
Abstract
Purpose
Coding mutations in the Transthyretin (TTR) gene cause a hereditary form of amyloidosis characterized by a complex genotype-phenotype correlation with limited information regarding differences among worldwide populations.
Methods
We compared 676 diverse individuals carrying TTR amyloidogenic mutations (rs138065384, Phe44Leu; rs730881165, Ala81Thr; rs121918074, His90Asn; rs76992529, Val122Ile) to 12,430 non-carriers matched by age, sex, and genetically-inferred ancestry to assess their clinical presentations across 1,693 outcomes derived from electronic health records in UK biobank.
Results
In individuals of African descent (AFR), Val122Ile mutation was linked to multiple outcomes related to the circulatory system (fold-enrichment = 2.96, p = 0.002) with the strongest associations being cardiac congenital anomalies (phecode 747.1, p = 0.003), endocarditis (phecode 420.3, p = 0.006), and cardiomyopathy (phecode 425, p = 0.007). In individuals of Central-South Asian descent (CSA), His90Asn mutation was associated with dermatologic outcomes (fold-enrichment = 28, p = 0.001). The same TTR mutation was linked to neoplasms in European-descent individuals (EUR, fold-enrichment = 3.09, p = 0.003). In EUR, Ala81Thr showed multiple associations with respiratory outcomes related (fold-enrichment = 3.61, p = 0.002), but the strongest association was with atrioventricular block (phecode 426.2, p = 2.81 × 10− 4). Additionally, the same mutation in East Asians (EAS) showed associations with endocrine-metabolic traits (fold-enrichment = 4.47, p = 0.003). In the cross-ancestry meta-analysis, Val122Ile mutation was associated with peripheral nerve disorders (phecode 351, p = 0.004) in addition to cardiac congenital anomalies (fold-enrichment = 6.94, p = 0.003).
Conclusions
Overall, these findings highlight that TTR amyloidogenic mutations present ancestry-specific and ancestry-convergent associations related to a range of health domains. This supports the need to increase awareness regarding the range of outcomes associated with TTR mutations across worldwide populations to reduce misdiagnosis and delayed diagnosis of TTR-related amyloidosis.
Similar content being viewed by others

Introduction
Transthyretin (TTR) is a homo-tetrameric protein involved in a wide range of physiological processes [1, 2]. The dissociation of the TTR tetramer initiates an amyloidogenic process, where the misfolded monomers lead to non-native oligomers and finally amyloid fibrils [3]. Coding mutations in the TTR gene cause TTR misfolding and are responsible for a hereditary form of amyloidosis, TTR-related amyloidosis (hATTR) [4]. TTR amyloid fibrils can affect a range of tissues and organs, resulting in a high clinical variability among individuals carrying TTR amyloidogenic mutations [5, 6]. While hATTR is an autosomal dominant disease, penetrance is variable, and patients can present with distinct phenotypes and differential organ involvement including cardiomyopathy, polyneuropathy, vasculopathy, gastrointestinal impairment, nephropathy, ocular deposition, and genitourinary involvement [7,8,9,10,11]. hATTR is often misdiagnosed or diagnosed several years after the onset of the initial symptoms due to the heterogeneous clinical presentation of TTR amyloidogenic mutations12,13. A consistent variation in hATTR clinical presentation has been also reported among different population origins [5, 6, 8]. However, population comparisons have mostly been limited to cohorts of European and East Asian descent for most TTR amyloidogenic mutations (e.g., TTR Val30Met, rs28933979) and to individuals of African descent for TTR Val122Ile mutation (rs76992529) [8, 10, 12]. Recently, molecular and computational studies demonstrated that non-coding mechanisms regulating transcriptomic and epigenetic variation of the TTR gene partially explain hATTR clinical heterogeneity [13,14,15,16], including the differences among diverse populations [17,18,19]. However, the knowledge of the clinical presentation associated with TTR amyloidogenic mutations is still too limited for several human populations. This can also lead to a lack of awareness among clinicians in areas that do not have a previous history of hATTR cases.
To expand the understanding of the clinical spectrum of TTR mutations among underrepresented, diverse ancestral groups, we performed a phenome-wide analysis comparing TTR mutations in individuals of African (AFR), Admixed-American (AMR), Central/South Asian (CSA), East Asian (EAS), and Middle Eastern (MID) descents to non-carriers matched for age, sex, and genetically-inferred ancestry. Specifically, we systematically tested associations across 1,693 outcomes derived from electronic health records available from the UK Biobank (UKB) [20] and investigated ancestry-specific and ancestry-convergent enrichment for health domains and comorbidity networks linking TTR-associated outcomes.
Materials and methods
Study population
The UKB cohort is a controlled access genomics resource containing information on a wide range of illnesses as well as normal-range traits [20]. This project has recruited more than 500,000 people. Phenotypic information was collected for each participant using multiple data sources. In the present study, we derived clinical information regarding a range of health outcomes from UKB electronic health records. Specifically, we used previously defined phecode categorization [21] to translate the International Classification of Diseases 9th and 10th (ICD9/ICD10) codes into clinically meaningful phecode outcomes. A total of 1,693 phecodes were available from UK Biobank (Supplemental Table 1). UKB phecodes are grouped into 17 categories: circulatory system (N = 155), congenital anomalies (N = 55), dermatologic (N = 95), digestive (N = 155), endocrine/metabolic (N = 151), genitourinary (N = 156), hematopoietic (N = 54), infectious diseases (N = 58), injuries & poisonings (N = 133), mental disorders (N = 71), musculoskeletal (N = 122), neoplasms (N = 135), neurological (N = 78), pregnancy complications (N = 49), respiratory (N = 75), sense organs (N = 113), and symptoms (N = 38).
Genome-wide genotyping was performed on all UKB participants using the UKB Axiom Array, with approximately 850,000 variants directly measured and > 90 million variants imputed using the Haplotype Reference Consortium and UK10K + 1000 Genomes Project reference panels [20]. Pan-UKB investigators used genome-wide data to infer the ancestral backgrounds of UKB participants. Details are available at https://pan.ukbb.broadinstitute.org/docs/qc. Briefly, ancestries (i.e., AFR, AMR, CSA, EAS, EUR, and MID) were assigned using a random forest classifier based on features predictive of similarities with reference populations derived from a combined 1,000 Genomes Project [22] and Human Genome Diversity Panel [23]. Considering Pan-UKB ancestry assignments and genetically unrelated individuals (kinship coefficients < 0.125), we identified 676 individuals carrying four different TTR mutations (rs138065384, Phe44Leu, p.Phe64Leu; rs730881165, Ala81Thr, p.Ala101Thr; rs121918074, His90Asn, p.His110Asn.; rs76992529, Val122Ile, p.Val142Ile; Table 1). No other potentially pathogenic TTR mutation was identified in UKB cohort. Phe44Leu, Ala81Thr, and Val122Ile were classified as amyloidogenic (Supplemental Table 2) according to a curated database [24] available at http://www.amyloidosismutations.com/. This online registry aims to collect information on mutations associated with hereditary amyloidosis, providing details regarding their pathogenicity based on (i) sufficient clinical information, (ii) histological evidence of amyloid deposition, and (iii) appropriate amyloid fibril type [24]. In addition to the three mutations, we also considered His90Asn, because of the recent evidence supporting its pathogenicity [25]. Considering ClinVar germline classification [26] performed according to the criteria recommended by the American College of Medical Genetics and Genomics and the Association for Molecular Pathology (ACMG/AMP) [27], Val122Ile is classified as pathogenic, while Phe44Leu, Ala81Thr, His90Asn are reported as “Conflicting classifications of pathogenicity” (Supplemental Table 2). High-quality genotype data were available for Phe44Leu, Ala81Thr, His90Asn, and Val122Ile in UKB (INFO > 0.6; Supplemental Table 2). The minor allele frequency of these variants was in line with what reported in the reference populations available from the 1,000 Genomes Project [22] and the Genome Aggregation Database [28] (Supplemental Table 3). To define genetically comparable non-carrier group, we used MatchIT R package [29], considering age, sex, and the first ten within-ancestry principal components as matching criteria. To achieve the best balance in our dataset, we used the “nearest” method that performs greedy nearest neighbor matching by computing a distance between carrier and non-carrier samples. The optimal number of matched non-carriers to each carrier was defined using a k:1 matching. Chi-square and t-test analyses were performed to compare carriers and non-carriers with respect to binary and quantitative matching criteria, respectively. No statistical difference (p > 0.1) was observed for age, sex, and within-ancestry principal components between carriers and matched non-carriers in each of the ancestry-mutation groups investigated (Supplemental Table 4).
Statistical analyses
To investigate the association of TTR amyloidogenic mutations (Phe44Leu, Ala81Thr, His90Asn, and Val122Ile; Supplemental Table 2) with clinically meaningful phenotypes (Supplemental Table 1), we compared carrier group and matched non-carriers using Fisher’s exact test. This approach was chosen because it is robust to investigate genetic associations when there is an extreme case-control imbalance due to low minor allele frequency and/or to the rare conditions investigated [30]. In the present study, we used fisher.test R function, analyzing ancestry-mutation groups separately (Table 1). A cross-ancestry meta-analysis was performed to investigate ancestry-convergent associations of TTR amyloidogenic mutations. This analysis was conducted using the sample-size weighted approach available in METAL [31]. Specifically, we converted Fisher’s exact test ancestry-specific p values into signed z scores where positive values correspond to positive associations between TTR mutations and the phecodes and negative values correspond to negative associations. With the METAL sample-size weighted approach [31], the ancestry-specific z scores were combined across samples with weights proportional to the square-root of the effective sample size. The effective sample size was calculated with the following formula: \(4/(1/{N}_{cases}+1/{N}_{controls})\). Heterogeneity statistics (I2, chi-square, and p values) were calculated to estimate the variation among ancestry-specific effects. While all ancestry-specific effects were entered in the cross-ancestry meta-analysis, this was limited to phecodes with at least two ancestry-specific z scores≠0.
To test the over-representation of categories among the associations between TTR mutations and the phecodes investigated, we calculated the statistical significance of the phenotypic enrichment. Considering the hypergeometric cumulative distribution function, we compared the proportions of the phenotypic classes associated with the variants investigated with the proportion of phenotypic classes across the overall phenotypic spectrum investigated for each ancestry-mutation group. Over-representation analysis was also conducted with respect to cross-ancestry associations observed for each mutation.
Because the limited sample size available did not provide adequate statistical power to test individual phecode associations applying a stringent multiple testing correction, the primary outcomes of the study were the category enrichments surviving false discovery rate (FDR q < 0.05) accounting for the number of category enrichments tested. Within each FDR-significant category, we prioritized the top phecode associations.
Comorbidity analysis
To investigate comorbidities among clinical outcomes associated with TTR mutations, we used previously calculated UK Biobank data [32]. Specifically, we considered information regarding relative risk (RR) to measure the tendency of co-occurrence among disease pairs. The RR for two diseases was measured as the ratio of risk between the diseases based on the disease prevalence. RR > 1 indicates a co-occurrence among the disease pair tested, while RR < 1 corresponds to a less probable co-occurrence. Bonferroni correction was applied to account for the number of disease pairs tested.
Results
In UKB cohorts, we identified four TTR amyloidogenic mutations: Phe44Leu, Ala81Thr, His90Asn, and Val122Ile (Table 1). While Phe44Leu was observed only in AFR individuals, the other mutations were observed in multiple ancestry groups. Specifically, Val122Ile was identified in AFR, AMR, CSA, EUR, and MID; His90Asn in CSA, EUR, and MID; Ala81Thr in EAS and EUR. Ancestry-specific allele frequency of these mutations was in line with that observed in the reference populations available from the 1,000 Genomes Project [22] and the Genome Aggregation Database [28] (Supplemental Table 3).
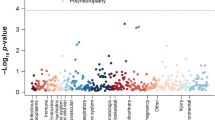
In our phenome-wide analysis, we identified a total of 179 nominally significant associations (p < 0.05; Fig. 1, Supplemental Table 5) with respect to TTR Ala81Thr, His90Asn, and Val122Ile mutations (60, 54, and 65 associations, respectively). No associations were observed with respect to TTR Phe44Leu variant (p > 0.05; Supplemental Table 5). Considering phecode categories, we observed statistically significant overrepresentation of associations across the mutation-by-ancestry analyses (Table 2; Supplemental Table 6). Five of them survived FDR multiple testing correction (FDR q < 0.05). Because no phecode reached a nominally significant association with respect to Phe44Leu, we did not perform an overrepresentation test for this mutation. In AFR, Val122Ile associations related to circulatory system were significantly enriched (fold-enrichment = 2.96, p = 0.002). In this category, the strongest AFR-Val122Ile associations were endocarditis (phecode 420.3, p = 0.006) and cardiomyopathy (phecode 425, p = 0.007). Although they were included among congenital anomalies, Val122Ile in AFR was also associated with cardiac congenital anomalies (phecode 747.1, p = 0.003). No category enrichment survived multiple testing correction for Val122Ile associations in the other ancestry groups (FDR q > 0.05). Conversely, multiple ancestry-specific enrichments for Ala81Thr and His90Asn associations survived FDR multiple testing correction (Table 2). With respect to Ala81Thr mutations, EAS showed an overrepresentation of endocrine/metabolic associations (fold-enrichment = 4.47, p = 0.003) such as pituitary hyperfunction (phecode 253.1, p = 0.01) and hypoosmolality/hyponatremia (phecode 276.12, p = 0.03). In EUR, Ala81Thr mutation was enriched for respiratory associations (fold-enrichment = 3.61, p = 0.002) such as obstructive chronic bronchitis (phecode 496.21, p = 0.009). However, the strongest EUR-Ala81Thr association was with atrioventricular block (phecode 426.2, p = 2.81 × 10− 4) although the overrepresentation for circulatory associations was only nominally significant (fold-enrichment = 2.47, p = 0.005, FDR q = 0.056). With respect to His90Asn mutation, CSA was associated with dermatologic outcomes (fold-enrichment = 28, p = 0.001), such as changes in skin texture (phecode 687.3, p = 0.01). In the EUR-His90Asn analysis, we observed an overrepresentation of associations related to neoplasms category (fold-enrichment = 3.09, p = 0.003). These included neoplasms located in different body sites such as malignant neoplasm of female breast (phecode 174.11, p = 0.003), malignant neoplasm of other urinary organs (phecode 189.4, p = 0.01), and neurofibromatosis (phecode 199.4, p = 0.01).

Phenome-wide associations of TTR amyloidogenic mutations across ancestry groups. Plotted results include those with p < 1. Full results are available in Supplemental Table 5. AFR: African; EUR: European; MID: Middle Eastern
In the cross-ancestry meta-analysis (Supplemental Table 7), the strongest association was between Val122Ile and other peripheral nerve disorders (phecode 351, p = 0.004). No cross-ancestry heterogeneity (heterogeneity p = 0.693) was observed in the ancestry-specific effects in AFR and EUR (AFR p = 0.029; EUR p = 0.059). With respect to Ala81Thr mutation, the strongest cross-ancestry association was observed with respect to dysphagia (phecode 532, p = 0.007; cross-ancestry heterogeneity p = 0.362) where consistent effects were observed in EUR and EAS (EUR p = 0.026; EAS p = 0.08). Considering category overrepresentation (Supplemental Table 8), Val122Ile mutation was enriched for congenital anomalies (fold-enrichment = 6.94, p = 0.003) with the strongest evidence observed with respect to cardiac congenital anomalies (phecode 747.1, cross-ancestry p = 0.005). Although there was no statistically significant heterogeneity (heterogeneity p = 0.110), the cross-ancestry association was primarily driven by the effect observed in AFR (AFR p = 0.003), which was much stronger than the one in EUR (EUR p = 0.156). Considering cross-ancestry heterogeneity statistics, we observed an overrepresentation of nominally significant heterogeneous effects of Val122Ile among neoplasm-related outcomes (fold-enrichment = 4.53, p = 0.005). The strongest evidence was related to lipoma (phecode 214, cross-ancestry heterogeneity p = 0.006) where AFR and AMR Val122Ile associations showed opposite effect directions (AFR p = 0.077, direction +; AMR p = 0.010, direction -).
Because multiple phecodes were associated with Val122Ile mutation in the cross-ancestry meta-analysis (Supplemental Table 7), we investigated their comorbidity network. This analysis was limited to 11 phecodes with comorbidity data available [32]. Utilizing a Bonferroni correction to account for the number of pair-wise comparisons tested (p < 8.62×10− 4), we identified 35 statistically significant comorbid pairs (Fig. 2; Supplemental Table 9). Twenty-seven of them were pairs of phecodes related to different categories. Among these cross-category pairs, the highest RR estimates were observed for the comorbidity of cardiac congenital anomalies (phecode 747.1) with heart valve replaced (phecode 395.6, circulatory category; RR = 20.29, p = 2.34×10− 114), esophageal bleeding (phecode 530.2, digestive category; RR = 5.14, p = 2.20×10− 7), and rheumatoid arthritis (phecode 714.1, musculoskeletal category; RR = 4.18, p = 7.89×10− 7).

Comorbidity network of phecodes associated with TTR Val122Ile mutation in the cross-ancestry meta-analysis. Edges are proportional to the relative risk of pair-wise comorbid phecodes surviving Bonferroni multiple testing correction (p < 8.62×10− 4). Full results are available in Supplemental Table 9. 351: Other peripheral nerve disorders; 395.6: Heart valve replaced; 530.2: Esophageal bleeding (varices_hemorrhage); 565: Anal and rectal conditions; 565.1: Anal and rectal polyp; 714: Rheumatoid arthritis and other inflammatory polyarthropathies; 714.1: Rheumatoid arthritis; 727: Other disorders of synovium, tendon, and bursa; 747: Cardiac and circulatory congenital anomalies; 747.1: Cardiac congenital anomalies: 747.13: Congenital anomalies of great vessels
Discussion
The present study leveraged genetic and clinical data from UKB cohort to understand the spectrum of health outcomes associated with TTR amyloidogenic mutations among diverse ancestral backgrounds. Several studies highlighted differences in the genotype-phenotype correlation of TTR mutations among human populations [8, 10, 12]. However, there are still several ancestry groups where no information is available regarding TTR mutations. In the present study, we broaden the knowledge regarding the distribution and the clinical spectrum of TTR amyloidogenic mutations in six ancestry groups. For example, TTR Val122Ile mutation is well-known to affect primarily AFR individuals, but it can be present also in EUR populations due to an independent mutation event rather than genetic admixture [33, 34]. In UKB, Val122Ile was identified in unrelated participants of AFR, AMR, CSA, EUR, and MID descent. While Val122Ile mutation has been previously reported in Hispanic and Latino America populations [35], very limited information is available regarding hATTR in CSA and MID individuals [36, 37]. In line with the known causal role of Val122Ile in cardiac amyloidosis [38], we observed an overrepresentation of Val122Ile associations with circulatory phecodes in AFR. One of the strongest findings was related to cardiomyopathy, which is a primary Val122Ile outcome due to the accumulation of TTR fibrils in the myocardium [39]. We also observed that Val122Ile mutation in AFR could be linked to endocarditis (phecode 420.3). While there is no previous information regarding endocarditis and Val122Ile, this association may be related to endocarditis risk observed after pacemaker implantation [40], which is recommended for patients with cardiac amyloidosis to prevent bradycardia and syncope [41]. In the cross-ancestry meta-analysis, Val122Ile was enriched for associations with cardiac congenital anomalies with consistent effects in both AFR and EUR. Similarly, we also observed an AFR-EUR cross-ancestry association between Val122Ile mutation and peripheral nerve disorders (phecode 351). While cardiac amyloidosis is the primary Val122Ile outcome [39], our finding is consistent with previous reports supporting that Val122Ile may be related to peripheral neuropathy symptoms that are more often reported with respect to other TTR amyloidogenic mutations [42]. This is in line with the results of a previous phenome-wide analysis in UKB-AFR participants, reporting an association of Val122Ile with polyneuropathy [43]. The comorbidity analysis highlighted high RR among Val122Ile-associated phecodes, also when considering the whole UKB cohort. Indeed, while congenital anomalies (cardiac and of great vessels) and heart valve replacement showed a RR about four times larger than the other cross-category pairs, 16 of the 26 cross-category pairs had a RR > 2. This suggests that genetic testing remain a primary tool to distinguish comorbidity patterns due to Val122Ile.
Ala81Thr was identified in EAS and EUR participants enrolled in UKB cohort. Very limited information is available regarding this TTR amyloidogenic mutation, which has been mostly reported in EUR populations [44,45,46]. In EAS, Ala81Thr showed multiple associations with endocrine/metabolic outcomes. In this category, the most significant evidence was related to phecodes linked to neurohypophysis disorders and hypoosmolality/hyponatremia. Hyponatremia due to altered neurohypophysis regulation of vasopressin is a common electrolyte imbalance in neurologic patients [47]. In the context of hATTR, hyponatremia has been observed in cases of cardiac amyloidosis [48, 49]. Further studies will be needed to confirm and understand Ala81Thr link with neurohypophysis disorders and hypoosmolality/hyponatremia in EAS carriers. In EUR, Ala81Thr presented associations with respiratory outcomes such as obstructive chronic bronchitis. This is in line with cases of pulmonary amyloidosis reported among hATTR patients [50, 51]. Additionally, the strongest Ala81Thr association was with atrioventricular block, which is observed in 40% of patients with hATTR-cardiac amyloidosis [52]. These findings contribute to our understanding of the spectrum of Ala81Thr mutation, which is currently unclear in the current literature.
We identified TTR His90Asn mutation in CSA, EUR, and MID. Although this variant was observed in EUR patients with cardiac amyloidosis and amyloidotic polyneuropathy [25, 53,54,55,56], it has been previously classified as a variant of uncertain significance according to the criteria of the Dilated Cardiomyopathy Precision Medicine Study [57]. In CSA, His90Asn was enriched for associations with dermatological outcomes. These were related to changes in skin texture. Cutaneous manifestations of hATTR have been previously reported [58] and skin biopsies have been previously proposed as a potential biomarker of disease severity in affected patients [59]. As mentioned above, very limited information is available regarding the presentation of TTR mutations in CSA populations [37]. Our findings suggest that His90Asn is associated with dermatologic presentations in CSA. In EUR, His90Asn was associated with neoplasms at different body sites (e.g., breast, urinary organs, and neurofibromatosis). There is no literature regarding the relationship between hATTR and cancer risk. Because TTR protein has been linked to tumor growth and severity [60,61,62,63], His90Asn associations observed in our study may be related to the effect of this mutation on TTR function rather than on the amyloidogenic cascade. This is in line with the associations observed for TTR non-coding variants in a previous phenome-wide analysis [15]. The lack of His90Asn enrichment for well-known hATTR-related outcomes may support the uncertain amyloidogenicity of His90Asn mutation.
Although our study provided novel information regarding the clinical spectrum of TTR mutations across multiple ancestry groups, our analyses were based on UK Biobank, which is a cohort that largely overrepresents EUR participants. Because this is a general-population cohort from UKB, we identified only a limited number of TTR mutations. To account for the high case-control imbalance, we applied Fisher’s exact test which is a highly conservative approach to investigate genetic associations [30]. This may have limited the power of our association analysis. While FDR multiple testing correction was applied to our overrepresentation analyses of health categories, we discussed nominally significant phecode associations within the FDR-significant categories. Further studies will be needed to confirm the associations identified in our study. Finally, we observed only a trend-association of Val122Ile with amyloidosis phecode (270.33) in AFR (p = 0.068). This may be due to amyloidosis referring to a heterogeneous group of disorders [64] or to TTR amyloidosis being underdiagnosed [65].
In conclusion, the present study provided novel insights regarding the possible associations of TTR amyloidogenic mutations across human populations. In particular, we identified TTR mutations in ancestries that are underrepresented in research and literature. Our findings also highlighted differences in hATTR-related health outcomes observed among diverse ancestral backgrounds. This contributes to expand our understanding of the spectrum of clinical outcomes potentially associated with TTR mutations and confirms the need to increase awareness regarding hATTR to reduce misdiagnosis and delayed diagnosis due to the complex genotype-phenotype correlation of the disease.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- AFR:
-
African
- AMR:
-
Admixed American
- CSA:
-
Central South Asian
- EAS:
-
East Asian
- EUR:
-
European
- hATTR:
-
Hereditary transthyretin amyloidosis
- MID:
-
Middle Eastern
- RR:
-
Relative Risk
- TTR:
-
Transthyretin
- UKB:
-
UK Biobank
References
Liz MA, Coelho T, Bellotti V, Fernandez-Arias MI, Mallaina P, Obici L. A narrative review of the role of transthyretin in health and disease. Neurol Ther. 2020;9(2):395–402.
Vieira M, Saraiva MJ. Transthyretin: a multifaceted protein. Biomol Concepts. 2014;5(1):45–54.
Si JB, Kim B, Kim JH. Transthyretin misfolding, a fatal structural pathogenesis mechanism. Int J Mol Sci. 2021;22(9).
Manganelli F, Fabrizi GM, Luigetti M, Mandich P, Mazzeo A, Pareyson D. Hereditary transthyretin amyloidosis overview. Neurol Sci. 2022;43(Suppl 2):595–604.
Ando Y, Coelho T, Berk JL, Cruz MW, Ericzon BG, Ikeda S, et al. Guideline of transthyretin-related hereditary amyloidosis for clinicians. Orphanet J Rare Dis. 2013;8:31.
Obi CA, Mostertz WC, Griffin JM, Judge DP. ATTR epidemiology, genetics, and prognostic factors. Methodist Debakey Cardiovasc J. 2022;18(2):17–26.
Adams D, Theaudin M, Cauquil C, Algalarrondo V, Slama M. FAP neuropathy and emerging treatments. Curr Neurol Neurosci Rep. 2014;14(3):435.
Buxbaum JN, Ruberg FL. Transthyretin V122I (pV142I)* cardiac amyloidosis: an age-dependent autosomal dominant cardiomyopathy too common to be overlooked as a cause of significant heart disease in elderly African americans. Genet Med. 2017;19(7):733–42.
Plante-Bordeneuve V, Kerschen P. Transthyretin familial amyloid polyneuropathy. Handb Clin Neurol. 2013;115:643–58.
Sekijima Y, Ueda M, Koike H, Misawa S, Ishii T, Ando Y. Diagnosis and management of transthyretin familial amyloid polyneuropathy in Japan: red-flag symptom clusters and treatment algorithm. Orphanet J Rare Dis. 2018;13(1):6.
Skrahina V, Grittner U, Beetz C, Skripuletz T, Juenemann M, Kramer HH, et al. Hereditary transthyretin-related amyloidosis is frequent in polyneuropathy and cardiomyopathy of no obvious aetiology. Ann Med. 2021;53(1):1787–96.
Parman Y, Adams D, Obici L, Galan L, Guergueltcheva V, Suhr OB, et al. Sixty years of transthyretin familial amyloid polyneuropathy (TTR-FAP) in Europe: where are we now? A European network approach to defining the epidemiology and management patterns for TTR-FAP. Curr Opin Neurol. 2016;29(Suppl 1Suppl 1):S3–13.
Pathak GA, De Lillo A, Wendt FR, De Angelis F, Koller D, Cabrera Mendoza B, et al. The integration of genetically-regulated transcriptomics and electronic health records highlights a pattern of medical outcomes related to increased hepatic transthyretin expression. Amyloid. 2022;29(2):110–9.
De Lillo A, Pathak GA, De Angelis F, Di Girolamo M, Luigetti M, Sabatelli M, et al. Epigenetic profiling of Italian patients identified methylation sites associated with hereditary transthyretin amyloidosis. Clin Epigenetics. 2020;12(1):176.
De Lillo A, De Angelis F, Di Girolamo M, Luigetti M, Frusconi S, Manfellotto D, et al. Phenome-wide association study of TTR and RBP4 genes in 361,194 individuals reveals novel insights in the genetics of hereditary and wildtype transthyretin amyloidoses. Hum Genet. 2019;138(11–12):1331–40.
Iorio A, De Lillo A, De Angelis F, Di Girolamo M, Luigetti M, Sabatelli M, et al. Non-coding variants contribute to the clinical heterogeneity of TTR amyloidosis. Eur J Hum Genet. 2017;25(9):1055–60.
Pathak GA, Wendt FR, De Lillo A, Nunez YZ, Goswami A, De Angelis F, et al. Epigenomic profiles of African-American transthyretin Val122Ile carriers reveals putatively dysregulated amyloid mechanisms. Circ Genom Precis Med. 2021;14(1):e003011.
Polimanti R, Nunez YZ, Gelernter J. Increased risk of multiple outpatient surgeries in African-American carriers of transthyretin Val122Ile mutation is modulated by non-coding variants. J Clin Med. 2019;8(2).
Iorio A, De Angelis F, Di Girolamo M, Luigetti M, Pradotto LG, Mazzeo A, et al. Population diversity of the genetically determined TTR expression in human tissues and its implications in TTR amyloidosis. BMC Genomics. 2017;18(1):254.
Bycroft C, Freeman C, Petkova D, Band G, Elliott LT, Sharp K, et al. The UK Biobank resource with deep phenotyping and genomic data. Nature. 2018;562(7726):203–9.
Bastarache L. Using phecodes for research with the electronic health record: from PheWAS to PheRS. Annu Rev Biomed Data Sci. 2021;4:1–19.
Genomes Project C, Auton A, Brooks LD, Durbin RM, Garrison EP, Kang HM, et al. A global reference for human genetic variation. Nature. 2015;526(7571):68–74.
Li JZ, Absher DM, Tang H, Southwick AM, Casto AM, Ramachandran S, et al. Worldwide human relationships inferred from genome-wide patterns of variation. Science. 2008;319(5866):1100–4.
Rowczenio DM, Noor I, Gillmore JD, Lachmann HJ, Whelan C, Hawkins PN, et al. Online registry for mutations in hereditary amyloidosis including nomenclature recommendations. Hum Mutat. 2014;35(9):E2403–12.
Di Stefano V, Lupica A, Alonge P, Pignolo A, Augello SM, Gentile F, et al. Genetic screening for hereditary transthyretin amyloidosis with polyneuropathy in western Sicily: two years of experience in a neurological clinic. Eur J Neurol. 2024;31(1):e16065.
Landrum MJ, Kattman BL. ClinVar at five years: delivering on the promise. Hum Mutat. 2018;39(11):1623–30.
Richards S, Aziz N, Bale S, Bick D, Das S, Gastier-Foster J, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and genomics and the association for molecular pathology. Genet Med. 2015;17(5):405–24.
Karczewski KJ, Francioli LC, Tiao G, Cummings BB, Alfoldi J, Wang Q, et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature. 2020;581(7809):434–43.
Ho D, Imai K, King G, Stuart EA. MatchIt: nonparametric preprocessing for parametric causal inference. J Stat Softw. 2011;42(8):1–28.
Li B, Leal SM. Methods for detecting associations with rare variants for common diseases: application to analysis of sequence data. Am J Hum Genet. 2008;83(3):311–21.
Willer CJ, Li Y, Abecasis GR. METAL: fast and efficient meta-analysis of genomewide association scans. Bioinformatics. 2010;26(17):2190–1.
Nam Y, Jung SH, Yun JS, Sriram V, Singhal P, Byrska-Bishop M et al. Discovering comorbid diseases using an inter-disease interactivity network based on biobank-scale PheWAS data. Bioinformatics. 2023;39(1).
Mazzarotto F, Argiro A, Zampieri M, Magri C, Giotti I, Boschi B, et al. Investigation on the high recurrence of the ATTRv-causing transthyretin variant Val142Ile in central Italy. Eur J Hum Genet. 2023;31(5):541–7.
Batra J, Rosenblum H, Cappelli F, Zampieri M, Olivotto I, Griffin JM, et al. Racial differences in Val122Ile-associated transthyretin cardiac amyloidosis. J Card Fail. 2022;28(6):950–9.
Damrauer SM, Chaudhary K, Cho JH, Liang LW, Argulian E, Chan L, et al. Association of the V122I hereditary transthyretin amyloidosis genetic variant with heart failure among individuals of African or Hispanic/Latino ancestry. JAMA. 2019;322(22):2191–202.
Abouelhoda M, Mohty D, Alayary I, Meyer BF, Arold ST, Fadel BM, et al. Established and candidate transthyretin amyloidosis variants identified in the Saudi population by data mining. Hum Genomics. 2021;15(1):52.
Mohan B, Singh S, Tandon R, Batta A, Singal G, Singh G, et al. Clinical profile of patients with cardiac amyloidosis in India. Indian Heart J. 2023;75(1):73–6.
Ruberg FL, Grogan M, Hanna M, Kelly JW, Maurer MS. Transthyretin amyloid cardiomyopathy: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(22):2872–91.
Chandrashekar P, Alhuneafat L, Mannello M, Al-Rashdan L, Kim MM, Dungu J, et al. Prevalence and outcomes of p.Val142Ile TTR amyloidosis cardiomyopathy: a systematic review. Circ Genom Precis Med. 2021;14(5):e003356.
De Silva K, Fife A, Murgatroyd F, Gall N. Pacemaker endocarditis: an important clinical entity. BMJ Case Rep. 2009;2009.
Briasoulis A, Kourek C, Papamichail A, Loritis K, Bampatsias D, Repasos E et al. Arrhythmias in patients with cardiac amyloidosis: a comprehensive review on clinical management and devices. J Cardiovasc Dev Dis. 2023;10(8).
Zampino S, Sheikh FH, Vaishnav J, Judge D, Pan B, Daniel A, et al. Phenotypes associated with the Val122Ile, Leu58His, and late-onset Val30Met variants in patients with hereditary transthyretin amyloidosis. Neurology. 2023;100(19):e2036–44.
Parker MM, Damrauer SM, Tcheandjieu C, Erbe D, Aldinc E, Hawkins PN, et al. Association of the transthyretin variant V122I with polyneuropathy among individuals of African ancestry. Sci Rep. 2021;11(1):11645.
Damy T, Kristen AV, Suhr OB, Maurer MS, Plante-Bordeneuve V, Yu CR, et al. Transthyretin cardiac amyloidosis in continental Western Europe: an insight through the transthyretin amyloidosis outcomes survey (THAOS). Eur Heart J. 2019;43(5):391–400.
Sperry BW, Reyes BA, Ikram A, Donnelly JP, Phelan D, Jaber WA, et al. Tenosynovial and cardiac amyloidosis in patients undergoing carpal tunnel release. J Am Coll Cardiol. 2018;72(17):2040–50.
Quarta CC, Solomon SD, Uraizee I, Kruger J, Longhi S, Ferlito M, et al. Left ventricular structure and function in transthyretin-related versus light-chain cardiac amyloidosis. Circulation. 2014;129(18):1840–9.
Kim DK, Joo KW. Hyponatremia in patients with neurologic disorders. Electrolyte Blood Press. 2009;7(2):51–7.
Butt EJ, Boyars MC. An unusual case of heart failure: sometimes when you hear hoof beats you should think of Zebras. Cureus. 2021;13(12):e20801.
Ye F, Pu M, Rodriguez C, Callahan K, Seals A, Vasu S, et al. Risk factors associated with one year mortality from the time of cardiac amyloid diagnosis. J Heart Lung Transplantation. 2022;41(4):S218–9.
Baumgart JV, Stuhlmann-Laeisz C, Hegenbart U, Nattenmuller J, Schonland S, Kruger S, et al. Local vs. systemic pulmonary amyloidosis-impact on diagnostics and clinical management. Virchows Arch. 2018;473(5):627–37.
Berk JL. Pleuropulmonary manifestations of amyloidosis. UpToDate [September 29, 2023]. Available from: https://www.uptodate.com/contents/pleuropulmonary-manifestations-of-amyloidosis#
Donnellan E, Wazni OM, Saliba WI, Hanna M, Kanj M, Patel DR, et al. Prevalence, incidence, and impact on mortality of conduction system disease in transthyretin cardiac amyloidosis. Am J Cardiol. 2020;128:140–6.
Skare J, Jones LA, Myles N, Kane K, Milunsky A, Cohen A, et al. Two transthyretin mutations (glu42gly, his90asn) in an Italian family with amyloidosis. Clin Genet. 1994;45(6):281–4.
Skare JC, Milunsky JM, Milunsky A, Skare IB, Cohen AS, Skinner M. A new transthyretin variant from a patient with familial amyloidotic polyneuropathy has asparagine substituted for histidine at position 90. Clin Genet. 1991;39(1):6–12.
Skare JC, Saraiva MJ, Alves IL, Skare IB, Milunsky A, Cohen AS, et al. A new mutation causing familial amyloidotic polyneuropathy. Biochem Biophys Res Commun. 1989;164(3):1240–6.
Trachtenberg BH, Jimenez J, Morris AA, Kransdorf E, Owens A, Fishbein DP, et al. TTR variants in patients with dilated cardiomyopathy: an investigation of the DCM precision medicine study. Genet Med. 2022;24(7):1495–502.
Morales A, Kinnamon DD, Jordan E, Platt J, Vatta M, Dorschner MO, et al. Variant interpretation for dilated cardiomyopathy: refinement of the American College of Medical Genetics and Genomics/ClinGen guidelines for the DCM precision medicine study. Circ Genom Precis Med. 2020;13(2):e002480.
Lanoue J, Wei N, Gorevic P, Phelps RG. Cutaneous manifestations of familial transthyretin amyloid polyneuropathy. Am J Dermatopathol. 2016;38(10):719–25.
Ebenezer GJ, Liu Y, Judge DP, Cunningham K, Truelove S, Carter ND, et al. Cutaneous nerve biomarkers in transthyretin familial amyloid polyneuropathy. Ann Neurol. 2017;82(1):44–56.
Lee CC, Ding X, Zhao T, Wu L, Perkins S, Du H, et al. Transthyretin stimulates tumor growth through regulation of tumor, immune, and endothelial cells. J Immunol. 2019;202(3):991–1002.
Sharma S, Malhotra L, Mukherjee P, Kaur N, Krishanlata T, Srikanth CV, et al. Putative interactions between transthyretin and endosulfan II and its relevance in breast cancer. Int J Biol Macromol. 2023;235:123670.
Shimura T, Shibata M, Gonda K, Okayama H, Saito M, Momma T, et al. Serum transthyretin level is associated with prognosis of patients with gastric cancer. J Surg Res. 2018;227:145–50.
Ke K, Lin J, Huang N, Yan L, Liao R, Yang W. Transthyretin promotes the invasion of combined hepatocellular cholangiocarcinoma by tumor-associated macrophages. Cancer Rep (Hoboken). 2023:e1888.
Picken MM. The pathology of amyloidosis in classification: a review. Acta Haematol. 2020;143(4):322–34.
Gertz M, Adams D, Ando Y, Beirao JM, Bokhari S, Coelho T, et al. Avoiding misdiagnosis: expert consensus recommendations for the suspicion and diagnosis of transthyretin amyloidosis for the general practitioner. BMC Fam Pract. 2020;21(1):198.
Acknowledgements
The authors thank participants and investigators involved in the UK Biobank.
Funding
This study was supported by a grant from the Transthyretin Amyloid Polyneuropathy (ATTR-PN) Research Competitive Program for Junior Investigators from Pfizer Inc. to ADL. Pfizer Inc. had no role in the study design, data analysis, and data interpretation of the present study. FDA acknowledges support from the project: MNESYS—a multiscale integrated approach to the study of the nervous system in health and disease (PNRR).
Author information
Authors and Affiliations
Contributions
ADL and RP conceived the study design; ADL performed the analyses. All authors contributed to data interpretation; ADL and RP drafted the original manuscript. All authors critically evaluated and revised the manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was approved under protocol 227/20 by the Comitato Etico Indipendente, Fondazione Policlinico Tor Vergata—Rome, Italy. This research was performed using the UKB Resource under the application 58146.
Consent for publication
Not Applicable.
Competing interests
ADL received a grant from Pfizer. The other authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
De Lillo, A., Pathak, G.A., Low, A. et al. Clinical spectrum of Transthyretin amyloidogenic mutations among diverse population origins. Hum Genomics 18, 31 (2024). https://doi.org/10.1186/s40246-024-00596-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40246-024-00596-7