
Abstract
Objectives
This study aimed to validate the content of the specialized competency frameworks for pharmacists working in hospital settings (hospital and clinical pharmacists) and pilot the frameworks for practice assessment.
Methods
This online cross-sectional study was carried out between March and October 2022 among a sample of 96 Lebanese pharmacists working in hospital settings. The frameworks were distributed to full-time hospital and clinical pharmacists, who filled them out according to their role in the hospital.
Results
Overall, the competencies were distributed over five domains for hospital pharmacists (fundamental skills, safe and rational use of medicines, patient-centered care, professional skills, and preparedness for emergencies), while for clinical pharmacists, competencies were distributed over seven domains (quality improvement, clinical knowledge and skills, soft skills, ability to conduct clinical research, ability to provide effective education, use information technology to make decisions and reduce errors, and emergency preparedness). Moreover, Cronbach alpha values were appropriate, indicating sufficient to high internal consistency. Pharmacists were highly confident in most competencies, with some exceptions related to research in emergency settings (data evaluation, research, and reporting).
Conclusions
This study could validate competency frameworks for clinical and hospital pharmacists, with the competencies and their respective behaviors showing an adequate construct analysis. It also identified the domains that require further development, i.e., soft skills and research in emergency settings. Both these domains are timely and needed to overcome the current practice challenges in Lebanon.
Similar content being viewed by others

Introduction
For many decades, hospital and clinical pharmacy services have been growing, benefiting from pharmacists with extra training and expertise to improve aspects of pharmaceutical care in hospitals [1]. Decentralization of services was promoted, and the participation of clinical pharmacists in a structured clinical multidisciplinary team was related to a decrease in hospital admissions [2, 3]. Several countries have adopted such services, while pharmacy professional organizations have emphasized the need to define the competencies and further training necessary for advanced practice and recognize specializations within the field [4, 5]. Components of advanced training and experience are required to practice successfully as clinical or hospital pharmacists.
Clinical pharmacists offer patients in all healthcare settings complete drug management and associated care. They are highly qualified professionals who have received extensive education and training. They possess the clinical skills necessary to work in healthcare settings, where teamwork and direct patient care are emphasized. Their responsibilities go beyond just dispensing medication, as they also monitor for potential drug interactions, provide patient counseling, and work with other healthcare professionals to create personalized treatment plans [6]. As patients move through various healthcare settings and interact with different healthcare providers, it is vital to ensure that their treatment is coordinated and effective. Clinical pharmacists are trained to assess patients, evaluate their medication therapy, and develop and implement individualized plans of care. They also play a critical role in monitoring patients’ medication use over time to ensure that treatment remains safe and effective [7].
As for hospital pharmacists, they have a critical role in patient care that goes beyond the traditional tasks of medication preparation and dispensing. They also contribute to disease management, medication review, and health promotion [5, 8]. Research has shown that the involvement of hospital pharmacists in prescribing and medication management can lead to improved outcomes, including reduced medication errors and adverse drug events [9,10,11]. In many countries, there is a growing recognition of the benefits of increased collaboration among healthcare professionals in making prescription choices, and the expanded role of pharmacists in prescribing has been particularly effective [12, 13]. Hospital pharmacists provide various types of patient care support, such as recommendations on medication use and storage, medication substitution, and participation in clinical studies involving individualized, high-tech medications [14].
Furthermore, pharmacists who wish to participate in pharmacy practice research and clinical research must possess the knowledge and skills to describe, explain, and discuss commonly used research methodology. They must also be able to organize, direct, and conduct research and practice development programs that promote the safe and responsible use of medications while also collaborating with other healthcare professionals [4, 15]. Several minimum and specialized competency standards/frameworks have been established beyond those required by formal training programs to ensure that pharmacists possess the necessary competencies to work effectively in these roles. These standards encompass a range of behavioral competencies and knowledge elements, each with its own set of outcomes. By meeting these standards, pharmacists can work safely and competently in research and practice development, helping to advance the pharmacy profession and improve patient care [16,17,18,19].
In Lebanon, few pharmacists choose clinical/hospital pharmacy as a career path due to the paucity of positions and the fact that these specialties are not recognized by local authorities [20, 21]. Although schools of pharmacy provide various didactic and clinical hours in patient care, the exposure to such programs varies, affecting the knowledge, abilities, and perspectives of new graduates when it comes to providing patient care. Since there is a smaller number of pharmacists with formal training in hospitals, hospital pharmacists often need significant on-the-job training to attain a basic level of proficiency in caring for patients, in addition to training aimed at developing broad clinical and organizational abilities relevant to all patient demographics and pharmacy environments [22]. Before engaging in an unsupervised practice, pharmacists providing patient care in a hospital setting must demonstrate competence in fundamental knowledge and abilities. Pharmacists who have not completed hospital residency training may need to attain this basic level of proficiency through institution-based on-the-job training programs [23, 24].
Currently, there are no established minimum competency requirements for entry-level pharmacists who work in hospital settings. The Order of Pharmacists of Lebanon (OPL), the professional association of pharmacists in Lebanon, had issued a core competencies framework to improve the quality, safety, and equality of patient care in Lebanon [24, 25]. It has also developed guiding principles for service reform of clinical/hospital pharmacists, which includes suggested frameworks for academic institutions to incorporate into their curricula and for healthcare institutions to use in service redesign [23]. The subsequent pharmaceutical reform should be patient-centered, engage all relevant parties, encourage effective teamwork, and enhance the patient experience and response. Of note, these suggested that frameworks have not been validated or assessed in practice settings.
Therefore, this study aimed to validate the content of the specialized competency frameworks for pharmacists (hospital and clinical) working in hospital settings (SCF–PHS) and pilot the frameworks for practice assessment.
Methods
Source of the competency frameworks
The two frameworks were built upon previous frameworks suggested by the OPL [23]. In addition, given the challenging socioeconomic and sanitary crisis in Lebanon during the current assessment, the authors included a section on emergency preparedness, customized to the responsibilities of pharmacists in hospital settings [26,27,28,29].
Content validation of the frameworks
A panel of six pharmacy experts with academic backgrounds assessed the content of the frameworks. The panel consisted of two hospital pharmacists and four clinical pharmacists; all experts were also researchers. A Delphi technique was applied to agree by more than 90% on the suggested items until reaching a consensus [30, 31]. The final frameworks were finalized and created on Google Forms for diffusion and subsequent assessment.
Piloting the competency frameworks
This online cross-sectional study was carried out between March and October 2022. The frameworks were distributed to full-time hospital and clinical pharmacists in Lebanon (overall estimated n = 150). Pharmacists completed the questionnaire according to their role in the hospital (hospital or clinical). Respondents were briefed about the topic and the different aspects of the questionnaire before filling it out in the introductory section of the questionnaire. Each framework required approximately 30 min to be completed.
Ethics approval
The Lebanese International University Ethics and Research Committee approved the project (Approval number: 2020RC-063-LIUSOP). Before enrolling in the survey, participants were required to read and consent to the study objectives and the average expected time to complete the questionnaire. Participation was voluntary, and pharmacists received no incentive in return for their participation. No follow-up was possible as data were collected anonymously.
Sample size calculation
The CDC Epi-info software was used to calculate the minimum sample size using the [32]. The frequency was set at 90%, since the specialized competencies and domains were expected to be fulfilled by working pharmacists. Accordingly, based on a total of 150 pharmacists in hospital settings, a minimum sample size of 93 participants was required to produce an acceptable error of 5%, an expected level of competency confidence of 80%, and a 95% confidence interval, with a 5% alpha error and a power of 80%. Data collection was stopped when 96 pharmacists completed the frameworks.
Description of the questionnaires
The questionnaires were available in English, because it is a widely spoken language among health professionals in Lebanon, including pharmacists in hospital settings (Additional files 1 and 2).
The first section covered sociodemographic, educational, and professional characteristics. In this part of the questionnaire, participants were asked about several features, e.g., age, gender, nationality, area of work, university of graduation, highest educational level, years of experience, and the number of days of work per week.
The second part of the questionnaire consisted of the respective frameworks. Domains included competencies and behaviors (one question per item) related to hospital or clinical pharmacy practice. Behaviors were rated on a 5-point Likert scale from highly confident (5 points) to fairly confident (4 points), not sure/I do not know (3 points), slightly confident (2 points), and not confident at all (1 point). Competency scores were calculated by summing the answers to items (behaviors); answers were standardized over one hundred for ease of comparison.
Statistical analysis
The data were analyzed using SPSS software version 25. A descriptive analysis was performed using counts and percentages for categorical variables and means (M) and standard deviations (SD) for continuous measures, in addition to median and interquartile range (IQR). Bivariate analysis was conducted using nonparametric tests, since the normality of continuous variables was not ensured; the Mann–Whitney test was used to compare two groups, and the ANOVA was used to compare three groups or more. A p value of more than 0.05 would be considered significant.
Results
A total of 96 pharmacists (86 hospital pharmacists and 10 clinical pharmacists), who graduated from all universities in Lebanon, participated in this study. Regarding hospital pharmacists, 83.9% were females, and 35% had a BS Pharmacy. In contrast, 70% of clinical pharmacists were females, and all had a Doctor of Pharmacy degree from the Lebanese American University (LAU) or the Saint Joseph University of Beirut (USJ). Only clinical pharmacists provided direct patient care. Around 40% of participants had another field of work, such as academia and community pharmacy practice. Finally, hospital pharmacists had more years of experience than clinical pharmacists (Table 1).
Table 2 presents the factor analysis of the competencies and their related behaviors, showing adequate construct analysis. Cronbach alpha values were appropriate, indicating sufficient to high internal consistency. Overall, the competencies were distributed over five domains, i.e., fundamental skills, safe and rational use of medicines, patient-centered care, professional skills, and preparedness for emergencies (Table 2).
Table 3 displays clinical pharmacists’ competencies. Exploratory factor analysis shows the validity of the construct for the majority of competencies; patient data collection and assessment, interdisciplinary approach, professionalism and ethics, and leadership and self-management had very low variability of results. Moreover, the internal consistency of all competencies was shown to be high, except for leadership and self-management competencies, which showed a very low consistency value. Competencies were distributed on seven domains, i.e., quality improvement, clinical knowledge and skills, soft skills, ability to conduct clinical research, ability to provide effective education, use of information technology to make decisions, and emergency preparedness (Table 3).
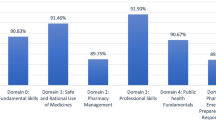
Tables 4 and 5 describe hospital and clinical pharmacy competencies domains. Pharmacists were highly confident in most competencies, with some exceptions related to research in emergency settings (data evaluation, research, and reporting).
In the bivariate analysis, hospital pharmacists who had higher degrees than a BS Pharm were more confident in Domain 3 (professional skills); those who worked in larger hospitals were more confident in Domains 1 and 3 (safe and rational use of medications and professional skills), and those who had other fields of work were more confident in Domain 1 (safe and rational use of medications) (Table 6).
Clinical pharmacists, who were English educated, had a BS Pharm, and graduated from LAU were more confident in Domain 3 (soft skills) (Table 7).
Discussion
This study could validate competency frameworks for clinical and hospital pharmacists. The factor analysis of the competencies and their respective behaviors showed an adequate construct analysis. Moreover, Cronbach alpha values were appropriate, indicating sufficient to high internal consistency.
Overall, the competencies were distributed over five domains for hospital pharmacists, i.e., fundamental skills, safe and rational use of medicines, patient-centered care, professional skills, and emergency preparedness. From the content point of view, these domains are similar (although not parallel) to those suggested by the European Association of Hospital Pharmacists [33, 34] (i.e., patient care, medicines and their use, management competencies, and professional competencies), except for the emergency preparedness aspect that was added in the current framework. Similarly, at the global level, the Basel statements (2008) included standards (not competency domains); they covered all areas of medication management in a hospital setting, including procurement, preparation and delivery, prescribing, administration monitoring of patient outcomes, and human resources, but not emergency preparedness aspects. The standards are to be upgraded in 2024 by the FIP [35, 36]. Mapping this framework to the new statements would be of primary interest.
For clinical pharmacists, competencies were distributed over seven domains, i.e., quality improvement, clinical knowledge and skills, soft skills, ability to conduct clinical research, ability to provide effective education, use information technology to make decisions and reduce errors, and emergency preparedness. The domains derived from this study encompass those suggested by the American College of Clinical Pharmacy [4] (direct patient care, pharmacotherapy knowledge, system-based care and population health, communication, professionalism, and continuous professional development) and add the areas of research, education, information technology, and emergency preparedness. However, except for emergency preparedness, the competency domains suggested in this study are closer to those developed in Sweden [37], which include clinical pharmacy practice, working relationships and communication, leadership and motivation, service development, education and training, and research and evaluation. Further mapping exercises and validation studies are warranted to confirm the validity of the suggested framework.
As for assessment results, hospital pharmacists seemed to have had more years of work experience than clinical pharmacists, most probably because of the lack of regulations requiring the presence of clinical pharmacists in hospitals throughout Lebanon [38, 39]. Although patient-centered care was provided by both hospital and clinical pharmacists, as evidenced by Domains 1 and 2 in hospital pharmacists and Domain 1 in clinical pharmacists, the reported confidence in these domains varied, being higher among clinical pharmacists. Pharmacists working in hospital settings in Lebanon, including clinical and hospital pharmacists, reported receiving appropriate orientation into their career paths from their universities. Despite adequate guidance, the professional satisfaction of having their knowledge and skills fully used was very low at 18% in comparison with other career paths [38]. Not only does this finding emphasize the importance of advocating for pharmacy practice reform as previously suggested [40], but it also calls for pharmacists and pharmacy leaders to exhibit more leadership in advocating for the full utilization of pharmacists’ skills and competencies in hospital settings. Pharmacists could be offered continuing education sessions that tackle this particular competency to enhance their expertise and satisfaction.
Indeed, the exploratory factor analysis demonstrated the validity of the construct for the majority of the competencies, except for leadership and self-management, which showed a considerably low consistency value and might be a sign of differential confidence in various leadership aspects. Several studies have identified the lack of leadership among pharmacy students in the United States [41,42,43]. In Lebanon, in a previous study, LAU pharmacy students reported that the curriculum provided them with more theoretical than practical opportunities to develop their leadership skills [44]. Nevertheless, a recent study conducted in Lebanon [45] showed that 60–70% of pharmacists reported appropriate leadership and management behaviors, but pharmacists’ overconfidence in their competencies could not be ruled out. Further studies on pharmacists’ leadership are required to depict this finding, particularly in the hospital setting. In parallel, many pharmacy schools in the United States have developed new leadership courses, programs, retreats, or other extracurricular activities in response to the recognition of leadership by different pharmacy organizations and accrediting bodies [46,47,48,49]. In Lebanon, efforts are still needed at the undergraduate and continuing education levels to improve pharmacists’ leadership.
As per Lebanese law, pharmacists are permitted to teach even if they work full-time in other institutions [38]. Both hospital and clinical pharmacists were involved in teaching/precepting 17.2% and 40%, respectively. Although the current study did not distinguish between pharmacists teaching on or off hospital premises, if it is on hospital premises, such arrangements are beneficial to all parties involved, pharmacists, student pharmacists, institutions, and patients. Student pharmacists are given the opportunity to implement the skills learned in didactic and laboratory courses, such as the pharmacist patient care process, and contribute to error interception [11, 50]. Pharmacists and institutions also benefit from having student learners as pharmacist extenders, bridging the gap from academia to practice [51].
Pharmacists who worked in larger hospitals were confident in the safe and rational use of medications and professional skills, and those who had additional fields of work were more confident in the safe and rational use of medications. This result was expected, since big hospitals are mainly teaching hospitals [39] with better clinical pharmacy services and better ranking on Lebanese accreditation systems that require continuing education for hospital staff [52]. Furthermore, pharmacists with additional fields of work might have more exposure to information, such as in academia. More studies are necessary to explore these findings.
In this study, clinical pharmacists who graduated from an American-system university had a higher confidence level in the soft skills domain. This finding should be interpreted cautiously due to the small sample size of clinical pharmacists. Nevertheless, it can be explained by the results of a study assessing the integration of the personal and professional development (PPD) subdomains (self-assessment, leadership, innovation and entrepreneurship, and professionalism) in the pharmacy curriculum at LAU School of Pharmacy. The four mapping activities performed found these subdomains to be woven across curricular, co-curricular, and extra-curricular activities and showed their sequential integration at different depths and breadths in the curriculum [44]. Such integration may be more evident in American universities, since it is required by accrediting bodies, such as the Accreditation Council for Pharmacy Education [53].
Pharmacists were highly confident in most competencies, with some exceptions related to research in emergency settings (data evaluation, research, and reporting). In 2021, the American Society of Health-System Pharmacists issued guidelines on Emergency Medicine Pharmacy Services, delineating the role of Emergency Medicine Pharmacists (EMPs), including emergency-based research and scholarly activities [54]. Pharmacy research in the emergency medicine environment is on the rise, exploring the impact of various clinical activities and describing the progress in the medication-use process and pharmacy activities in emergency settings [55]. In Lebanon, the role of hospital pharmacists in emergency settings is still undermined; an example being their role during the COVID-19 pandemic, where they had difficulties practicing despite their adequate knowledge [56]. Clinical and hospital pharmacy leaders should strive to provide the necessary evidence that demonstrates the benefit emergency medicine pharmacists can provide to the quality and safety of care in various emergency settings, such as pandemics, wars, and other disasters.
Recommendations
A national assessment of domains and competencies related to soft skills and research in emergency settings is needed at multiple levels throughout the country, including academic curricula, postgraduate training programs, drafted legislation governing pharmacy practice, and hospital accreditation standards [57]. The development of observable tasks related to each competency domain would help provide feedback and identify areas needed for professional development [58].
It is essential to improve pharmacist competency domains related to leadership and self-management. It is also necessary to incorporate more leadership-focused educational opportunities into pharmacy education, such as curricular, co-curricular, and extracurricular activities for student pharmacists, and develop targeted research to assess leadership competency outcomes. Involving students and postgraduate trainees in interprofessional education and practice teaches leadership through a collaborative rather than a vertical hierarchical approach [59, 60]. The Order of Pharmacists of Lebanon is also encouraged to establish training programs and provide continuing education opportunities that promote leadership among pharmacists [61]. Finally, advocacy for the pharmacy profession can help improve pharmacist job satisfaction and, in turn, stimulate interest, opportunities, and competency development in leadership [45].
Interventions can be instituted at multiple levels across the country to develop pharmacist competencies related to research in emergency settings. Given the recent disaster experiences in Lebanon, i.e., the COVID-19 pandemic and the Beirut blast on August 4, 2020, creating a repository of accessible publications related to pharmacist interventions or interprofessional interventions and improved patient outcomes would provide recognition for the role of pharmacists in emergency preparedness and response [29]. Moreover, such databases would serve as resources for competency development in this domain. At the academic level, pharmacy curricula across the country could educate students about emergency preparedness and response and collaborate to develop joint research initiatives to strengthen this competency among graduating professionals [40].
Limitations
Despite its importance, this pilot study has several limitations to consider. A possible selection bias could exist due to the limited number of participants in the assessment. However, even with larger samples, the reliable structure of the framework and the significant associations and differences are expected to remain unchanged. Another possible limitation is information bias, which may arise due to the lengthy questionnaire and potential fatigue of participants, in addition to the self-reported nature of the information and the possibility of not understanding all questions. Indeed, no hospital pharmacists answered positively on the direct patient care question, although they are known to review medication prescriptions in most of the Lebanese hospitals [39], as recommended by the Lebanese accreditation standards for hospitals [62]; in addition, hospital pharmacists holding degrees higher than a BS Pharm were more confident in the professional skills domain than holders of higher education degrees, which is probably an overestimation of their own performance. Nevertheless, the suspected information bias would be non-differential and only lead to results leaning toward the null. Finally, confounding could not be reduced through multivariable analysis during the assessment of associations. Therefore, further large-scale studies are recommended to overcome these limitations and confirm our results.
Conclusion
This study could validate competency frameworks for clinical and hospital pharmacists, with the competencies and their respective behaviors showing an adequate construct analysis. It also examined hospital and clinical pharmacists’ perceptions of the domains that need strengthening for an optimal public health system. Notably, domains that require further development are the soft skill domains and research in emergency settings. Both these domains are timely and needed to overcome the current practice challenges in Lebanon. A national assessment of these domains and competencies is needed at multiple levels to help develop observable tasks that would provide feedback and identify areas needed for professional development.
Data availability
The data sets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
American College of Clinical Pharmacy, Burke JM, Miller WA, Spencer AP, Crank CW, Adkins L, et al. Clinical pharmacist competencies. Pharmacotherapy. 2008;28:806–15. https://doi.org/10.1592/phco.28.6.806.
Carter BL. Evolution of clinical pharmacy in the USA and future directions for patient care. Drugs Aging. 2016;33:169–77. https://doi.org/10.1007/s40266-016-0349-2.
Aspden T, Wearn A, Petersen L. Skills by stealth: developing pharmacist competencies using art. Med Educ. 2020;54:442–3. https://doi.org/10.1111/medu.14098.
Saseen JJ, Ripley TL, Bondi D, Burke JM, Cohen LJ, McBane S, et al. ACCP clinical pharmacist competencies. Pharmacotherapy. 2017;37:630–6. https://doi.org/10.1002/phar.1923.
Jebara T, Cunningham S, MacLure K, Pallivalapila A, Awaisu A, Al Hail M, et al. A modified-Delphi study of a framework to support the potential implementation of pharmacist prescribing. Res Soc Adm Pharm RSAP. 2020;16:812–8. https://doi.org/10.1016/j.sapharm.2019.09.005.
Francis J, Abraham S. Clinical pharmacists: bridging the gap between patients and physicians. Saudi Pharm J SPJ. 2014;22:600–2. https://doi.org/10.1016/j.jsps.2014.02.011.
Chandrasekhar D, Farisa, Mathew AC, Yahiya M. Insights into the perceptions of health care providers towards clinical pharmacy services for advanced pharmaceutical care. Clin Epidemiol Glob Health. 2020;8:976–82. https://doi.org/10.1016/j.cegh.2020.03.007.
Nissen L. Pharmacist prescribing: what are the next steps? Am J Health-Syst Pharm AJHP. 2011;68:2357–61. https://doi.org/10.2146/ajhp110216.
Kucukarslan SN, Peters M, Mlynarek M, Nafziger DA. Pharmacists on rounding teams reduce preventable adverse drug events in hospital general medicine units. Arch Intern Med. 2003;163:2014–8. https://doi.org/10.1001/archinte.163.17.2014.
Viktil KK, Blix HS. The impact of clinical pharmacists on drug-related problems and clinical outcomes. Basic Clin Pharmacol Toxicol. 2008;102:275–80. https://doi.org/10.1111/j.1742-7843.2007.00206.x.
Chamoun NR, Zeenny R, Mansour H. Impact of clinical pharmacy interventions on medication error nodes. Int J Clin Pharm. 2016;38:1436–44. https://doi.org/10.1007/s11096-016-0384-4.
Hobson RJ, Sewell GJ. Supplementary prescribing by pharmacists in England. Am J Health-Syst Pharm AJHP. 2006;63:244–53. https://doi.org/10.2146/ajhp050178.
Cooper RJ, Lymn J, Anderson C, Avery A, Bissell P, Guillaume L, et al. Learning to prescribe—pharmacists’ experiences of supplementary prescribing training in England. BMC Med Educ. 2008;8:57. https://doi.org/10.1186/1472-6920-8-57.
International Pharmaceutical Federation (FIP). FIP Global Conference on the Future of Hospital Pharmacy-Final Basel Statements. Basel, Switzerland: International Pharmaceutical Federation (FIP); 2008.
Brown JN, Britnell SR, Stivers AP, Cruz JL. Medication safety in clinical trials: role of the pharmacist in optimizing practice, collaboration, and education to reduce errors. Yale J Biol Med. 2017;90:125–33.
American Society of Hospital Pharmacists. ASHP guidelines: minimum standard for pharmacies in hospitals. Am J Health-Syst Pharm AJHP. 2013;70:1619–30. https://doi.org/10.2146/sp130001.
American College of Clinical Pharmacy. Standards of practice for clinical pharmacists. Pharmacotherapy. 2014;34:794–7. https://doi.org/10.1002/phar.1438.
Forsyth P, Warren A, Thomson C, Bateman J, Greenwood E, Williams H, et al. A competency framework for clinical pharmacists and heart failure. Int J Pharm Pract. 2019;27:424–35. https://doi.org/10.1111/ijpp.12465.
Duncan N, Moreno-Martinez M-E, Pires V, Domingos V, Bonnin A, Nezvalova-Henriksen K, et al. Role and competencies of the EBMT clinical pharmacists and clinical pharmacologists: a pan-European survey. Bone Marrow Transplant. 2023. https://doi.org/10.1038/s41409-023-01983-9.
Hallit S, Sacre H, Hajj A, Sili G, Zeenny RM, Salameh P. Projecting the future size of the Lebanese pharmacy workforce: forecasts until the year 2050. Int J Pharm Pract. 2019;27:582–8. https://doi.org/10.1111/ijpp.12564.
Hallit S, Sacre H, Zeenny RM, Hajj A, Sili G, Salameh P. Credentialing and recognition of pharmacy specializations: the Lebanese order of pharmacists initiative. ACCP Int Clin Pharm. 2019;9:1–2.
Hajj A, Zeenny RM, Akel M, Sacre H, Salameh P. RESEARCH ARTICLE: the Lebanese experience for early career development: Bridging the gap to reach the International Pharmaceutical Federation (FIP) Global Competency Framework. Pharm Educ. 2022;22:211–20. https://doi.org/10.46542/pe.2022.221.211220.
Sacre H, Hallit S, Hajj A, Zeenny RM, Raad E, Akel M, et al. SHORT REPORT: upgrading pharmacy education to produce practice-ready pharmacists in Lebanon. Pharm Educ. 2020;20:379–94. https://doi.org/10.46542/pe.2020.201.379394.
Sacre H, Hallit S, Hajj A, Zeenny RM, Akel M, Raad E, et al. Developing core competencies for pharmacy graduates: the Lebanese experience. J Pharm Pract. 2022;35:332–9. https://doi.org/10.1177/0897190020966195.
Hajj A, Hallit S, Sacre H, Akel M, Zeenny RM, Salameh P. Lebanese pharmacy core competencies framework: tool validation for self-declared assessment. Int J Pharm Pract. 2021;29:598–604. https://doi.org/10.1093/ijpp/riab055.
International Pharmaceutical Federation (FIP). Responding to disasters: Guidelines for pharmacy. The Hague, The Netherlands: International Pharmaceutical Federation (FIP); 2016.
International Pharmaceutical Federation (FIP). FIP STATEMENT OF POLICY: Role of the pharmacist in disaster management. The Hague, The Netherlands: International Pharmaceutical Federation (FIP).; 2017.
International Pharmaceutical Federation (FIP). FIP Global Humanitarian Competency Framework (GbHCF). Supporting pharmacists and the pharmaceutical workforce in a humanitarian arena. Version 1. The Hague, The Netherlands: International Pharmaceutical Federation (FIP); 2021.
Aruru M, Truong H-A, Clark S. Pharmacy Emergency Preparedness and Response (PEPR): a proposed framework for expanding pharmacy professionals’ roles and contributions to emergency preparedness and response during the COVID-19 pandemic and beyond. Res Soc Adm Pharm RSAP. 2021;17:1967–77. https://doi.org/10.1016/j.sapharm.2020.04.002.
Barrett D, Heale R. What are Delphi studies? Evid Based Nurs. 2020;23:68–9. https://doi.org/10.1136/ebnurs-2020-103303.
Ng J. Delphi method: a qualitative approach for quantitative results. Value Health. 2018;21:S54. https://doi.org/10.1016/j.jval.2018.04.447.
Epi InfoTM | CDC 2022. https://www.cdc.gov/epiinfo/index.html (accessed April 13, 2023).
The Common Training Framework (CTF) Working Group. EAHP Competency Framework for Hospital Pharmacy. Hosp Pharm CTF Proj n.d. https://www.hospitalpharmacy.eu/competency-framework (accessed April 26, 2023).
Eriksson T. What is a hospital pharmacist, our competencies? Eur J Hosp Pharm. 2019;26:185–6. https://doi.org/10.1136/ejhpharm-2019-001969.
The Basel Statements on the future of hospital pharmacy. Am J Health Syst Pharm 2009;66:s61–6. https://doi.org/10.2146/ajhp080666.
Basel Statements: The future of hospital pharmacy practice. FIP Basel Statements—Req Input n.d. https://www.fip.org//basel-statements (accessed April 26, 2023).
Eriksson T, Melander AC. Clinical pharmacists’ services, role and acceptance: a national Swedish survey. Eur J Hosp Pharm Sci Pract. 2021;28:e203–6. https://doi.org/10.1136/ejhpharm-2020-002600.
Nassar E, Kassouf S, Hajj A, Sacre H, Akel M, Zeenny RM, et al. A pilot assessment of the career and job satisfaction of the pharmaceutical workforce in Lebanon. J Pharm Policy Pract. 2022;15:93. https://doi.org/10.1186/s40545-022-00498-w.
Chamoun N, Usta U, Karaoui LR, Salameh P, Hallit S, Shuhaiber P, et al. Current trends in hospital pharmacy practice in Lebanon. Hosp Pharm. 2020;55:112–8. https://doi.org/10.1177/0018578718823733.
Hajj A, Zeenny RM, Sacre H, Akel M, Haddad C, Salameh P. Pharmacy education and workforce: strategic recommendations based on expert consensus in Lebanon. J Pharm Policy Pract. 2023;16:1. https://doi.org/10.1186/s40545-022-00510-3.
Janke KK, Sorensen TD, Traynor AP. Instruction for student pharmacists on leading change. Am J Pharm Educ. 2009;73:30. https://doi.org/10.5688/aj730230.
Maine L. Maintaining the quality of education during difficult times. Am J Pharm Educ. 2010;74:55. https://doi.org/10.5688/aj740355.
White SJ, Enright SM. Is there still a pharmacy leadership crisis? A seven-year follow-up assessment. Am J Health-Syst Pharm AJHP. 2013;70:443–7. https://doi.org/10.2146/ajhp120258.
Ramia E, Salameh P, Btaiche IF, Saad AH. Mapping and assessment of personal and professional development skills in a pharmacy curriculum. BMC Med Educ. 2016;16:19. https://doi.org/10.1186/s12909-016-0533-4.
Zeineddine L, Sacre H, Haddad C, Zeenny RM, Akel M, Hajj A, et al. The association of management and leadership competencies with work satisfaction among pharmacists in Lebanon. J Pharm Policy Pract. 2023;16:48. https://doi.org/10.1186/s40545-023-00554-z.
Tucci M, Tong K, Chia K, DiVall M. Curricular and Co-curricular coverage of leadership competencies and the influence of extracurricular engagement on leadership development. Am J Pharm Educ. 2019;83:6535. https://doi.org/10.5688/ajpe6535.
Feller TT, Doucette WR, Witry MJ. Assessing opportunities for student pharmacist leadership development at schools of pharmacy in the United States. Am J Pharm Educ. 2016;80:79. https://doi.org/10.5688/ajpe80579.
Gafni Lachter LR, Ruland JP. Enhancing leadership and relationships by implementing a peer mentoring program. Aust Occup Ther J. 2018;65:276–84. https://doi.org/10.1111/1440-1630.12471.
Ali R, Alnaimi SJ, Abdulrahim S, Mraiche F. Developing leadership skills in pharmacy education. Med Sci Educ. 2022;32:533–8. https://doi.org/10.1007/s40670-022-01532-x.
Nasser SC, Chamoun N, Kuyumjian YM, Dimassi H. Curricular integration of the pharmacists’ patient care process. Curr Pharm Teach Learn. 2021;13:1153–9. https://doi.org/10.1016/j.cptl.2021.06.035.
Chamoun NR, Saad AH, Btaiche IF, Zalloua PA. Experience with clinical pharmacy implementation: bridging a gap between academia and practice in Lebanon. ACCP Int Clin Pharm. 2016;6:1–2.
Iskandar K, Raad EB, Hallit S, Chamoun N, Usta U, Akiki Y, et al. Assessing the perceptions of pharmacists working in Lebanese hospitals on the continuing education preferences. Pharm Pract. 2018;16:1159. https://doi.org/10.18549/PharmPract.2018.02.1159.
Accreditation Council for Pharmacy Education. Accreditation Standards and Key Elements for The Professional Program in Pharmacy Leading to the Doctor of Pharmacy Degree. Chicago, Illinois: Accreditation Council for Pharmacy Education; 2015.
Ortmann MJ, Johnson EG, Jarrell DH, Bilhimer M, Hayes BD, Mishler A, et al. ASHP guidelines on emergency medicine pharmacist services. Am J Health-Syst Pharm AJHP. 2021;78:261–75. https://doi.org/10.1093/ajhp/zxaa378.
Welch S. Pharmacy research in the emergency medicine environment. J Pharm Pract Res. 2019;49:104–6. https://doi.org/10.1002/jppr.1547.
Zeenny RM, Ramia E, Akiki Y, Hallit S, Salameh P. Assessing knowledge, attitude, practice, and preparedness of hospital pharmacists in Lebanon towards COVID-19 pandemic: a cross-sectional study. J Pharm Policy Pract. 2020;13:54. https://doi.org/10.1186/s40545-020-00266-8.
Engle JP, Burke JM, Ashjian EJ, Avery L, Borchert JS, Faro SJE, et al. ACCP clinical pharmacist competencies: Advocating alignment between student, resident, and practitioner competencies. JACCP J Am Coll Clin Pharm. 2020;3:124–32. https://doi.org/10.1002/jac5.1200.
Haines ST, Pittenger AL, Stolte SK, Plaza CM, Gleason BL, Kantorovich A, et al. Core entrustable professional activities for new pharmacy graduates. Am J Pharm Educ. 2017;81:S2. https://doi.org/10.5688/ajpe811S2.
Northouse PG. Leadership: theory and practice, 7th Edition. 7th ed. Los Angeles: SAGE Publications, Inc; 2015.
Reed BN, Klutts AM, Mattingly TJ. A systematic review of leadership definitions, competencies, and assessment methods in pharmacy education. Am J Pharm Educ. 2019;83:7520. https://doi.org/10.5688/ajpe7520.
Cole JD, Ballou JM, DeClue A, Ruble MJ, Noble M, Euler M, et al. The impact of leadership program formatting on perceived development within pharmacy cohorts. Am J Pharm Educ. 2023;87:ajpe9005. https://doi.org/10.5688/ajpe9005.
Ministry of Public Health. Revised Accreditation Standards for Hospitals in Lebanon-December 2022 2022. https://www.moph.gov.lb/en/Pages/3/20553/-revised-hospital-accreditation-standards-in-lebanon-december-2022 (accessed April 15, 2023).
Acknowledgements
The authors would like to express their appreciation to the members of the Clinical and Hospital Committee 2022 at the Order of Pharmacists of Lebanon (Drs. Amal Al-Hajje, Anna-Maria Henaine, Ayman Alameddine, Bahia Chahine, Carole Deeb, Iqbal Fahs, Mirella Aratimos, Samah Tawil, Sanaa Awada, Soula Abramian, Souraya Domiati, Zahra Shaitly) and to Dr. Fouad Sakr for their valuable support in facilitating the data collection process.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by KI, AH, HS, CH, JN, and PS. The first draft of the manuscript was written by NC, ER, MH, HS, and PS. All authors commented on previous versions of the manuscript and read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The Lebanese International University Ethics and Research Committee approved the project (Approval number: 2020RC-063-LIUSOP). Before enrolling in the survey, informed consent was obtained from all participants. Participation was voluntary, and pharmacists received no incentive in return for their participation. No follow-up was possible as data were collected anonymously.
Competing interests
The authors have no competing interests to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Advanced Competencies for Hospital Pharmacists.
Additional file 2.
Advanced Competencies for Clinical Pharmacists.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chamoun, N., Ramia, E., Sacre, H. et al. Validation of the specialized competency framework for pharmacists in hospital settings (SCF–PHS): a cross-sectional study. J of Pharm Policy and Pract 16, 86 (2023). https://doi.org/10.1186/s40545-023-00592-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40545-023-00592-7