
Abstract
Purpose
The indication for surgical treatment of the chronic exertional compartment syndrome is evaluated by measuring intracompartmental pressures. The validity of these invasive intracompartmental pressure measurements are increasingly questioned in the absence of a standardized test protocol and uniform cut-off values. The aim of the current study was to test compartment pressure monitors and needles for uniformity, thereby supporting the physician’s choice in the selection of appropriate test materials.
Methods
A compartment syndrome was simulated in embalmed above-knee cadaveric leg specimen. Four different terminal devices (Compass manometer, Stryker device, Meritrans transduce, and arterial line) were tested with 22 different needle types. Legs were pressurized after introduction of the four terminal devices in the anterior compartment, using the same needle type. Pressure was recorded at a 30-second interval for 11 minutes in total. Before and after pressurization, the intravenous bag of saline was weighed.
Results
The simulation of a compartment syndrome resulted in intracompartmental pressure values exceeding 100 mmHg in 17 of the 22 legs (77%). In the other five legs, a smaller built-up of pressure was seen, although maximum intracompartmental pressure was in between 70 and 100 mmHg. The intraclass correlation coefficient was above 0.700 for all possible needle types. Excellent to good resemblance was seen in 16 out of 22 instrumental setups (73%). The mean volume of saline infusion required in runs that exceeded 100 mmHg (309 ± 116 ml) was significantly lower compared to the legs in which 100 mmHg was not achieved (451 ± 148 ml; p = 0.04).
Conclusion
The intracompartmental pressure recordings of the four terminal devices were comparable, when tested with a standardized pressurization model in a human cadaver model. None of the included terminal devices or needle types were found to be superior. The results provide evidence for more diverse material selection when logistic choices for intracompartmental pressure measurement devices are warranted.
Level of evidence
Level IV.
Similar content being viewed by others


Introduction
The Chronic Exertional Compartment Syndrome (CECS), a disorder mostly affecting the lower extremities, can result in significant morbidity and limitations in activities of athletes, military personnel and recreational sportsmen [12]. It is characterized by a sensation of tightness and pain during or after performing repetitive physical activity. The etiology of CECS is largely unknown but may be related to pathologically elevated intracompartmental pressures (ICP) following muscular expansion during exercise [4, 5, 27, 30]. In the diagnostic work-up, these ICPs are measured using an invasive needle or catheter manometry before, during, or after provocative exercise [23]. However, consensus regarding the cut-off value indicative for CECS is currently lacking [1, 17].
Invasive ICP manometry is considered a user-dependent assessment, since a reproducible or standardized protocol is absent and readings were shown to be dependent on education [8, 11]. Hislop and Tierney [8] concluded that discrepancies were mainly found in the number of legs or compartments that were tested, the exercise used to provoke symptoms, and the position of the leg during needle placement or pressure recording. Also, physicians often do not use ultrasound to confirm correct placement of the needle or catheter, even though studies denounce a clear risk for inaccurate placement, particularly in the deep compartment [28, 29].
In addition, the setup used to perform ICP measurements is not standardized and can be performed with various types of available manometers, needles, and catheters. Several instrumental setups appear to be acceptable to perform ICP measurements, under the condition that a locally established protocol with cut-off values is adhered to [17]. However, studies demonstrated that absolute ICP values vary when either a slit catheter, side-port needle, or straight needle was used in the same experimental setup [2, 3, 7, 14, 22]. Boody et al. [2] declared to have a preference for the handheld Stryker manometer over the Whitesides [25], whereas Hammerberg et al. [7] compared a standard electronic arterial pressure monitor (Datex-Ohmeda S/5) with the Whitesides technique and did not find a significant difference between the two pressure monitors at all. Although all setups are based on the principle of installing a continuous saline fluid column between tissue in a compartment and the pressure device, exact clinimetric properties for these instrumental setups is often missing.
In the absence of a standardized test protocol and uniform cut-off values, the validity of ICP manometry is increasingly questioned [1, 8, 11, 17]. In addition, with the commonly applied Stryker device being no longer commercially available in Europe, physicians are forced to look for alternatives. As different setups (i.e. combination of different devices and needles) might result in different outcomes, information concerning the theoretically most precise setup might be helpful to support clinicians in their choice for alternative setups. Therefore, the aim of this study was to contribute to (partial) standardization of the diagnostic test protocol for CECS and to support the physician’s choice in the selection of the appropriate ICP measurement device and needle combination. This study further evaluated the results obtained during a comparable experiment conducted with a simulation model in the laboratory and was hypothesized to find comparable results [24].
Materials and methods
A cadaver study was performed. Under [Dutch] law, and under these conditions no approval of the medical research ethics committee was required. The study was performed in the Procedural Skills Laboratory of an academic hospital ([Erasmus MC, Rotterdam, the Netherlands]). Post-mortem human specimen (PMHS) were obtained through the Department of Anatomy, which were flushed with Anubifix® to regain elasticity after rigor mortis and embalmed with a 4.4% formalin solution. All total body donors were part of the national donor program and have given written consent for tissue donation for educational and scientific purposes before passing away. Due to [European] privacy regulations, medical history was only available to the general practitioner of the donor and not to the receiving academic medical center.
Equipment
Four manometer devices were tested: (1) A commonly used arterial line (Xtrans® system; CODAN, Lensahn, Germany & IntelliVue MX500 monitor; Philips, Eindhoven, the Netherlands); (2) the Stryker device (Stryker Intracompartmental Pressure Monitor System; Stryker, Kalamazoo, Michigan); (3) the Compass pressure monitor (Compass UniversalHg; Iskus Health, Ltd., Dublin, Ireland); and (4) the Meritrans transducer (Meritrans DTXPlus® Disposable Transducers; Merit Medical Systems, Jordan, Utah & IntelliVue MX500 monitor; Philips, Eindhoven, the Netherlands). The four terminal devices were each combined with 22 different commercially available needles (Supplementary Table 1), all varying in diameter and length, resulting in a total of 88 instrumental variations (Table 1). Connection between the continuous water column, free of air bubbles, and one of the four terminal devices was established using saline filled intravenous tubing with a three-way stopcock. A schematic representation of this setup can be found in Fig. 1.

Schematic representation of the experimental setup. Four different terminal devices were evaluated using the simulation of a compartment syndrome in a post-mortem human specimen (PMHS): 1. Compass UniversalHg; Iskus Health, Ltd., Dublin, Ireland, 2. Stryker Intracompartmental Pressure Monitor System; Stryker, Kalamazoo, Michigan, 3. Meritrans DTXPlus® Disposable Transducers; Merit Medical Systems, Jordan, Utah & IntelliVue MX500 monitor; Philips, Eindhoven, the Netherlands, 4. Xtrans® system; CODAN, Lensahn, Germany & IntelliVue MX500 monitor; Philips, Eindhoven, the Netherlands
Experimental compartment model
Above-knee amputated legs of PMHS were used to create a compartment syndrome model, comparable to previously published studies [11, 14, 15, 18,19,20]. The lower limb was visibly free of trauma or postsurgical changes. A 14-gauge angiocatheter was inserted in the proximal part of the anterior compartment of the lower leg and connected to the intravenous bag using standard IV tubes and connectors. Normal 0.9% saline (B. Braun Healthcare Corporation, Oss, the Netherlands) was infused using a manual pressure infusion bag with manometer.
Experimental procedure
All measurements were performed on two consecutive days, to keep location, room temperature, and humidity at a constant. The experimental setup was left unchanged in a secured room throughout this period.
Development of a decay model
A decay model, inspired by Teng et al. [20], was developed and tested with three embalmed PMHS legs to optimize pressurization and to evaluate natural pressure decay over time. In addition, a fresh-frozen PMHS leg was tested with the decay model to confirm the previously described similarities between fresh-frozen and embalmed PMHS types [6, 9, 21] and to justify the selection of embalmed PMHS for the current experiment.
The most commonly encountered instrumental setup (Side-port needle & Stryker Intracompartmental Pressure Monitor; Stryker Instruments, Kalamazoo, Michigan) was used to measure ICP continuously proximal, central, and distal in the anterior compartment. In the first minute, saline was infused with a pressure of 300 mmHg (Fig. 2). Subsequently, pressure was lowered to 200 mmHg, allowing for equilibration of the saline infusion. After every 2 min, 50 mmHg was released from the pressure bag. ICP was recorded at baseline and hereinafter with a 30-second interval. The saline fluid bag was kept at a constant height of 75 cm above the PMHS leg at all times. One hour hereinafter, the same run was repeated with the exact same experimental setup, to see whether a leg could be used repeatedly.

Timeline of the experiment
Pressurization
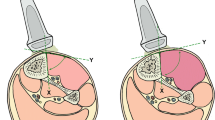
Prior to the start of the experimental procedures, all terminal devices were calibrated as prescribed. Every type of needle was tested on a different leg, meaning 22 specimens were required to test all available needles. Per leg, four identical needles were introduced at a right angle to the surface, halfway of the anterior compartment (Fig. 3). To these needles, the four different terminal devices were connected with saline filled IV tubing. All instrumental setups were flushed with 0.5–1 ml saline and pressure was allowed to equalize so baseline pressure could be recorded. Pressurization was executed according to the previously defined decay model with continuous pressure monitoring by all four terminal devices. Pressure was recorded at a 30-second interval for 11 minutes in total (Fig. 2).

Example of a limb with the experimental setup installed, using the Stryker side-ported needle. The four different terminal devices are: 1. Xtrans® system; CODAN, Lensahn, Germany & IntelliVue MX500 monitor; Philips, Eindhoven, the Netherlands, 2. Meritrans DTXPlus® Disposable Transducers; Merit Medical Systems, Jordan, Utah & IntelliVue MX500 monitor; Philips, Eindhoven, the Netherlands, 3. Stryker Intracompartmental Pressure Monitor System; Stryker, Kalamazoo, Michigan, 4. Compass UniversalHg; Iskus Health, Ltd., Dublin, Ireland
Additional data collection
Before and after pressurization, the intravenous bag of saline was weighed (to determine the amount of saline infused) and calf circumference of the leg was measured. Also, the leg was monitored at all times for possible signs of leakage (e.g. edema formation in the ankle, saline leakage from the amputation site, or absence of bulging of the anterior compartment).
Statistical analysis
Statistical analysis was performed using SPSS statistics (v25, IBM Corporation, Armonk, New York). All recordings per needle were plotted in one graph. Subsequently, the Intraclass Correlation Coefficient (ICC) [10] was used to compare the recordings of the four different terminal devices, thereby evaluating potential presence of instrumental bias. This was done using a two-way mixed method with absolute measures. Reliability and precision were quantified using the 95% confidence interval (CI) (poor < 0.500, moderate 0.500–0.750, good 0.750–0.900, or excellent > 0.900).
Additionally, the correlation between the amount of saline infusion and the overall change in ICP values was analyzed for instrumental setups with an ICC > 0.700. For this analysis, the 22 trials were arranged in two groups, with the first group comprising all trials in which ICPs exceeded 100 mmHg and the second group those in which this elevation could not be achieved. The amount of saline infusion in milliliters was calculated by subtracting the weight of the saline IV bag before and after the decay model, followed by a conversion with standard values for the density of saline solution at a given temperature. Furthermore, the area under the curve was calculated for the four different terminal devices per needle type. The mean AUC per needle type was correlated to the amount of saline infusion using a Pearson Correlation. An independent sample T-test was used to compare the mean of saline infusion needed in measurements that did or did not exceed 100 mmHg. Two-sided p-values ≤0.05 were considered significant.
Results
The 25 experimental procedures (3 test procedures + 22 procedures with possible needle and device combinations) and corresponding ratings were independently performed by the three assigned researchers ([SV, ER and DdV]) according to the described decay model. The four devices were similar in ease of use and no technical difficulties were encountered. Three embalmed and one fresh-frozen legs used to optimize the decay model showed that elevated pressures up to 204 mmHg could be simulated with this protocol. Moreover, these runs revealed that 2 minutes of equilibration was sufficient for the ICP to stabilize and that the decay model could run comparably in both the embalmed and the fresh-frozen leg. Also, similar pressures were recorded irrespective of needle location (i.e. proximal or distal). A repeat run in the same leg did not result in comparable or stable elevated pressures.
Pressurization with the decay model
The compartment syndrome was simulated successfully in all 22 legs. At baseline, a mean ICP of 9 (±4) mmHg with a range of 3 to 24 mmHg was recorded. With this decay model, ICP values exceeding 100 mmHg could be provoked in 17 of the 22 legs (77%; Table 2). In the other five legs, a smaller built-up of pressure was seen, although maximum pressures exceeded 70 mmHg. However, no visible signs of saline leakage were witnessed. Examples of a successful and less successful buildup of 100 mmHg with the decay model are depicted in Fig. 4A and B, respectively. Additional graphical illustrations of the recorded pressures for the four terminal devices (with the side-ported needle of Stryker, the C2Dx slit catheter, or the Sonoplex straight needle (21 gauge)) can be found in Supplementary Fig. 1 (A-C).

Graphical illustration of the pressure recordings throughout the decay model for the four terminal devices (Compass manometer, the Stryker device, Meritrans transducer, and an arterial line) in combination with (A) a Venflon Pro Safety catheter (18 gauge) and (B) a Microlance straight needle (21 gauge)
The ICC comparing the results of the four terminal devices per needle was above 0.700 for all possible combinations (Table 2). Excellent to good reliability was seen in 16 out of 22 instrumental setups (73%).
Correlation saline infusion and pressurization
The mean volume of saline infused during the decay model in the 22 legs was 343 ± 133 ml. The amount of saline infused and the area under the pressurization curve were shown to have a statistically significant linear relationship (r = − 0.709, p < 0.01; Fig. 5), indicating that an increase in saline infusion resulted in a smaller overall pressurization with the decay model. Moreover, the mean volume of saline infusion required in runs that exceeded 100 mmHg (309 ± 116 ml) was significantly lower compared to those which did not exceed this threshold (451 ± 148 ml; p = 0.04).

Correlation between the amount of saline infusion and the overall change in ICP values (Area Under the Curve). A statistically significant negative relation was found amongst all 22 trials (r = − 0.709, p < 0.01). Also, the mean volume of saline infusion required in runs that exceeded 100 mmHg was significantly lower compared to those which did not exceed this threshold (p = 0.04)
Discussion
The presented PMHS model evaluated four different ICP measurement devices and revealed that similar ICP pressures were recorded by all devices, irrespective of the type of needle used in the instrumental setup. All 22 possible device and needle combinations were shown to record comparable absolute measures. In nine of these combinations, the confidence interval denoted an excellent reliability and precision in measurements. No superiority for a specific device and needle combination was reported.
In daily clinical practice, the presence of CECS is often confirmed using ICP manometry. Up until recently, this was mainly done by using the Stryker Intracompartmental pressure Monitor System (Stryker, Kalamazoo, Michigan) as instrumental setup. However, with these materials recently becoming unavailable worldwide, the clinical practice of sports physicians and surgeons was challenged. Especially since the search for appropriate alternative setups was hampered by the fact that clinimetric properties of alternative setups are often missing. Subsequently, professionals were required to work with less familiar instrumental setups, in a time when validity of the ICP manometry is already increasingly debated due to the absence of a uniform cut-off value or test protocol.
The present study provides an updated overview regarding the reliability of available ICP measurement materials in clinical practice. In the past, studies reported that ICP measurements were preferably obtained using either a side-ported needle or a slit catheter, rather than a simple needle [2, 14]. Contrary to this, a more recent study reported not to find superiority amongst these needles and concluded all needles could be used with clinical confidence [7]. The present study confirms the data from the latter study. Looking at the terminal devices, the conventional arterial line manometer or the device by Stryker was shown to be superior to the Whitesides apparatus [2, 22, 25, 26]. If any of these materials would be unavailable, a single study indicated that an IV pump with pressure sensor would be a suitable and satisfactory alternative [22].
Naturally, products that came available hereinafter are not mentioned in previous literature. A first attempt in doing so involved an ex vivo experiment with a graduated water column, comparable to Uliasz et al. [22] and Boody et al. [2]. This study concluded that only the conventional arterial line and Stryker materials remained reliable in the measurement of ICP values in a porcine gluteal muscle sample [24]. The two other and newly developed terminal devices (Compass UniversalHg and the pressure transducer by Meritrans) seemed to lose accuracy after the addition of a muscle sample in the model.
The findings of this previously performed experiment with the water column model [24] are contradicted by this experiment with a PMHS model. The current results namely show that all terminal devices report comparable ICP values with an excellent to moderate reliability after introduction into muscle tissue, without superiority for a specific type of needle. This difference could have been instigated by the way the compartment syndrome was induced in the current PMHS model; with saline being infused directly and under high pressure in the compartment of an embalmed leg, rather than intravenously in a fresh frozen body [13]. Because of this, the saline could have collected in the intracompartmental space, without diffusion into the embalmed muscle tissue. It is therefore hypothesized that current measurements possibly reflect pressures of free-floating saline in the compartment, rather than actual tissue pressure of the tibialis anterior muscle. If that is the case, this PMHS model more closely resembles the graduated water column without a porcine muscle sample at the bottom. However, this explanation is challenged by the finding that a repeat run of the decay model gave overall higher and less variable pressure values, suggestive for the presence of diffused saline in the muscle tissue. So, although the presented findings might imply that all available materials are suitable for clinical ICP measurement, results have to be interpreted with caution and preferably tested with living patients first.
The variability in pressurization in the different legs might be due to a variation in the anatomy of the tested subjects. A sizable case series comparing three methods for ICP manometry (the Stryker materials, an arterial line, and an electronic transducer-tipped catheter) already suggested that the limited reliability of all single pressure measurements might be due to heterogeneous anatomy of the tested muscle compartments [3]. In the current study it was noted that throughout the experiment a wide range of ICP values could be achieved using different quantities of saline despite standardization of the pressurization model. This fluctuation in volume could be inherent to variation in the size of the muscle compartment, elasticity of the embalmed fascia or the amount of subcutaneous fat in a leg specimen. Also, although no visible signs of leakage were detected, the significant difference in saline infusion between legs that could or could not exceed 100 mmHg pressurization (Fig. 5) makes leakage via for example facial hernias highly suspected. Nevertheless, with all trials showing a minimum elevation of at least 70 mmHg, all simulations did exceed Pedowitz’ 30 mmHg threshold [16] and could therefore still be regarded as successfully.
The study was subject to several limitations. Possible generalization of the current study result is limited due to several reasons, the most prominent being the use of an ex vivo environment and the use of a different PMHS specimen per needle tested. Also, contrary to the experiments performed in a graduated water column, the actual ICP value inside the compartment throughout trial with the decay model was not known. Therefore, measurements in the current study could not be compared to a known reference pressure, but only to the pressure recordings of the other devices. So, the results reflect the extent to which the terminal devices agree, rather than knowing whether the devices actually measured the physiological ICP. Nevertheless, by standardizing the pressurization model and most of the environmental factors, this should have a negligible effect on current data. Also, with a PMHS model having a more close resemblance to the in vivo situation, current findings could present important data to support future choices in clinical practice.
Conclusion
The ICP recordings of the four terminal devices were comparable, when tested with a standardized pressurization model in a PMHS model. None of the included terminal devices or needle types were found to be superior. The results provide evidence for more diverse material selection when logistic choices for ICP measurement devices are warranted.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CECS:
-
Chronic exertional compartment syndrome
- ICP:
-
Intracompartmental pressure
- PMHS:
-
Post-mortem human specimen
References
Aweid O, Del BA, Malliaras P, Iqbal H, Morrissey D, Maffulli N et al (2012) Systematic review and recommendations for intracompartmental pressure monitoring in diagnosing chronic exertional compartment syndrome of the leg. Clin J Sport Med 22:356–370
Boody AR, Wongworawat MD (2005) Accuracy in the measurement of compartment pressures: a comparison of three commonly used devices. J Bone Joint Surg Am 87:2415–2422
Collinge C, Kuper M (2010) Comparison of three methods for measuring intracompartmental pressure in injured limbs of trauma patients. J Orthop Trauma 24:364–368
Fraipont MJ, Adamson GJ (2003) Chronic exertional compartment syndrome. J Am Acad Orthop Surg 11:268–276
Fronek J, Mubarak SJ, Hargens AR, Lee YF, Gershuni DH, Garfin SR et al (1987) Management of chronic exertional anterior compartment syndrome of the lower extremity. Clin Orthop Relat Res. (220):217–227
Gatt A, Schembri-Wismayer P, Chockalingam N, Formosa C (2019) Kinematic and kinetic comparison of fresh frozen and Thiel-embalmed human feet for suitability for biomechanical educational and research settings. J Am Podiatr Med Assoc 109:113–121
Hammerberg EM, Whitesides TE Jr, Seiler JG III (2012) The reliability of measurement of tissue pressure in compartment syndrome. J Orthop Trauma 26:24–31
Hislop M, Tierney P (2011) Intracompartmental pressure testing: results of an international survey of current clinical practice, highlighting the need for standardised protocols. Br J Sports Med 45:956–958
Hohmann E, Keough N, Glatt V, Tetsworth K, Putz R, Imhoff A (2019) The mechanical properties of fresh versus fresh/frozen and preserved (Thiel and formalin) long head of biceps tendons: a cadaveric investigation. Ann Anat 221:186–191
Koo TK, Li MY (2016) A guideline of selecting and reporting Intraclass correlation coefficients for reliability research. J Chiropr Med 15:155–163
Large TM, Agel J, Holtzman DJ, Benirschke SK, Krieg JC (2015) Interobserver variability in the measurement of lower leg compartment pressures. J Orthop Trauma 29:316–321
Lohrer H, Malliaropoulos N, Korakakis V, Padhiar N (2019) Exercise-induced leg pain in athletes: diagnostic, assessment, and management strategies. Phys Sportsmed 47:47–59
Messina FC, Cooper D, Huffman G, Bartkus E, Wilbur L (2013) A human cadaver fascial compartment pressure measurement model. J Emerg Med 45:e127–e131
Moed BR, Thorderson PK (1993) Measurement of intracompartmental pressure: a comparison of the slit catheter, side-ported needle, and simple needle. J Bone Joint Surg Am 75:231–235
Morris MR, Harper BL, Hetzel S, Shaheen M, Davis A, Nemeth B et al (2014) The effect of focused instruction on orthopaedic surgery residents' ability to objectively measure intracompartmental pressures in a compartment syndrome model. J Bone Joint Surg Am 96:e171
Pedowitz RA, Hargens AR, Mubarak SJ, Gershuni DH (1990) Modified criteria for the objective diagnosis of chronic compartment syndrome of the leg. Am J Sports Med 18:35–40
Roberts A, Franklyn-Miller A (2012) The validity of the diagnostic criteria used in chronic exertional compartment syndrome: a systematic review. Scand J Med Sci Sports 22:585–595
Sellei RM, Hingmann SJ, Weber C, Jeromin S, Zimmermann F, Turner J et al (2015) Assessment of elevated compartment pressures by pressure-related ultrasound: a cadaveric model. Eur J Trauma Emerg Surg 41:639–645
Shuler FD, Dietz MJ (2010) Physicians' ability to manually detect isolated elevations in leg intracompartmental pressure. J Bone Joint Surg Am 92:361–367
Teng AL, Huang JI, Wilber RG, Wilber JH (2005) Treatment of compartment syndrome: transverse fasciotomy as an adjunct to longitudinal dermatofasciotomy: an in vitro study. J Orthop Trauma 19:442–447
Topp T, Müller T, Huss S, Kann PH, Weihe E, Ruchholtz S et al (2012) Embalmed and fresh frozen human bones in orthopedic cadaveric studies: which bone is authentic and feasible? Acta Orthop 83:543–547
Uliasz A, Ishida JT, Fleming JK, Yamamoto LG (2003) Comparing the methods of measuring compartment pressures in acute compartment syndrome. Am J Emerg Med 21:143–145
Vajapey S, Miller TL (2017) Evaluation, diagnosis, and treatment of chronic exertional compartment syndrome: a review of current literature. Phys Sportsmed 45:391–398
Vogels S, Ritchie ED, Bakker EWP, Vogels MAJM, Zimmermann WO, Verhofstad MHJ et al (2022) Measuring intracompartmental pressures for the chronic exertional compartment syndrome: challenging commercially available devices and their respective accuracy. J Biomech 135:111026
Whitesides TE, Haney TC, Morimoto K, Harada H (1975) Tissue pressure measurements as a determinant for the need of fasciotomy. Clin Orthop Relat Res. https://doi.org/10.1097/00003086-197511000-0000743-51
Whitesides TE Jr, Haney TC, Harada H, Holmes HE, Morimoto K (1975) A simple method for tissue pressure determination. Arch Surg 110:1311–1313
Wilder RP, Magrum E (2010) Exertional compartment syndrome. Clin Sports Med 29:429–435
Wiley JP, Short WB, Wiseman DA, Miller SD (1990) Ultrasound catheter placement for deep posterior compartment pressure measurements in chronic compartment syndrome. Am J Sports Med 18:74–79
Winkes MB, Tseng CM, Pasmans HL, Cruijsen-Raaijmakers M, Hoogeveen AR, Scheltinga MR (2016) Accuracy of palpation-guided catheter placement for muscle pressure measurements in suspected deep posterior chronic Exertional compartment syndrome of the lower leg: a magnetic resonance imaging study. Am J Sports Med 44:2659–2666
Wuellner JC, Nathe CD, Kreulen CD, Burnham KJ, Giza E (2017) Chronic Exertional compartment syndrome: the Athlete's claudication. Oper Tech Sports Med 25:52–58
Acknowledgements
We would like to thank Gert Visser (senior purchasing advisor, Alrijne Hospital, Leiderdorp, the Netherlands), Twan W. Smit (medical instrumentation technician, Alrijne Hospital, Leiderdorp, the Netherlands), and Lucas Verdonschot (pathology assistant, department of Neuroscience-Anatomy, Erasmus Medical Center, Rotterdam, the Netherlands) for assistance with arranging all technical equipment and resources.
Funding
This study was partly funded by the Alrijne Hospital, a non-academic teaching hospital in Leiderdorp, the Netherlands, and the Dutch Ministry of Defense. No other support or resources were provided.
Author information
Authors and Affiliations
Contributions
SV, ER, G-JK, and RH conceptualized the study. SV wrote the study protocol. SV, ER, and DdV performed the data extraction. SV performed all statistical analysis and drafted all sections of the manuscript. All authors critically revised the draft manuscript and contributed to the subsequent revisions and the final version of the manuscript. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Under Dutch law, and under these conditions no approval of the medical research ethics committee was required.
Consent for publication
All total body donors were part of the national donor program and have given written consent for tissue donation for educational and scientific purposes before passing away.
Competing interests
The authors report there are no competing interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1: Supplementary Table 1.
Different needle types used in the experimental setup.
Additional file 2: Supplementary Figure 1.
Graphical illustration of the pressure recordings for the four terminal devices (Compass manometer, the Stryker device, Meritrans transducer, and an arterial line) in combination with a Styker side-ported needle (A), C2Dx slit catheter (B), and a Sonoplex straight needle (21 gauge; C).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Vogels, S., Ritchie, E.D., de Vries, D. et al. Applicability of devices available for the measurement of intracompartmental pressures: a cadaver study. J EXP ORTOP 9, 98 (2022). https://doi.org/10.1186/s40634-022-00529-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40634-022-00529-0