
Abstract
Background
Sexual and marital satisfaction is considered one of the important factors in happiness and life satisfaction of couples. COVID-19 pandemic results in psychological effects, such as increased anxiety levels which can affect sexual and marital satisfaction. This study aimed to investigate the impact of positive psychology on women’s sexual and marital satisfaction.
Methods
A randomized controlled trial was conducted on 72 married women of reproductive age in Tabriz, Iran between February 2021 and May 2022. The participants were randomly divided into the intervention and control groups. There was no significant difference between the control and intervention groups in terms of the socio-demographic characteristics (p < 0.05). The mean age of the participants in the intervention and control groups was 31.8 ± 6.92 and 30.97 ± 5.09 years, respectively. The intervention group attended seven 60–90 min counseling sessions at weekly intervals. The Spielberger anxiety, sexual satisfaction and marital satisfaction questionnaires were completed before and four weeks after the intervention.
Results
The results of this study indicated that after counseling, the average overall score of marital satisfaction [MD: 15.46, 95% CI: 7.47 to 23.41, p = 0.034] and sexual satisfaction [MD: 7.83, 95% CI: 6.25 to 9.41, p = 0.001] significantly increased in the intervention group compared to the control group. Also, the mean score of state anxiety [MD: -2.50, 95% CI: -4.19 to -0.80, p = 0.001] and trait anxiety [MD: -1.03, 95% CI: -2.46 to -0.09, p = 0.032] significantly decreased after counseling in the intervention group compared to the control group.
Conclusions
Using counseling based on a positive psychology approach can improve anxiety, sexual and marital satisfaction, and anxiety of women of reproductive age during the COVID-19 pandemic. However, further randomized clinical trials are needed before making a definitive conclusion.
Trial registration
Iranian Registry of Clinical Trials (IRCT): IRCT20171007036615N8. Date of registration: 11/28/21. Date of first registration: 11/28/21. URL: https://www.irct.ir/user/trial/58680/view; Date of recruitment start date: 12/01/21.
Similar content being viewed by others


Background
Marital satisfaction is one of the common concepts used to evaluate marital happiness and stability. In fact, the success of marriage and couple’s satisfaction with their married life is more important than the marriage itself [1]. Marital satisfaction refers to a condition in which couples meet each other’s needs and the partner is understood, supported, and approved [2]. In general, sexual satisfaction and marital compatibility are positive and enjoyable attitudes arising from various aspects of marital relations [3]. On the other hand, marital relations are the main source of social support for most couples, acting as a protective factor against psychological and physiological injuries [4] An increase in marital satisfaction leads to the enhancement of sexual and marital satisfaction, marriage stability and consolidation of the family foundation, and even improvement of the quality of life, and success in work and social relations [4,5,6,7]. Marital satisfaction can lead to the fulfillment of many physical and psychological needs, and in case of dissatisfaction, couples and especially children will be encountered to severe psychological injuries [8]. Also, the decrease in marital satisfaction can cause dissatisfaction with sexual relations and the couple’s decision to divorce [9, 10]. Sexual and marital satisfaction are influenced by factors, such as individual variables, including women’s sexual knowledge and awareness, sexual disorders, personality traits, physical illness, and mental problems, such as anxiety and depression [11] The results of early studies revealed that sexual and interpersonal factors, communication factors, and mental health have a significant effect on marital satisfaction [12].
Global crises, such as Covid-19 are known to increase fear and anxiety, create significant disruption in daily functioning, and threaten mental health [13, 14]. During the last few years, Covid-19 pandemic has been associated with many psychological consequences, of which anxiety is one of the most common [15]. Based on the results of some studies, COVID-19 pandemic and long-term quarantine lead to the occurrence and increase of mental disorders, such as depression, anxiety, stress, post-traumatic stress, anger, and feelings of social isolation [16,17,18,19,20]. Finally, the high level of chronic stress reduces factors, such as libido [21], satisfaction with sexual life [15,16,17,18,19,20,21,22], and marital satisfaction [23], and leads to an increase in sexual dysfunction of couples [24, 25]. Therefore, the fear of COVID-19 contraction, long-term quarantine, and relatively high mortality rate caused anxiety and decreased satisfaction in relations [26, 27].
Based on the findings of psychological research, positive emotions play a significant role in the psychological recovery process of people experienced severe stress or suffered from mental disorders, such as anxiety and depression [28]. Positive psychology is a new domain of psychology that was officially founded by Professor Martin Seligman (2000), the president of the American Psychological Association. Seligman et al. believed that positive psychology is a scientific study of positive experiences and positive personal traits, and the institutions facilitating their development and seeking to improve the quality of life of people and prevent psychological damage caused by a fruitless and meaningless life [29]. The effectiveness of positive psychology-based interventions by focusing on concepts, such as gratitude, personal skills and capabilities, expressing emotions and feelings, effective communication, hope and happiness on sexual satisfaction [30], women’s marital satisfaction [25], and stress, anxiety, and depression [31] are demonstrated in past studies. However, the issues related to sexual health and fertility in times of crisis should be given special attention, since they are closely related to general health and quality of life [22].
The Covid-19 pandemic led to the prevalence of psychological complications and an increase in the level of anxiety in society [19, 32]. In the same vein, sexual and marital satisfaction is influenced by psychological factors [33], as conducted studies indicated the adverse effect of the COVID-19 pandemic on these outcomes [12]. Likewise, marital and sexual dissatisfaction affects the common life by reducing the quality of sexual life and disrupting the relationship of couples [10]. Therefore, psychological factors should be regarded to provide counseling for improving sexual and marital satisfaction. Given the adverse psychological effects of the Covid-19 pandemic in recent years and the lack of studies in this field, the present study aimed to evaluate the effect of positive psychology-based counseling on sexual and marital satisfaction and women’s anxiety during the Covid-19 pandemic.
Methods
Study design and participants
A randomized controlled trials (RCTs) are considered the highest level of evidence to establish causal associations in clinical research [34]. This type of study is a definitive tool for the evaluation of the effectiveness of an intervention and can establish a cause-and-effect relationship between an intervention and an improved disease outcome [35]. This RCT was conducted on 72 women referring to health centers in Tabriz, Iran from February 2021 to May 2022. The inclusion criteria were married women at reproductive age of 18–49 years old, having a surviving spouse, being sexually active, anxiety score from 43 to 53, sexual satisfaction score less than 100, and not receiving individual counseling services during the participation in the therapy sessions. The exclusion criteria included having a history of physical diseases influencing sexual desire (such as having organ damage, suffering from a chronic physical disease, etc.), having physically debilitating diseases (such as cancer, MS, etc.), stressful variables (such as disability or illness of a family member, such as cancer, retardation, etc.), the wife, the spouse or one of the family members mental illnesses based on the patient’s health record, the occurrence of recent unfortunate events and acute stressful problems (such as the death of a first-degree family member in the last few months, such as death of a child, father, etc.), smoking, the use of alcohol and drugs and other drugs influencing an individuals’ body and mind, taking drugs reducing libido (antidepressants: fluoxetine, sertraline, and paroxetine, antihistamines: chlorpheniramine, drugs affecting blood pressure: clonidine, captopril, benzodiazepines, such as alprazolam (Xanax), etc.), premature menopause and marital discord affecting sexual relations (such as severe marital discords leading to the petition for divorce).
Sample size
The sample size was calculated 36 per group based on the mean score of marital satisfaction in the study of Vojdani et al. (2014) [25] and considering m1 = 32.36, m2 = 42.18, sd1 = 14.22, and sd2 = 13.37, and two-sided α = 0.05, power = 80%, with the assumption of 20% attrition. Based on the variable of sexual satisfaction in the study of Gheshlaghi et al. (2012) [36] and considering m1 = 55.48, m2 = 61.03, with the assumption of 20% increase in the mean score of sexual satisfaction, sd1 = 14.13, sd2 = 13.47, and two-sided α = 0.05, and power = 80%, the sample size was estimated to be 15 per group. Owing the anxiety variable in the study of Chan et al. (2004) [37], regarding m1 = 45.56, with the assumption of 20% attrition in the anxiety score after the intervention, m2 = 36.45, SD1 = SD2 = 11.16, power = 90%, and Two-sided test, with the assumption of 20% attrition, the final sample size was obtained 34 in each group.
Sampling and random assignment
This clinical trial was conducted on 72 women of reproductive age of 18 to 49 years old referring to health centers in Tabriz, Iran. Sampling was done after obtaining permission from the ethics committee of Tabriz University of Medical Sciences (IR.TBZMED.REC.1400.677) and registration of the study in the Iranian Registry of Clinical Trials (IRCT code: IRCT20171007036615N8, Date of first registration: 11/28/21).
The city of Tabriz has 92 health centers and the details of all women of reproductive age, including phone numbers and addresses, are available in the web-based system (SIB System). The researcher attended the health centers and extracted the list of all married women of reproductive age along with their phone numbers and addresses. Then, all women were called and briefly explained the objectives and method of the study, and those who were willing to participate in the study were requested to be present at the health center at a certain time. In the first introductory session, the research objectives and method were fully explained, the inclusion criteria were examined, and eligible women signed the written informed consent form to participate in the research. Then, the Spielberger anxiety questionnaire and Larson’s sexual satisfaction questionnaire were completed and women with anxiety scores of 43–53 and sexual satisfaction scores less than 100 were included in the study. ’Other pretest questionnaires, including socio-demographic and obstetric characteristic questionnaire and Enrich’s marital satisfaction questionnaire were also completed by the participants before the intervention (in the first session( by interview. The participants were assigned into the intervention and control groups with a ratio of 1:1 by block randomization using random allocation software (RAS) with a block size of 4 and 6. Block randomization was done by a non-involved person in the sampling and data analysis. The type of allocation was written on a piece of paper and put in opaque envelopes numbered in consecutive order for allocation concealment. A non-involved person in the sampling process opened the envelopes in the order in which the participants entered the study.
Intervention
Seven counseling sessions (three face-to-face and four virtual sessions) in a group of 3 women for 90 min and in compliance with health protocols to prevent COVID-19 infection, such as masks, disinfectants, and disposable gloves, were held once a week for seven consecutive weeks by the researcher (MSc student in midwifery counseling and certified positive counseling workshop) for the intervention group in the health education hall of the nearest health center to the participants’ residence. Furthermore, the control group attended four counseling sessions (two face-to-face sessions and two virtual sessions) regarding self-care methods for breast and cervical diseases for 60–90 min. In addition, women with an anxiety score in the severe anxiety category were referred to a psychiatrist.
The summary of the content of counseling sessions is presented in the following table (Table 1):
Data collection tools
The data were collected using the questionnaire of socio-demographic characteristics, ENRICH Marital Satisfaction (EMS) Scale, Larson’s sexual satisfaction questionnaire, and Spielberger State-Trait Anxiety Inventory (STAI) before and 4 weeks after intervention by both control and intervention groups. The socio-demographic questionnaire included questions about age, age at marriage, occupation, level of education, history of illness and drug use in the individual and spouse, number of children, income sufficiency, duration of marriage, history of infertility and contraception method.
Larson’s sexual satisfaction questionnaire
Larson’s sexual satisfaction questionnaire [38], developed by Larson et al. (1998), was used to check sexual satisfaction, as the higher the score, the more sexual satisfaction. This instrument composed of the components of willingness to have sex, sexual attitude, and sexual compatibility with 25 items, scored on a 5-point Likert scale, ranging from 1 to 5 (never = 1, rarely = 2, sometimes = 3, most of the time = 4, and always = 5). The scores range from 25 to 125 and sexual satisfaction is classified into the levels of no sexual satisfaction (score less than 50), low satisfaction (score between 51 and 75), moderate satisfaction (score between 76 and 100) and high satisfaction (score above 101). The Cronbach’s alpha coefficient of the tool was estimated to be 0.93 in the study of Bahrami et al. [39].
Enrich marital satisfaction questionnaire
Enrich marital satisfaction questionnaire [40] developed by Olson and Fowers was employed to assess marital satisfaction. This tool includes the dimensions of idealistic distortion, marital satisfaction, communication, and conflict resolution. The items are scored based on a 5-point Likert scale, ranging from 1 to 5 (I completely agree = 5, I agree = 4, neither agree nor disagree = 3, I disagree = 2, and I completely disagree = 1). The total score range is between 35 and 175. A score of 0–15%,16–35%, 36–60%, 61–80%, and 81–100% represents high dissatisfaction, somewhat dissatisfaction, somewhat happiness, high happiness, and high satisfaction with all aspects of marital relations, respectively. Soleimanian [41] investigated the psychometrics of this questionnaire in Iran and its reliability was reported to be 0.9 using Cronbach’s alpha coefficient.
Spielberger state-trait anxiety inventory (STAI)
The STAI includes 40 items in two parts. The first part measures state anxiety and includes 20 items scored on a 4-point Likert scale (never = 1 to always = 4). The second part of STAI assesses trait anxiety, consisting of 20 items (21–40) scored based on a 4-point Likert scale (almost never = 1 to almost always = 4). Scores of state and trait anxieties are calculated separately and summed [42]. The total score range is between 20 and 80 for items 1 to 20 of state and trait forms. This questionnaire has been validated in Iran and its Cronbach’s alpha has been reported as 0.91 and 0.90 for state and trait anxiety, respectively [43].
Data analysis
Data were analyzed using SPSS version 26 software. The normality of quantitative data was checked using the Kolmogorov-Smirnov test and all data had a normal distribution. The socio-demographic characteristics were compared through independent t-test and Chi-square test. The independent t-test was used before the intervention and ANCOVA by adjusting the baseline score was applied four weeks after the intervention to compare the mean scores of marital and sexual satisfaction and state and trait anxiety and p < 0.05 was considered significant.
Results
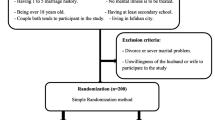
Figure 1 displays the flowchart of the study. After checking the inclusion criteria and willingness to participate in the study, out of a total of 98 women aged 18–45 years, 72 eligible women entered the study and were randomly assigned into the intervention (n = 36) and control (n = 36) groups. The number of participants remained constant throughout the study and during four four-week follow-up after the sessions ended. There was no significant difference between the control and intervention groups in terms of the socio-demographic characteristics (p < 0.05). The mean age of the participants in the intervention and control groups was 31.8 ± 6.92 and 30.97 ± 5.09years, respectively (the participant’s age range was between 19 and 47). The educational level of more than half of the women in the study groups was Bachelor’s and Master’s degree. Furthermore, less than 10% of women from each group did not have a university education. Most of the women in the intervention (61.1%) and control (80.6%) groups were housekeepers. The income level of more than half of the families was almost sufficient and about one-third of the families had completely sufficient income and only 11.1% of women in the intervention group did not have enough income (Table 2).
Before the intervention, there was no significant difference between the two groups in terms of sexual satisfaction (p = 0.97). Based on the ANCOVA test by adjusting the baseline score, the mean score of sexual satisfaction in the intervention group was significantly higher than that in the control group, four weeks after the intervention [MD: 7.83, 95% CI: 6.25 to 9.41, p = 0.001] (Table 3).
The results revealed that the intervention was effective in increasing the total score of marital satisfaction and all its components, including marital satisfaction, communication, conflict resolution, and ideal distortion. Before the intervention, the results of the independent t-test indicated no significant difference between the total score of marital satisfaction and its components between the intervention and control groups (p = 0.63). Four weeks after the intervention, the analysis of the results indicated a significant increase in the total score of marital satisfaction [MD: 15.46, 95% CI: 7.47 to 23.41, p = 0.03] (Table 4). Before the intervention, there was no significant difference in the state (p = 0.33) and trait (p = 0.73) anxiety scores between the intervention and control groups. After the intervention, a significant decrease was observed in the level of state anxiety [MD: -2.50, 95% CI, -4.19 to -0.80, p = 0.001] and trait anxiety [MD: -1.03, 95% CI: 2.46 to -0.09, p = 0.03] in the intervention group compared to the control group (Table 5).

Flowchart of the study
Discussion
Positive psychology interventions can be effective in the enhancement of subjective and psychological well-being, as well as in helping to reduce depressive symptoms [44]. The application of topics such as meaning, coping, self-compassion, courage, gratitude, character strengths, positive emotions, positive interpersonal processes, and high-quality communication in positive psychology has also been demonstrated in supporting individuals during a pandemic [45]. Based on the findings, holding counseling sessions with a positive approach can increase the sexual and marital satisfaction of women of reproductive age and reduce their anxiety during the COVID-19 pandemic.
The results showed positive counseling increases women’s sexual satisfaction from medium to high level in the intervention group after receiving counseling. In line with the results of the present study, Salehi Moghaddam et al. [46] examined the effectiveness of the sexual skills training program on women’s sexual satisfaction and the sexual satisfaction score before and after counseling in the intervention group was higher than that in the current study and was in the range of high sexual satisfaction. However, positive counseling resulted in a greater increase in the sexual satisfaction score in the present study. Further, in the study of the effect of mindfulness counseling on improving the sexual satisfaction of women of reproductive age [47], the sexual satisfaction score of 20 women in the intervention group significantly increased after receiving the counseling. The increase in the sexual satisfaction score in the aforementioned study was more than in the present study and the effect of combining the online sessions with face-to-face sessions and the special conditions of the Covid-19 pandemic in the current study are considered as influential factors. Alimohammadi et al. [48] investigated the effectiveness of group counseling based on Bandura’s self-efficacy theory on the sexual satisfaction of newlywed women and reported no statistically significant difference between the two groups in terms of sexual satisfaction (p = 0.058), which was inconsistent with the findings of the present study. The researchers revealed that the duration of the follow-up and the limited number of counseling sessions affect the ineffectiveness of the intervention on women’s sexual satisfaction. This study demonstrated the necessity of conducting psychological interventions with diverse and innovative approaches to find the most effective intervention based on the desired outcome. To the best of our knowledge, no study similar to the present study was found during the COVID-19 pandemic in the literature review.
The results of the present study illustrated that positive psychology (optimistic) based counseling was effective in increasing the total score of marital satisfaction and all its components. The highest enhancement was seen in marital satisfaction and conflict resolution, respectively. Actually, positive psychology-based counseling is effective in reducing differences and increasing the ability to control conflicts between couples through creating positive feelings and increasing the capability and self-confidence of the studied women. Finally, the formation of better marital relations and fewer conflicts lead to the improvement of marital satisfaction of couples. In another study, Zahedi et al. [49] compared the effect of acceptance and commitment therapy (ACT) and cognitive-behavioral therapy (CBT) on marital satisfaction of 45 women assigned into the ACT, CBT, and control groups. They indicated that the marital satisfaction of women increased in both intervention groups and ACT-based counseling had a greater impact on women’s marital satisfaction compared to the CBT-based counseling. In a study, Zarei Abolkheir et al. [50] reported that although CBT-based counseling is effective in increasing women’s marital satisfaction, this increase was not statistically significant. The counseling content was provided to the participants in the form of five online audio files for 5 weeks. Uncertainty of the follow-up sessions by the participants can be a reason for the results of the study.
The results of the present study illustrated that positive psychology-based counseling is effective on the state-trait anxiety of women and reduces their anxiety. It is worth mentioning that despite the significant decrease in the anxiety score of women in the intervention group after receiving the intervention, the mean score of state-trait anxiety was still at an average level. In line with the findings of the present study, the investigation of the effect of online psychological interventions, including CBT, stress reduction techniques, mindfulness, and positive counseling on the anxiety of patients with COVID-19 [51] indicated the positive effect of the intervention in reducing the participants’ anxiety. In the same vein, Jinzhi Li et al. [52] denoted the effectiveness of CBT-based counseling on mental health and reducing anxiety in patients with COVID-19. Further, Dincer and Inangil [53] evaluated the effect of Emotional Freedom Techniques (EFT) on the anxiety level of nurses during the COVID-19 epidemic using the Spielberger questionnaire and reported that the intervention led to a decrease in the anxiety score in the intervention group. The state anxiety score in the aforementioned study was reduced more than that in the present study, and trait anxiety was not investigated. The presence of participants from among educated people and medical staff can influence the better results of the study.
In addition, the results of some descriptive studies demonstrated the negative effects of the COVID-19 pandemic on the outcomes investigated in the present study. A study in Spain indicated that quarantine affected the sexual life of half of the people studied (47.7%), especially women [54]. Although the number of sexual relations increased among the participants compared to before, the scores of the sexual performance index of women were higher before the Covid-19 pandemic and the quality of sexual life of people decreased during the Covid-19 epidemic [21]. Researchers in a review study reported that the marital satisfaction of couples decreased during the Covid-19 pandemic and consequently, the couple’s common life is at risk and psychoeducational counseling is required for couples to improve marital adjustment and communication, emotion regulation, conflict management, and problem resolution during the Covid-19 pandemic [55]. The stress inflicted on couples during the COVID-19 pandemic decreases their marital satisfaction level. Therefore, researchers suggested that psychological interventions should be done considering the damage inflicted on the couples during the COVID-19 pandemic [56], indicating the importance and necessity of appropriate educational and counseling interventions to improve couples’ relationships and their mental health level during the COVID-19 pandemic.
Given that mental health and the level of stress and anxiety of people are closely associated with the quality of their marital health [2, 20, 57], women with low sexual and marital satisfaction and high-stress levels were selected as the target population in the present study. Therefore, it is recommended to consider mental health and the quality of marital relations when providing counseling programs during the epidemic of physical diseases. Additionally, based on the results of the conducted studies, the level of knowledge of marital relations and sexual awareness plays an important role in the level of sexual satisfaction [58] and the quality and stability of marital relations of couples [11]. Therefore, it seems that increasing women’s sexual awareness and empowering them in communication skills can be effective in preventing marital disputes and couples’ dissatisfaction.
Strengths and limitations
One of the strengths of this study is observing all principles of randomized controlled trial, including random allocation and allocation concealment. Also, providing practical exercises in each session for a better understanding of the topics raised is one of the strengths of the study. Standard and valid questionnaires were used in the present study, which their psychometric properties have been assessed in Iran already. The limitation of this study was that it coincided with the coronavirus pandemic and severe restrictions due to social distancing and quarantine for counseling sessions. In addition, it was not possible to blind the participants and data assessor due to the nature of the intervention. Further, other limitations are the relatively small sample size and the short follow-up period. Therefore, it is recommended to conduct randomized clinical trials with larger sample size and longer follow-up period.
Conclusion
In general, the results indicated that counseling leads to an increase in sexual and marital satisfaction among women. Therefore, counseling techniques, such as positive psychology can be used to improve women’s satisfaction with their marital relations and sex lives, and help women manage their marital problems and disputes and reduce their anxiety in critical and special situations. In addition, family health policymakers should pay more attention to the negative effects of health crisis conditions on the satisfaction of couples and women’s mental health, and provide solutions to improve marital relations and prevent wide-ranging disputes in the family through holding counseling sessions. It is also suggested to create programs to increase the awareness of health care providers about the important role of marital satisfaction in the health of the family and society, and lead health care providers to identify and improve sexual problems. This can be implemented by changing the continuing education programs or adding psychology units to the educational curriculum of universities and using senior experts in counseling in midwifery in health centers. Holding monthly meetings, providing educational sites and group meetings for discussion and counseling with the presence of a positive psychotherapist in person or online are also suggestions that can be implemented in health care centers.
Data availability
Data sets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- AMD:
-
Adjusted Mean Difference
- MD:
-
Mean Difference
- STAI:
-
State-Trait Anxiety Inventory
References
Khalatbari J, Ghorbanshiroudi S, Azari KN, Bazleh N, Safaryazdi N. The relationship between marital satisfaction (based on religious criteria) and emotional stability. Procedia-social Behav Sci. 2013;84:869–73.
Rahimi A, Amiri H, Afsharriniya K, Arefi M. Comparing the effectiveness of cognitive behavioral therapy (CBT) with Acceptance and Commitment Therapy (ACT) in the enhancement of marital satisfaction and sexual intimacy in couples referred to counseling centers. Avicenna J Neuropsychophysiology. 2020;7(2):126–32.
Mansouri N, Rasouli A. The effectiveness of group therapy based on acceptance and commitment to increase the life expectancy, marital intimacy and reducing the marital conflicts of women. Iran J Psychiatric Nurs. 2019;7(1):82–8.
Aman J, Abbas J, Nurunnabi M, Bano S. The relationship of religiosity and marital satisfaction: the role of religious commitment and practices on marital satisfaction among Pakistani respondents. Behav Sci. 2019;9(3):30.
Heiman JR, Long JS, Smith SN, Fisher WA, Sand MS, Rosen RC. Sexual satisfaction and relationship happiness in midlife and older couples in five countries. Arch Sex Behav. 2011;40(4):741–53.
Mark KP, Milhausen RR, Maitland SB. The impact of sexual compatibility on sexual and relationship satisfaction in a sample of young adult heterosexual couples. Sex Relatsh Therapy. 2013;28(3):201–14.
Rahmani A, Khoei EM, Gholi LA. Sexual satisfaction and its relation to marital happiness in iranians. Iran J Public Health. 2009;38(4):77–82.
Kamaly A, Dehghani S, Ghasemi H. Meta-analysis of effectiveness of psychological interventions–counseling on enhancing marital satisfaction (Iran: 2002_2012). Couns Psychother Cult. 2014;5(19):95–122.
Merghati Khoei E, Maasoumi R, Talebi S, Hajimirzaie S, Bayat A, Rimaz S, et al. Factors affecting sexual satisfaction in Iranian women. Women’s Health Bull. 2015;2(4):1–4.
Tavakol Z, Nikbakht Nasrabadi A, Behboodi Moghadam Z, Salehiniya H, Rezaei E. A review of the factors associated with marital satisfaction. Galen Med J. 2017;6(3).
Mofid V, Ahmadi A, Etemadi O. The comparison of cognitive-behavioral counseling and solution-oriented counseling on women’s sexual satisfaction in Isfahan. 2014.
Banaei M, Safarzadeh S, Moridi A, Dordeh M, Dashti S, Abdi F et al. Associated factors of marital satisfaction in Iranian women during the covid-19 pandemic: a population-based study. Shiraz E-Medical J. 2021;22(11).
Schimmenti A, Billieux J, Starcevic V. The four horsemen of fear: an integrated model of understanding fear experiences during the COVID-19 pandemic. Clin Neuropsychiatry. 2020;17(2):41.
Wang C, Pan R, Wan X, Tan Y, Xu L, McIntyre RS, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. 2020;87:40–8.
Bäuerle A, Teufel M, Musche V, Weismüller B, Kohler H, Hetkamp M, et al. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: a cross-sectional study in Germany. J Public Health. 2020;42(4):672–8.
Shah SMA, Mohammad D, Qureshi MFH, Abbas MZ, Aleem S. Prevalence, psychological responses and associated correlates of depression, anxiety and stress in a global population, during the coronavirus disease (COVID-19) pandemic. Commun Ment Health J. 2021;57(1):101–10.
Othman N. Depression, anxiety, and stress in the time of COVID-19 pandemic in Kurdistan region, Iraq. Kurdistan J Appl Res. 2020:37–44.
Xiong J, Lipsitz O, Nasri F, Lui LM, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64.
Khademian F, Delavari S, Koohjani Z, Khademian Z. An investigation of depression, anxiety, and stress and its relating factors during COVID-19 pandemic in Iran. BMC Public Health. 2021;21(1):1–7.
Karli P, Gürbüz T, Şentürk M. COVID-19 pandemic and the quality of couples’ sexual relationships. Anatol Curr Med J. 2021;3(2):104–8.
Yuksel B, Ozgor F. Effect of the COVID-19 pandemic on female sexual behavior. Int J Gynecol Obstet. 2020;150(1):98–102.
Döring N. How is the COVID-19 pandemic affecting our sexualities? An overview of the current media narratives and research hypotheses. Arch Sex Behav. 2020;49(8):2765–78.
Kasalova P, Prasko J, Holubová M, Vrbova K, Zmeskalova D, Slepecky M, et al. Anxiety disorders and marital satisfaction. Neuroendocrinol Lett. 2018;38(8):555–64.
Yazdanpanahi Z, Beygi Z, Akbarzadeh M, Zare N. To investigate the relationship between stress, anxiety and depression with sexual function and its domains in women of reproductive age. Int J Med Res Health Sci. 2018;5(10):223–31.
Vojdany S, Golzari M, Borjali A. The effectiveness of positive psychotherapy on depression and marital satisfaction of depressed women. J Appl Psychol. 2014;8(2):30.
Panzeri M, Ferrucci R, Cozza A, Fontanesi L. Changes in sexuality and quality of couple relationship during the COVID-19 lockdown. Front Psychol. 2020:2523.
Reizer A, Koslowsky M, Geffen L. Living in fear: the relationship between fear of COVID-19, distress, health, and marital satisfaction among Israeli women. Health Care Women Int. 2020;41(11–12):1273–93.
Yamaguchi K, Takebayashi Y, Miyamae M, Komazawa A, Yokoyama C, Ito M. Role of focusing on the positive side during COVID-19 outbreak: Mental health perspective from positive psychology. Psychol Trauma: Theory Res Pract Policy. 2020;12(S1):S49.
Seligman ME, Csikszentmihalyi M. Positive psychology: an introduction. Flow and the foundations of positive psychology. Springer; 2014. pp. 279–98.
Haroon Rashidi H, Kiyaniyan Mehr Z. The effect of the positive couple therapy on the marital intimacy and sexual satisfaction of female students. Family Pathol Couns Enrich J. 2019;5(1):125–38.
Anderson A, Hattie J, Hamilton RJ. Locus of Control, Self-Efficacy, and motivation in different schools: is moderation the key to success? Educational Psychol. 2005;25(5):517–35.
Hawes MT, Szenczy AK, Klein DN, Hajcak G, Nelson BD. Increases in depression and anxiety symptoms in adolescents and young adults during the COVID-19 pandemic. Psychol Med. 2022;52(14):3222–30.
Zaheri F, Dolatian M, Shariati M, Simbar M, Ebadi A, Azghadi SBH. Effective factors in marital satisfaction in perspective of Iranian women and men: a systematic review. Electron Physician. 2016;8(12):3369.
Jadad AR, Enkin MW. Randomized controlled trials: questions, answers and musings. Wiley; 2007.
Vamvakas EC. Rationale, objectives, and interpretation of randomized controlled trials. J Clin Apheresis Off J Am Soc Apheresis. 1997;12(3):130–9.
Gheshlaghi F, Dorvashi G, Aran F, Shafiei F, Najafabadi GM. The study of sexual satisfaction in Iranian women applying for divorce. Int J Fertility Steril. 2014;8(3):281.
Chan Y, Lee P, Ng T, Ngan H. Could precolposcopy information and counseling reduce women’s anxiety and improve knowledge and compliance to follow-up? Gynecol Oncol. 2004;95(2):341–6.
Larson JH, Anderson SM, Holman TB, Niemann BK. A longitudinal study of the effects of premarital communication, relationship stability, and self-esteem on sexual satisfaction in the first year of marriage. J Sex Marital Ther. 1998;24(3):193–206.
Bahrami N, Yaghoob Zadeh A, Sharif Nia H, Soliemani MA, Haghdoost AA. Validity and reliability of the persian version of Larson sexual satisfaction questionnaire in couples. J Kerman Univ Med Sci. 2016;23(3):344–56.
Fowers BJ, Olson DH. ENRICH marital inventory: a discriminant validity and cross-validation assessment. J Marital Fam Ther. 1989;15(1):65–79.
Soleimanian A. An investigation on illogical thoughts on marital satisfaction. Tehran: Tarbiat Moallem University; 1997.
Spielberger CD. State-trait anxiety inventory for adults. 1983.
Rigi F, Feizi A, Naseri M, Salehi Ardabili S, Bazdar P. The effect of foot reflexology on anxiety in patients with coronary artery bypass surgery referred to Seyed-Al-Shohada teaching hospital, Urmia, 2012. Nurs Midwifery J. 2013;11(8):0.
Bolier L, Haverman M, Westerhof GJ, Riper H, Smit F, Bohlmeijer E. Positive psychology interventions: a meta-analysis of randomized controlled studies. BMC Public Health. 2013;13:1–20.
Waters L, Algoe SB, Dutton J, Emmons R, Fredrickson BL, Heaphy E, Moskowitz JT, Neff K, Niemiec R, Pury C, Steger M. Positive psychology in a pandemic: Buffering, bolstering, and building mental health. J Positive Psychol. 2022;17(3):303-23.
Moghaddam FS, TorkZahrani S, Moslemi A, Azin SA, Ozgoli G, Rad NJ. Effectiveness of sexual skills training program on promoting sexual intimacy and satisfaction in women in Tehran (Iran): a randomized clinical trial study. Urology J. 2020;17(3):281-8.
Farajkhoda T, Sohran F, Molaeinezhad M, Fallahzadeh H. The effectiveness of mindfulness-based cognitive therapy consultation on improving sexual satisfaction of women in reproductive age: a clinical trial study in Iran. J Adv Pharm Educ Res. 2019;9(S2).
Alimohammadi L, Mirghafourvand M, Zarei F, Pirzeh R. The effectiveness of group counseling based on Bandura’s self-efficacy theory on sexual function and sexual satisfaction in Iranian newlywed women: a randomized controlled trial. Appl Nurs Res. 2018;42:62–9.
Zahedi Z, Azizi A, Rahmani S, Zarein F, Ranjbar M. Compare the effectiveness of Acceptance and Commitment Therapy and cognitive-behavioral therapy on marital satisfaction. Family Couns Psychother. 2021;10(2):75–100.
Zarei Abolkheir A, Allahdadian M, Mosharraf S, Ghasemi Tehrani H. Exploring the Effect of cognitive–behavioral counseling on marital satisfaction and quality of life through virtual education. Avicenna J Nurs Midwifery Care. 2021;29(1):53–60.
Shaygan M, Yazdani Z, Valibeygi A. The effect of online multimedia psychoeducational interventions on the resilience and perceived stress of hospitalized patients with COVID-19: a pilot cluster randomized parallel-controlled trial. BMC Psychiatry. 2021;21(1):1–12.
Li J, Li X, Jiang J, Xu X, Wu J, Xu Y, et al. The effect of cognitive behavioral therapy on depression, anxiety, and stress in patients with COVID-19: a randomized controlled trial. Front Psychiatry. 2020;11:580827.
Dincer B, Inangil D. The effect of Emotional Freedom techniques on nurses’ stress, anxiety, and burnout levels during the COVID-19 pandemic: a randomized controlled trial. Explore. 2021;17(2):109–14.
Ballester-Arnal R, Nebot-Garcia JE, Ruiz-Palomino E, Giménez-García C, Gil-Llario MD. INSIDE project on sexual health in Spain: sexual life during the lockdown caused by COVID-19. Sexuality Res Social Policy. 2021;18(4):1023–41.
Epifani I, Wisyaningrum S, Ediati A, editors. Marital distress and satisfaction during the COVID-19 pandemic: a systematic review. International Conference on Psychological Studies (ICPSYCHE 2020); 2021: Atlantis Press.
Turliuc MN, Candel OS. Not all in the same boat. Socioeconomic differences in marital stress and satisfaction during the Covid-19 pandemic. Front Psychol. 2021;12:635148.
Mousavi SF. Psychological well-being, marital satisfaction, and parental burnout in Iranian parents: the effect of home quarantine during COVID-19 outbreaks. Front Psychol. 2020;3.305.
Besharat MA, Rafiezadeh B. Prediction of sexual satisfaction and marital adjustment levels according to job variables, commitment, intimacy, and sexual knowledge and attitude. J Fam Psychol. 2021;3(1):31–46.
Acknowledgements
The author would like to express his gratitude to all the officials of Tabriz University of Medical Sciences, the personnel of the studied health centers, and also to all the women who patiently attended the counseling sessions.
Funding
This study was done with the budget of Tabriz University of Medical Sciences. The funding agency had no role in the study design, collection, analysis and interpretation of data and writing of the manuscript.
Author information
Authors and Affiliations
Contributions
Authors’ contributions MAB contributed to the concept and design, data collection, conducting consultation sessions and drafting the manuscript. EM contributed to the conception and design, data collection, blinded data analysis, data interpretation, and writing of this manuscript. RN, SH, and SAM contributed to the conception and design of the interpretation and revision of this manuscript. All authors gave their final approval for publication of this manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent for the company
The ethics committee of Tabriz University of Medical Sciences, Tabriz, East Azerbaijan Province, Iran approved this study (IR.TBZMED.REC.1400.677) and it was registeredin the Iranian Registry of Clinical Trials (IRCT code: IRCT20171007036615N8). Written informed consent was obtained from all individual participants who participated in the study. In present study all methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Bafrani, M.A., Nourizadeh, R., Hakimi, S. et al. The impact of positive psychology counseling on sexual and marital satisfaction and anxiety among reproductive-aged women during the COVID-19 pandemic: a randomized controlled clinical trial. BMC Psychol 12, 313 (2024). https://doi.org/10.1186/s40359-024-01826-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-024-01826-2