical Big Data Center of Wenzhou Medical University.
Recruitment strategies
Prior to the commencement of the study, the Wenzhou Education Bureau notified the principals of each school about the CAMS. Subsequently, the principals conveyed the notification to the school health nurses and school doctors. Meanwhile, the education bureau sent text messages about the CAMS to all elementary, middle, and high school students. In addition, posters and radio broadcasts were displayed throughout the schools to further promote the study. It was gratifying to observe that no parents or students refused to participate in the CAMS, except for those with very specific personal reasons, such as sick leave and personal leave. The participation rate (the number of participants/the total number invited to participate) was 99.37% (1,054,251/1,060,925).
Information management system and electronic vision health records
To promote the efficiency of vision screening, it is necessary to establish a modernized information management system. In the preparation phase, we set up an online eyesight status information management system (OESIMS) for children and adolescents (see Additional file 1 Supplementary Materials 1 for details). The OESIMS was developed to upload, store, and manage vision screening data. With the support and assistance of the Wenzhou Education Bureau, the students’ general information (including the full name, student ID, ID number, class, grade, school type, school name, and administrative division) had been imported into the system by our team before the investigation. It is worth mentioning that the system supports real-time data uploads from an autorefractor via wireless networks or Bluetooth. Moreover, based on the OESIMS, an EVHR system was created to allow parents to query all visual examination results through their mobile phones.
Screening personnel
Vision screening personnel consisted school health nurses, health care physicians (school doctors), and volunteers from graduate students in Optometry. The guidelines proposed earlier for school vision screening indicated that school health nurses are capable screeners in a majority of countries [77]. Therefore, it is reasonable to incorporate school health nurses as screeners. To guarantee that the vision screening project could be carried out smoothly and professionally, the local government issued a policy to train one capable screener per 250 students. The training mission was delegated to the Eye Hospital of Wenzhou Medical University by the Wenzhou government. Subsequently, the eye hospital organized senior optometrists to train the targeted training groups, including school nurses and health care physicians. The entire training comprised four hours of theoretical training and four hours of practical training, and was carried out twice a year. The locations for centralized training were local hospitals of each district and county of Wenzhou. The exams were carried out immediately after training, and only by passing the exam could a screener be regarded as a capable screener.
Data collection procedures
The data acquisition process was as follows: (1) contact elementary, middle, and high schools; (2) schedule the survey days and organize screening; (3) choose suitable examination sites (usually the classroom); (4) distribute the brochures with personal information and a quick response (QR) code to each student through teachers; (5) propagate knowledge of eye health care; (6) perform ocular examination and upload data; and (7) download data from the OESIMS for further analysis and decision-making.
Ophthalmic examination
a) Distance visual acuity examination
Distance visual acuity (DVA) was assessed monocularly with a Chinese standard logarithm visual acuity E chart (GB 11533-2011) in an illuminated cabinet (WSVC-100, Wenzhou, China). If participants' prescription was worn, both uncorrected distance visual acuity (UDVA) and presenting distance visual acuity (PDVA) were measured. Otherwise, only UDVA was measured. Visual acuity (VA) examination was carried out at a distance of 5 meters from the chart [78,79,80]. Participants who failed to identify any optotypes were asked to approach the E chart until they could identify the optotypes. Subsequently, VA was recorded as (0.1 × distance)/5′ [81]. If any optotypes were still unrecognized, VA was assessed as counting fingers, hand motions, light perception, or no light perception. The results of VA examination were temporarily recorded in the students' brochures, waiting for input into the system.
b) Non-cycloplegic autorefraction
Every participant underwent a non-cycloplegic autorefraction after the VA measurement. Prior to examination, the screeners used a digital tablet to scan each participant’s QR code to enter the individual editing module of OESIMS and filled in the VA test results. Non-cycloplegic autorefraction tests were conducted using “Goaleye RM-9000 (Shenzhen Aist Industrial Co., Ltd., China; Former name: GoldEye RM-9000) autorefractors”. Each eye was measured three times. Thereafter, the results of autorefraction were automatically uploaded into the corresponding OESIMS editing module via wireless or Bluetooth.
Definition for visual impairment and refraction
Visual impairment
According to the World Health Organization (WHO) 2003 criteria, no visual impairment was defined as PDVA ≥ 6/12, mild impairment as 6/18 ≤ PDVA < 6/12, moderate visual impairment as 6/60 ≤ PDVA < 6/8, and severe visual impairment as 3/60 ≤ PDVA < 6/60 [82].
Refraction
The spherical equivalent (SE) reported in the present study were non-cycloplegic SE. Since non-cycloplegic autorefraction is likely to overestimate myopia prevalence in the young population [83, 84], we adopted a stricter definition of myopia. Likely myopia was defined as − 1.00 D < SE ≤ − 0.50 D in at least one eye, and myopia was defined as SE ≤ − 1.00 D in at least one eye [83]. It was further subdivided for analysis into low myopia (− 3.00 D < SE ≤ − 1.00 D), moderate myopia (− 6.00 D < SE ≤ − 3.00 D), and high myopia (SE ≤ − 6.00 D) [85]. Hyperopia was defined as SE ≥ + 2.00 D in any eye [84, 86]. Astigmatism was defined as minus cylinders ≤ − 0.75 D in any eye [86]. Anisometropia was defined as SE difference between both eyes based on 1.50 D [87].
Data quality control and analysis
To ensure the reliability and accuracy of the domestic autorefractor (Goaleye RM-9000), 449 individuals aged from 9 to 18 years (12.3 ± 2.1 years) chosen randomly from Wenzhou city were measured by three autorefractors in random sequence, including Goaleye RM-9000 and two reputable autorefractors (Topcon RM-800 (Tokyo, Japan) and Nidek AR-1 (Nagoya, Japan)) [88]. Then, a senior optometrist performed a subjective refraction for them by phoropter [88]. To monitor the validity of the data, each school carried out the self-examination by simple random sampling of 5% of the students. In the meantime, the local health department randomly selected 5% of the students from 5% of the schools randomly selected, to conduct ocular examinations for further verification.
The data downloaded from OESIMS was filtered by quality control procedures before analysis (Fig. 1c). The statistical analyses were performed by SPSS software (version 20.0). The prevalence of myopia and high myopia was calculated by the worse eye. As for categorical variables, Pearson chi-squared tests were performed. All confidence intervals were 95% intervals.
Results
Establishing the advanced information management system
After evaluating the effectiveness of the project process, on the basis of Wilcoxon signed ranks test, we found that the differences of SE between Goaleye RM-9000 and subjective refraction were even smaller compared with that between Topcon RM-800/Nidek AR-1 and subjective refraction [88]. Therefore, based on the Goaleye RM-9000, and combining high-precision technology with the vision screening, the OESIMS for the large-scale myopia survey of children and adolescents was developed by our team in the early stages. The system, generating sole index numbers and unique QR codes for each student, was developed to upload, store, and manage vision screening data. By scanning the QR code distributed by the teachers in advance, screeners could quickly enter the individual editing module of OESIMS and input the results of the VA test. More than that, the OESIMS also supports real-time data upload from the autorefractors via wireless networks or Bluetooth. These functions greatly facilitated data collection and uploading, reduced the workload, and saved time.
Baseline information
The baseline characteristics are presented as follows: of 1,060,925 individuals eligible for myopia screening, 1,054,251 took part in the study (99.37% participation rate). With data quality control, 1,002,626 (95.10%) were included for further analysis. The average myopia rate of each county was close to 55.83% (n = 559,784), as shown in Fig. 2a. In addition, the survey shows significant differences in the rate of myopia among children in urban and rural areas (Table 1). Myopia (SE ≤ − 0.50 D) prevalence was 58.64% (95% CI 58.53%–58.75%) in urban schools, and 50.30% (95% CI 50.30%–50.54%) in rural schools (P < 0.0001). The prevalence of high myopia was 5.05% (95% CI 5.00%–5.10%) in urban schools, and 3.12% (95% CI, 3.03%–3.20%) in rural schools (P < 0.0001). Figure 2b and c show the distribution of myopia and high myopia rates in elementary, middle, and high schools in different areas of Wenzhou, with myopia rates reaching 38.16%, 77.52%, and 84.00%, respectively.

Myopia prevalence of different regions in Wenzhou. a A total of eleven counties, districts, and cities. b Myopia prevalence. c High myopia prevalence
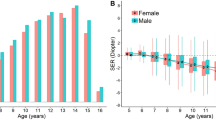
Over half of the participants were males (54.98%, n = 551,251). The average age was 12.21 ± 3.32 years (ranging from 6 to 20 years). In addition, the prevalence of myopia between males and females exhibited significant differences (53.29% for males vs. 58.94% for females, P < 0.0001), as shown in Table 2. We analyzed the VA status of students of different ages. The mean SE of participants and the prevalence of myopia and high myopia are reported in Tables 2 and 3. We found that the myopia prevalence in elementary and middle school students continued to increase with age (Fig. 3), and the rate of high myopia rose exponentially with age. In terms of VA of students in different grades, we hypothesized that the education phase is another influencing factor associated with myopia. The prevalence of myopia was 38.16% (95% CI 38.03%–38.28%) in elementary schools, 77.52% (95% CI 77.36%–77.68%) in middle schools, and 84.00% (95% CI 83.83%–84.18%) in high schools. High myopia prevalence in elementary, middle, and high schools were 0.95% (95% CI 0.93%–0.98%), 6.90% (95% CI 6.80%–7.00%), and 12.98% (95% CI 12.82%–13.14%), respectively. Statistical tests showed that there was a significant difference between grades for both myopia and high myopia (P < 0.0001).

Spherical equivalent (SE) distribution and myopia prevalence for children and adolescents. a SE distribution for school students aged 6 to 20 years. b Myopia prevalence for school students aged 6 to 20 years. c SE distribution for school students with different grades. d Myopia prevalence for school students of different grades
There were obvious differences in the prevalence of myopia among various types of schools. The myopia rate in key schools was significantly higher than that in general schools (Pearson chi-squared test, P < 0.0001). Figure 4a shows that there were significant differences in myopia and high myopia rates between key and non-key schools at different stages. The myopia rate in middle schools at the provincial second level was more than 82%, and that in high schools at the provincial first level was more than 90%. Moreover, in primary school, the myopia rate of martial arts schools was 19.61%, significantly lower than that of general schools (37.73%, P < 0.0001) at the same stage (Table 4). In middle and high schools, the myopia rates in martial arts schools, art schools, and sports schools were significantly lower than that in general schools.

Prevalence of myopia and high myopia in different school levels and school types. a & b According to school level, elementary, middle, and high schools were divided into provincial first level, provincial second level, ordinary, municipal first level and municipal second level. c & d According to school type, elementary, middle, and high schools were divided into art school, general school, vocational school, sport school and martial school. Pearson chi-squared test was performed to determine significance between each pair of condition. P-value: **P < 0.01, ***P < 0.001, ****P < 0.0001
The CAMS analyzed the vision and refractive status of children and adolescents in Wenzhou. More than 358,317 school students have not corrected myopia. The percentages of students with undercorrected VA in elementary, junior high, and senior high school were 13.13% (95% CI 12.74%–13.52%), 18.49% (95% CI 18.08%–18.90%), and 15.65% (95% CI 15.16%–16.13%), respectively (Table 5). The percentage of students with uncorrected VA was 68.18% (95% CI 67.94%–68.41%) in elementary schools, 42.29% (95% CI 41.95%–42.63%) in middle schools, and 30.86% (95% CI 30.43%–31.30%) in high schools.
Discussion
In this study, we described the design, methodology, and baseline profile of students in the CAMS. During the process, the Wenzhou government, the Wenzhou Education Bureau, and the Eye Hospital of Wenzhou Medical University came together to make this vision screening successful. The myopia survey is the first step of the CAMS project. The next step involves exploring environmental factors and genetic factors associated with myopia. We started a series of follow-up studies in 2020, including whole-exome sequencing and ophthalmic examination for students with high myopia along with diet and lifestyle questionnaires. CAMS strives to facilitate the automation of information collection, cloud data transmission, modular data storage, and intelligent data analysis. Data from the CAMS will not only provide detailed information on the prevalence of myopia/high myopia in school-age children and adolescents aged 6 to 20 years for the entire city of Wenzhou, but also is a powerful aid in devising myopia control strategies for China. The baseline information obtained from vision screening indicated that the current situation of students’ myopia control in Wenzhou is truly grim. There is still much work to be done to improve myopia prevention and control and eye care services.
Our study evaluated the prevalence of myopia in Wenzhou schoolchildren in southeast China. The myopia prevalence was 55.83% (55.73%–55.93%) for the 6- to 20-year-old age group and the SE was myopic (− 3.10 ± 1.91 D). Prior research indicated myopia prevalence in China, ranging from 33.9% in Chongqing (children aged 7 to 13 years) [89], 36.7% in the Chaoyang District of Beijing (children aged 5 to 14 years) [90] to 47.4% in Guangzhou (children grades 1 to 9) [91]. For myopia prevalence in other countries in Asia, the prevalence ranged from 23.8% in north India (children aged 13 to 15 years) [27], 54.05% in Japan (children aged 12 to 14 years) [92], 73.0% in South Korea (children aged 12 to 18 years) [93] to 74.9% in Singapore (children aged 15 to 19 years) [94]. It was particularly worrying that the prevalence of myopia in our research exceeded the previous report in Singapore, reaching 77.54% (children aged 15 to 19 years). In addition, the prevalence of myopia varied greatly among different types of schools (Fig. 4a, b) in our data. In high school, myopia prevalence at key schools was the highest (Fig. 4c, d), while that of the sports school and martial arts school was lower (Fig. 4). Key schools in China usually mean a richer learning environment, with better teacher resources, better electronic equipment resources, compared with other school types. Students at key schools tend to spend more time on reading and completing learning tasks, while students from sports school and martial arts school tend to have more outdoor time and exercise time. This indirectly shows that near work can promote myopia, while outdoor and sports can help to reduce the risk of developing myopia.
In the CAMS project, the first round of the myopia survey for children and adolescents in the whole city was successfully completed in May 2019, indicating that the standardized and procedural process created by our committee can be implemented and promoted nationwide as a model. We have established an elaborate workflow for vision screening through integrating automated technology into traditional vision screening. The workflow has the following advantages.
First, fast screening: With real-time data uploads from an autorefractor via wireless networks or Bluetooth, it takes only 22.5 seconds for each student to complete the whole process, and only 15 min to complete all the examinations of 40 students in a class.
Second, low cost: The costs of each student's examinations are cut by 90%, to as low as 3.5 RMB (0.53 USD) per person. In terms of this large-scale vision screening in millions of students, we put forward two solutions: purchasing services from relevant companies and purchasing equipment for on-campus self-examination by trained school nurses, trained school doctors, and volunteers from graduate students majoring in Optometry. After repeated detailed accounting for the work intensity, manpower, and overall cost of the two methods, we found that the cost of purchasing the service would be 10 RMB (1.52 USD) per student. However, the on-campus self-examination scheme would cost only 3.5 RMB (0.53 USD) per student if the vision screening was conducted twice annually. This average cost included the depreciation of equipment cost of 1.5 RMB (0.23 USD) and a service fee of 2 RMB (0.3 USD) per student. Therefore, our committee introduced this survey model of in-school self-examination, which reduced costs by 90% compared to purchasing the service.
Third, full coverage of the following three aspects: (1) The full coverage of school ages: all students that ranged from the first grade of elementary school to the last year of high school enrolled in the survey. (2) The full coverage of area: each type of school in Wenzhou was included in the survey; only by covering the entire city could we truly understand and evaluate visual impairment and refractive errors. (3) The full coverage of screening frequency: initial vision screening was conducted four times annually, followed by at least two screenings each year. The screenings make it possible for researchers and the government to follow the dynamic process of myopia progression in real time.
Last, convenient system of information management: each child's EVHR was established after data collection. For the parents, the EVHR supports self-service query for eye examination result and provides scientific myopia control suggestions based on their children's vision status (see Additional file 1 Supplementary Materials 2 and 3 for details). For the government, mastering the EVHR is conducive to understanding the current myopia situation in the region, and is an immense help for tracking myopia status and developing public health strategies to effectively reduce the public health burden caused by myopia. For epidemiologists, EVHR provide helpful clues for reducing the incidence and delaying the progress of myopia.
With the CAMS, we carried out training for school doctors and general teachers and promoted the introduction of myopia prevention and control techniques into schools. At present, a total of 4,000 school doctors, school health nurses, and teachers have been trained in myopia-related professional knowledge and skills, and an echelon of personnel and a public network have been formed for myopia surveying, prevention, and control. The CAMS offers a new way to promote public knowledge of eye health, improve the awareness of eye health, and monitor the dynamics of the myopia prevalence rate.
Using cycloplegic autorefraction is a practical necessity in our research. Although cycloplegic autorefraction is an important means to obtain accurate diopters, it is hard to achieve in such a large-scale myopia screening. Time and resources were difficult to coordinate, and parents had great resistance to cycloplegia [80]. Admittedly, cycloplegia is the gold standard for refractive error measurement in young children. However, the application of cycloplegia is also a barrier for large-scale detection. Compared with the pursuit of accurate measurement results, we thought it is more important for more children to have the opportunity to know the status of their vision, which is particularly important for a country like China with a high prevalence of myopia and a large population. Therefore, the study committee decided to adopt a non-cycloplegic refraction.
Conclusions
In summary, the CAMS is the largest-to-date study that investigated the prevalence of myopia in children and adolescents aged 6 to 20 years in Wenzhou, China. Furthermore, we established the Wenzhou vision screening pattern, which is an integration of modernized vision screening, OESIMS, and EVHR. The pattern possessed the characteristics of practicability, high feasibility, low cost, and modernization. It is hoped that the study can contribute insights for the designing of eye care strategies to alleviate the burden of visual impairment, myopia, and high myopia.
Availability of data and materials
The datasets used and/or analyzed during the current study are not publicly available, due to the local government’s policy on non-disclosure of student information.
Abbreviations
- D:
-
Diopters
- GDP:
-
Gross domestic product
- EVHR:
-
Electronic vision health records
- PDVA:
-
Presenting distance visual acuity
- OESIMS:
-
Online eyesight status information management system
- QR:
-
Quick response
- SE:
-
Spherical equivalent
- UDVA:
-
Uncorrected distance visual acuity
- VA:
-
Visual acuity
- CAMS:
-
Child and adolescent myopia survey
- WHO:
-
World Health Organization
References
Vos T, Abajobir AA, Abbafati C, Abbas KM, Abate KH, Abd-Allah F, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–59.
Williams KM, Verhoeven VJ, Cumberland P, Bertelsen G, Wolfram C, Buitendijk GH, et al. Prevalence of refractive error in Europe: the European Eye Epidemiology (E(3)) Consortium. Eur J Epidemiol. 2015;30(4):305–15.
Dolgin E. The myopia boom. Nature. 2015;519(7543):276–8.
Grzybowski A, Kanclerz P, Tsubota K, Lanca C, Saw SM. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020;20(1):27.
Li L, Zhong H, Li J, Li CR, Pan CW. Incidence of myopia and biometric characteristics of premyopic eyes among Chinese children and adolescents. BMC Ophthalmol. 2018;18(1):178.
Li Y, Liu J, Qi P. The increasing prevalence of myopia in junior high school students in the Haidian District of Beijing, China: a 10-year population-based survey. BMC Ophthalmol. 2017;17(1):88.
Wang SK, Guo Y, Liao C, Chen Y, Su G, Zhang G, et al. Incidence of and factors associated with myopia and high myopia in Chinese children, based on refraction without cycloplegia. JAMA Ophthalmol. 2018;136(9):1017–24.
Banker AS, Freeman WR. Retinal detachment. Ophthalmol Clin North Am. 2001;14(4):695–704.
Fan DS, Lam DS, Li KK. Retinal complications after cataract extraction in patients with high myopia. Ophthalmology. 1999;106(4):pp. 688–91; discussion 691–2.
Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31(6):622–60.
Haarman A, Enthoven CA, Tideman JWL, Tedja MS, Verhoeven VJM, Klaver CCW. The complications of myopia: a review and meta-analysis. Invest Ophthalmol Vis Sci. 2020;61(4):49.
Lam DS, Fan DS, Chan WM, Tam BS, Kwok AK, Leung AT, et al. Prevalence and characteristics of peripheral retinal degeneration in Chinese adults with high myopia: a cross-sectional prevalence survey. Optom Vis Sci. 2005;82(4):235–8.
Qiu M, Wang SY, Singh K, Lin SC. Association between myopia and glaucoma in the United States population. Invest Ophthalmol Vis Sci. 2013;54(1):830–5.
Richter GM, Torres M, Choudhury F, Azen SP, Varma R, Los Angeles Latino Eye Study Group. Risk factors for cortical, nuclear, posterior subcapsular, and mixed lens opacities: the Los Angeles Latino Eye Study. Ophthalmology. 2012;119(3):547–54.
Verhoeven VJ, Wong KT, Buitendijk GH, Hofman A, Vingerling JR, Klaver CC. Visual consequences of refractive errors in the general population. Ophthalmology. 2015;122(1):101–9.
Naidoo KS, Fricke TR, Frick KD, Jong M, Naduvilath TJ, Resnikoff S, et al. Potential lost productivity resulting from the global burden of myopia: systematic review, meta-analysis, and modeling. Ophthalmology. 2019;126(3):338–46.
Bruce A. Re: Holden et al.: Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050 (Ophthalmology 2016;123:1036–1042). Ophthalmology. 2017;124(3):e24–5.
Casson RJ, Kahawita S, Kong A, Muecke J, Sisaleumsak S, Visonnavong V. Exceptionally low prevalence of refractive error and visual impairment in schoolchildren from Lao People’s Democratic Republic. Ophthalmology. 2012;119(10):2021–7.
Goh PP, Abqariyah Y, Pokharel GP, Ellwein LB. Refractive error and visual impairment in school-age children in Gombak District. Malaysia. Ophthalmology. 2005;112(4):678–85.
Kato K, Kondo M, Takeuchi M, Hirano K. Refractive error and biometrics of anterior segment of eyes of healthy young university students in Japan. Sci Rep. 2019;9(1):15337.
Kim H, Seo JS, Yoo WS, Kim GN, Kim RB, Chae JE, et al. Factors associated with myopia in Korean children: Korea National Health and Nutrition Examination Survey 2016–2017 (KNHANES VII). BMC Ophthalmol. 2020;20(1):31.
Lee K, Kwon JW, Jahng WJ, Park YH, Jee D. Age- and sex-based evaluation of the association between refractive error and age-related macular degeneration in the Korean population. PLoS One. 2020;15(1):e228468.
Megreli J, Barak A, Bez M, Bez D, Levine H. Association of myopia with cognitive function among one million adolescents. BMC Public Health. 2020;20(1):647.
Ostadimoghaddam H, Fotouhi A, Hashemi H, Yekta A, Heravian J, Rezvan F, et al. Prevalence of the refractive errors by age and gender: the Mashhad Eye Study of Iran. Clin Exp Ophthalmol. 2011;39(8):743–51.
Rezvan F, Khabazkhoob M, Fotouhi A, Hashemi H, Ostadimoghaddam H, Heravian J, et al. Prevalence of refractive errors among school children in Northeastern Iran. Ophthalmic Physiol Opt. 2012;32(1):25–30.
Saw SM, Goh PP, Cheng A, Shankar A, Tan DT, Ellwein LB. Ethnicity-specific prevalences of refractive errors vary in Asian children in neighbouring Malaysia and Singapore. Br J Ophthalmol. 2006;90(10):1230–5.
Singh NK, James RM, Yadav A, Kumar R, Asthana S, Labani S. Prevalence of myopia and associated risk factors in schoolchildren in North India. Optom Vis Sci. 2019;96(3):200–5.
Wang X, He H, Wang X, Shan G, Tao Z, Pan L, et al. Prevalence and risk factors of myopia in Han and Yugur older adults in Gansu, China: a cross-sectional study. Sci Rep. 2020;10(1):8249.
Yahya AN, Sharanjeet-Kaur S, Akhir SM. Distribution of refractive errors among healthy infants and young children between the age of 6 to 36 months in Kuala Lumpur, Malaysia-a pilot study. Int J Environ Res Public Health. 2019;16(23):4730.
Huang X, Wang F, Lin Z, He Y, Wen S, Zhou L, et al. Visual quality of juvenile myopes wearing multifocal soft contact lenses. Eye Vis (Lond). 2020;7:41.
Labiris G, Panagiotopoulou EK, Chatzimichael E, Tzinava M, Mataftsi A, Delibasis K. Introduction of a digital near-vision reading test for normal and low vision adults: development and validation. Eye Vis (Lond). 2020;7:51.
Czepita D, Mojsa A, Zejmo M. Prevalence of myopia and hyperopia among urban and rural schoolchildren in Poland. Ann Acad Med Stetin. 2008;54(1):17–21.
Hashemi H, Fotouhi A, Mohammad K. The age- and gender-specific prevalences of refractive errors in Tehran: the Tehran Eye Study. Ophthalmic Epidemiol. 2004;11(3):213–25.
Hagen LA, Gjelle J, Arnegard S, Pedersen HR, Gilson SJ, Baraas RC. Prevalence and possible factors of myopia in norwegian adolescents. Sci Rep. 2018;8(1):13479.
Matamoros E, Ingrand P, Pelen F, Bentaleb Y, Weber M, Korobelnik JF, et al. Prevalence of myopia in France: a cross-sectional analysis. Medicine (Baltimore). 2015;94(45):e1976.
O’Donoghue L, McClelland JF, Logan NS, Rudnicka AR, Owen CG, Saunders KJ. Refractive error and visual impairment in school children in Northern Ireland. Br J Ophthalmol. 2010;94(9):1155–9.
Sandfeld L, Weihrauch H, Tubaek G. Analysis of the current preschool vision screening in Denmark. Acta Ophthalmol. 2019;97(5):473–7.
Nowak MS, Jurowski P, Grzybowski A, Smigielski J. Characteristics of refractive errors in a population of adults in the central region of Poland. Int J Environ Res Public Health. 2018;15(1):90.
Sandfeld L, Weihrauch H, Tubaek G, Mortzos P. Ophthalmological data on 4.5- to 7-year-old Danish children. Acta Ophthalmol. 2018;96(4):379–83.
Tideman JW, Snabel MC, Tedja MS, van Rijn GA, Wong KT, Kuijpers RW, et al. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol. 2016;134(12):1355–63.
Choudhury F, Meuer SM, Klein R, Wang D, Torres M, Jiang X, et al. Prevalence and characteristics of myopic degeneration in an adult Chinese American population: the Chinese American Eye Study. Am J Ophthalmol. 2018;187:34–42.
Galvis V, Tello A, Otero J, Serrano AA, Gomez LM, Castellanos Y. Refractive errors in children and adolescents in Bucaramanga (Colombia). Arq Bras Oftalmol. 2017;80(6):359–63.
Hendler K, Mehravaran S, Lu X, Brown SI, Mondino BJ, Coleman AL. Refractive errors and amblyopia in the UCLA preschool vision program; first year results. Am J Ophthalmol. 2016;172:80–6.
Maul E, Barroso S, Munoz SR, Sperduto RD, Ellwein LB. Refractive error study in children: results from La Florida, Chile. Am J Ophthalmol. 2000;129(4):445–54.
Richter GM, Wang M, Jiang X, Wu S, Wang D, Torres M, et al. Ocular determinants of refractive error and its age- and sex-related variations in the Chinese American Eye Study. JAMA Ophthalmol. 2017;135(7):724–32.
Fu A, Watt K, Junghans BM, Delaveris A, Stapleton F. Prevalence of myopia among disadvantaged Australian schoolchildren: a 5-year cross-sectional study. PLoS One. 2020;15(8):e238122.
Ojaimi E, Rose KA, Morgan IG, Smith W, Martin FJ, Kifley A, et al. Distribution of ocular biometric parameters and refraction in a population-based study of Australian children. Invest Ophthalmol Vis Sci. 2005;46(8):2748–54.
Pai AS, Wang JJ, Samarawickrama C, Burlutsky G, Rose KA, Varma R, et al. Prevalence and risk factors for visual impairment in preschool children the Sydney Paediatric Eye Disease Study. Ophthalmology. 2011;118(8):1495–500.
Sanfilippo PG, Yazar S, Kearns L, Sherwin JC, Hewitt AW, Mackey DA. Distribution of astigmatism as a function of age in an Australian population. Acta Ophthalmol. 2015;93(5):e377-85.
Badmus SA, Ajaiyeoba AI, Adegbehingbe BO, Onakpoya OH, Adeoye AO, Ameye SA. Relationship between refraction, anthropometrics, and educational status in a Nigerian young adult population. Middle East Afr J Ophthalmol. 2018;25(1):30–4.
Elnahry AG, Khafagy MM, Esmat SM, Mortada HA. Prevalence and associations of posterior segment manifestations in a cohort of Egyptian patients with pathological myopia. Curr Eye Res. 2019;44(9):955–62.
Mvogo SRE, Dohvoma VA, Fangwa JSN, Tsimi CM, Zoua MEA, Nguena MB, et al. Age of onset of presbyopia in the black Cameroonian subject. Pan Afr Med J. 2019;32:162.
Naidoo KS, Raghunandan A, Mashige KP, Govender P, Holden BA, Pokharel GP, et al. Refractive error and visual impairment in African children in South Africa. Invest Ophthalmol Vis Sci. 2003;44(9):3764–70.
Wajuihian SO, Hansraj R. Refractive error in a sample of black high school children in South Africa. Optom Vis Sci. 2017;94(12):1145–52.
Guo K, Yang DY, Wang Y, Yang XR, Jing XX, Guo YY, et al. Prevalence of myopia in schoolchildren in Ejina: the Gobi Desert Children Eye Study. Invest Ophthalmol Vis Sci. 2015;56(3):1769–74.
He M, Huang W, Zheng Y, Huang L, Ellwein LB. Refractive error and visual impairment in school children in rural southern China. Ophthalmology. 2007;114(2):374–82.
Lam CS, Lam CH, Cheng SC, Chan LY. Prevalence of myopia among Hong Kong Chinese schoolchildren: changes over two decades. Ophthalmic Physiol Opt. 2012;32(1):17–24.
Lee JH, Jee D, Kwon JW, Lee WK. Prevalence and risk factors for myopia in a rural Korean population. Invest Ophthalmol Vis Sci. 2013;54(8):5466–71.
Lee YY, Lo CT, Sheu SJ, Yin LT. Risk factors for and progression of myopia in young Taiwanese men. Ophthalmic Epidemiol. 2015;22(1):66–73.
Li SM, Liu LR, Li SY, Ji YZ, Fu J, Wang Y, et al. Design, methodology and baseline data of a school-based cohort study in central China: the Anyang Childhood Eye Study. Ophthalmic Epidemiol. 2013;20(6):348–59.
Ma Y, Qu X, Zhu X, Xu X, Zhu J, Sankaridurg P, et al. Age-specific prevalence of visual impairment and refractive error in children aged 3–10 years in Shanghai. China. Invest Ophthalmol Vis Sci. 2016;57(14):6188–96.
Matsumura H, Hirai H. Prevalence of myopia and refractive changes in students from 3 to 17 years of age. Surv Ophthalmol. 1999;44(Suppl 1):S109-15.
Sun J, Zhou J, Zhao P, Lian J, Zhu H, Zhou Y, et al. High prevalence of myopia and high myopia in 5060 Chinese university students in Shanghai. Invest Ophthalmol Vis Sci. 2012;53(12):7504–9.
Wu JF, Bi HS, Wang SM, Hu YY, Wu H, Sun W, et al. Refractive error, visual acuity and causes of vision loss in children in Shandong, China. The Shandong Children Eye Study. PLoS One. 2013;8(12):e82763.
Adhikari S. Myopia in school children from high mountain region of Nepal. Nepal J Ophthalmol. 2013;5(2):246–9.
Awasthi S, Pant BP, Langaas T. Refractive error prevalence among school children in Dadeldhura District of Nepal. Kathmandu Univ Med J (KUMJ). 2020;18(70):149–54.
Xiang F, He M, Zeng Y, Mai J, Rose KA, Morgan IG. Increases in the prevalence of reduced visual acuity and myopia in Chinese children in Guangzhou over the past 20 years. Eye (Lond). 2013;27(12):1353–8.
Mountjoy E, Davies NM, Plotnikov D, Smith GD, Rodriguez S, Williams CE, et al. Education and myopia: assessing the direction of causality by mendelian randomisation. BMJ. 2018;361:k2022.
Schneider J, Leeder SR, Gopinath B, Wang JJ, Mitchell P. Frequency, course, and impact of correctable visual impairment (uncorrected refractive error). Surv Ophthalmol. 2010;55(6):539–60.
Salcedo A, Yar S, Cherelus G. Coronavirus travel restrictions, across the globe. New York Times; 2020. 2. https://www.nytimes.com/article/coronavirustravel-restrictions.html. Accessed 16 July 2020.
United Nations Educational, Scientific and Cultural Organization (UNESCO). COVID-19 Educational Disruption and Response. https://en.unesco.org/covid19/educationresponse. Accessed 14 May 2020.
Singh NK. Letter to the editor: myopia epidemic post-coronavirus disease 2019. Optom Vis Sci. 2020;97(10):911–2.
Wang J, Li Y, Musch DC, Wei N, Qi X, Ding G, et al. Progression of myopia in school-aged children after COVID-19 home confinement. JAMA Ophthalmol. 2021;139(3):293–300.
Bureau of Statistics of Wenzhou City. Major data bulletin of Wenzhou population in 2019. 2019. http://wztjj.wenzhou.gov.cn/art/2020/3/2/art_1243860_42058089.html. Accessed 2 Mar 2020.
National Bureau of Statistics of China. Residents Personal Income and Consumption Expenditure 2018. 2019. http://www.stats.gov.cn/tjsj/zxfb/201901/t20190121_1645791.html. Accessed 21 Jan 2019.
People's Government of Wenzhou City. Government Work Report of Wenzhou 2019. 2019. http://www.wenzhou.gov.cn/art/2020/4/9/art_1229004361_42539435.html. Accessed 5 Mar 2019.
Metsing IT, Hansraj R, Jacobs W, Elsabe WN. Review of school vision screening guidelines. African Vision and Eye Health. 2018;1(77):1–11.
National Standard of People’s Republic of China. Standard Logarithmic Visual Acuity E Chart (GB 11533–2011). Beijing: China Standard Press; 2011.
Deng Y, Liang Y, Lin S, Wen L, Li J, Zhou Y, et al. Design and baseline data of a population-based metabonomics study of eye diseases in eastern China: the Yueqing Ocular Diseases Investigation. Eye Vis (Lond). 2020;7:8.
He X, Zhao R, Sankaridurg P, Zhu J, Naduvilath T, Ma Y, et al. Design and methodology of the Shanghai child and adolescent large-scale eye study (SCALE). Clin Exp Ophthalmol. 2018;46(4):329–38.
Chapter 6: Visual function examination, part 2 optometry. In: Wang YL, Li K, eds. Ophthalmology & Optometry. Beijing: People's Military Medical Press; 2008. p. 100.
World Health Organization. Consultation on development of standards for characterization for vision loss and visual functioning. Geneva: WHO/PBL; 2003. http://whqlibdoc.who.int/hq/2003/WHO_PBL_03.91.pdf?ua=1.
Flitcroft DI, He M, Jonas JB, Jong M, Naidoo K, Ohno-Matsui K, et al. IMI - defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20-30.
Gopalakrishnan A, Hussaindeen JR, Sivaraman V, Swaminathan M, Wong YL, Armitage JA, et al. The Sankara Nethralaya Tamil Nadu Essilor Myopia (STEM) Study-Defining a threshold for non-cycloplegic myopia prevalence in children. J Clin Med. 2021;10(6):1215.
Hu Y, Zhu S, Xiong L, Fang X, Liu J, Zhou J, et al. A multicenter study of the distribution pattern of posterior corneal astigmatism in Chinese myopic patients having corneal refractive surgery. Sci Rep. 2020;10(1):16151.
Salomao SR, Cinoto RW, Berezovsky A, Mendieta L, Nakanami CR, Lipener C, et al. Prevalence and causes of visual impairment in low-middle income school children in Sao Paulo, Brazil. Invest Ophthalmol Vis Sci. 2008;49(10):4308–13.
Thorisdottir RL, Faxen T, Blohme J, Sheikh R, Malmsjo M. The impact of vision screening in preschool children on visual function in the Swedish adult population. Acta Ophthalmol. 2019;97(8):793–7.
Lu CJ, Song D, Chen YZ, Tu C, Mao XJ, Xu LD, et al. Comparison of refractive measures of three autorefractors in school-aged children and adolescents. Chin J Optom Ophthalmol Vis Sci. 2019;21:721–6.
Xie Z, Long Y, Wang J, Li Q, Zhang Q. Prevalence of myopia and associated risk factors among primary students in Chongqing: multilevel modeling. BMC Ophthalmol. 2020;20(1):146.
Lyu Y, Zhang H, Gong Y, Wang D, Chen T, Guo X, et al. Prevalence of and factors associated with myopia in primary school students in the Chaoyang District of Beijing, China. Jpn J Ophthalmol. 2015;59(6):421–9.
Guo L, Yang J, Mai J, Du X, Guo Y, Li P, et al. Prevalence and associated factors of myopia among primary and middle school-aged students: a school-based study in Guangzhou. Eye. 2016;30(6):796–804.
Annual report of school health statistics research: Annual statistics (Article in Japanese). 2016. http://www.e-stat.go.jp/SG1/estat/GL08020103.do?_toGL08020103_&tclassID=000001014499&cycleCode=0&requestSender=dsearch. Accessed 5 Apr 2016.
Rim TH, Kim SH, Lim KH, Choi M, Kim HY, Baek SH. Refractive errors in Koreans: the Korea National Health and Nutrition Examination Survey 2008–2012. Korean J Ophthalmol. 2016;30(3):214–24.
Quek TP, Chua CG, Chong CS, Chong JH, Hey HW, Lee J, et al. Prevalence of refractive errors in teenage high school students in Singapore. Ophthalmic Physiol Opt. 2004;24(1):47–55.
Acknowledgements
The authors wish to thank all members of our lab. Additionally, we appreciate the generous support offered by the Wenzhou Education Bureau and School of Ophthalmology & Optometry and Eye Hospital, Wenzhou Medical University for this study. In addition, we thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript.
Funding
This work was supported by the Key Research and Development Program of Zhejiang Province (Grant Numbers 2020C03036 and 2021C03102), the National Natural Science Foundation of China (Grant Numbers 31801098 and 81830027), National Key Research and Development Program for Active Health and Aging Response (Grant Number 2020YFC2008200), the Major Scientific and Technological Innovation Projects of Wen Zhou (Grant Number ZY2020013), and the Internal Fund Project of Eye Hospital of Wenzhou Medical University (Grant Numbers YJGG20181001 and KYQD20190101).
Author information
Authors and Affiliations
Contributions
Conception and design of the study: JQ, XL, JS, FL, and HW. Statistical analysis and interpretation of data: YM, GZ, YZ, XL, and JL. Illustrations: GZ and WW. Administrative, technical, or material support: JY, CT, ML, XL, ZX, MZ, JB, JS, and ML. Drafting of the manuscript: LX and YZ. Critical revision of the manuscript: JQ, FL, HW, and JS. Study supervision: JQ, FL, and JS. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study complied with the Declaration of Helsinki and was approved by the Ethics Committee of the Eye Hospital of Wenzhou Medical University (2021-015-k-12).
Consent for publication
Not applicable.
Competing interests
JQ is the Editor-in-Chief of the journal. The other authors declare that they have no competing interests.
Supplementary Information
Additional file 1.
Supplementary Materials.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Xu, L., Zhuang, Y., Zhang, G. et al. Design, methodology, and baseline of whole city-million scale children and adolescents myopia survey (CAMS) in Wenzhou, China. Eye and Vis 8, 31 (2021). https://doi.org/10.1186/s40662-021-00255-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40662-021-00255-1