
Abstract
Background
Transforming growth factor (TGF)-β is involved in many physiologic processes, it often promotes metastasis, and its high expression is correlated with poor prognosis. In the present study, we analyzed the correlation between transforming growth factor beta 1 (TGF-β1) expression and prognosis in intrahepatic cholangiocarcinoma.
Results
We examined the expression of TGF-β1 in 78 intrahepatic cholangiocarcinomas by immunohistochemistry and correlated the expression with clinicopathological parameters. TGF-β1 was expressed in 37 of 78 (47.4 %) intrahepatic cholangiocarcinomas. The expression of TGF-β1 was significantly correlated with lymph node metastasis, distant metastasis, and tumour recurrence. Patients with TGF-β1-positive tumours had significantly shorter survival time. In a multivariant analysis, the expression of TGF-β1 and the tumour stage were independent prognostic factors.
Conclusions
Our data suggest that expression of TGF-β1 is a novel prognostic marker for intrahepatic cholangiocarcinoma.
Similar content being viewed by others
Background
Intrahepatic cholangiocarcinoma (ICC) is the second most common, primary hepatobiliary cancer after hepatocellular carcinoma. Despite overall advances in the diagnosis and treatment of patients with ICC, the prognosis of this disease still remains poor [1, 2]. One of the most important factors influencing the dismal prognosis of ICC is based on the late diagnosis at an advanced stage of disease, when tumour cell invasion into the blood and lymphatic vessels has resulted in metastatic spread and complete curative resection can no longer be achieved [3]. However, the molecular mechanisms underlying and driving metastasis remain unclear.
Transforming growth factor (TGF)-β is involved in various physiologic processes, such as wound healing, tissue development, and remodelling. TGF-β has also been implicated in many pathological conditions, including cancer, and has been shown to regulate a number of critical processes, such as angiogenesis, immune suppression, and cell migration [4–8]. TGF-β also induces a cytostatic response in most normal cell types and promotes metastasis in malignant tumour cells. Furthermore, high expression of TGF-β is correlated with poor prognosis in many malignant tumours [9–15].
There are three known mammalian isoforms of TGF-β, TGF-β1, −β2, and -β3, and all share significant structural and functional similarities [16]. Most malignant tumour cells exhibit positive TGF-β1 expression, with the most prominent expression in the plasma [14, 17]. Clinically, TGF-β1 is often elevated in the plasma of patients with malignant tumours. Preclinically, several models have shown correlations between TGF-β1 expression and increased tumourigenicity and increased invasion in many malignant tumours [8–10]. In this study, we analysed the expression of TGF-β1 in 78 ICC cases by immunohistochemistry, and investigated the association between TGF-β1 expression with clinicopathological parameters and patient survival.
Results
Expression of TGF-β1 protein in ICC
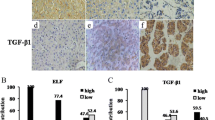
In normal liver tissue, TGF-β1 was not expressed in hepatocytes or bile ducts (Fig. 1a). TGF-β1 was detected in 37 of 78 tumours (47.4 %). Among the 37 tumours positive for TGF-β1 expression, 14 tumours had weak staining and 23 tumours had moderate to strong staining. The tumours showed cytoplasmic staining of TGF-β1 (Fig. 1b–e). Generally, TGF-β1 expression showed considerable heterogeneity in the intratumoral distribution.

Immunohistochemical staining of TGF-β1 in ICC and normal liver. a TGF-β1 is not expressed in hepatocyte or bile duct. b ICC with negative TGF-β1 staining. c ICC with weak TGF-β1 staining. d ICC with moderate TGF-β1 cytoplasmic staining. e ICC with strong TGF-β1 cytoplasmic staining (×200)
Clinicopathologic significance of TGF-β1 expression in ICC
To evaluate whether TGF-β1 protein was associated with clinicopathological features of patients with ICC, we correlated immunohistochemical TGF-β1 staining results with major clinicopathologic features of ICC. As shown in Table 1, TGF-β1 expression was positively associated with lymph node metastasis, lymphovascular invasion, distant metastasis and tumour recurrence, but not with sex, patient age, tumour stage, and histologic differentiation or tumour size (pT).
Univariant survival analysis
In univariant survival analysis, we used the Kaplan–Meier method to calculate the cumulative survival curve and the differences in survival were accessed by the log-rank method. The conventional prognostic parameters including tumour size, nodal status, and disease stage reached significance for the overall survival. Patients with TGF-β1-positive tumours had a significant shorter survival than those with TGF-β1-negative tumours (P = 0.017; Fig. 2). The median survival of patients with TGF-β1-positive and − negative tumours was 7.3 and 16.6 months, respectively.

Univariant survival analysis of TGF-β1 in all 78 ICCs demonstrates that TGF-β1 positive tumours are associated with poor prognosis
Multivariant survival analysis
A multivariant progression analysis based on the Cox proportional hazard model was performed to analyse the independent value of each parameter predicting overall survival (Table 2). In this analysis, we included tumour size, nodal status, disease stage, and TGF-β1 expression. Tumour stage (P = 0.0000) and TGF-β1 expression (P = 0.001) proved to be independent prognostic factors for shortened overall survival in ICC.
Discussion
In this study, we demonstrate that patients with ICC that express high levels of TGF-β1 have a higher chance of tumour recurrence, lymph node metastasis, lymphovascular invasion and distant metastasis than those with tumours that lack TGF-β1 expression. ICC is a highly aggressive tumour with generally poor prognosis characterized by intense desmoplastic stromal reaction and extensive vascular and perineural invasion.
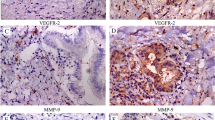
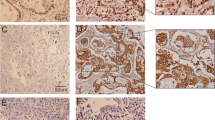
In our series, immunohistochemical TGF-β1 expression is an independent prognostic indicator for ICC patients irrespective of vascular and lymphovascular characteristics. The high significance of our statistical data supports the hypothesis that TGF-β1 expression may interfere with the invasion process in ICC. TGF-β1 is an upstream effector of MMPs and VEGF, which could promote invasion, angiogenesis, and proliferation in many cancers [1–6], and thus could be a biological predictor of survival for ICC patients [6]. However, the current understanding of invasion and metastasis processes in ICC is poor and future studies should focus on identification of the specific molecular pathways involving TGF-β1 in these tumours.
The possibility of long-term survival of ICC patients depends on early diagnosis and the feasibility of a surgical resection in cases with localized disease [18, 19]. Patients not suitable for surgery generally face rapid disease progression with a survival rate of months according to the series [18]. Prognostic markers are needed to identify ICC patients with poor prognosis that might benefit from more aggressive surgical strategies [20].
Sulkowski et al. reported a high frequency of TGF-β1 positive colorectal cancers (up to 87 % of studied cases) with cytoplasmic accumulation both in malignant cells and inflammatory cells. Their results suggested that blockage of anticancer immunity is maintained by TGF-β1 and cell growth is not restricted by TGF-β1 as much in cancer cells as in normal intestinal epithelial cells [21]. According to the clinical-pathological reports on ICC, we also found that vascular invasion was a poor prognostic predictor of early tumour recurrence in ICCs (P < 0.05) and tumour invasion was a poor prognostic factor only in pancreatic cancers at univariate analysis [22]. Expression of TGF-β1 in our ICC series turned out to be a significant predictor of survival (P = 0.017) at univariate tests and an independent indicator of early tumour recurrence, regardless of vascular invasion.
Conclusions
Our results indicate that TGF-β1 expression seems to represent a specific and independent neoplastic trait of ICC. Its immunohistochemical detection should provide a novel biological prognostic marker for ICC.
Methods
Ethical approval
The study was approved by The 180th Hospital of People’s Liberation Army, Quanzhou, and written informed consents were obtained from all participants prior to study entry.
Patients
Between 2008 and 2012, 78 consecutive patients underwent surgical resection of ICC at General Surgery department at the 180th Hospital of the People’s Liberation Army. The group comprised 38 men and 40 women with a mean age of 64 years (range, 23.6–78.3 years). The distribution of TNM staging was as follows: stage I, n = 32; stage II, n = 8; stage III, n = 21, and stage IV, n = 16. At the end of follow-up, 49 patients were dead. A total of 64 patients were followed up at least 12 months or until death.
Immunohistochemical analysis
Sections (4 μm) mounted on poly-L-lysine-coated slides were incubated for 30 min at 60 °C, deparaffinised by standard methods, and placed in 0.05 M Tris-HCI buffer, pH 7.2. Antigen retrieval was performed for 20 min in 10 mm sodium citrate buffer (pH 6) heated at 95 °C in a steamer, followed by cooling for 20 min. After blocking endogenous peroxidase activity with 0.3 % aqueous hydrogen peroxide for 5 min, the primary polyclonal rabbit anti-TGF-β1 antibody (DAKO, Carpinteria, CA, USA) was incubated with the sections at a final dilution of 2 mg/mL for 30 min. A control slide was incubated with Tris-HCI buffer substituted for the primary antibody. The DAKO LSAB™ kit/HRP was used for the detection of immunostaining. The sections were counterstained with Mayer’s haematoxylin. The staining intensity of TGF-β1 was semiquantitatively scored as negative, weak or moderate/strongly positive. A complete negative staining was scored as negative. A weak staining was defined as a minimal but unequivocal staining in less than 10 % of tumour cells. Stronger or more extensive staining was scored as moderate (10–50 %) or strong (≥50 %) positive expression. For statistical analysis, patients with weak and moderate/strong staining were lumped together as the TGF-β1-positive group in comparison with those with TGF-β1-negative tumours.
Statistical analysis
Statistical analysis of TGF-β1 expression between specimen groups was carried out using the unpaired Χ 2 test. Comparisons of clinicopathological factors (i.e. sex, age at diagnosis, histological type, pathological stage, differentiation, tumour stage, pathological stage, lymph node metastasis and metastasis) between positive—and negative-staining groups were performed using Χ 2 tests. The log-rank test was used to compare survival distributions between the positive and negative staining groups, and Kaplan–Meier curves were plotted for the two groups. The clinical factors were accounted as being reasonable by fitting Cox’s proportional hazards models. Differences were considered statistically significant when the P-value was <0.05.
Consent
Written informed consent was obtained from the patient for the publication of this report and any accompanying images.
References
Neuhaus P, Jonas S, Bechstein WO, Lohmann R, Radke C, Kling N, et al. Extended resections for hilar cholangiocarcinoma. Ann Surg. 1999;230:808–18.
Farley DR, Weaver AL, Nagorney DM. “Natural history” of unresected cholangiocarcinoma: patient outcome after noncurative intervention. Mayo Clin Proc. 2005;70:425–9.
Bismuth H, Nakache R, Diamond T. Management strategies in resection for hilar cholangiocarcinoma. Ann Surg. 2002;215:31–8.
Donovan D, Harmey JH, Toomey D, Osborne DH, Redmond HP, Bouchier-Hayes DJ. TGF-β1regulation of VEGF production by breast cancer cells. Ann Surg Oncol. 1997;4:621–7.
Huber MA, Kraut N, Beug H. Molecular requirements for epithelial-mesenchymal transition during tumour progression. Curr Opin Cell Biol. 2005;17:548–58.
Jeon SH, Chae BC, Kim HA. Mechanisms underlying TGF-β1-induced expression of VEGF and Flk-1in mouse macrophages and their implications for angiogenesis. J Leukoc Biol. 2007;81:557–66.
Pepper MS. Transforming growth factor-β: vasculogenesis, angiogenesis, and vessel wall integrity. Cytokine Growth Factor Rev. 1997;8:21–43.
Muraoka RS, Dumont N, Ritter CA. Blockade of TGF-β inhibits mammary tumour cell viability, migration, and metastases. J Clin Invest. 2002;109:1551–9.
Mitropoulos D, Kiroudi A, Christelli E, Serafetinidis E, Zervas A, Anastasiou I, et al. Expression of transforming growth factor beta in renal cell carcinoma and matched non-involved renal tissue. Urol Res. 2004;32:317–22.
Dong L, Ge XY, Wang YX, Yang LQ, Li SL, Yu GY, et al. Transforming growth factor-β and epithelial-mesenchymal transition are associated with pulmonary metastasis in adenoid cystic carcinoma. Oral Oncol. 2013;49:1051–8.
Reis ST, Pontes-Júnior J, Antunes AA, Sousa-Canavez JM, Abe DK, Cruz JA, et al. Tgf-β1 expression as a biomarker of poor prognosis in prostate cancer. Clinics (Sao Paulo). 2011;66:1143–7.
Von Rahden BH, Stein HJ, Feith M, Pühringer F, Theisen J, Siewert JR, et al. Overexpression of TGF-beta1 in esophageal (Barrett's) adenocarcinoma is associated with advanced stage of disease and poor prognosis. Mol Carcinog. 2006;45:786–94.
Fukai Y, Fukuchi M, Masuda N, Osawa H, Kato H, Nakajima T, et al. Reduced expression of transforming growth factor-beta receptors is an unfavorable prognostic factor in human esophageal squamous cell carcinoma. Int J Cancer. 2003;104:161–6.
Saito H, Tsujitani S, Oka S, Kondo A, Ikeguchi M, Maeta M, et al. An elevated serum level of transforming growth factor-beta 1 (TGF-beta 1) significantly correlated with lymph node metastasis and poor prognosis in patients with gastric carcinoma. Anticancer Res. 2000;20:4489–93.
Tsushima H, Kawata S, Tamura S, Ito N, Shirai Y, Kiso S, et al. High levels of transforming growth factor beta 1 in patients with colorectal cancer: association with disease progression. Gastroenterology. 1996;110:375–82.
Patil AS, Sable RB, Kothari RM. An update on transforming growth factor-β (TGF-β): sources, types, functionsand clinical applicability for cartilage/bone healing. J Cell Physiol. 2011;226:3094–103.
Lin Y, Kikuchi S, Obata Y, Yagyu K. Tokyo Research Group on Prevention of Gastric Cancer. Serum levels of transforming growth factor beta1 are significantly correlated with venous invasion in patients with gastric cancer. J Gastroenterol Hepatol. 2006;21:432–7.
Krasagakis K, Thölke D, Farthmann B, Eberle J, Mansmann U, Orfanos CE. Elevated plasma levels of transforming growth factor (TGF)-beta1 and TGF-beta2 in patients with disseminated malignant melanoma. Br J Cancer. 1998;77:1492–4.
Nakagohri T, Asano T, Kinoshita H, Kenmochi T, Urashima T, Miura F. Aggressive surgical resection for hilar-invasive and peripheral intrahepatic cholangiocarcinoma. World J Surg. 2013;27:289–93.
Gores GJ. Cholangiocarcinoma: current concepts and insights. Hepatology. 2013;37:961–9.
Sulkowski S, Wincewicz A, Sulkowska M, Koda M. Ann N Y Acad Sci. 2009;1171:116–23.
Hanazaki K, Kajikawa S, Shimozawa N, Shimada K, Hiraguri M, Koide N. Prognostic factors of intrahepatic cholangiocarcinoma after hepatic resection: univariate and multivariate analysis. Hepatogastroenterology. 2012;49:311–6.
Acknowledgement
This work was supported by the Military youth support program of China (13QNP167).
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
YJC and QH collected the clinical material; CHZ and SBZ participated in the design of the study and performed the statistical analysis; WJ and CHZ carried out the immunohistochemical analysis; YJC and LM helped to draft the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Chen, Y., Ma, L., He, Q. et al. TGF-β1 expression is associated with invasion and metastasis of intrahepatic cholangiocarcinoma. Biol Res 48, 26 (2015). https://doi.org/10.1186/s40659-015-0016-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40659-015-0016-9