
Abstract
Background
Social support is a well-known protective factor against depressive symptoms and substance use problems, but very few studies have examined its protective effects among residents of permanent supportive housing (PSH), a housing program for people with a history of chronic homelessness. We utilized unconditional latent growth curve models (LGCMs) and parallel process growth models to describe univariate trajectories of social support, depressive symptoms, and substance use problems and to examine their longitudinal associations in a large sample of adults residing in PSH.
Methods
Participants were 653 adult PSH residents in North Texas (56% female; 57% Black; mean age: 51 years) who participated in a monthly health coaching program from 2014 to 2017. Their health behaviors were assessed at baseline and tracked every six months at three follow-up visits.
Results
Unconditional LGCMs indicated that over time, social support increased, whereas depressive symptoms and substance use problems decreased. However, their rates of change slowed over time. Further, in parallel process growth models, we found that at baseline, individuals with greater social support tended to have less severe depressive symptoms and substance use problems (coefficients: − 0.67, p < 0.01; − 0.52, p < 0.01, respectively). Individuals with a faster increase in social support tended to have steeper rates of reduction in both depressive symptoms (coefficient: − 0.99, p < 0.01) and substance use problems (coefficient: − 0.98, p < 0.01), respectively.
Conclusions
This study suggests that plausibly, increases in social support, though slowing over time, still positively impact depressive symptoms and substance use problems among PSH residents. Future PSH programs could emphasize social support as an early component as it may contribute to clients’ overall health.
Similar content being viewed by others


Introduction
People who are homeless are at higher risk for health problems, such as malnutrition, stress, communicable diseases, and violence [1]. The elevated health risks among people who are homeless contribute to significantly higher mortality rates, shorter life expectancy, and more frequent hospitalizations and acute care services utilization, compared with people in the general population [2,3,4]. In particular, depression is approximately three times more prevalent among adults who are homeless (20–25%), compared with 8.1% among the general adult population of the United States (US) [2, 5]. Moreover, over a third of homeless individuals experience alcohol and drug problems, rates that are far greater than those seen among individuals with supportive housing [6]. Some evidence suggests that social support is negatively associated with both depressive symptoms and substance use problems among people who are homeless [7,8,9,10,11,12]. For example, in a sample of homeless women residing in a temporary shelter, marijuana use and drinking to intoxication were both predicted by lower social support [8]. Likewise, social support appears to be an important mediator of the effects of stress on depressive symptoms among people with limited resources [12]. Permanent supportive housing (PSH), which combines a housing voucher with supportive services, has been recognized as an effective model for stabilizing the mental and physical needs of homeless adults [1, 13]. Hence, the number of PSH beds in the US has increased by 380% or 144,000 more from 2007 to 2019 [14]. Despite this progress, a crucial knowledge gap remains: little empirical evidence exists to guide program decisions after homeless adults enter PSH. In particular, few studies have examined the longitudinal associations of social support with either depressive symptoms or substance use problems among PSH residents with a history of homelessness.
Permanent supportive housing and social support
Though PSH residents are affected by many of the same issues that homeless individuals experience, PSH may provide the opportunity to begin new and steady social relationships and to gain support through newly formed connections [15]. For many people, it is a life-changing event. By providing stable housing and supportive case management services, PSH can be instrumental in breaking the negative reciprocal cycle that often exists between unstable housing, mental health, and substance use problems [16,17,18,19]. However, at the same time, PSH may also introduce new challenges to people who were once homeless [20, 21]. For example, some PSH residents experience social isolation after being housed in unfamiliar locations, while others feel stigmatized in environments without access to former peers [21]. However, very little longitudinal information on social support exists among the PSH residents. It remains an empirical question whether perceived social support increases in this population over time and whether changes in social support are related to health outcomes.
Social support and depressive symptoms
In general, research suggests that depressive symptoms are negatively related to social support among people with current or past homelessness [22,23,24]. For instance, in two samples of homeless adults in a large metropolitan area, perceived social support buffered the effects of psychological stress [23]. In another sample of people residing in PSH, increases in social support over six months were associated with decreased depressive symptoms. However, most of the available evidence is either cross-sectional [23, 24] or focuses on temporally concurrent associations without examining the individual variability in underlying growth curves [22]. A growth perspective over time, as well as its limits or individual differences in the growth, may provide more helpful information for the purpose of improving care services. Given the heterogeneity in the course of adaptation and outlook for PSH residents, it may be important to study how changes in social support over time are associated with trajectories of depressive symptoms, while simultaneously estimating individual trajectories to assess their boundaries of promotive effects of one behavior over the other.
Social support and substance use problems
Similarly, there is a dearth of information on the longitudinal relationship between social support and substance use problems among PSH population. A randomized trial of a “Housing First” PSH program on substance use problems among homeless individuals in Canada found an inconsistent effect of the housing intervention (vs. the treatment as usual group) on substance use problems [25]. Compared to the usual-care group, the treatment group experienced fewer substance-related problems after 12 months, but not after 24 months. Moreover, some substance use problems (e.g., relationship problems) decreased, while other problems (e.g., physiological tolerance) did not decrease over the 2 years following their housing placement [25]. In fact, findings from a few available studies suggest that substance use problems may continue even after housing has been provided [26, 27], and that more specific efforts to address stress and social support may be needed to help reduce substance use problems, especially if residents use substances to cope with stress [26]. The scant research on this population suggests that there are important knowledge gaps that need to be addressed—that is, whether substance use problems tend to decrease over time and whether a concurrent increase in social support plays a protective role.
Measurement limitations of prior research
The existing research on PSH residents has often encountered measurement limitations. Many of the measures used in previous studies were adapted from scales developed for other purposes without empirical validation for applications to this specific population. For example, the measure of social support used by Durbin et al. [26] consisted of subscales from three different instruments designed for community residents with chronic mental illness, hospitalized patients with chronic psychiatric disorders, and the general US population [28,29,30]. A similar approach was employed in Kirst et al. [25], where they measured the substance use problems with items from one subscale of the Global Appraisal of Individual Needs Short Screener (GAIN-SS) [31], a screening tool designed for general populations. A recent psychometric study showed that this subscale might not be suited for people at low and high levels of severity [32].
The current study addresses these measurement weaknesses and provides a more rigorous test of the longitudinal relationships of social support, depressive symptoms, and substance use problems. We adapted the existing measures of social support and substance use problems for the PSH population: the Interpersonal Support Evaluation List (ISEL) [33, 34] and the Inventory of Drug Use Consequences (InDUC) [35]. To our knowledge, ISEL and InDUC have never been used or tested specifically in this population. Therefore, we modified the scales for this population and tested their psychometric properties in a series of confirmatory factor analyses (see Methods and Table 1). Using a latent variable modeling approach, we simultaneously tested measurement models for these three constructs over time and examined their parallel trajectories. Additionally, by simultaneously tackling measurement models and growth models in one analysis, we more efficiently use all available data and gain precision in estimation, while accounting for measurement errors, testing measurement invariance over time, and addressing missing data. We further included age, sex, race, and length of stay in the current neighborhood, as covariates to examine whether the initial levels of social support, depressive symptoms and substance use problems are explained by these covariates.
We hypothesized that in the context of monthly health coaching, perceived social support would increase over time, whereas both depressive symptoms and substance use problems would decrease over time. We further hypothesized that individuals with lower levels of perceived social support at baseline would have higher levels of depressive symptoms and substance use problems at baseline and show slower rates of growth in social support over time, which would, in turn, predict slower rates of decline in depressive symptoms and substance use problems.
Methods
Mobile community health assistance for tenants
The current study used data from a health coaching program called “Mobile Community Health Assistance for Tenants” (m.chat). This program provided in-person health coaching to PSH residents as part of the Regional Healthcare Partnership (RHP 10) Medicaid Waiver program in the state of Texas (see more details of the m.chat program in [36]). In addition to the usual housing and case management services offered by the PSH programs, m.chat provided additional in-person health coaching to encourage PSH residents to adopt healthy behaviors, such as improved diet, exercise, recreation activities, or reducing substance use. The program consisted of monthly visits with a health coach who was trained in motivational interviewing and brief solution-focused therapy, a coaching software that provided feedback on health status, and access to wellness incentives (up to $60 in USD per month) that could be used to purchase health-related supplies. Health coaches began visits by eliciting areas of health concern and motivation for making changes. Clients discussed long-term health goals and developed short-term action items (using “SMART” goal planning). Coaches used the computer interface to set text reminders for clients who wanted to receive them and provided an overall summary of the visit. Follow-up visits included a review of recent progress (at the beginning) and discussion of how to use wellness incentives to achieve health goals (near the end). Coaching visits mostly took place in public locations, such as recreation centers, fast food restaurants, or the project office. Typically, participants completed one coaching visit per month for up to 18 months, and each visit lasted 52 min on average.
Participants
Participants were 653 PSH residents (56% female; 57% Black; mean age: 51 years with a range of 20–80) recruited from six local housing agencies in Fort Worth, TX, from 2014 to 2017. Table 2 describes the sample and measures. In this sample of 653 people, 70% (n = 455) participated in the first follow-up (6 months after baseline), 46% (n = 299) in the second follow-up (12 months after baseline), and 38% (n = 249) in the third follow-up (18 months after baseline). All m.chat participants were Medicaid enrolled or low income uninsured, and self-reported one of the following mental health conditions in the past year: prescribed medication for psychological or emotional problems, experienced hallucinations, received a pension for a psychiatric disability, or scored greater than nine on a depressive symptoms screener, the Patient Health Questionnaire-9 (PHQ-9) [37]. Exclusion criteria included: (1) residing in other types of housing not considered PSH (e.g., Transitional Housing or homeless shelter), (2) any physical or sensory impairment that would substantially limit program participation, (3) non-English-speaking, or (4) limited autonomy or decision-making capabilities (e.g., substantially neurologically or cognitively impaired). This project was approved by the North Texas Regional Institutional Review Board.
Measures
Social support
Social support was assessed with a modified version of the Interpersonal Support Evaluation List (ISEL) [33, 34]. The original ISEL measures perceived social support across four domains, each consisting of 10 items: (1) appraisal support, which is the perceived availability of other people to offer advice, guidance, and information, (2) tangible support, which includes aid or instrumental support, (3) self-esteem maintenance, which is the perceived availability of positive comparison to others, and (4) belonging support, which is the perceived availability of others for companionship [33, 34]. To simplify the language and make the examples more relevant to PSH residents, the ISEL was modified by removing the self-esteem maintenance domain, reducing the number of items in each domain from ten to three (nine items in total), and changing the scoring rubric. A series of statements about different aspects of social support (e.g., “When I feel lonely, I have people I can talk to,” “I could easily find someone to loan me $10 if I needed it”) were self-rated on a 5-point scale from “Hardly ever” to “Almost always” (Table 1). Cronbach’s alpha for the current sample was 0.87.
Depressive symptoms
Depressive symptoms were assessed with the Patient Health Questionnaire-9 (PHQ-9) [37]. The nine items on the PHQ-9 correspond to the nine criteria for major depressive disorder based on the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) [38]. The items ask how frequently the individual has experienced each symptom during the last two weeks and assigns a score of 0, 1, 2, and 3 for not at all, several days, more than half of the days, and nearly every day, respectively. Items are summed for a total PHQ-9 score, which can be categorized as follows: mild if the resulting sum score ranges from 5 to 9, moderate for 10 to 14, moderately severe for 15 to 19, and severe for 20 to 27 [37]. Cronbach’s alpha for the current sample was 0.81.
Substance use problems
Substance use problems were assessed with a modified version of the Inventory of Drug Use Consequences (InDUC) [35]. The original version of the InDUC includes 50 items that evaluate both lifetime and recent (past three months) substance use problems from five domains: Physical, Interpersonal, Intrapersonal, Impulse Control, and Social Responsibility. In this study, the InDUC was modified by reducing the number of questions in each dimension from five to three and by asking participants only about recent (past three months) problems. Response options were: 0 = Never, 1 = Once or few times, 2 = Once or twice a week, and 3 = Daily or almost daily (see also Table 1). Cronbach’s alpha for the current sample was 0.96.
Data analyses
We first conducted a confirmatory factor analysis to examine the structure and performance of social support, substance use problems, and depressive symptoms at each time point. We then used latent growth curve models (LGCM) to estimate changes in social support, depressive symptoms, and substance use problems at baseline, 6-month, 12-month, and 18-month post-baseline [39]. We tested several longitudinal measurement invariance models following recommendations and steps from Muthén and Christoffersson [40], Meredith [41], and Widaman and Reise [42] to ensure that item measures and latent traits are comparable across time. We started with the least restrictive measurement model (configural invariance) and moved to test stricter invariance models [41] by increasingly constraining parameters (factor loadings, intercepts, and residual variances) across time. We used the chi-square test of model fit to determine whether adding constraints to the model resulted in a poor fit. We selected the strictest invariance model with an acceptable fit.
We used the maximum likelihood estimator in the LGCM for social support and depressive symptoms and the robust maximum likelihood (MLR) estimator for the LGCM of substance use problems. The scaled difference chi-square test statistic [43] was calculated accordingly for models using MLR. We subsequently modeled the parallel trajectories [44, 45] of social support and depressive symptoms, and the parallel trajectories of social support and substance use problems in two separate, bivariate longitudinal analyses [46] to examine the relationships of the parameters from one trajectory with those from the other trajectory [47].
We estimated the parameters using all available information under the full information maximum likelihood (FIML) method for missing data [48]. The adequacy of model fit was examined using several absolute and relative fit indices, including the chi-square degrees of freedom ratio (χ2/df), the root mean squared error approximation (RMSEA) [49, 50], and the comparative fit index (CFI) [51]. Chi-square to df ratios less than 3; RMSEA scores less than 0.08; and CFI scores greater than 0.90 are generally considered acceptable [52,53,54,55,56]. All data preparation was conducted using SAS 9.4 (SAS Institute Inc., Cary, NC), and all factor analyses and latent growth curve modeling were conducted using Mplus 8.4 [57]. Figures 2 and 3 and all additional file figures were drawn using Microsoft PowerPoint.
Results
Measurement models: confirmatory factor analysis
Before fitting univariate growth curve models, we separately fitted measurement models for social support, depressive symptoms, and substance use problems at baseline and follow-ups (6-month, 12-month, and 18-month post-baseline). Table 2 provides a descriptive summary of the three health behaviors at the four assessment time points. All measurement models were fitted following the structure of the measurement tool for that health behavior (a 2nd-order, three-factor model for social support, a single-factor model for depressive symptoms, and a 2nd order, five-factor model for substance use problems; see Additional file 1: Figs. S1–S12). Note that we allowed residual item variances to covary (see detail in Additional file 1: Figs. S1–S12, and measurement model fit indices for the three health behaviors across four waves in Additional file 1: Table S1). We kept these residual covariances in the subsequent univariate growth curve models. Overall, the model fit was adequate for all three behaviors, and all factor loadings were statistically significant, supporting the validity of the measurement models (full results available upon request).
Univariate unconditional latent growth curve analysis
We tested up to the 2nd polynomial term in all growth curve models. Based on our prior experience, we anticipated that participants would have non-zero values at baseline that significantly vary across individuals. We further expected that all three behaviors could be modeled by a linear growth term and a quadratic growth term to capture their change over time. Table 3 presents the model fit information and the growth parameters of the univariate unconditional latent growth curve models of all three health behaviors. All three models fit the data adequately.
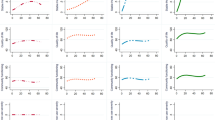
The intercept represents the average baseline level, the linear growth term quantifies the linear rate of change, and the quadratic term quantifies the rate of change in the linear growth rate over time. Social support significantly linearly increased (0.34) over time, with the rate of increase in social support slowing (− 0.09) over time (Fig. 1). For depressive symptoms, the negative linear growth term for depressive symptoms indicates that they significantly decreased (− 0.51) over time; however, the positive and statistically significant quadratic term indicates that reductions in depressive symptoms slowed (0.12) over time. For substance use problems, the negative linear growth term shows that they significantly decreased (− 0.08) over time, while the positive and statistically significant quadratic term indicates that the rate of reductions in substance use problems slowed (0.02) over time. We constrained the variances of quadratic growth terms to zero, specifying that any individual differences for the quadratic terms are trivial, which is a common observation in growth analysis [57]. Hence, there was no covariation between the quadratic terms and other growth parameters.

Estimated individual and average growth trajectories of social support (top), depressive symptoms (middle), and substance use problems (bottom) for a randomly selected 25% sample. Y-axis values indicate the average item score of each measure. Social Support: 1 = hardly ever to 5 = almost always. Depressive symptoms: 0 = not at all, 1 = several days, 2 = more than half of the days, and 3 = nearly every day. Substance Use Problems: 0 = never, 1 = once or few times, 2 = once or twice a week, and 3 = daily or almost daily
In testing measurement invariance across time points, the LGCMs of both social support and substance use problems held the strong factorial invariance in which invariance constraints were placed on the configural patterns, the factor loadings, and the intercepts of the measured item variables. The LGCM of depressive symptoms held the configural invariance, in which the pattern of fixed and free factor loadings of measured variables remained the same across time points.
Parallel-process growth models
The associations between the growth parameter terms for social support and depressive symptoms, and for social support and substance use problems were simultaneously assessed in two separate parallel-process growth models (Fig. 2). By setting the variance of the intercept and slope term to one, we directly estimated the correlation coefficients among them. The intercept-to-intercept, slope-to-slope, and intercept-to-slope correlation coefficients are presented in Table 4. The initial status of social support was negatively related to the initial status of both depressive symptoms and substance use problems. The intercept-to-slope associations within the same behavior domain showed the same patterns as those reported in the previous section on univariate unconditional latent growth curve analysis. Cross-domain correlations in the intercept and slope were statistically significant and large in magnitude. Higher levels of social support at baseline were related to lower levels of depressive symptoms (− 0.67) and substance use problems (− 0.52) at baseline. After controlling for the baseline differences and within-domain associations, the rates at which social support grew almost perfectly correlated with the rates at which depressive symptoms (− 0.99) and substance use problems (− 0.98) decreased.

The unconditional parallel process growth curve models, examining the trajectories of social support and depressive symptoms (top), and social support and substance use problems (bottom). αss: Intercept for social support; βss1: Linear slope for social support; βss2: Quadratic slope for social support; αdep: Intercept for depressive symptoms; βdep1: Linear slope for depressive symptoms; βdep2: Quadratic slope for depressive symptoms; αsu: Intercept for substance use problems; βsu1: Linear slope for substance use problems; βsu2: Quadratic slope for substance use problems. ss@0-ss@18, dep@0-dep@18, and su@0-su@18 represent data over four observations for social support, depressive symptoms, and substance use problems. The residual variances (error variances) are not shown for better readability. *p < 0.05; **p < 0.01
We added covariates, including age, sex, race, and length of stay in the current neighborhood, to examine whether the initial levels of depressive symptoms and substance use problems are explained by these covariates (see Fig. 3). Among all the covariates, women, compared to men, presented a significantly higher intercept level of social support in both models and a significantly lower intercept level of substance use problems. However, compared to the unconditional models, key growth parameters in the conditional models remained the same with a few negligible changes.

The conditional parallel process growth curve models, with the latent intercepts of social support and depressive symptoms (top), and social support and substance use problems (bottom) regressed on age, race, sex, and length of stay in the current neighborhood. αss: Intercept for social support; βss1: Linear slope for social support; βss2: Quadratic slope for social support; αdep: Intercept for depressive symptoms; βdep1: Linear slope for depressive symptoms; βdep2: Quadratic slope for depressive symptoms; αsu: Intercept for substance use problems; βsu1: Linear slope for substance use problems; βsu2: Quadratic slope for substance use problems. ss@0-ss@18, dep@0-dep@18, and su@0-su@18 represent data over four observations for social support, depressive symptoms, and substance use problems. The residual variances (error variances) are not shown for better readability. *p < 0.05; **p < 0.01
Discussion
The current study examined the trajectories of social support, depressive symptoms, and substance use problems in a sample of adult PSH residents over 18 months after entering a health coaching program. Over 18 months, significant improvements were observed in all three health behaviors. Specifically, perceived social support increased, whereas depressive symptoms and substance use problems decreased over time, although the rate of positive changes slowed over time. This is an encouraging finding, given that PSH residents have a greater need for physical and mental health services when providing adequate professional care could be costly [4]. With monthly brief health coaching lasting for about an hour or less, residents’ social support increased along with concurrent reductions in depressive symptoms and substance problems. Health coaching may be a relatively inexpensive and feasible way to promote healthy behavior change among PSH residents who are motivated to change their health behaviors.
More specifically, the findings highlight a sizable variability in perceived social support at baseline, with higher perceived social support associated with less severe depressive symptoms and lower levels of substance use problems. The baseline associations suggest that it may be important for PSH case managers to consider the degree of social support received by their clients. As shown in this study, baseline social support was significantly correlated with the indicators of mental health and substance use problems. This may help case managers to develop need-based customized case management plans.
Furthermore, we found that the PSH residents with low social support at baseline showed increasing social support over time. The data show their rate of growth in social support was faster than those with higher levels of social support at baseline. In addition, PSH residents showed steeper rates of reduction in depressive symptoms and substance use problems when their social support increased at faster rates, as we observed a negative association between the slopes of the trajectory of social support and depressive symptoms and the trajectory of social support and substance use problems. The strong cross-domain correlations in the linear slopes suggests that the benefit of improving social support among PSH residents may provide non-disorder-specific overall support for behavior change and improved psychological well-being.
To the best of our knowledge, this is the first study to examine the association between rates of social support and depressive symptoms, as well as between social support and substance use problems in a PSH sample using parallel-process growth models. Evidence from this study provides a strong rationale for improving social support for PSH residents with mental health and substance use problems. Because m.chat was not an experimental study, it is difficult to determine if positive changes were due to health coaching, other PSH supportive services, or natural changes over time. Nevertheless, the current study suggests that coaching and increased social support can help initiate positive changes in other areas of health.
We also note that this is the most extensive longitudinal study of PSH residents participating in a health coaching program. The results suggest several important implications for the future design of supportive housing programs. First, programs should include regular follow-ups to assess the status of related health behaviors among residents. Since improvements in social support and depressive symptoms may not be consistent over time, frequent regular assessment follow-ups may help case managers identify any emerging challenges or difficulties and offer corresponding services. Follow-up intervals may need to be even shorter than every six months, which we had in this study, to more accurately pinpoint the timing of an inflection where growth slows and consequently plan for an additional coaching session or short booster sessions, delivered briefly over phone calls or text messages, to empower their agency in health-promotive behaviors and further reinforce newly adopted healthy behaviors. Second, future programs could emphasize social support as an early component as it may bring a favorable prognosis on mental health and substance use outcomes. The findings from the current study further emphasize the importance of understanding the status and needs of social support among PSH residents, as stated in the classic work of Cohen and Wills [58]. The need for social support may be different based on the specific difficulties or stressors that people try to cope with [58]. Thus, a baseline social support survey is crucial to understand the specific support that PSH residents will need the most.
Similar directions of correlation between the growth pattern of social support and substance use problems were observed in the other parallel process model. As expected, the statistically significant negative link between the baseline social support and the linear changing rate of substance use indicates that PSH residents who had higher perceived social support at baseline experienced faster improvements in substance use problems. Similarly, the negative link between the baseline substance use problems and the changing rate of social support indicates that PSH residents who had more severe substance use problems at baseline experienced a slower increase in social support. Some researchers have speculated that social support and substance use might be mutually exclusive strategies to cope with stress, such that greater social support might suppress substance use problems [8]. The findings from the current study may reiterate the protective association between social support and substance use problems and emphasize the necessity of understanding the social support among PSH residents from the perspective of improving substance use problems. In the future, program officers might consider ways to strengthen social connections for people newly placed in PSH, for example, by encouraging social support groups, matching residents with a peer mentor, or considering the proximity of a person’s natural support networks when determining the location of supportive housing placement.
Our findings should be interpreted with several cautions. First, there are significant variations among healthcare and case management services, demographic distributions, and their interest in participating in health coaching programs within the PSH population. Because all participants in this study received monthly health coaching, it is challenging to attribute their positive changes solely to health coaching. Second, it is also possible that PSH residents with improving health may report greater social support, although the reported interpretation of the association between social support and health behaviors is more consistent with the literature. Considering the findings from past studies indicating that PSH programs alone may not be sufficient to improve social support among PSH residents [20, 21], we believe that an experimental or quasi-experimental study is needed to confirm and verify the effects of social support on depressive symptoms and substance use problems in this population over time. Third, measures of social support and substance use problems in this study were modified from the original versions, though they were all formally tested in the current study. Fourth, this was a study conducted in one US metropolitan area with limited diversity/heterogeneity in samples, methods, and coaching programs. Therefore, how well the findings from this study can be generalized is an open question. Finally, we had infrequent health outcomes assessment by a team of assessors every six months at 6, 12, and 18-months following baseline. Future studies using shorter and more frequent intervals, especially early during coaching, would support more fine-grained analysis and evidence to help guide PSH programs.
Conclusions
This study is one of the few longitudinal studies to examine social support, depressive symptoms, and substance use problems among PSH residents, an underserved population. With relatively frequent follow-ups over 18 months, this study reveals the pattern of change in two sets of health behaviors simultaneously using parallel process models. The use of latent variable models, including measurement models and latent growth curve models, allows us to formally test our measurement tools to assure good performance and stable properties across time as well as to maximize the available data to examine the research questions. The findings in this study suggest that the trajectory of social support is very likely to influence the trajectories of depressive symptoms and substance use problems. These findings suggest new ways to integrate these behavioral health targets in the development of intervention and prevention programs for PSH residents.
Availability of data and materials
The datasets used and analyzed during the current study cannot be made publicly available due to IRB restrictions, but may be available from the corresponding author on reasonable request.
Abbreviations
- PSH:
-
Permanent supportive housing
- LGCM:
-
Latent growth curve model
- m.chat:
-
Mobile community health assistance for tenants
- MLR:
-
Robust maximum likelihood
- RMSEA:
-
Root mean squared error approximation
- CFI:
-
Comparative fit index
- PHQ-9:
-
Patient Health Questionnaire-9
- InDUC:
-
Inventory of drug use consequences
- ISEL:
-
Interpersonal support evaluation list
References
National Academies of Sciences Engineering and Medicine. Permanent supportive housing: evaluating the evidence for improving health outcomes among people experiencing chronic homelessness. Washington, DC: National Academies Press; 2018.
Fazel S, Geddes JR, Kushel M. The health of homeless people in high-income countries: descriptive epidemiology, health consequences, and clinical and policy recommendations. Lancet. 2014;384(9953):1529–40.
Romaszko J, Cymes I, Dragańska E, Kuchta R, Glińska-Lewczuk K. Mortality among the homeless: causes and meteorological relationships. PLoS ONE. 2017;12(12):e0189938. https://doi.org/10.1371/journal.pone.0189938.
Larimer ME, Malone DK, Garner MD, Atkins DC, Burlingham B, Lonczak HS, et al. Health care and public service use and costs before and after provision of housing for chronically homeless persons with severe alcohol problems. JAMA. 2009;301(13):1349–57. https://doi.org/10.1001/jama.2009.414.
Brody DJ, Pratt LA, Hughes JP. Prevalence of depression among adults aged 20 and over: United States, 2013–2016. National Center for Health Statistics Data Brief. 2018;303:1–8.
Miller-Archie SA, Walters SC, Singh TP, Lim S. Impact of supportive housing on substance use–related health care utilization among homeless persons who are active substance users. Ann Epidemiol. 2019;32(1–6):e1. https://doi.org/10.1016/j.annepidem.2019.02.002.
Turner LR, Mermelstein R, Hitsman B, Warnecke RB. Social support as a moderator of the relationship between recent history of depression and smoking cessation among lower-educated women. Nicotine Tob Res. 2008;10(1):201–12. https://doi.org/10.1080/14622200701767738.
Tucker JS, D’Amico EJ, Wenzel SL, Golinelli D, Elliott MN, Williamson S. A prospective study of risk and protective factors for substance use among impoverished women living in temporary shelter settings in Los Angeles County. Drug Alcohol Depend. 2005;80(1):35–43. https://doi.org/10.1016/j.drugalcdep.2005.03.008.
Durden ED, Hill TD, Angel RJ. Social demands, social supports, and psychological distress among low-income women. J Soc Pers Relat. 2007;24(3):343–61. https://doi.org/10.1177/0265407507077226.
Warren JI, Stein JA, Grella CE. Role of social support and self-efficacy in treatment outcomes among clients with co-occurring disorders. Drug Alcohol Depend. 2007;89(2–3):267–74. https://doi.org/10.1016/j.drugalcdep.2007.01.009.
Fitzpatrick KM. How positive is their future? Assessing the role of optimism and social support in understanding mental health symptomatology among homeless adults. Stress Health. 2017;33(2):92–101. https://doi.org/10.1002/smi.2676.
Irwin J, LaGory M, Ritchey F, Fitzpatrick K. Social assets and mental distress among the homeless: exploring the roles of social support and other forms of social capital on depression. Soc Sci Med. 2008;67(12):1935–43. https://doi.org/10.1016/j.socscimed.2008.09.008.
Stergiopoulos V, Hwang SW, Gozdzik A, Nisenbaum R, Latimer E, Rabouin D, et al. Effect of scattered-site housing using rent supplements and intensive case management on housing stability among homeless adults with mental illness: a randomized trial. JAMA. 2015;313(9):905–15. https://doi.org/10.1001/jama.2015.1163.
Henry M, Watt R, Mahathey A, Ouellette J, Sitler A. The 2019 Annual Homeless Assessment Report (AHAR) to Congress. Washington, DC: US Department of Housing and Urban Development; 2020. p. 80.
Kleit RG. Draining ties: Tie quality versus content in low-income women’s social networks when displaced by redevelopment. J Soc Pers Relat. 2010;27(4):573–88. https://doi.org/10.1177/0265407510363430.
Cobb S. Social support as a moderator of life stress. Psychosom Med. 1976;38(5):300–14. https://doi.org/10.1097/00006842-197609000-00003.
Coe AB, Moczygemba LR, Gatewood SB, Osborn RD, Matzke GR, Goode JV. Medication adherence challenges among patients experiencing homelessness in a behavioral health clinic. Res Soc Adm Pham. 2015;11(3):e110–20. https://doi.org/10.1016/j.sapharm.2012.11.004.
Harris RA, Xue X, Selwyn PA. Housing stability and medication adherence among HIV-positive individuals in antiretroviral therapy: a meta-analysis of observational studies in the United States. J Acquir Immune Defic Syndr. 2017;74(3):309–17. https://doi.org/10.1097/QAI.0000000000001213.
Johnstone M, Parsell C, Jetten J, Dingle G, Walter Z. Breaking the cycle of homelessness: housing stability and social support as predictors of long-term well-being. Hous Stud. 2016;31(4):410–26. https://doi.org/10.1080/02673037.2015.1092504.
Tsai J, Mares AS, Rosenheck RA. Does housing chronically homeless adults lead to social integration? Psychiat Serv. 2012;63(5):427–34. https://doi.org/10.1176/appi.ps.201100047.
Yanos PT, Stefancic A, Tsemberis S. Objective community integration of mental health consumers living in supported housing and of others in the community. Psychiat Serv. 2012;63(5):438–44. https://doi.org/10.1176/appi.ps.201100397.
Holmes EJ, Yang L, Aryal S, Walters ST. Influence of lifestyle behaviors and social support on depressive symptoms. Health Behav Policy Rev. 2018;5(5):28–36. https://doi.org/10.14485/HBPR.5.5.3.
Toro PA, Tulloch E, Ouellette N. Stress, social support, and outcomes in two probability samples of homeless adults. J Community Psychol. 2008;36(4):483–98. https://doi.org/10.1002/jcop.20190.
Stein JA, Dixon EL, Nyamathi AM. Effects of psychosocial and situational variables on substance abuse among homeless adults. Psychol Addict Behav. 2008;22(3):410–6. https://doi.org/10.1037/0893-164X.22.3.410.
Kirst M, Zerger S, Misir V, Hwang S, Stergiopoulos V. The impact of a housing first randomized controlled trial on substance use problems among homeless individuals with mental illness. Drug Alcohol Depend. 2015;146:24–9. https://doi.org/10.1016/j.drugalcdep.2014.10.019.
Durbin A, Nisenbaum R, Kopp B, O’Campo P, Hwang SW, Stergiopoulos V. Are resilience and perceived stress related to social support and housing stability among homeless adults with mental illness? Health Soc Care Community. 2019;27(4):1053–62. https://doi.org/10.1111/hsc.12722.
Tsai J, Kasprow WJ, Rosenheck RA. Alcohol and drug use disorders among homeless veterans: prevalence and association with supported housing outcomes. Addict Behav. 2014;39(2):455–60. https://doi.org/10.1016/j.addbeh.2013.02.002.
Barker S, Barron N, McFarland BH, Bigelow DA. A community ability scale for chronically mentally ill consumers: Part I. Reliability and validity. Community Ment Health J. 1994;30(4):363–83. https://doi.org/10.1007/BF02207489.
Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–33.
Lehman AF. The well-being of chronic mental patients: assessing their quality of life. Arch Gen Psychiatry. 1983;40(4):369–73. https://doi.org/10.1001/archpsyc.1983.01790040023003.
Dennis ML, Chan Y-F, Funk RR. Development and validation of the GAIN Short Screener (GSS) for internalizing, externalizing and substance use disorders and crime/violence problems among adolescents and adults. Am J Addict. 2006;15(s1):s80–91. https://doi.org/10.1080/10550490601006055.
Stucky BD, Edelen MO, Ramchand R. A psychometric assessment of the GAIN Individual Severity Scale (GAIN-GISS) and Short Screeners (GAIN-SS) among adolescents in outpatient treatment programs. J Subst Abuse Treat. 2014;46(2):165–73. https://doi.org/10.1016/j.jsat.2013.07.007.
Cohen S, Hoberman H. Positive events and social supports as buffers of life change stress. J Appl Soc Psychol. 1983;13(2):99–125. https://doi.org/10.1111/j.1559-1816.1983.tb02325.x.
Cohen S, Mermelstein R, Kamarck T, Hoberman HM. Measuring the functional components of social support. In: Sarason IG, Sarason BR, editors. Social support: theory, research and applications. Springer: Dordrecht; 1985. p. 73–94.
Tonigan JS, Miller WR. The inventory of drug use consequences (InDUC): test-retest stability and sensitivity to detect change. Psychol Addict Behav. 2002;16(2):165–8.
Walters S, Spence-Almaguer E, Hill W, Abraham S. Integrating health coaching and technology with vulnerable clients. Soc Work Today. 2015;15(5):6.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. https://doi.org/10.1046/j.1525-1497.2001.016009606.x.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed. American Psychiatric Association; 1994.
McArdle JJ, Epstein D. Latent growth curves within developmental structural equation models. Child Dev. 1987;58(1):110–33. https://doi.org/10.2307/1130295.
Muthén B, Christoffersson A. Simultaneous factor analysis of dichotomous variables in several groups. Psychometrika. 1981;46(4):407–19. https://doi.org/10.1007/BF02293798.
Meredith W. Measurement invariance, factor analysis and factorial invariance. Psychometrika. 1993;58(4):525–43. https://doi.org/10.1007/BF02294825.
Widaman KF, Reise SP. Exploring the measurement invariance of psychological instruments: applications in the substance use domain. In: Bryant KJ, Windle M, West SG, editors. The science of prevention: methodological advances from alcohol and substance abuse research. Washington, DC: American Psychological Association; 1997. p. 281–324.
Satorra A, Bentler PM. Ensuring positiveness of the scaled difference Chi-square test statistic. Psychometrika. 2010;75(2):243–8. https://doi.org/10.1007/s11336-009-9135-y.
McArdle JJ. Dynamic but structural equation modelling of repeated measures data. In: Nesselroade JR, Cattell RB, editors. Handbook of multivariate experimental psychology. Boston, MA: Springer; 1988. p. 561–614.
MacCallum RC, Kim C, Malarkey WB, Kiecolt-Glaser JK. Studying multivariate change using multilevel models and latent curve models. Multivar Behav Res. 1997;32(3):215–53. https://doi.org/10.1207/s15327906mbr3203_1.
Muthén BO. Beyond SEM: general latent variable modeling. Behaviormetrika. 2002;29(1):81–117. https://doi.org/10.2333/bhmk.29.81.
Schulenberg J, Maggs JL. Moving targets: modeling developmental trajectories of adolescent alcohol misuse, individual and peer risk factors, and intervention effects. Appl Dev Sci. 2001;5(4):237–53. https://doi.org/10.1207/S1532480XADS0504_05.
Hartley HO, Hocking RR. The analysis of incomplete data. Biometrics. 1971;27(4):783–823. https://doi.org/10.2307/2528820.
Steiger JH. Structural model evaluation and modification: an interval estimation approach. Multivar Behav Res. 1990;25(2):173–80. https://doi.org/10.1207/s15327906mbr2502_4.
Steiger JH, Lind JC. Statistically-based tests for the number of common factors. Iowa City, IA: The annual meeting of the Psychometric Society; 1980.
Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–46. https://doi.org/10.1037/0033-2909.107.2.238.
Browne W, Cudeck R. Alternative ways of assessing model fit. In: Bollen K, Long JS, editors. Testing structural equation models. Newbury Park, CA: Sage Publications; 1993. p. 136–62.
Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55. https://doi.org/10.1080/10705519909540118.
Garnier-Villarreal M, Jorgensen TD. Adapting fit indices for Bayesian structural equation modeling: comparison to maximum likelihood. Psychol Methods. 2020;25(1):46–70. https://doi.org/10.1037/met0000224.
Schumacker RE, Lomax RG. A beginner’s guide to structural equation modeling. 2nd ed. Mahwah, NJ: Lawrence Erlbaum Associates Publishers; 2004.
Hu L-T, Bentler PM. Evaluating model fit. In: Hoyle RH, editor. Structural equation modeling: concepts, issues, and applications. Thousand Oaks, CA: Sage Publications Inc; 1995. p. 76–99.
Muthén LK, Muthén BO. Mplus user’s guide, 8th ed. Los Angeles, CA: Muthén & Muthén; 1998–2020.
Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–57.
Acknowledgements
The authors would like to thank the clients and staff who participated in the m.chat project.
Funding
This study was supported by a Medicaid 1115 Waiver to the State of Texas by Centers for Medicare and Medicaid Services (CMS) and in part by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) of the National Institutes of Health (NIH) under Award Number R01 AA019511. CMS had no role in the study design, collection, analysis or interpretation of the data, writing the manuscript, or the decision to submit the paper for publication. Likewise, the content of this paper is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA or the NIH.
Author information
Authors and Affiliations
Contributions
ZT and EYM developed the overall scope of this paper and drafted early versions of this manuscript. STW designed the original m.chat study and oversaw data collection and implementation of the m.chat study. ZT, EYM, USN, and STW reviewed and edited this manuscript over multiple rounds. All authors made substantial contributions to the interpretation of data, and critically revised the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This project was approved by the North Texas Regional Institutional Review Board, and participants were given assurances of confidentiality. Written informed consent was obtained from each study participant.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1
. Supplemental table for measurement model fit indices and diagrams for measurement models and latent growth curve models.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Tan, Z., Mun, EY., Nguyen, US.D.T. et al. Increases in social support co-occur with decreases in depressive symptoms and substance use problems among adults in permanent supportive housing: an 18-month longitudinal study. BMC Psychol 9, 6 (2021). https://doi.org/10.1186/s40359-020-00507-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40359-020-00507-0