
Abstract
Purpose
Improved understanding of the factors that predispose TKA patients to infection has considerable economic and medical impact. BMI is commonly used as a proxy for obesity to determine the risk of postoperative infection. However, this metric appears to be fraught with inconsistency in this application. BMI is a simple calculation which provides general insight into body habitus. But it fails to account for anatomic distribution of adipose tissue and the proportion of the mass that is skeletal muscle. Our objective was to review the literature to determine if local adiposity was more predictive than BMI for infection following TKA.
Methods
A database search was performed for the following PICO (Population, Intervention, Comparison, and Outcome) characteristics: local measurements of adiposity (defined as soft tissue thickness or fat thickness or soft tissue envelope at the knee) in patients over 18 years of age treated with total knee arthroplasty used to determine the relationship between local adiposity and the risk of infection (defined as prosthetic joint infection or wound complication or surgical site infection).
Quality was assessed using the GRADE framework and bias was assessed using ROBINS-I .
Results
Six articles (N=7081) met the inclusion criteria. Four of the six articles determined that adiposity was more associated with or was a better predictor for infection risk than BMI. One of the six articles concluded that increased adiposity was protective for short term infection and that BMI was not associated with the outcome of interest. One of the six articles determined that BMI was more strongly associated with PJI risk than soft tissue thickness.
Conclusion
The use of adiposity as a proxy for obesity in preoperative evaluation of TKA patients is an emerging concept. Although limited by heterogeneity, the current literature suggests that local adiposity may be a more reliable predictor for infection than BMI following primary TKA.
Level of evidence
IV systematic review
Similar content being viewed by others

Introduction
Infection is a well-documented complication following total knee arthroplasty (TKA) with considerable morbidity to the patient and burden to the health care system [2, 15, 16, 21]. Although the aggregate incidence of prosthetic joint infection (PJI) following TKA remains stable, there is expectation for increasing volume of post-TKA infection given the projections for increasing rates of primary TKA [1, 4, 14, 18, 20].
Body mass index (BMI in kilograms/meters2) is a simple calculation which provides general insight into body habitus. However, it fails to account for the anatomic distribution of adipose tissue and the proportion of the mass that is skeletal muscle. Further, the anatomic distribution of adipose has been shown to be an important variable in associating obesity with comorbid conditions [6, 8, 29]. Despite being commonly utilized as a predictor for infection following TKA, BMI has demonstrated inconsistency in this application [19, 24, 27]. Recent practice has restricted access to primary TKA based on obesity [5, 13]. Often these restrictions utilize a maximum BMI value [17]. Whether this practice is reasonable based on the efficacy of BMI is debated [11].
Recent investigations indicate that local adiposity is gaining momentum as a reliable predictor for postoperative infection. Subcutaneous fat thickness has been associated with increased rates of infection following abdominal surgery [22], spine surgery [7], hip fracture surgery [9], and colorectal surgery [10]. Therefore, it is a reasonable assessment that the same physiologic and mechanical factors which predispose to infection in these procedures may further the risk of infection following TKA. The local adipose-related variables which may contribute to infection include lengthened operative time, increased insult due to retraction and dissection and the metabolic and immune related compromise that are inherent to adipose tissue. Given the expansion of recent investigations, a comprehensive aggregation of evidence is needed to better understand the predictive capacity of local adiposity for infection following TKA.
Our objective was to review the literature to determine if local adiposity was more predictive for infection than BMI following primary TKA.
Materials and methods
Search protocol
A database search was performed in Google Scholar and PubMed on September 28, 2023, in keeping with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Keywords utilized were “soft tissue”, “adipose”, “adiposity”, “fat”, “obesity” AND “TKA/knee arthroplasty/knee replacement”. Duplicate and irrelevant articles were identified by title and author list.
Guidelines for study inclusion
The Population, Intervention, Comparison, and Outcome characteristics (PICO) were the following: local measurement of adiposity (defined as soft tissue thickness or fat thickness or soft tissue envelope) in patients over 18 years of age treated with primary total knee arthroplasty used to determine the relationship between local adiposity and the risk of infection (defined as prosthetic joint infection or wound complication or surgical site infection or superficial/deep infection).
P = TKA > 18yo.
I = local measurement of adiposity.
C = adiposity and BMI.
O = risk of infection.
Exclusion criteria were articles that evaluated the risk of infection following revision TKA, and articles that did not describe the parameters for measuring local adiposity. Articles that described systemic adipose (body fat percentage) were excluded.
Risk of bias assessment
The Cochrane ROBINS-I (risk of bias in non-randomized studies of interventions) was used to assess the risk of bias for each included article. The following domains were compiled: confounding, selection of participants, classification of interventions, deviation from intended interventions, missing data, measurement of outcomes, and selection of reported result. For each domain, a low, moderate, or serious level of risk was selected. For each article, the overall level of risk equated to the highest level of risk across the domains.
Quality assessment
The GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) framework was used to assess the quality of the evidence. Determining the phase of investigation was the starting point for the quality evaluation. The following factors were used to downgrade the presenting evidence: limitations, inconsistency, indirectness, imprecision, and publication bias.
Data extraction
The following variables were collected: study methodology, the specific parameters for measuring adiposity and the data for postoperative infection. Articles were grouped based on the reported method of measuring adiposity. One group measured adiposity on lateral radiograph. The other group measured adiposity on lateral and anteroposterior radiograph. Statistical analyses were unable to be performed due to the methodological heterogeneity of the included articles. Thus, the current work is analytical in nature without aggregate quantified outcomes.
Results
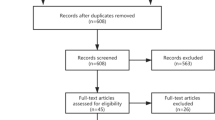
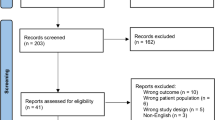
Six articles (N = 7081) met the inclusion criteria following assessment of 518 by title and abstract (Fig. 1). There were no criteria disagreements between authors regarding inclusions and exclusions.

The sequence of database search and identification of included and excluded articles
All included articles had at least one domain that was identified as having a moderate risk of bias (Table 1). This indicates that none of the articles can be considered comparative to a well-executed randomized trial, per the established interpretations. None of the articles contained domains identified as having a critical risk of bias.
Within the GRADE framework, all included articles were classified as phase I investigations which indicates an emerging topic with weak evidence (Table 2). The outcomes were grouped according to the following radiographic methods of local adipose measurement: on anteroposterior radiograph, and on anteroposterior and lateral radiograph. All groups demonstrated limitations for inconsistency and publication bias.
Four articles measure adiposity on lateral radiograph, and two measured adiposity on anteroposterior and lateral radiograph (Table 3). Two of the six articles evaluated infection at one year postoperatively [19, 28] and one of six evaluated infection at a minimum of two years postoperatively [23]. Three of the six reported 90-day data on reoperation for wound complication or infection [27], and surgical site infection (SSI) [12].
Four of the six articles determined that adiposity was more associated with or was a better predictor for infection risk than BMI [23, 24, 27, 28]. These findings were significant in three of the six articles [23, 24, 27]. One of the six articles concluded that increased adiposity was protective for short term infection and that BMI was not associated with the outcome of interest [12]. One of the six articles determined that BMI was more strongly associated with PJI risk than soft tissue thickness [19].
Discussion
The evaluation of adiposity as a predictor for infection following TKA is an emerging concept as evidenced by five of the six reviewed articles being published within the last five years. The current results demonstrate that local adiposity may be a more reliable predictor than BMI for infection following TKA. These findings occurred across multiple methodologies and adiposity measurements including prepatellar, pretubercular, medial joint line and anterior femoral. Within some reports, these findings were statistically significant [23, 24, 27]. Vahedi et al. (Vahedi) demonstrated that increased soft tissue thickness was significantly associated with increased risk of prosthetic joint infection (PJI) at a minimum of two years postoperatively. This finding was independent of BMI levels. In contrast, the report by Shearer et al. [19] across a large sample (62% of the collective N) reinforce the already prevalent use of BMI as a predictor for postoperative infection. The authors concluded that BMI was more predictive for PJI at one year postoperatively than local adiposity. Notably, Gupta et al. [12] demonstrated that increased fat thickness may be protective against infection. This finding was postulated to be due to the vascular anatomy which may remain intact with an appreciable depth of subcutaneous adipose.
Recent reports estimate that nearly 50% of adults in the United States (US) will be classified as obese (BMI ≥ 30 kg/m2) and nearly 25% will be classified as severely obese (BMI ≥ 35 kg/m2) by the year 2030 [26]. Additionally, nearly 70% of primary TKA patients are projected to be obese by the end of the current decade [3]. Although a clear understanding of obesity is still developing, the local and systemic impact of obesity is well documented. Obesity is often identified as a marked risk factor for post-TKA PJI [2, 16].
Despite being a relatively rare complication, PJI and its associated morbidity carry extensive implications from the individual patient level to the health care system level. Projections estimate the US financial burden of PJI following TKA will be over $1 billion by the end of the current decade [15]. Improved understanding of the factors that predispose TKA patients to infection has considerable economic and medical impact.
Although there is agreement regarding the impact of obesity on postoperative infection, the utility of BMI as a proxy for obesity has been fraught with inconsistency. There is momentum for local adiposity to be used to stratify infection risk. Waisbren et al. [25] determined that the magnitude of adiposity was a more precise measure of infection risk for SSI across a spectrum of elective surgical procedures. Based on the current methodology, the majority of the current evidence suggests that BMI is not a reliable predictor for infection following TKA. However, the lack of uniformity of the published data demonstrates the need for further investigation into the methods that may best predict the risk of infection following TKA.
Limitations of the current work should be considered when interpretating the derived conclusions. Inherent weaknesses of systematic reviews include the potential for error when aggregating data compiled by numerous sources. Inconsistencies in adipose measurement techniques are a feasible contributor. Although, the current work was able to group six of the included articles based on radiographic measurement, the techniques varied. Within the aggregate sample, one study comprised 62% of the whole which has the potential to bias the findings. The broad search strategy and narrow inclusion criteria strengthen the specificity of the results. Despite the current analysis being made without quantified results, the qualitative descriptive nature of the current work is consistent with an emerging concept which is likely to become more homogenized with increasing investigation.
Conclusion
The use of adiposity as a proxy for obesity in preoperative evaluation of TKA patients is an emerging concept. Although limited by heterogeneity, the current literature suggests that local adiposity may be a more reliable predictor for infection than BMI following primary TKA.
Availability of data and materials
The current data will be made available upon reasonable request.
References
Ackerman IN, Bohensky MA, Zomer E, Tacey M, Gorelik A, Brand CA et al (2019) The projected burden of primary total knee and hip replacement for osteoarthritis in Australia to the year 2030. BMC Musculoskelet Disord 20:90
Blanco JF, Díaz A, Melchor FR, da Casa C, Pescador D (2020) Risk factors for periprosthetic joint Infection after total knee arthroplasty. Arch Orthop Trauma Surg 140:239–245
Carender CN, Glass NA, DeMik DE, Elkins JM, Brown TS, Bedard NA (2022) Projected prevalence of obesity in primary total knee arthroplasty: how big will the Problem. Get? J Arthroplasty 37:1289–1295
Collaborative MA (2022) Incidence and Predictors of prosthetic joint infection following primary total knee arthroplasty: a 15-year population-based cohort study. J Arthroplasty 37:367-372e361
Davis W, Porteous M (2007) Joint replacement in the overweight patient: a logical approach or new form of rationing? Ann R Coll Surg Engl 89:203–206 (discussion 203)
Després JP (2012) Body fat distribution and risk of Cardiovascular disease: an update. Circulation 126:1301–1313
Donnally CJ, Henstenburg JM, Pezzulo JD, Farronato D, Patel PD, Sherman M et al (2022) Increased surgical site subcutaneous fat thickness is associated with infection after posterior cervical fusion. Surg Infect (Larchmt) 23:364–371
Frank AP, de Souza Santos R, Palmer BF, Clegg DJ (2019) Determinants of body fat distribution in humans may provide insight about obesity-related health risks. J Lipid Res 60:1710–1719
Frenkel Rutenberg T, Markman R, Rutenberg R, Daglan E, Rubin T, Shemesh S (2022) Thickness of the subcutaneous fat as a risk factor for surgical site infection following fragility hip fracture surgery. Geriatr Orthop Surg Rehabil 13:21514593221080270
Fujii T, Tsutsumi S, Matsumoto A, Fukasawa T, Tabe Y, Yajima R et al (2010) Thickness of subcutaneous fat as a strong risk factor for wound infections in elective colorectal surgery: impact of prediction using preoperative CT. Dig Surg 27:331–335
Giori NJ, Amanatullah DF, Gupta S, Bowe T, Harris AHS (2018) Risk reduction compared with access to care: quantifying the trade-off of enforcing a body mass index eligibility criterion for joint replacement. J Bone Joint Surg Am 100:539–545
Gupta VK, Kejriwal R (2020) Pretubercular Subcutaneous thickness is a protective factor for superficial wound complications after total knee arthroplasty in nonmorbidly obese patients. J Arthroplasty 35:255–258
Lash H, Hooper G, Hooper N, Frampton C (2013) Should a patients BMI status be used to restrict access to total hip and knee arthroplasty? Functional outcomes of Arthroplasty relative to BMI - single centre retrospective review. Open Orthop J 7:594–599
Namba RS, Inacio MC, Paxton EW (2013) Risk factors associated with deep surgical site Infections after primary total knee arthroplasty: an analysis of 56,216 knees. J Bone Joint Surg Am 95:775–782
Premkumar A, Kolin DA, Farley KX, Wilson JM, McLawhorn AS, Cross MB et al (2021) Projected economic burden of periprosthetic joint infection of the hip and knee in the United States. J Arthroplasty 36:1484-1489e1483
Resende VAC, Neto AC, Nunes C, Andrade R, Espregueira-Mendes J, Lopes S (2021) Higher age, female gender, osteoarthritis and blood transfusion protect against periprosthetic joint Infection in total hip or knee arthroplasties: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 29:8–43
Richardson G, Dusik C, Lethbridge L, Dunbar M (2021) Variable effects of obesity on access to total hip and knee arthroplasty. Can J Surg 64:E84-e90
Rodriguez-Merchan EC, Delgado-Martinez AD (2022) Risk factors for periprosthetic joint infection after primary total knee arthroplasty. J Clin Med 11(20):6128. https://doi.org/10.3390/jcm11206128
Shearer J, Agius L, Burke N, Rahardja R, Young SW (2020) BMI is a Better predictor of periprosthetic joint infection risk than local measures of adipose tissue after TKA. J Arthroplasty 35:S313–S318
Singh JA, Yu S, Chen L, Cleveland JD (2019) Rates of total joint replacement in the United States: future projections to 2020–2040 using the National Inpatient Sample. J Rheumatol 46:1134–1140
Tarazi JM, Chen Z, Scuderi GR, Mont MA (2021) The epidemiology of revision total knee arthroplasty. J Knee Surg 34:1396–1401
Teppa R, Sude NS, Karanam VPK, Mallipudi BVP (2022) Relevance of subcutaneous fat thickness as a risk factor for surgical site infections in abdominal surgeries. Cureus 14:e20946
Vahedi H, Ward DT, Lee YS, Shohat N, Chen AF (2020) Greater knee soft tissue thickness predisposes patients to subsequent periprosthetic joint Infection after total knee arthroplasty. J Arthroplasty 35:1924–1927
Wagner RA, Hogan SP, Burge JR, Bates CM, Sanchez HB (2018) The Radiographic prepatellar fat thickness ratio correlates with infection risk after total knee arthroplasty. J Arthroplasty 33:2251–2255
Waisbren E, Rosen H, Bader AM, Lipsitz SR, Rogers SO Jr, Eriksson E (2010) Percent body fat and prediction of surgical site infection. J Am Coll Surg 210:381–389
Ward ZJ, Bleich SN, Cradock AL, Barrett JL, Giles CM, Flax C et al (2019) Projected U.S. State-Level prevalence of adult obesity and severe obesity. N Engl J Med 381:2440–2450
Watts CD, Houdek MT, Wagner ER, Taunton MJ (2016) Subcutaneous fat thickness is associated with early reoperation and infection after total knee arthroplasty in morbidly obese patients. J Arthroplasty 31:1788–1791
Yu S, Siow M, Odeh K, Long WJ, Schwarzkopf R, Iorio R (2018) Periarticular soft tissue envelope size and postoperative wound complications following total knee arthroplasty. J Arthroplasty 33:S249–S252
Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P et al (2005) Obesity and the risk of myocardial infarction in 27,000 participants from 52 countries: a case-control study. Lancet 366:1640–1649
Acknowledgements
We appreciate the expertise and assistance of Odely, Mayra and Maveliza.
Informed consent
Not applicable for the current work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Author roles: JJH (1,2,3,5,6,7,13,14), PAS (2,3,5,6,13), RJR (2,3,5,6,13), AC (1,3,6,7,13,14).
1)conceptualization, 2) data curation, 3) formal analysis, 4) funding acquisition, 5) investigation, 6) methodology, 7) project administration, 8) resources, 9) software, 10) supervision, 11) validation, 12) visualization, 13) writing, original draft, 14) writing, review, and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable for the current work.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have influenced the current work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Heifner, J.J., Sakalian, P.A., Rowland, R.J. et al. Local adiposity may be a more reliable predictor for infection than body mass index following total knee arthroplasty: a systematic review. J EXP ORTOP 10, 110 (2023). https://doi.org/10.1186/s40634-023-00680-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40634-023-00680-2