
Abstract
Purpose
This review seeks to examine the current state of postpartum social support and psychosocial conditions among women around the world, as well as explore the relationship between these factors. Additionally, it aims to propose a logical framework for enhancing postpartum social support and psychosocial conditions in this population.
Methods
Following the development of a search strategy, two databases, PubMed and Science Direct, were searched for studies published between January 2019 and May 2023. The search was conducted throughout the entire month of May 2023. The risk of bias in the included cross-sectional studies was assessed using the Newcastle–Ottawa Quality Assessment Scale, which was adapted for this specific study design. To determine if the main objective of the cross-sectional studies was to investigate the relationship between social support and postpartum psychosocial conditions, a review was conducted based on the AMSTAR checklist, PRISMA checklist and PRISMA flow diagram. Data extraction was performed with the consensus of two authors, and a narrative synthesis approach was chosen for data synthesis, following the guidelines provided by the Centre for Reviews and Dissemination (CRD).
Results
Eleven cross-sectional studies were included in the final analysis. Our findings revealed that all reviewed studies provided evidence of a positive association between social support and healthy psychosocial conditions in postpartum period. However, due to the absence of standardized measurement indicators to identify and compare the outcomes of various studies, there was a need to develop a conceptual framework that could enhance our understanding of the postpartum psychosocial condition including anxiety, depression, unfavorable quality of life and social support status up to 24 month after child birth. This framework aimed to incorporate childbirth and motherhood as "stressful events," while considering social support as a crucial "coping resource." Furthermore, it acknowledged empowerment, help-seeking behavior, and peer support as important "coping actions," alongside implementing client-centered interventions. Lastly, it recognized postpartum mental health and optimal quality of life as significant "effects" of these factors.
Conclusions
The proposed conceptual framework could define postpartum women’s health as “the ability to adapt and self-manage.”
Similar content being viewed by others


Introduction
Birth and motherhood are considered neuro-psycho-social events, and the first year postpartum, although a pleasant time for a family, is a crucial developmental life stage for women [1, 2]. During this transitional period, women face a dual challenge: Firstly, they must adapt to the changes in their physical appearance and the added expectations of new responsibilities. Secondly, they experience physical discomforts resulting from pregnancy and childbirth, potential marital discord, and negative social interactions such as conflict, insensitivity and interference, especially with their husbands [2,3,4]. These changes and problems can be challenging and far-reaching, resulting in undesirable psychosocial well-being or psychosocial problems [5,6,7].
Psychosocial well-being is a superordinate construct that includes emotional or psychological well-being, as well as social and collective well-being [5]. So, postpartum psychosocial problems are defined as anxiety, depression, other mental disorders, unfavorable quality of life and increasing the incidence of suicidal ideation and behavior [1, 5,6,7]. Postpartum depression (PPD) is a type of major depressive episode that occurs during pregnancy or within 4 weeks following delivery [8]. Another related illness is postpartum post-traumatic stress disorder (PP-PTSD), which is an anxiety disorder that can develop as a result of a difficult or traumatic birth experience. It's important to note that women may experience PP-PTSD even after a successful birth [9]. Both PPD and anxiety disorder are serious psychosocial problems that require proper diagnosis and treatment [8, 9]. Notably, postpartum psychosocial problems can impede successful adjustment to the maternal role, impact the entire family, and impose significant economic costs on the healthcare system [10,11,12].
However, current postpartum care, which is often standardized in terms of content and structure, is associated with low satisfaction rates among mothers [13]. Furthermore, most studies focusing on mothers’ health outcomes in the postpartum period have centered on measures such as breastfeeding rates, hospital admissions, and physical health indicators of mothers and infants [14,15,16,17]. While these outcomes are undoubtedly important, mothers have also indicated that maternal functioning and mental health are essential for health [14, 18, 19]. To aid in coping with the stress of motherhood and promote maternal well-being, effective social support can be instrumental in facilitating a successful transition to motherhood [20,21,22].
Theoretical frameworks suggest that social support, which refers to the availability of others to provide emotional, psychological, and material resources, can serve as a coping resource that impacts health [23]. In addition, social support is also recognized as a protective factor against stress, anxiety, depression, and other mental disorders that can negatively impact the quality of life [24,25,26]. Negative postpartum health outcomes highlight the critical need for increased support and resources [14].
Further investigation is necessary to deepen our understanding of the status of social support after childbirth and how it can contribute to maternal psychosocial well-being during the transition to motherhood [20]. Although psychosocial conditions are crucial, because of persistent mother’s mental disorders up to 24 months after childbirth, they are often not the primary focus of research [24, 25]. Mothers’ low satisfaction rates with standardized postpartum care also highlight the need for a client-centered approach [13]. Ultimately, by identifying evidence-based factors that affect women’s psychosocial conditions and the necessity for plans in this area, postpartum can be one of life’s most pleasant experiences, and the challenges confronting them can be an opportunity for personal growth and skill enhancement [11].
In fact, the majority of current studies on postpartum women primarily focus on physical issues such as postpartum bleeding or pain, as well as psychological problems like breastfeeding difficulties and PPD [15,16,17]. Unfortunately, other psycho-social conditions that arise after childbirth are often overlooked and receive little attention [14, 24, 25]. To enhance the psycho-social well-being of women following childbirth, it is crucial to gain a comprehensive understanding of these conditions and assess the factors that influence them [11, 18]. Among these factors, social support plays a significant role and warrants further investigation to determine its importance during the postpartum period [20, 26].
Based on the background above, the current review aims to achieve the following objectives: 1) to explore evidence for the status of women’s social support in postpartum period (up to 24 month after child birth), 2) to assess the evidence for the status of women’s psychosocial problems including anxiety, PPD and unfavorable quality of life up to 24 month after child birth, 3) to evaluate the evidence for associations between social support and psychosocial problems in postpartum period, and 4) to propose a logical framework for enhancing postpartum social support and psychosocial conditions.
Materials and methods
The present study utilized a systematic review based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) [27] checklist, We chose two databases based on recommendations from the PRISMA group paper, which suggests searching at least one database, and the Assessing the Methodological Quality of Systematic Reviews (AMSTAR) checklist, which recommends searching at least two databases [28, 29]. Our search included well-known databases PubMed and Science Direct, and we used the following search strategy: keywords for each search term (Table 1), Field “Title/Abstract,” free full-text (access to some scientific articles is limited for Iranian universities due to debt, not having a subscription, etc.). Our investigation covered a period of five years, from January 2019 to May 2023. This timeframe was chosen to ensure that our evidence syntheses were as up-to-date as possible when published, as this is often neglected by authors of overviews [30].
Study criteria
The inclusion criteria for the studies consisted of four key factors: (1) the participation of postpartum mothers up to 24 months, as research has shown that mothers can continue to experience mental disorders for up to 24 months after giving birth. This extended timeframe highlights the need for ongoing support and care for postpartum mothers beyond the traditional 12-month postpartum period [25]; (2) the use of self-administered questionnaires or scales to assess social support; (3) publication in full-text English; and (4) a descriptive or cross-sectional designs. Since, according to the Oxford Center's table of Evidence-Based Medicine 2011 and Dehkordi AH et al. review study, a review of descriptive or cross-sectional studies is necessary to examine the status of a medical or health condition and its relationship with other conditions [31, 32].
Exclusion criteria included studies that were: (1) clinical/controlled trials, qualitative, longitudinal, or non-original articles; (2) solely for psychometric purposes; and (3) targeted specific groups of postpartum women.
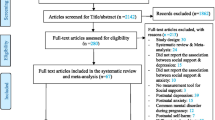
A total of 991 articles were initially identified in various databases and imported into EndNote X7 software [33], with duplicates removed. Out of the 956 articles, 19 papers were selected for inclusion after being assessed for relevance by two independent reviewers who achieved consensus on which studies to include [27]. Eight full-text studies were excluded due to failure to report intended results (n = 2) and no intended design (n = 6). Finally, 11 papers were reviewed. The study search and selection process are illustrated in Fig. 1.

Study search and selection process
Risk of bias in included studies
The Newcastle–Ottawa Quality Assessment Scale (adapted for cross-sectional studies) [34] was used to determine the risk of bias. Five studies (45%) were determined to have a low risk of bias, 6 of them (55%) were a medium risk of bias, and no study (0%) was assessed as having a high risk of bias. Figure 2 presents the details of the risk-of-bias items separately for each article.

Summary of risk of bias; authors' assessment of the risk of bias for each study
Data synthesis
A meta-analysis is often not feasible due to the presence of significant heterogeneity in quantitative indices or measurement tools. In such cases, a narrative approach to synthesis may be more appropriate and effective [32, 35]. So, in present study a narrative and deductive approach to synthesis was selected, following the steps outlined in the Centre for Reviews and Dissemination (CRD). These steps included developing a preliminary synthesis of the results of included studies, exploring relationships in the data, and considering the robustness of the synthesis [36].
Results
Description of studies
Eleven cross-sectional studies were included in the final analysis, and the majority of studies (N = 8) took place in Asian nations. Only one study was conducted in Europe, while two were conducted in Africa. The maximum time after childbirth was 18 months. The characteristics of the studies are shown in Table 2.
Aim 1: Status of Postpartum Social support
Five studies used the Multidimensional Scale of Perceived Social Support (MSPSS) to assess social support. In comparison, two studies utilized the Maternity Social Support Scale (MSSS), and the remaining employed different questionnaires (see Tables 2 and 3).
In two studies, the majority of women reported their postpartum social support level as medium (56.1% and 53%) [42, 46]. In three other studies, most women reported high-level social support (ranging from 39.5% to 66.6%) [8, 40, 43]. However, one study found that 73.3% of participants had low social support [44]. Additionally, in two studies, the authors interpreted the level of postpartum social support based on its mean score as moderate and high [37, 39]. It is important to note that the scoring for social support varied across these studies, as shown in Table 3.
Aim 2: Status of postpartum psychosocial conditions
The Edinburgh Postnatal Depression Scale (EPDS) was utilized in all, but one of the studies [39]. The prevalence of Postpartum Depression (PPD) with a score of ≥ 13 was reported as 22%- 29.08% in four of the studies [8, 40, 41, 44]. Meanwhile, three studies reported the prevalence of PPD with a score of ≥ 10 as 21.3%- 41.49% [41,42,43, 45]. Furthermore, one study reported the prevalence of PPD with a score of ≥ 8.5 as 23.7% [46] (Table 3).
The prevalence of anxiety was assessed using the Perinatal Post-Traumatic Stress Questionnaire (PPQ) with a score of ≥ 19 and the State-Trait Anxiety Inventory (STAI) with a score of ≥ 75 percentile, reported rates of 6.1% and 27.80%, respectively [8, 45] (Table 3). The PPQ is a self-rating scale to identify women suffering from PTSD symptoms (i.e. re-experiencing, avoidance- numbing, and hyperarousal) at 1–18 months postpartum [8].
The level of mental health was assessed using the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) in a study, with authors interpreting the mean score as low [38] (refer to Table 3 for details).
Only three studies explored the postpartum quality of life using the World Health Organization Quality of Life Assessment-BREF (WHOQOL-BREF), Spiritual Wellbeing Scale (SWBS), and Postpartum Quality of Life (PQOL). In a study, the level of PQOL was interpreted as medium based on its mean score [39]. Additionally, findings from a separate study showed that 72.43% of non-depressive women had a high score (100–120) on SWB [44] (Table 3).
Aim 3: Association between postpartum social support and psychosocial conditions
Ten studies were identified that investigated the association between social support and postpartum depression (PPD), with results showing that social support was a statistically significant factor in the development of PPD [8, 37, 38, 40,41,42,43,44,45,46]. Only three studies, however, evaluated the link between women’s social support and mental health disorders such as anxiety and PTSD in postpartum period. These studies suggested that low levels of social support were a contributing risk factor for postpartum anxiety and other mental illnesses [8, 38, 45] (the statistical tests used are given in Table 2).
Moreover, three studies specifically examined the association between social support and quality of life in the postpartum period, where an association was confirmed [37, 39, 41, 44]. Furthermore, two of these studies found that this relationship was reciprocal [39, 44] (the statistical tests used are given in Table 2).
Figure 3 summarizes the studies, analyses, and syntheses pertaining to the relationship between social support and psychosocial conditions in the postpartum period.

Relationship between social support and psychosocial conditions in postpartum period
Discussion
In this study, we systematically reviewed cross-sectional reports on the relationships between social support and psychosocial conditions in postpartum period. This review pursued four aims: 1) to explore evidence for social support status in postpartum period, 2) to assess the evidence for psychosocial conditions status in postpartum period, 3) to evaluate the evidence for associations between social support and psychosocial conditions in postpartum period, and 4) to propose a logic framework for improving postpartum social support and psychosocial conditions.
Regarding aim 1, our review found that the social support status of the majority of women in postpartum period was at a moderate to high level. There was a sufficient level of social support, as the majority of evidence came from Asia, where the appropriate level of support for postpartum women is associated with socio-cultural norms. For example, in Saudi culture, it is common for a mother to spend the puerperium period, especially the first forty days, at her mother's house to receive the necessary support until she recovers [37]. However, more research is needed to fully understand mothers’ social support in the postpartum period, as this is crucial in developing strategies to improve maternal health [47].
Concerning aim 2, our review found that the prevalence of PPD (EPDS score ≥ 13) was 22- 29.08%, but there was insufficient evidence to determine the prevalence of other mental disorders. Similar to our findings, the aggregate data meta-analyses (AGMAs) results of the systematic review studies revealed a prevalence of 17.22% to 27% for PPD [21, 48,49,50,51]. PPD is a major mental health issue that impacts about 1 in 8 women, as the transition to motherhood is not always smooth and can be overwhelming [52]. During this transitional period, women encounter numerous challenges including changes in their physical appearance, increased expectations of new responsibilities, physical discomforts from pregnancy and childbirth, and potential marital discord leading to psychosocial issues, particularly PPD [2,3,4]. Furthermore, PPD is a widespread social health concern that not only affects the mother and her newborn, but also has repercussions for other family members and various aspects of their lives [48, 49]. Consequently, there is a need to implement routine postpartum screening for maternal mental health to ensure early detection and treatment of PPD [53].
Regarding aim 3, our systematic review indicated that low social support is a significant predictor of self- reported PPD and anxiety symptoms. Furthermore, our findings demonstrated that social support and postpartum quality of life were mutually dependent. These results are consistent with previous studies, including review or meta-analysis studies with random- effects model, which have identified a lack of social support as a major risk factor for PPD [49,50,51, 54, 55]. Riem et al.’s review study also supports our results, as it found that low social support is associated with self- reported mental disorders symptoms, such as stress and anxiety, during postpartum [7]. Postpartum stress and anxiety are crucial to address as they have been linked to negative health behaviors in women, such as unhealthy diet, smoking relapse, and postpartum weight retention. Additionally, they are key factors associated with PPD, which can develop into self- reported major depression and pose significant risks to morbidity and mortality if left underdiagnosed [56]. It is important to recognize and address these issues in order to support the overall well-being of new mothers [52]. Social support is essential in reducing the risk of postpartum psychosocial problems by providing a protective effect. This includes feeling understood, accepted, and respected, which can help alleviate individual psychological pressure, inhibit negative emotions, and provide positive emotional experiences. Additionally, social support can aid in bonding and coping by improving self-evaluation, helping to form a positive self-image, and promoting self-esteem. Furthermore, social support can act as a buffer against the negative effects of stressors during the postpartum period [52, 56]. As such, providing adequate social and psychological support from family members, providing reassurance, conducting appropriate educational interventions, and regularly assessing the psychological state of women by healthcare providers can help them adapt to postpartum changes, improve their quality of life, and enhance their overall health [57].
Aim 4: A proposed logic framework for improving postpartum social support and psychosocial conditions
Social support was protective against all postpartum psychosocial disorders; therefore, these findings provide a foundation for developing and tailoring interventions and strategies to improve mental health outcomes [58, 59]. The major components of our proposed logic framework are depicted in Fig. 4 and described below.

Proposed logic framework for improving postpartum social support and psychosocial conditions
In the logic framework, stressful events are associated with childbirth and motherhood [1,2,3,4]. Social support is the coping resource in this framework [22]. According to this coping resource, during the coping action stage, researchers and healthcare providers should attempt to improve perceived social support by encouraging and empowering women to be actively involved in adapting to the physical and psychosocial changes occurring, acquiring the necessary knowledge, engaging in help-seeking behavior, and developing novel social roles throughout the postpartum period [18, 60,61,62]. In addition, health policymakers should be aware that flexible education-care-support planning is a promising tool for facilitating more client-centered care during the postpartum care period. In other words, it is crucial to transition from narrow-minded to comprehensive plans that integrate care, education, and support, as well as from uniformity to customization based on individual conditions, resources, and requirements. This shift entails prioritizing clients' personal needs and preferences over organizational constraints, which can help address challenges like escalating healthcare expenses and staffing deficiencies in care facilities. Also, it is consistent with the proposed positive definition of health, which shifts from total well-being to the “ability to adapt and self-manage.” As a result, health professionals encourage patients to participate in their own care processes more than ever before [13, 47].
Finally, the effects of this framework are optimal postpartum mental health and quality of life [58, 59].
The present systematic review is limited by its focus on English-language publications of the included studies. Additionally, a meta-analysis was not conducted due to shortcomings in quantitative indices and varying measuring tools. Nonetheless, this review provides a valuable and broad geographic overview of social support for postpartum psychosocial conditions. The novel contribution of this study is the development of a conceptual framework that offers insights into designing programs for postpartum mental health and quality of life. We recommend using standard protocols for designing, implementing, and evaluating interventions to facilitate comparison in systematic review and meta-analysis studies. Our proposed logic framework can be tested as a guiding framework in intervention design. We also recommend conducting a systematic review that focuses on specific types of action, such as empowerment. Client-tailored and risk-based maternity cares are two important strategies that empower postpartum women [63]. These interventions are designed to address the physical and psychosocial changes that women experience during this time, and they encourage women to actively participate in adapting to these changes [18]. By tailoring care to each individual's needs and addressing potential risks, women can feel more supported and empowered as they navigate the postpartum period.
Conclusions
In conclusion, this systematic review indicates a positive association between social support and postpartum psychosocial conditions. Social support is viewed as a coping mechanism during the postpartum period, which can result in improved quality of life and mental health. This is achieved by empowering women, promoting help-seeking behaviors, and providing client-centered care. As such, the “ability to adapt and self-manage” defines postpartum women’s health.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Olza I, Uvnas-Moberg K, Ekström-Bergström A, Leahy-Warren P, Karlsdottir SI, Nieuwenhuijze M, et al. Birth as a neuro-psycho-social event: An integrative model of maternal experiences and their relation to neurohormonal events during childbirth. PLoS ONE. 2020;15(7):e0230992. https://doi.org/10.1371/journal.pone.0230992.
Bright KS, Charrois EM, Mughal MK, Wajid A, McNeil D, Stuart S, et al. Interpersonal Psychotherapy to Reduce Psychological Distress in Perinatal Women: A Systematic Review. Int J Environ Res Public Health. 2020;17(22):8421. https://doi.org/10.3390/ijerph17228421.
Jackson K, Smart D, Henderson EJ, Newham JJ, McGovern R, Kaner E, et al. Exploring care from extended family through rural women’s accounts of perinatal mental illness - a qualitative study with implications for policy and practice. Health Place. 2020;66:102427. https://doi.org/10.1016/j.healthplace.2020.102427.
Puddister S, Ali-Saleh O, Cohen-Dar M, Baron-Epel O. Health may be compromised by social interactions depending on culture among postpartum Arab and Jewish Israeli women. BMC Pregnancy Childbirth. 2020;20(1):480. https://doi.org/10.1186/s12884-020-03168-4.
Eiroa-Orosa FJ. Understanding Psychosocial Wellbeing in the Context of Complex and Multidimensional Problems. Int J Environ Res Public Health. 2020;17(16):5937. https://doi.org/10.3390/ijerph17165937.
Asselmann E, Kunas SL, Wittchen HU, Martini J. Maternal personality, social support, and changes in depressive, anxiety, and stress symptoms during pregnancy and after delivery: A prospective-longitudinal study. PLoS ONE. 2020;15(8):e0237609. https://doi.org/10.1371/journal.pone.0237609.
Riem MME, Bakermans-Kranenburg MJ, Cima M, van IJzendoorn MH. Grandparental Support and Maternal Postpartum Mental Health: A Review and Meta-Analysis. Hum Nat. 2023;34(1):25–45. https://doi.org/10.1007/s12110-023-09440-8.
Liu Y, Zhang L, Guo N, Jiang H. Postpartum depression and postpartum post-traumatic stress disorder: prevalence and associated factors. BMC Psychiatry. 2021;21(1):487. https://doi.org/10.1186/s12888-021-03432-7.
Dekel S, Stuebe C, Dishy G. Childbirth Induced Posttraumatic Stress Syndrome: A Systematic Review of Prevalence and Risk Factors. Front Psychol. 2017;8:560. https://doi.org/10.3389/fpsyg.2017.00560.
Schobinger E, Vanetti M, Ramelet AS, Horsch A. Social support needs of first-time parents in the early-postpartum period: A qualitative study. Front Psychiatry. 2022;13:1043990. https://doi.org/10.3389/fpsyt.2022.1043990.
Asadi M, Noroozi M, Alavi M. Factors Affecting Women’s Adjustment to Postpartum Changes: A Narrative Review. Iran J Nurs Midwifery Res. 2020;25(6):463–70. https://doi.org/10.4103/ijnmr.IJNMR_54_20.
McLeish J, Redshaw M. “Being the best person that they can be and the best mum”: a qualitative study of community volunteer doula support for disadvantaged mothers before and after birth in England. BMC Pregnancy Childbirth. 2019;19(1):21. https://doi.org/10.1186/s12884-018-2170-x.
Lambermon FJ, van Duijnhoven NTL, Kremer JAM, Dedding CWM. Mothers’ experiences of client-centred flexible planning in home-based postpartum care: A promising tool to meet their diverse and dynamic needs. Midwifery. 2021;102:103068. https://doi.org/10.1016/j.midw.2021.103068.
Benoit B, Aston M, Price S, Iduye D, Sim SM, Ollivier R, et al. Mothers’ Access to Social and Health Care Systems Support during Their Infants’ First Year during the COVID-19 Pandemic: A Qualitative Feminist Poststructural Study. Nurs Rep. 2023;13(1):412–23. https://doi.org/10.3390/nursrep13010038.
Gayesa RT, Ngai FW, Xie YJ. The effects of mHealth interventions on improving institutional delivery and uptake of postnatal care services in low-and lower-middle-income countries: a systematic review and meta-analysis. BMC Health Serv Res. 2023;23(1):611. https://doi.org/10.1186/s12913-023-09581-7.
Symonds NE, Vidler M, Wiens MO, Omar S, English LL, Ukah UV, et al. Risk factors for postpartum maternal mortality and hospital readmission in low- and middle-income countries: a systematic review. BMC Pregnancy Childbirth. 2023;23(1):303. https://doi.org/10.1186/s12884-023-05459-y.
Jones E, Stewart F, Taylor B, Davis PG, Brown SJ. Early postnatal discharge from hospital for healthy mothers and term infants. Cochrane Database Syst Rev. 2021;6(6):CD002958. https://doi.org/10.1002/14651858.CD002958.pub2.
Duvivier H, Decroo T, Nelson A, Cassidy T, Mbakaz Z, Duran LT, et al. Knowledge transmission, peer support, behaviour change and satisfaction in post Natal clubs in Khayelitsha, South Africa: a qualitative study. Reprod Health. 2020;17(1):107. https://doi.org/10.1186/s12978-020-00957-0.
Hampanda KM, Mweemba O, Ahmed Y, Hatcher A, Turan JM, Darbes L, et al. Support or control? Qualitative interviews with Zambian women on male partner involvement in HIV care during and after pregnancy. PLoS ONE. 2020;15(8):e0238097. https://doi.org/10.1371/journal.pone.0238097.
McLeish J, Harvey M, Redshaw M, Alderdice F. A qualitative study of first time mothers’ experiences of postnatal social support from health professionals in England. Women Birth. 2021;34(5):e451–60. https://doi.org/10.1016/j.wombi.2020.10.012.
Dadi AF, Akalu TY, Baraki AG, Wolde HF. Epidemiology of postnatal depression and its associated factors in Africa: A systematic review and meta-analysis. PLoS ONE. 2020;15(4):e0231940. https://doi.org/10.1371/journal.pone.0231940.
Gholizadeh Shamasbi S, Barkin JL, Ghanbari-Homayi S, Eyvazzadeh O, Mirghafourvand M. The Relationship between Maternal Functioning and Mental Health after Childbirth in Iranian Women. Int J Environ Res Public Health. 2020;17(5):1558. https://doi.org/10.3390/ijerph17051558.
Buchwald P. Social support. Curated ref collect Neurosci Biobehav Psychol. 2017;435–41. https://doi.org/10.1016/B978-0-12-809324-5.05719-9.
Dadi AF, Miller ER, Mwanri L. Postnatal depression and its association with adverse infant health outcomes in low- and middle-income countries: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2020;20(1):416. https://doi.org/10.1186/s12884-020-03092-7.
De Sousa MT, Chur-Hansen A, Due C. First-time mothers’ perceptions of social support: Recommendations for best practice. Health Psychol Open. 2020;7(1):2055102919898611. https://doi.org/10.1177/2055102919898611.
Schwarzer C, Buchwald P. Social Support, Encycl. Appl Psychol. 2004;3:435–41. https://doi.org/10.1016/B0-12-657410-3/00414-1.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71.
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med.2009;6(7): e1000097. https://doi.org/10.1371/journal.pmed.1000097.
Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. https://doi.org/10.1136/bmj.j4008.
Pieper D, Antoine SL, Neugebauer EA, Eikermann M. Up-to-dateness of reviews is often neglected in overviews: a systematic review. J Clin Epidemiol. 2014;67(12):1302–8. https://doi.org/10.1016/j.jclinepi.2014.08.008.
Howick J, Chalmers I, Glasziou P, Greenhalgh T, Heneghan C, Liberati A, et al. “Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence (Background Document)”. Oxford Centre for Evidence-Based Medicine. https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence.
Dehkordi AH, Mazaheri E, Ibrahim HA, Dalvand S, Ghanei GR. How to Write a Systematic Review: A Narrative Review. Int J Prev Med. 2021;12:27. https://doi.org/10.4103/ijpvm.IJPVM_60_20.
he EndNote Team. EndNote X7 (Version 64 bit) [Computer software]. 2013. Philadelphia, PA: Clarivate. https://endnote.com/downloads.
Modesti PA, Reboldi G, Cappuccio FP. Newcastle-Ottawa Quality Assessment Scale (adapted for cross sectional studies). PLoS One. 2016;11(1):e0147601. https://scholar.google.com/scholar?hl=en&as_sdt=0%2C5&q=Modesti%2C+P.%2C+G.+Reboldi%2C+and+F.+Cappuccio%2C+Newcastle-Ottawa+Quality+Assessment+Scale+%28adapted+for+cross+sectional+studies%29.+PLoS+One%2C+2016.+11%281%29%3A+p.+e0147601.&btnG=.
Motamed-Jahromi M, Kaveh MH. Effective Interventions on Improving Elderly’s Independence in Activity of Daily Living: A Systematic Review and Logic Model. Front Public Health. 2021;8:516151. https://doi.org/10.3389/fpubh.2020.516151.
Tacconelli E. Systematic reviews: CRD’s guidance for undertaking reviews in health care. Lancet Infect Dis. 2010;10(4):226. https://doi.org/10.1016/S1473-3099(10)70065-7.
Al Rehaili BO, Al-Raddadi R, ALEnezi NK, ALYami AH. Postpartum quality of life and associated factors: a cross-sectional study. Qual Life Res. 2023;32(7):2099–106. https://doi.org/10.1007/s11136-023-03384-3.
Jamshaid S, Malik NI, Ullah I, Saboor S, Arain F, De Berardis D. Postpartum Depression and Health: Role of Perceived Social Support among Pakistani Women. Diseases. 2023;11(2):53. https://doi.org/10.3390/diseases11020053.
Khademi K, Kaveh MH, Ghahremani L, Nazari M, Karimi M. The impact of family social support on postpartum quality of life among Iranian women: structural equation modelling. J Int Med Res. 2023;51(2):3000605221147198. https://doi.org/10.1177/03000605221147198.
Wedajo LF, Alemu SS, Jarso MH, Golge AM, Dirirsa DE. Late postpartum depression and associated factors: community-based cross-sectional study. BMC Womens Health. 2023;23(1):280. https://doi.org/10.1186/s12905-023-02444-7.
Qi W, Liu Y, Lv H, Ge J, Meng Y, Zhao N, et al. Effects of family relationship and social support on the mental health of Chinese postpartum women. BMC Pregnancy Childbirth. 2022;22(1):65. https://doi.org/10.1186/s12884-022-04392-w.
Xayyabouapha A, Sychareun V, Quyen BTT, Thikeo M, Durham J. Prevalence and Risk Factors Associated With Postpartum Depressive Symptoms Among Women in Vientiane Capital. Lao PDR Front Public Health. 2022;10:791385. https://doi.org/10.3389/fpubh.2022.791385.
Basu S, Budh N, Garg S, Singh MM, Sharma A. Postpartum depression burden and associated factors in mothers of infants at an urban primary health center in Delhi. India Tzu Chi Med J. 2019;33(1):70–3. https://doi.org/10.4103/tcmj.tcmj_190_19.
Akbari V, Rahmatinejad P, Shater MM, Vahedian M, Khalajinia Z. Investigation of the relationship of perceived social support and spiritual well-being with postpartum depression. J Educ Health Promot. 2020;9:174. https://doi.org/10.4103/jehp.jehp_56_20.
Feligreras-Alcalá D, Frías-Osuna A, Del-Pino-Casado R. Personal and Family Resources Related to Depressive and Anxiety Symptoms in Women during Puerperium. Int J Environ Res Public Health. 2020;17(14):5230. https://doi.org/10.3390/ijerph17145230.
Shitu S, Geda B, Dheresa M. Postpartum depression and associated factors among mothers who gave birth in the last twelve months in Ankesha district, Awi zone, North West Ethiopia. BMC Pregnancy Childbirth. 2019;19(1):435. https://doi.org/10.1186/s12884-019-2594-y.
Sharifipour F, Javadnoori M, Moghadam ZB, Najafian M, Cheraghian B, Abbaspoor Z. Primiparous Mothers’ Perception and Expectations Regarding Social Support during the Postpartum Period: A Qualitative Study. Iran J Nurs Midwifery Res. 2023;28(1):38–46. https://doi.org/10.4103/ijnmr.ijnmr_383_21.
Alshikh Ahmad H, Alkhatib A, Luo J. Prevalence and risk factors of postpartum depression in the Middle East: a systematic review and meta-analysis. BMC Pregnancy Childbirth. 2021;21(1):542. https://doi.org/10.1186/s12884-021-04016-9.
Zeleke TA, Getinet W, Tadesse Tessema Z, Gebeyehu K. Prevalence and associated factors of post-partum depression in Ethiopia. A systematic review and meta-analysis. PLoS One. 2021;16(2): e0247005. https://doi.org/10.1371/journal.pone.0247005.
Ekpenyong MS, Munshitha M. The impact of social support on postpartum depression in Asia: A systematic literature review. Ment Health Prev. 2023;30:200262. https://doi.org/10.1016/j.mhp.2023.200262.
Duko B, Wolde D, Alemayehu Y. The epidemiology of postnatal depression in Ethiopia: a systematic review and meta-analysis. Reprod Health. 2020;17(1):180. https://doi.org/10.1186/s12978-020-01035-1.
Alshowkan A, Shdaifat E, Alnass FA, Alqahtani FM, AlOtaibi NG, AlSaleh NS. Coping strategies in postpartum women: exploring the influence of demographic and maternity factors. BMC Womens Health. 2023;23(1):582. https://doi.org/10.1186/s12905-023-02751-z.
Dlamini LP, Mahanya S, Dlamini SD, Shongwe MC. Prevalence and factors associated with postpartum depression at a primary healthcare facility in Eswatini. S Afr J Psychiatr. 2019;25:1404. https://doi.org/10.4102/sajpsychiatry.v25i0.1404.
Agrawal I, Mehendale AM, Malhotra R. Risk Factors of Postpartum Depression. Cureus. 2022;14(10):e30898. https://doi.org/10.7759/cureus.30898.
Nweke M, Ukwuoma M, Adiuku-Brown AC, Ugwu P, Nseka E. Characterization and stratification of the correlates of postpartum depression in sub-Saharan Africa: A systematic review with meta-analysis. Womens Health (Lond). 2022;18:17455057221118772. https://doi.org/10.1177/17455057221118773.
Walker LO, Murry N. Maternal Stressors and Coping Strategies During the Extended Postpartum Period: A Retrospective Analysis with Contemporary Implications. Womens Health Rep. 2022;3(1):104–14. https://doi.org/10.1089/whr.2021.0134.
Asadi M, Noroozi M, Alavi M. Exploring the experiences related to postpartum changes: perspectives of mothers and healthcare providers in Iran. BMC Pregnancy Childbirth. 2021;21(1):7. https://doi.org/10.1186/s12884-020-03504-8.
Mauri D. «Becoming parents as mending the past»: care-experienced parents and the relationship with their birth family. Child Youth Serv Rev. 2023;148:106911. https://doi.org/10.1016/j.childyouth.2023.106911.
Bhushan NL, Stockton MA, Harrington BJ, DiPrete BL, Maliwichi M, Jumbe AN, et al. Probable perinatal depression and social support among women enrolled in Malawi’s Option B+ Program: A longitudinal analysis. J Affect Disord. 2022;306:200–7. https://doi.org/10.1016/j.jad.2022.03.017.
Amaro JS, Pessalli MRTFB, da Cunha LB, Betrán AP, Torloni MR, Siaulys MM. The Godmother Project: A Virtual Initiative to Support Pregnant and Postpartum Women in Brazil During the COVID-19 Pandemic. Glob Health Sci Pract. 2023;11(2): e2200500. https://doi.org/10.9745/GHSP-D-22-00500.
Itai M, Harada S, Nakazato R, Sakurai S. Transition to Motherhood of Mothers Receiving Continuity of Child-Rearing Support. Int J Environ Res Public Health. 2022;19(14):8440. https://doi.org/10.3390/ijerph19148440.
Doyle FL, Klein L. Postnatal Depression Risk Factors: An Overview of Reviews to Inform COVID-19 Research, Clinical, and Policy Priorities. Front Glob Womens Health. 2020;1:577273. https://doi.org/10.3389/fgwh.2020.577273.
Lagendijk J, Been JV, Ernst-Smelt HE, Bonsel GJ, Bertens LCM, Steegers EAP. Client-tailored maternity care to increase maternal empowerment: cluster randomized controlled trial protocol; the healthy pregnancy 4 All-2 program. BMC Pregnancy Childbirth. 2019;19(1):4. https://doi.org/10.1186/s12884-018-2155-9.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
KH. KH analyzed the data and wrote manuscript; MH. K reviewed the manuscript. The authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Khademi, K., Kaveh, M.H. Social support as a coping resource for psychosocial conditions in postpartum period: a systematic review and logic framework. BMC Psychol 12, 301 (2024). https://doi.org/10.1186/s40359-024-01814-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-024-01814-6