
Abstract
In recent years, large scale genomics and genome-wide studies using comprehensive genomic tools have reshaped our understanding of cancer evolution and heterogeneity. Hepatocellular carcinoma, being one of the most deadly cancers in the world has been well established as a disease of the genome that harbours a multitude of genetic and epigenetic aberrations during the process of liver carcinogenesis. As such, in depth understanding of the cancer epigenetics in cancer specimens and biopsy can be useful in clinical settings for molecular subclassification, prognosis, and prediction of therapeutic responses. In this review, we present a concise discussion on recent progress in the field of liver cancer epigenetics and some of the current works that contribute to the progress of liver cancer therapeutics.
Similar content being viewed by others

Liver cancer—hepatocellular carcinoma (HCC)
Liver cancer is the second most lethal cancer worldwide [1]. Liver cancer presents an important public health issue in many countries due to its highly aggressive nature and poor survival rate. Hepatocellular carcinoma (HCC) is the most prevalent form of the primary liver cancer and accounts for up to 90% of all cases. The incidence rates for HCC is rising in many countries due to increasing associated risks factors such as diabetes and obesity [2]. Other well-recognized risk factors for HCC includes chronic hepatitis B or C infection, exposure to dietary aflatoxin, alcohol-induced cirrhosis and smoking.
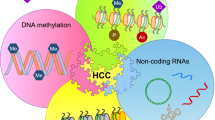
Deregulation of gene expression and aberrant molecular signalling confer survival advantages to cancer cells and are key hallmarks of cancer. Recently, it has been shown that undesirable changes in epigenetic alterations may enhance the selective advantage of cancer cells [3]. The reason why it is important to study epigenetics in the liver is due to the fact that it is the one of the organs that is constantly adapting to highly variable environmental conditions. The liver constantly adapts to circadian cues, metabolic processes, changes in the microbiota, and external factors such as viral infections and xenobiotics which results in the need for its constant repair and regeneration [4]. Therefore, the liver epigenome is extremely sensitive to its highly variable environment. As such, metabolic risk factors such as obesity, excessive alcohol consumption and insults from viral hepatitis cause a disturbance in the hepatic epigenome. Alterations of the epigenome such as DNA methylation, chromatin modification, miRNAs, and lncRNAs propels uncontrolled cell growth and proliferation, invasion and metastasis as well as the progression of liver cancer from chronic inflammation, fibrosis, subsequent accumulation of mutations and consequently, liver cancer [4,5,6].
With the advancement of next generation DNA sequencing, our understanding of the genetic and molecular pathobiology of liver cancer has increased dramatically. Large international efforts have been initiated to provide researchers with comprehensive genomic/epigenomic data publicly. Two of the well-known large public cancer genomic databases include the international cancer genome consortium (ICGC; http://www.icgc.org) and the cancer genome atlas (TCGA; https://cancergenome.nih.gov/). Both public databases aim to generate a comprehensive information of genomic abnormalities in cancer such as somatic mutations, aberration expression of genes and epigenetic modifications that will be made publicly available to the research community. Another initiative launched in 2010 is the international human epigenome consortium (IHEC; http://ihec-epigenomes.org) with the goal of generating comprehensive reference maps of human epigenomes for key cellular states such as stemness, differentiation, proliferation, stress, senescence, and others relevant to human health and disease. With these multiple platforms of public databases and others, the understanding of epigenetic programming implicated in cancers and the prevention and treatment of these cancers will be greatly improved.
DNA methylation and HCC
DNA methylation is a process whereby DNA methyltransferases (DNMTs) transfer methyl groups from S-adenosyl methionine to cytosine bases of CpG dinucleotides at gene promoters and regulatory regions [7]. DNA methylation commonly occurs at the CpG dinucleotides in somatic cells with about 25% occurring in a non-CpG manner in embryonic stem cells (ESCs). CpG dinucleotides are commonly found in “CpG islands”, which are short CpG-rich regions. CpG islands, which occupy more than 50% of all promoters, can be methylated during development and promotes long-term gene silencing such as in the case of X-chromosomal inactivation and the imprinted genes. CpG shores are defined commonly as regions of low CpG density that are located within 2 kb up- and downstream of a CpG island (Fig. 1). CpG shelves refer to a region 2 kb outside of CpG shores, while regions with low methylation and are uncharacterized are known as CpG oceans. DNA methylation is tightly regulated by a family of DNMTs that consists of DNMT1, DNMT2, DNMT3A, DNMT3B and DNMT3L [8, 9]. DNMT1 has been proposed to be the maintenance methyltransferase that preferentially methylates hemi-methylated DNA over non-methylated DNA to maintain the original DNA methylation pattern during replication [10, 11]. DNMT3A and DNMT3B, on the other hand, are more likely to perform de novo methylation on unmethylated CpG dinucleotides during the developmental process [12]. In addition, cooperation of several DNMTs are also required to methylate certain regions of the genome, specifically the repetitive elements.

Schematic diagram displaying CpG annotations of genomic regions
Dysregulated DNA methylation is commonly observed in many cancers including HCC [13]. The earliest indications that provide a link between epigenetics and cancer came from studies that correlate gene expression data and DNA methylation. Epigenetic changes such as global hypomethylation and specific gene promoter hypermethylation (Fig. 2) have been demonstrated to be involved in genome instability and tumor suppressor gene silencing respectively [14]. In HCC, dysregulated DNA methylation is one of the early events in HCC pathogenesis and plays an important role in elevating chromosomal instability [15]. Table 1 summarizes a list of DNA methylation studies in HCC.

DNA methylation profile in cancer. Liver cancer cells typically exhibit DNA hypermethylation at promoter sites of tumor suppressor genes, resulting in silencing of these tumor suppressive genes
Aberrant hypermethylation of genes associated with HCC progression has been identified via several sequencing techniques. In an earlier study, Tao et al. performed a global methylation profile of single hepatocyte cells derived from hepatitis B positive HCC (HBHC) samples using Illumina Infinium Human Methylation27 BeadChips with combined bisulfite restriction analysis (COBRA) and bisulfite sequencing [16]. They found seven novel genes (EMILIN2, WNK2, TM6SF1, TLX3, HIST1H4F, TRIM58 and GRASP) that were significantly methylated in HBHC but were hypomethylated in their respective paired adjacent tissues. These novel aberrant methylated genes could potentially be novel biomarkers for HCC once validated in larger clinical cohorts. In another similar study on predominantly HBHC samples, differentially methylated genes were identified using the Illumina Infinium Human Methylation27 in 62 paired HCC tumors and their adjacent non-tumor tissues [17]. Shen et al. demonstrated that the panel of methylated genes identified in HCC can be used as potential HCC-specific biomarkers of plasma DNA for early diagnosis of HCC. They showed that DNA methylation measurement in HCC patients’ plasma is feasible, with at least one of the genes from the panel being hypermethylated in 87% of the cases, thus supporting the utility of this panel of methylated genes as early biomarkers of HCC.
In a larger genome-wide methylation study conducted by Song et al. using the Methylation450 BeadChip, significant differential DNA methylation patterns in the CpG islands were observed in HCC as compared to their normal adjacent tissues [18]. Specifically, they found that global hypomethylation was observed in HCC and promoter CpG islands exhibited higher frequency of hypermethylation events than the regions surrounding the CpG islands, i.e. the CpG shores and the CpG shelves. To identify tumor suppressor genes in HCC, Revill et al. conducted a genome-wide methylation analysis of 71 human HCC specimens with microarray data analysis of gene re-expression in four HCC cancer cell lines and performed epigenetic unmasking by exposing the cells to reagents that induced reverse DNA methylation [19]. The authors identified 13 tumor suppressor genes, of which two (neurofilament heavy polypeptide, NEFH and sphingomyelin phosphodiesterase 3, SMPD3) were functionally validated in vivo.
A study by Shen et al. focused on the genome-wide DNA methylation profiles of hepatitis C virus (HCV)-related HCC tumors using the Infinium HumanMethylation 450K BeadChip arrays [20]. Consistent with previous findings, they observed higher percentage (79%) of hypomethylated CpG sites than hypermethylated sites (21%). In addition, hypermethylated CpG sites were more commonly found at the CpG islands and shores in contrast to the hypomethylated CpG sites that occurred mainly in the open sea region. More importantly, the authors were able to identify 228 aberrantly methylated CpG sites covering a total of 147 genes that had strong associations with HCV infection. Interestingly, there were no overlapping CpG sites in both HCV and HCC, signifying that HCV-associated methylated CpG sites are independent to HCC development. In another genome-wide DNA methylation profile study of 69 paired HCC tumor and adjacent normal liver tissues, Gentilini et al. used a different approach to identify epigenetic markers using epigenetic mutation analysis [21, 22] instead of using p-value or effect size [17, 18]. A gradual increase in the number of stochastic epigenetic mutations (SEMs) from normal liver, peritumoral tissues to HCC tissues was observed, with HCC tissues having 13-folds higher median SEMs than normal liver tissues. In addition, a list of novel potential epidrivers were identified by analysing genomic position of SEMs in both HCC and peritumoral tissues. These epigenes include AJAP1, ADARB2, PTPRN2, and SDK1.
A recent large scale epigenomic landscape study on 373 liver cancer specimens reported the correlation between epigenetic features and genetic aberrations using whole-genome bisulfite, whole-genome shotgun, long read and virus-capture sequencing [23]. Using a comprehensive genome and methylome sequencing approach, the authors identified two epigenetically distinct genomic regions in which somatic genetic aberrations were enriched—a region that is tumor specific hypomethylated and displayed an inactive chromatin genome, and the other region is an actively transcribing region with a highly methylated gene body area that is vulnerable to genetic insults and in part positively selected during carcinogenesis. In addition, this study also assessed whether the methylation status is associated with the distribution of somatic mutations by examining the correlation between somatic mutation density and methylation level. They showed that somatic mutations may occur preferentially in highly methylated regions of the non-cancerous liver genome, indicating that chromatin status may regulate the frequency of somatic mutations in liver cancer genome. Their integrative analysis provided evidence of interdependency between genetic, viral, and epigenetic alterations in liver cancer.
ncRNAs and HCC
Noncoding RNAs (ncRNAs) can be categorized into two main subgroups according to their lengths [24]. Small or short noncoding RNAs include endogenous siRNAs and miRNAs that are less than 200 nucleotides. Long noncoding RNAs (lncRNAs) usually refer to RNAs more than 200 nucleotides in length. MicroRNAs (miRNAs), on the other hand, are small, noncoding RNAs of 18 to 25 bases in length that regulate post-transcriptional gene expression. In addition, the human genome has been reported to encode more than 1000 different miRNAs, each with distinct mRNA target(s). Hence, miRNAs represent a group of important epigenetic regulators that influence biological responses.
miRNAs are by far the most well-studied class of epigenetic regulators in liver cancer (Table 2). The first report of miRNA dysregulation in liver cancer is from Murakami et al. who reported the abnormal expression pattern of four miRNAs to be associated with HCC differentiation, namely miR-20, miR-92, miR-18 and precursor miR-18 [25]. Subsequently, numerous reports on miRNA dysregulation have been reported in HCC. Some of the consistently reported miRNAs that are differentially expressed in HCC tumors compared to normal liver tissues are miR-21, miR-26, miR-122, miR-199a, miR-200a, miR-221, miR-222, and miR-224 (Fig. 3).

MicroRNAs in cancer. Elevation of oncogenic miRNAs (oncomiRs) results in silencing of tumor suppressor genes while downregulation of tumor suppressor miRNAs leads to reduced inhibition of oncogenes, consequently lead to the development of liver cancer
Oncogenic miRNA that drives progression of HCC such as miR-21, miR-221, miR-222 and miR-224 are frequently found to be upregulated in HCC. For instance, miR-21 was found to be upregulated in HCC and inhibition of miR-21 resulted in a marked elevated expression of the tumor suppressor phosphatase and tensin homolog (PTEN) with accompanied reduction in tumor cell proliferation, migratory and invasive ability [26]. Furthermore, mitogen-activated protein kinase-kinase 3 (MAP2K3) was observed to be a direct target of miR-21 whereby MAP2K3 expression, which was repressed in HCC tissues, was observed to be inversely correlated with miR-21 [27]. miR-221 and miR-222 have been shown to be overexpressed in HCC and the elevated levels of these two miRNAs are correlated with PTEN and TIMP3 downregulation [28]. In addition, Pineau et al. showed that miR-221/222 upregulation is an early event and have the highest elevated expression in HCC samples. It has been shown to target CDK inhibitor p27 to induce tumor proliferation and its overexpression is correlated with poorer prognosis [29, 30]. miR-224 is another commonly upregulated HCC-specific miRNA. miRNA-224 has been shown to promote proliferation, inhibit apoptosis, migration and invasion of HCC tumor cells [31, 32]. More importantly, miRNA overexpression has been found to correlate with poorer survival in HCC patients [33]. Furthermore, early HCC patients showed upregulated levels of serum miR-224 as compared to those with liver cirrhosis, chronic hepatitis B and healthy control subjects, highlighting the potential of miR-224 as a reliable serum biomarker for early HCC detection [34].
Tumor suppressive miRNAs are usually silenced in human liver cancers and these include miR-26, miR-122, miR-199a and miR-200a. miR-26 has been shown to be downregulated in HCC and could directly repress the expression of CDK6 and cyclin E1, which induced a decreased in the phosphorylation of retinoblastoma protein (pRb) [35]. More recently, miR-26 was observed to play a crucial role in tumor angiogenesis [36]. Specifically, downregulation of miR-26 correlated with enhanced angiogenic potential of HCC and gain-of-function studies showed that miR-26 was able to inhibit expression of vascular endothelial growth factor A (VEGFA) which subsequently suppressed tumor promoting properties of HCC cells such as proliferation, migration and in vivo tumor angiogenesis. miR-122 is the most abundant miRNA that accounts for 70% of the total miRNA population in the liver [37]. miR-122 expression has been frequently found to be repressed in HCC [38, 39] and is an important marker for hepatocyte-specific differentiation [40, 41]. Importantly, reduced miR-122 expression is correlated to a subset of HCC tumors with bad prognosis [42]. In addition, loss of miR-122 resulted in increased cell migratory and invasive phenotype. Since miR-122 correlates with several clinical parameters such as tumor size and invasiveness, it presents an attractive therapeutic target for HCC intervention [42,43,44]. miR199 is another abundantly expressed miRNA in the normal liver tissue that is downregulated in HCC. In particular, miR-199a-3p and miR-199a-5p are frequently found to be repressed in human HCC tissues [45, 46]. Furthermore, low miR-199a-3p expression is observed to be strongly correlated with reduced survival of HCC patients [47]. miR-199a/b-3p has been found to target the HCC tumor-promoting PAK4 by repression of PAK4/Raf/MEK/ERK pathway both in vitro and in vivo, suggesting that miR-199a/b-3p could be a potential therapeutic option for HCC [47]. Chen et al. reported that the decreased miR-200a expression in HCC could lead to abnormal cell growth, migration and invasion via the regulation of its target, transcription factor forkhead box A2 (Foxa2) [48]. Furthermore, lower miR-200a expression also enhanced the side population (SP) of HCC tumors to metastasize via transactivation of ZEB2 expression and the subsequent epithelial-mesenchymal-transition (EMT) activation in HCC tumor cells [49]. The major challenge for the use of miRNAs will be the targeted delivery and control of expression of these therapeutic miRNAs. With greater understanding of the roles and biology of miRNAs and the integration of current emerging delivery advances, miRNAs could represent an attractive alternative therapeutic treatment for HCC.
lncRNAs are also important modulators of HCC progression (Table 2). Due to the advances in genomic techniques, the role of lncRNAs as central regulators in genome regulation and dynamics has begun to emerge. Some of the known lncRNAs implicated in HCC are HULC, HOTAIR, MEG3 and HOTTIP. HULC (highly up-regulated in liver cancer) was described by Panzitt et al. using HCC specific gene libraries and cDNA microarrays [50]. HULC is an oncogenic lncRNA approximately 1.6 kb in length and is highly upregulated in human HCCs. The upregulation of HULC is associated with tumor proliferation and is effected via downregulation of the p18 tumor suppressor. Additionally, the upregulation and stability of HULC is enhanced post-transcriptionally by IGF2 mRNA-binding protein 1 (IGF2BP1) [51]. Importantly, it has been shown that HULC is the first substrate to be destabilized by IGF2BP1, with CNOT1 protein as a crucial interacting partner. HULC is also known to act as a sponge to sequester miRNAs. Wang et al. showed that HULC inhibits and downregulates miR-372, leading to reduced translational repression of its target gene PRKACB, which is able to phosphorylate and activate cAMP response element binding protein (CREB), a key transcription factor in promoting proliferation and cellular adaptive responses [52]. Therefore, upregulation of HULC can lead to HCC progression by indirect activation of CREB transcription factor. Other miRNAs such as miR-107 and miR-200a-3p have also been shown to be sequestered by HULC and could subsequently lead to angiogenesis and EMT activation in HCC [53, 54]. HOTAIR (hox transcript antisense intergenic RNA) is an intergenic lncRNA of approximately 2.2 kb in length that has been implicated in multiple solid cancers such as breast, colorectal, pancreatic and HCC. In HCC, HOTAIR has been demonstrated to be overexpressed and is able to interact and recruit polycomb group complex 2 (PRC2) and lysine specific demethylase 1 (LSD1) complexes to mediate specific gene silencing via histone 3 lysine 27 trimethylation (H3K27me3) repressive marks [55, 56]. Depletion of HOTAIR has also been shown to reduce HCC proliferation, suggesting its role in promoting tumor cell growth [57]. More importantly, suppression of HOTAIR in HCC cells sensitizes them to chemotherapeutic treatments such as doxorubicin and cisplatin, suggesting HOTAIR to be a biomarker of HCC tumor recurrence [58]. More recently, HOTAIR has been implicated in maintaining HCC tumor microenvironment via HOTAIR-induced C–C motif chemokine ligand 2 (CCL2) expression [59]. It was shown that CCL2 is a downstream target of HOTAIR and is involved in the recruitment of myeloid-derived suppressor cells (MDSCs) and macrophages to the tumor microenvironment.
Chromatin modifiers and HCC
Chromatin modifiers or remodelers are an important class of proteins that take part in the regulation of accessibility to chromatin and positioning of nucleosome in the DNA [60]. Some of the well-studied chromatin modifiers in HCC include enhancer of zeste homologue 2 (EZH2), AT-Rich Interaction Domain 1A (ARID1A) and AT-rich interactive domain 2 (ARID2). EZH2, a methyltransferase belonging to the Polycomb Repressive Complex 2 (PRC2) which mediates gene silencing via H3K27me3, is frequently upregulated in HCC. It has been shown that depletion of EZH2 in HCC cells effectively reduced growth of HCC tumors and tumorigenicity in vivo [61]. More importantly, high expression levels of EZH2 is strongly associated with increased aggressiveness and metastatic properties along with poorer prognosis in HCC patients. In addition, EZH2 overexpression repressed miR-622 by enhanced H3K27 trimethylation, and is correlated with upregulation of CXCR4 and unfavourable prognosis in HCC patients [62]. More recently, EZH2 inhibition was found to facilitate natural killer (NK) cell-mediated cancer cell eradication through re-expression of NK cell ligands in HCC cells, suggesting the use of EZH2 inhibitors in rendering HCC cells more susceptible to NK-mediated cytotoxicity [63].
ARID1A and ARID2 are frequently found to be mutated in a subset of HCC patients [64, 65]. Both proteins belong to the SWItch/Sucrose Non-Fermentable (SWI/SNF) chromatin remodeling complexes and aid in regulating the accessibility of promoters to the transcriptional machinery. ARID1A encodes for BAF250a subunit of the SWI/SNF complex and has been shown to be a bona fide tumor suppressor based on several mutational and functional studies [66]. However, a recent study by Sun et al. described ARID1A as having both oncogenic and tumor suppressive roles that were context-dependent in HCC development and metastasis [67]. Specifically, the authors showed that while ARID1A supports initial HCC development, ARID1A loss after tumor establishment further accelerates and increases metastatic potential of HCC, suggesting the importance of protein subunit dosage in the proper regulation of global transcription. ARID2 belongs to the polybromo-associated BRG1-associated factor (PBAF) complex that can activate ligand-mediated transcription via nuclear receptors. ARID2 knockout studies showed that ARID2 is required for proper nucleotide excision repair (NER) of DNA damage induced by UV and cancer-causing compounds in HCC [68]. In addition, restoring ARID2 expression in hepatoma cells suppressed cell growth and tumor progression in mice while ARID2 inhibition resulted in upregulation of cell cycle proteins such as cyclin D1 and cyclin E1, suggesting a tumor suppressive role for ARID2 in HCC [69].
Histone deacetylation and HCC
Besides DNA methylation, ncRNAs and chromatin remodelers, histone modifications comprise another group of epigenetic mechanisms that play important roles in regulating gene expression and changes in chromatin structure. DNA is packed into chromatin with the help of histone protein octamers, and the amino acid residues on the histone tails that protrude from these nucleosome cores are subjected to various post-translational modifications, which includes acetylation, methylation, phosphorylation and ubiquitination [70]. These modifications affect the affinity of DNA binding to histones and are thus important for the regulation of gene transcription and expression [71]. For the purpose of this review, we chose to focus our discussion on histone deacetylases (HDACs) due to the many successful preclinical and clinical efficacies of using HDAC inhibitors in cancer. Readers can refer to other reviews for more in depth discussion on histone modifications and their implications in cancer [5, 72, 73].
Histone acetylation is a process that is regulated by two groups of enzymes with opposing functions: histone acetyltransferases (HATs), which add acetyl moieties to lysine residues, and HDACs that catalyse the removal of these acetyl groups [74]. Acetylation removes the positive charge of lysine residues, weakening the interaction of histones with negatively-charged DNA, which leads to a transcriptionally active chromatin state. In contrast, the removal of acetyl groups promotes a closed chromatin state by maintaining the strong interaction of DNA with positively-charged histones [75]. The dynamic balance between HAT and HDAC activity is critical in maintaining normal gene expression and this balance is often lost in various diseases including HCC [76].
The dysregulated expression of HDACs in HCC have been reported in several studies. Wu et al. discovered that overexpression of HDAC3 was an independent prognostic factor of tumor recurrence after liver transplantation in HBV-associated HCC patients [77]. HDAC3 also appeared to have functional roles in promoting tumor cell proliferation and invasion in vitro, indicating the potential for HDAC3 to serve as a biomarker and therapeutic target for HBV-associated HCC [77].
Besides, HDAC1 and HDAC2 have also been found to be upregulated in a cohort of Southeast Asian HCC patients, and are correlated with increased mortality [78]. The authors further demonstrated that inhibition of HDAC1/2 was able to suppress proliferation and induce tumor cell death in several HCC cell lines. Mechanistically, Yang et al. observed that upregulation of HDAC1 and HDAC2 suppresses the expression of a key metabolic enzyme in glucose metabolism, fructose-1,6-bisphosphatase (FBP1), resulting in increased lactate production in liver cancer cells [79]. The authors also showed that restoring FBP1 expression via HDAC inhibition was able to inhibit tumor cell growth in vitro and in vivo. In addition, HDAC2 knockdown transcriptomic studies revealed that HDAC2 dysregulation contributes to HCC pathogenesis by modulating expression of genes involved in apoptosis, cell cycle and lipid metabolism [80].
Epigenetic therapies in HCC
As various epigenetic mechanisms have been found to play significant roles in contributing to HCC pathogenesis, they have also become interesting/promising targets for cancer therapy. Here, we review the current development and progress of epigenetic therapies targeted against HCC, focusing on inhibitors of DNA methylation and histone acetylation as well as miRNA-based therapies. A summary of these HCC-specific epigenetic drugs and their clinical status can be found in Table 3.
DNA methylation inhibitors
Small molecule inhibitors of DNA methyltransferase (DNMT) were the earliest group of epigenetic drugs to be studied as an alternative approach to cancer treatment. In fact, azacytidine was the first epigenetic drug to be approved by the FDA in 2004 for the treatment of myelodysplastic syndrome (MDS). Since then, various DNMT inhibitors have been developed and tested against multiple cancer indications, including HCC, with promising preclinical results. Inhibitors of DNA methylation can be divided into two broad classes based on their mechanism—nucleoside analogues and non-nucleoside compounds. Many of the first generation DNMT inhibitors such as azacytidine (5-azacytidine) and decitabine (5-aza-2′-deoxycytidine) function as analogues of cytosine, and their incorporation into DNA prevents methylation by DNMTs.
Besides de-repressing silenced tumor suppressor genes, DNMT inhibitors can have other anti-cancer effects. A recent study by Gailhouste et al. demonstrated the ability of azacytidine in inducing hepatic cancer cell differentiation [81]. Using non-cytotoxic doses of azacytidine to achieve “epigenetic reconditioning”, the authors observed reduced tumor formation ability in mouse xenograft models and reported that azacytidine treatment sensitised the tumor cells to sorafenib, notably by converting the more drug-resistant liver progenitor-like cancer cells into mature hepatocytes. This study highlights the potential role of pre-treating liver cancer cells with DNMT inhibitors to recondition and prime these cells for more effective killing by other targeted or chemotherapeutic agents.
The use of DNMT inhibitors in sensitising HCC cells to sorafenib has also been reported in other studies. Liu et al. identified a possible mechanism of sorafenib resistance in HCC via the upregulation of NFκB/PDL1/STAT3/DNMT1 axis, leading to hypermethylation and silencing of tumor suppressor Cadherin 1 (CDH1) [82]. They showed that decitabine was able to re-sensitise resistant tumor cells to sorafenib and decreased colony formation ability. Due to the promising preclinical data, decitabine has been tested in various clinical trials for different indications. To mitigate the adverse events that accompany the usual dose of decitabine for treating solid tumors, two phase I/II trials have been conducted to examine the efficacy of using low-dose decitabine, alone or in combination with chemotherapy or adoptive immunotherapy [83, 84]. These trials demonstrated acceptable safety and toxicity profiles of low-dose decitabine in HCC, and the study by Fan et al. suggested the promising role of low-dose decitabine-based chemo-or immunotherapy in the treatment of cancer [84].
Despite the promising preclinical data, these DNMT inhibitors generally have short-half-lives due to metabolic inactivation by cytidine deaminase (highly expressed in the liver), which significantly reduces their efficacy in vivo [85]. Hence to overcome these limitations, second generation DNMT inhibitors have been developed, including guadecitabine (SGI-110). This compound was designed as a dinucleotide linking a deoxyguanosine with decitabine to enhance the stability of nucleoside analogues against degradation by cytidine deaminase [86]. In preclinical models, SGI-110 was able to suppress HCC progression and induce re-expression of tumor suppressor genes when used alone or in combination with sorafenib [87, 88]. This dinucleotide inhibitor recently completed phase II trials for advanced HCC patients who are refractory to sorafenib treatment and the results of its clinical efficacy are currently being awaited [89]. The ability of guadecitabine to prime HCC cells to other treatments has also been shown in a preclinical study by Kuang et al. [90]. Using HCC cell lines and mouse xenograft models, the authors demonstrated that pre-treatment with low-dose guadecitabine primed the tumor cells to oxaliplatin, resulting in enhanced cytotoxic and antiproliferative effects on tumor growth when compared to oxaliplatin treatment alone.
Histone deacetylation inhibitors
In many cancers, aberrant histone deacetylation, which results in deregulated gene silencing of important tumor suppressors, has emerged as a promising target for therapy. While several HDAC inhibitors have been approved by the FDA for treatment of haematological malignancies, the efficacy of these compounds in liver cancer is still being investigated, either pre-clinically or clinically.
Panobinostat is a pan-HDAC inhibitor that has been found to inhibit tumor cell proliferation, induce alternative pathways of apoptosis [91] and promote a more differentiated and less invasive phenotype in HCC cells [92]. In addition, alternative mechanisms of panobinostat activity have recently been discovered, including its ability to mediate anti-angiogenic effects via connective tissue growth factor (CTGF) pathway [93]. Moreover, panobinostat can affect cancer metabolism and tumor growth by restoring the expression of a key gluconeogenesis enzyme, fructose-1,6-bisphosphatase (FBP1), which is silenced by histone deacetylation in many cancers [79]. The clinical efficacy of panobinostat has been evaluated in several phase I trials as a combination therapy with sorafenib; however, no promising results were observed, and dose-limiting toxicities led to the termination of one such trial.
Another pan-HDAC inhibitor that has been shown to have antiproliferative and proapoptotic effects in HCC is belinostat [94]. In a phase I/II clinical trial that evaluated belinostat for the treatment of advanced unresectable HCC, the median PFS and OS were 2.64 and 6.6 months respectively, with 45.2% of patients achieving stable disease [95]. Interestingly, Yeo et al. also identified HR23B, a carrier protein involved in delivering ubiquitinated proteins to the proteasome, as a potentially useful biomarker for predicting response to HDAC inhibitors. Recently, a phase I/II trial of resminostat was conducted on advanced HCC patients who progressed with sorafenib to compare the efficacy of resminostat as a single treatment and in combination with sorafenib. The results from the study indicated poor efficacy of resminostat alone but showed that the HDAC inhibitor could restore sensitivity to sorafenib [96]. The median time to progression (TTP) and overall survival (OS) for resminostat monotherapy were 1.8 and 4.1 months respectively, whereas the combination of resminostat and sorafenib prolonged the TTP and OS to 6.5 and 8.0 months respectively [96].
Mechanistically, Fu et al. demonstrated that the cytotoxic effects of resminostat in HCC cell lines and patient-derived primary cells were dependent on activation of the mitochondrial apoptotic pathway [97]. In addition, the synergistic effects of resminostat and sorafenib were observed when addition of low dose resminostat enhanced sorafenib-induced mitochondrial apoptosis pathway [97]. These mechanisms were further investigated by Soukupova et al. recently, in which the authors postulated that changes in the epithelial-mesenchymal phenotype could be a sensitisation mechanism of HDAC inhibition [98]. They found that treatment of hepatic cancer cells with resminostat induced a more epithelial phenotype with less invasive and stem-like properties, which sensitised the cells to sorafenib-induced apoptosis [98].
As HDAC inhibitors have been shown to synergise or potentiate the effects of other anti-cancer therapies, there is great promise in using these drugs for combination therapy. Lai et al. adopted a similar approach but instead of using multiple drugs in combination, they designed a single small molecule inhibitor to work against various molecular targets [99]. CUDC-101 is novel compound that simultaneously targets HDAC along with epidermal growth factor receptor (EGFR) and human epidermal growth factor receptor 2 (HER2) [99]. The authors reported that CUDC-101 could effectively inhibit tumor cell growth and proliferation in vitro and in vivo, highlighting the potential of multi-targeted inhibitors as a new paradigm for the treatment of heterogenous and drug-resistant tumors. Subsequently, the safety of CUDC-101 was assessed in a phase Ib (expansion) study, and it was found to be well-tolerated in patients with advanced solid tumors including liver cancer, with early evidence of antitumor activity [100].
RNA-based epigenetic therapy
Various microRNAs (miRNAs) which are involved in regulating or being regulated by epigenetic processes have also been implicated in process of hepatic tumorigenesis, making them rational targets for miRNA-based strategies in epigenetic therapy. Several studies have established the therapeutic value of targeting aberrantly upregulated miRNAs in cancer, and miRNA inhibition can be achieved via several methods, including miRNA antisense oligonucleotides (AMOs) and miRNA sponges. Callegari et al. demonstrated that delivery of anti-miR-221 AMOs could reverse the tumorigenic effects of miR-221 in a transgenic mouse model [101]. To prolong the miRNA inhibition effects, Moshiri et al. devised an alternative approach using vector-encoded “miRNA sponges” [102]. These sponges contain several miR-221 antisense binding sites that can sequester miR-221 competitively, thus preventing its function. From the results of the study, miR-221 sponges were able to deplete endogenous miR-221 and its target genes as well as promote apoptosis in HCC cells [102]. While no tests have been conducted using miR-221 sponges in vivo yet, it would be interesting to examine the safety and efficacy of these sponges in a more clinically relevant setting for the treatment of HCC.
Another promising miRNA target for therapy is miR-122. In contrast to miR-221, miR-122 is found to act as a tumor suppressor in the liver [103, 104]. However, miR-122 levels do not always decrease in all cases of HCC and is dependent on the disease aetiology. For example, miR-122 has been found to be highly expressed in HCV-related HCC [105, 106], making it a relevant target for antiviral therapies aimed at impeding liver disease progression. Miravirsen is a locked nucleic acid (LNA)-modified antisense oligonucleotide that inhibits miR-122 by forming highly stable heteroduplexes with it [107]. In preclinical studies, miravirsen was able to sustain the suppression of HCV RNA levels in chronic HCV-infected chimpanzees, without evidence of resistance-conferring mutations developing in miR-122, and this was also observed in results from a phase IIa clinical trial [107, 108]. No dose-limiting adverse events were reported and miravirsen treatment was additionally found to reduce serum cholesterol levels, indicating possible relevance for use in fatty liver disease intervention [107]. The safety and efficacy of miravirsen were further evaluated by van der Ree et al. [109]. They reported that the 27 patients treated with miravirsen displayed no long-term safety issues after 35 months of follow-up, and these patients did not develop further liver diseases including HCV-related HCC [109]. In addition, miravirsen was shown to be highly specific for miR-122 as plasma levels of other miRNAs in patients treated with the inhibitor were unaffected [110].
Aside from miRNA inhibition, miRNAs can also be modulated by miRNA mimics, especially for tumor suppressive miRNAs that are often downregulated or suppressed in HCC. One such example is miR-185. Qadir et al. reported that modulating miR-185 expression using miRNA mimic oligonucleotides was able to suppress HCC cell growth and invasion [111]. They demonstrated that the tumor suppressive effects of miR-185 occurred via DNMT1 as overexpression of miR-185 depleted DNMT1, resulting in PTEN induction and subsequent inhibition of Akt. These promising preclinical data led the authors to propose miR-185 reactivation as a novel strategy for HCC treatment [111].
Conclusions
The liver cancer epigenome is highly complex and is adapted to changing environmental and developmental cues. While most of these epigenetic studies identified potential targets for therapeutic intervention in liver cancer, most studies lacked in-depth validations. The diversity of epigenetic alterations in different subsets of liver cancer is still poorly understood. Most studies focused on promoter hyper/hypo-methylation with lesser studies focusing on non-promoter or global histone modifications, non-coding RNAs, chromatin architecture and their integrated analysis. Since liver cancer is a highly heterogeneous disease, detailed analysis of epigenetic changes contributed by specific cell type in the bulk liver tumor should be carried out. Integration of laser capture microdissection, single cell analysis and flow cytometry cell sorting technologies could be incorporated with genome-wide studies in the future. With better understanding of how various epigenetic modifiers interact with one another to alter and maintain the epigenomic landscape, one can develop more clinically effective targeted epigenomic therapy for liver cancer.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A (2015) Global cancer statistics, 2012. CA A Cancer Journal for Clinicians 65:87–108
Bosch FX, Ribes J, Díaz M, Cléries R (2004) Primary liver cancer: Worldwide incidence and trends. Gastroenterology 127:S5–S16
Sadikovic B, Al-Romiah K, Squire JA, Zielenska M (2008) Cause and consequences of genetic and epigenetic alterations in human cancer. Current Genomics 9:394–408
Wilson CL, Mann DA, Borthwick LA (2017) Epigenetic reprogramming in liver fibrosis and cancer. Advanced Drug Delivery Reviews 121:124–132
Wahid B, Ali A, Rafique S, Idrees M (2017) New insights into the epigenetics of hepatocellular carcinoma. BioMed Research International 2017:1609575
Bhat V, Srinathan S, Pasini E, Angeli M, Chen E, Baciu C, Bhat M (2018) Epigenetic basis of hepatocellular carcinoma: A network-based integrative meta-analysis. World Journal of Hepatology 10:155–165
Stallcup MR (2001) Role of protein methylation in chromatin remodeling and transcriptional regulation. Oncogene 20:3014
Bestor TH (2000) The DNA methyltransferases of mammals. Human Molecular Genetics 9:2395–2402
Okano M, Xie S, Li E (1998) Cloning and characterization of a family of novel mammalian DNA (cytosine-5) methyltransferases. Nature Genetics 19:219
Probst AV, Dunleavy E, Almouzni G (2009) Epigenetic inheritance during the cell cycle. Nature Reviews Molecular Cell Biology 10:192
Song J, Teplova M, Ishibe-Murakami S, Patel DJ (2012) Structure-based mechanistic insights into DNMT1-mediated maintenance DNA methylation. Science 335:709–712
Okano M, Bell DW, Haber DA, Li E (1999) DNA methyltransferases Dnmt3a and Dnmt3b are essential for de novo methylation and mammalian development. Cell 99:247–257
Rakyan VK, Down TA, Balding DJ, Beck S (2011) Epigenome-wide association studies for common human diseases. Nature Reviews Genetics 12:529
Issa J-P (2004) CpG island methylator phenotype in cancer. Nature Reviews Cancer 4:988
Eden A, Gaudet F, Waghmare A, Jaenisch R (2003) Chromosomal instability and tumors promoted by DNA hypomethylation. Science 300:455
Tao R, Li J, Xin J, Wu J, Guo J, Zhang L, Jiang L et al (2011) Methylation profile of single hepatocytes derived from hepatitis B virus-related hepatocellular carcinoma. PLoS ONE 6:e19862
Shen J, Wang S, Zhang YJ, Kappil M, Wu HC, Kibriya MG, Wang Q et al (2012) Genome-wide DNA methylation profiles in hepatocellular carcinoma. Hepatology 55:1799–1808
Song M-A, Tiirikainen M, Kwee S, Okimoto G, Yu H, Wong LL (2013) Elucidating the landscape of aberrant DNA methylation in hepatocellular carcinoma. PLoS ONE 8:e55761
Revill K, Wang T, Lachenmayer A, Kojima K, Harrington A, Li J, Hoshida Y et al (2013) Genome-wide methylation analysis and epigenetic unmasking identify tumor suppressor genes in hepatocellular carcinoma. Gastroenterology 145(1424–1435):e1425
Shen J, Wang S, Zhang Y-J, Wu H-C, Kibriya MG, Jasmine F, Ahsan H et al (2013) Exploring genome-wide DNA methylation profiles altered in hepatocellular carcinoma using infinium humanmethylation 450 BeadChips. Epigenetics 8:34–43
Gentilini D, Garagnani P, Pisoni S, Bacalini MG, Calzari L, Mari D, Vitale G et al (2015) Stochastic epigenetic mutations (DNA methylation) increase exponentially in human aging and correlate with X chromosome inactivation skewing in females. Aging (Albany NY) 7:568
Gentilini D, Scala S, Gaudenzi G, Garagnani P, Capri M, Cescon M, Grazi GL et al (2017) Epigenome-wide association study in hepatocellular carcinoma: Identification of stochastic epigenetic mutations through an innovative statistical approach. Oncotarget 8:41890
Hama N, Totoki Y, Miura F, Tatsuno K, Saito-Adachi M, Nakamura H, Arai Y et al (2018) Epigenetic landscape influences the liver cancer genome architecture. Nature Communications 9:1643
Derrien T, Johnson R, Bussotti G, Tanzer A, Djebali S, Tilgner H, Guernec G et al (2012) The GENCODE v7 catalog of human long noncoding RNAs: Analysis of their gene structure, evolution, and expression. Genome Research 22:1775–1789
Murakami Y, Yasuda T, Saigo K, Urashima T, Toyoda H, Okanoue T, Shimotohno K (2006) Comprehensive analysis of microRNA expression patterns in hepatocellular carcinoma and non-tumorous tissues. Oncogene 25:2537
Meng F, Henson R, Wehbe-Janek H, Ghoshal K, Jacob ST, Patel T (2007) MicroRNA-21 regulates expression of the PTEN tumor suppressor gene in human hepatocellular cancer. Gastroenterology. 133:647–658
Xu G, Zhang Y, Wei J, Jia W, Ge Z, Zhang Z, Liu X (2013) MicroRNA-21 promotes hepatocellular carcinoma HepG2 cell proliferation through repression of mitogen-activated protein kinase-kinase 3. BMC Cancer 13:469
Garofalo M, Di Leva G, Romano G, Nuovo G, Suh S-S, Ngankeu A, Taccioli C et al (2009) miR-221&222 regulate TRAIL resistance and enhance tumorigenicity through PTEN and TIMP3 downregulation. Cancer Cell 16:498–509
Pineau P, Volinia S, McJunkin K, Marchio A, Battiston C, Terris B, Mazzaferro V et al (2010) miR-221 overexpression contributes to liver tumorigenesis. Proceedings of the National Academy of Sciences 107:264–269
Gramantieri L, Fornari F, Ferracin M, Veronese A, Sabbioni S, Calin GA, Grazi GL et al (2009) MicroRNA-221 targets Bmf in hepatocellular carcinoma and correlates with tumor multifocality. Clinical Cancer Research 15:5073–5081
Zhang Y, Takahashi S, Tasaka A, Yoshima T, Ochi H, Chayama K (2013) Involvement of microRNA-224 in cell proliferation, migration, invasion, and anti-apoptosis in hepatocellular carcinoma. Journal of Gastroenterology and Hepatology 28:565–575
Wang Y, Lee AT, Ma JZ, Wang J, Ren J, Yang Y, Tantoso E et al (2008) Profiling microRNA expression in hepatocellular carcinoma reveals microRNA-224 up-regulation and apoptosis inhibitor-5 as a microRNA-224-specific target. Journal of Biological Chemistry 283:13205–13215
Ladeiro Y, Couchy G, Balabaud C, Bioulac-Sage P, Pelletier L, Rebouissou S, Zucman-Rossi J (2008) MicroRNA profiling in hepatocellular tumors is associated with clinical features and oncogene/tumor suppressor gene mutations. Hepatology 47:1955–1963
Lin L, Lu B, Yu J, Liu W, Zhou A (2016) Serum miR-224 as a biomarker for detection of hepatocellular carcinoma at early stage. Clinics and Research in Hepatology and Gastroenterology 40:397–404
Zhu Y, Lu Y, Zhang Q, Liu J-J, Li T-J, Yang J-R, Zeng C et al (2011) MicroRNA-26a/b and their host genes cooperate to inhibit the G1/S transition by activating the pRb protein. Nucleic Acids Research 40:4615–4625
Yang X, Zhang XF, Lu X, Jia HL, Liang L, Dong QZ, Ye QH et al (2014) MicroRNA-26a suppresses angiogenesis in human hepatocellular carcinoma by targeting hepatocyte growth factor-cMet pathway. Hepatology 59:1874–1885
Lagos-Quintana M, Rauhut R, Yalcin A, Meyer J, Lendeckel W, Tuschl T (2002) Identification of tissue-specific microRNAs from mouse. Current Biology 12:735–739
Kutay H, Bai S, Datta J, Motiwala T, Pogribny I, Frankel W, Jacob ST et al (2006) Downregulation of miR-122 in the rodent and human hepatocellular carcinomas. Journal of Cellular Biochemistry 99:671–678
Girard M, Jacquemin E, Munnich A, Lyonnet S, Henrion-Caude A (2008) miR-122, a paradigm for the role of microRNAs in the liver. Journal of Hepatology 48:648–656
Tzur G, Levy A, Meiri E, Barad O, Spector Y, Bentwich Z, Mizrahi L et al (2008) MicroRNA expression patterns and function in endodermal differentiation of human embryonic stem cells. PLoS ONE 3:e3726
Chang J, Nicolas E, Marks D, Sander C, Lerro A, Buendia MA, Xu C et al (2004) miR-122, a mammalian liver-specific microRNA, is processed from hcr mRNA and maydownregulate the high affinity cationic amino acid transporter CAT-1. RNA Biology 1:106–113
Coulouarn C, Factor VM, Andersen JB, Durkin ME, Thorgeirsson SS (2009) Loss of miR-122 expression in liver cancer correlates with suppression of the hepatic phenotype and gain of metastatic properties. Oncogene 28:3526
Papaconstantinou I, Karakatsanis A, Gazouli M, Polymeneas G, Voros D (2012) The role of microRNAs in liver cancer. European Journal of Gastroenterology and Hepatology 24:223–228
Bai S, Nasser MW, Wang B, Hsu S-H, Datta J, Kutay H, Yadav A et al (2009) MicroRNA-122 inhibits tumorigenic properties of hepatocellular carcinoma cells and sensitizes these cells to sorafenib. Journal of Biological Chemistry 284:32015–32027
Fornari F, Milazzo M, Chieco P, Negrini M, Calin GA, Grazi GL, Pollutri D et al (2010) MiR-199a-3p regulates mTOR and c-Met to influence the doxorubicin sensitivity of human hepatocarcinoma cells. Cancer Research 70:5184–5193
Guo W, Qiu Z, Wang Z, Wang Q, Tan N, Chen T, Chen Z et al (2015) MiR-199a-5p is negatively associated with malignancies and regulates glycolysis and lactate production by targeting hexokinase 2 in liver cancer. Hepatology 62:1132–1144
Hou J, Lin L, Zhou W, Wang Z, Ding G, Dong Q, Qin L et al (2011) Identification of miRNomes in human liver and hepatocellular carcinoma reveals miR-199a/b-3p as therapeutic target for hepatocellular carcinoma. Cancer Cell 19:232–243
Chen S, Ma D, Chen Q, Zhang J, Tian Y, Wang Z, Cai H et al (2017) MicroRNA-200a inhibits cell growth and metastasis by targeting Foxa2 in hepatocellular carcinoma. Journal of Cancer. 8:617
Yang X, Wang J, Qu S, Zhang H, Ruan B, Gao Y, Ma B et al (2015) MicroRNA-200a suppresses metastatic potential of side population cells in human hepatocellular carcinoma by decreasing ZEB2. Oncotarget 6:7918
Panzitt K, Tschernatsch MM, Guelly C, Moustafa T, Stradner M, Strohmaier HM, Buck CR et al (2007) Characterization of HULC, a novel gene with striking up-regulation in hepatocellular carcinoma, as noncoding RNA. Gastroenterology 132:330–342
Hämmerle M, Gutschner T, Uckelmann H, Ozgur S, Fiskin E, Gross M, Skawran B et al (2013) Posttranscriptional destabilization of the liver-specific long noncoding RNA HULC by the IGF2 mRNA-binding protein 1 (IGF2BP1). Hepatology 58:1703–1712
Wang J, Liu X, Wu H, Ni P, Gu Z, Qiao Y, Chen N et al (2010) CREB up-regulates long non-coding RNA, HULC expression through interaction with microRNA-372 in liver cancer. Nucleic Acids Research 38:5366–5383
Lu Z, Xiao Z, Liu F, Cui M, Li W, Yang Z, Li J et al (2016) Long non-coding RNA HULC promotes tumor angiogenesis in liver cancer by up-regulating sphingosine kinase 1 (SPHK1). Oncotarget 7:241
Li S-P, Xu H-X, Yu Y, He J-D, Wang Z, Xu Y-J, Wang C-Y et al (2016) LncRNA HULC enhances epithelial-mesenchymal transition to promote tumorigenesis and metastasis of hepatocellular carcinoma via the miR-200a-3p/ZEB1 signaling pathway. Oncotarget 7:42431
Wu L, Murat P, Matak-Vinkovic D, Murrell A, Balasubramanian S (2013) Binding interactions between long noncoding RNA HOTAIR and PRC2 proteins. Biochemistry 52:9519–9527
Tsai M-C, Manor O, Wan Y, Mosammaparast N, Wang JK, Lan F, Shi Y et al (2010) Long noncoding RNA as modular scaffold of histone modification complexes. Science 329:689–693
Geng Y, Xie S, Li Q, Ma J, Wang G (2011) Large intervening non-coding RNA HOTAIR is associated with hepatocellular carcinoma progression. Journal of International Medical Research 39:2119–2128
Yang Z, Zhou L, Wu L-M, Lai M-C, Xie H-Y, Zhang F, Zheng S-S (2011) Overexpression of long non-coding RNA HOTAIR predicts tumor recurrence in hepatocellular carcinoma patients following liver transplantation. Annals of Surgical Oncology 18:1243–1250
Fujisaka Y, Iwata T, Tamai K, Nakamura M, Mochizuki M, Shibuya R, Yamaguchi K et al (2018) Long non-coding RNA HOTAIR up-regulates chemokine (C-C motif) ligand 2 and promotes proliferation of macrophages and myeloid-derived suppressor cells in hepatocellular carcinoma cell lines. Oncology Letters 15:509–514
Längst G, Manelyte L (2015) Chromatin remodelers: From function to dysfunction. Genes 6:299–324
Chen Y, Lin MC, Yao H, Wang H, Zhang AQ, Yu J, Hui CK et al (2007) Lentivirus-mediated RNA interference targeting enhancer of zeste homolog 2 inhibits hepatocellular carcinoma growth through down-regulation of stathmin. Hepatology. 46:200–208
Liu H, Liu Y, Liu W, Zhang W, Xu J (2015) EZH2-mediated loss of miR-622 determines CXCR62 activation in hepatocellular carcinoma. Nature Communications 6:8494
Bugide S, Green MR, Wajapeyee N (2018) Inhibition of Enhancer of zeste homolog 2 (EZH2) induces natural killer cell-mediated eradication of hepatocellular carcinoma cells. Proceedings of the National Academy of Sciences 115:E3509–E3518
Huang J, Deng Q, Wang Q, Li K-Y, Dai J-H, Li N, Zhu Z-D et al (2012) Exome sequencing of hepatitis B virus–associated hepatocellular carcinoma. Nature Genetics 44:1117
Guichard C, Amaddeo G, Imbeaud S, Ladeiro Y, Pelletier L, Maad IB, Calderaro J et al (2012) Integrated analysis of somatic mutations and focal copy-number changes identifies key genes and pathways in hepatocellular carcinoma. Nature Genetics 44:694
Wu JN, Roberts CW (2013) ARID1A mutations in cancer: Another epigenetic tumor suppressor? Cancer Discovery 3:35–43
Sun X, Wang SC, Wei Y, Luo X, Jia Y, Li L, Gopal P et al (2017) Arid1a has context-dependent oncogenic and tumor suppressor functions in liver cancer. Cancer Cell 32(574–589):e576
Oba A, Shimada S, Akiyama Y, Nishikawaji T, Mogushi K, Ito H, Matsumura S et al (2017) ARID2 modulates DNA damage response in human hepatocellular carcinoma cells. Journal of Hepatology 66:942–951
Duan Y, Tian L, Gao Q, Liang L, Zhang W, Yang Y, Zheng Y et al (2016) Chromatin remodeling gene ARID2 targets cyclin D1 and cyclin E1 to suppress hepatoma cell progression. Oncotarget 7:45863
Peterson CL, Laniel MA (2004) Histones and histone modifications. Current Biology 14:R546–R551
Cedar H, Bergman Y (2009) Linking DNA methylation and histone modification: Patterns and paradigms. Nature Reviews Genetics 10:295–304
Sawan C, Herceg Z (2010) Histone modifications and cancer. Advances in Genetics 70:57–85
Chervona Y, Costa M (2012) Histone modifications and cancer: Biomarkers of prognosis? American Journal of Cancer Research 2:589–597
Roth SY, Denu JM, Allis CD (2001) Histone acetyltransferases. Annual Review of Biochemistry 70:81–120
Ropero S, Esteller M (2007) The role of histone deacetylases (HDACs) in human cancer. Molecular Oncology 1:19–25
Haberland M, Montgomery RL, Olson EN (2009) The many roles of histone deacetylases in development and physiology: Implications for disease and therapy. Nature Reviews Genetics 10:32
Wu L-M, Yang Z, Zhou L, Zhang F, Xie H-Y, Feng X-W, Wu J et al (2010) Identification of histone deacetylase 3 as a biomarker for tumor recurrence following liver transplantation in HBV-associated hepatocellular carcinoma. PLoS ONE 5:e14460
Ler SY, Leung CHW, Khin LW, Lu GD, Salto-Tellez M, Hartman M, Iau PTC et al (2015) HDAC1 and HDAC2 independently predict mortality in hepatocellular carcinoma by a competing risk regression model in a Southeast Asian population. Oncology Reports. 34:2238–2250
Yang J, Jin X, Yan Y, Shao Y, Pan Y, Roberts LR, Zhang J et al (2017) Inhibiting histone deacetylases suppresses glucose metabolism and hepatocellular carcinoma growth by restoring FBP1 expression. Scientific Reports 7:43864
Lee Y-H, Seo D, Choi K-J, Andersen JB, Won M-A, Kitade M, Gómez-Quiroz LE et al (2014) Antitumor effects in hepatocarcinoma of isoform-selective inhibition of HDAC2. Cancer Research 74(17):4752–4761
Gailhouste L, Liew LC, Yasukawa K, Hatada I, Tanaka Y, Nakagama H, Ochiya T (2018) Differentiation therapy by epigenetic reconditioning exerts antitumor effects on liver cancer cells. Molecular Therapy 26(7):1840–1854
Liu J, Liu Y, Meng L, Liu K, Ji B (2017) Targeting the PD-L1/DNMT1 axis in acquired resistance to sorafenib in human hepatocellular carcinoma. Oncology Reports 38:899–907
Mei Q, Chen M, Lu X, Li X, Duan F, Wang M, Luo G et al (2015) An open-label, single-arm, phase I/II study of lower-dose decitabine based therapy in patients with advanced hepatocellular carcinoma. Oncotarget 6:16698–16711
Fan H, Lu X, Wang X, Liu Y, Guo B, Zhang Y, Zhang W et al (2014) Low-dose decitabine-based chemoimmunotherapy for patients with refractory advanced solid tumors: A phase I/II report. Journal of Immunology Research 2014:371087
Raynal NJ, Issa PJ (2016) DNA methyltransferase inhibitors. Drug discovery in cancer epigenetics. Academic Press, Boston, pp 169–190
Griffiths EA, Choy G, Redkar S, Taverna P, Azab M, Karpf AR (2013) SGI-110: DNA methyltransferase inhibitor oncolytic. Drugs of the Future 38:535–543
Jueliger S, Lyons J, Azab M, Taverna P (2012) 465 SGI-110, a novel second generation DNa hypomethylating agent, enhances sorafenib activity and alters methylation signature of HCC cell lines. European Journal of Cancer 48:144
Jueliger S, Lyons J, Cannito S, Pata I, Pata P, Shkolnaya M, Lo Re O et al (2016) Efficacy and epigenetic interactions of novel DNA hypomethylating agent guadecitabine (SGI-110) in preclinical models of hepatocellular carcinoma. Epigenetics 11:709–720
El-Khoueiry A, Mulcahy MF, Bekaii-Saab T, Kim R, Denlinger C, Goel R, Gupta S et al (2015) Abstract 2947: Pharmacodynamic (PD) and pharmacokinetic (PK) results of the second-generation hypomethylating agent, SGI-110, in patients with hepatocellular carcinoma (HCC) after progression on sorafenib. Cancer Research 75:2947
Kuang Y, El-Khoueiry A, Taverna P, Ljungman M, Neamati N (2015) Guadecitabine (SGI-110) priming sensitizes hepatocellular carcinoma cells to oxaliplatin. Molecular Oncology 9:1799–1814
Di Fazio P, Schneider-Stock R, Neureiter D, Okamoto K, Wissniowski T, Gahr S, Quint K et al (2010) The pan-deacetylase inhibitor panobinostat inhibits growth of hepatocellular carcinoma models by alternative pathways of apoptosis. Cellular Oncology 32:285–300
Di Fazio P, Montalbano R, Quint K, Alinger B, Kemmerling R, Kiesslich T, Ocker M et al (2013) The pan-deacetylase inhibitor panobinostat modulates the expression of epithelial-mesenchymal transition markers in hepatocellular carcinoma models. Oncology Letters 5:127–134
Gahr S, Mayr C, Kiesslich T, Illig R, Neureiter D, Alinger B, Ganslmayer M et al (2015) The pan-deacetylase inhibitor panobinostat affects angiogenesis in hepatocellular carcinoma models via modulation of CTGF expression. International Journal of Oncology 47:963–970
Ma BBY, Sung F, Tao Q, Poon FF, Lui VW, Yeo W, Chan SL et al (2010) The preclinical activity of the histone deacetylase inhibitor PXD101 (belinostat) in hepatocellular carcinoma cell lines. Investigational New Drugs 28:107–114
Yeo W, Chung HC, Chan SL, Wang LZ, Lim R, Picus J, Boyer M et al (2012) Epigenetic therapy using belinostat for patients with unresectable hepatocellular carcinoma: A multicenter phase I/II study with biomarker and pharmacokinetic analysis of tumors from patients in the mayo phase II consortium and the cancer therapeutics research group. Journal of Clinical Oncology 30:3361–3367
Bitzer M, Horger M, Giannini EG, Ganten TM, Wörns MA, Siveke JT, Dollinger MM et al (2016) Resminostat plus sorafenib as second-line therapy of advanced hepatocellular carcinoma—the SHELTER study. Journal of Hepatology 65:280–288
Fu M, Shi W, Li Z, Liu H (2016) Activation of mPTP-dependent mitochondrial apoptosis pathway by a novel pan HDAC inhibitor resminostat in hepatocellular carcinoma cells. Biochemical and Biophysical Research Communications 477:527–533
Soukupova J, Bertran E, Peñuelas-Haro I, Urdiroz-Urricelqui U, Borgman M, Kohlhof H, Fabregat I (2017) Resminostat induces changes in epithelial plasticity of hepatocellular carcinoma cells and sensitizes them to sorafenib-induced apoptosis. Oncotarget 8:110367–110379
Lai C-J, Bao R, Tao X, Wang J, Atoyan R, Qu H, Wang D-G et al (2010) CUDC-101, a multitargeted inhibitor of histone deacetylase, epidermal growth factor receptor, and human epidermal growth factor receptor 2. Exerts Potent Anticancer Activity. Cancer Research 70:3647
Fu S, Nemunaitis JJ, Bessudo A, Bauman JE, Hamid O, Witta SE, Dy GK et al (2012) A phase Ib study of CUDC-101, a multitargeted inhibitor of EGFR, HER2, and HDAC, in patients with advanced head and neck, gastric, breast, liver, and non-small cell lung cancer. Journal of Clinical Oncology 30:e13101
Callegari E, Elamin Bahaeldin K, Giannone F, Milazzo M, Altavilla G, Fornari F, Giacomelli L et al (2012) Liver tumorigenicity promoted by microRNA-221 in a mouse transgenic model. Hepatology 56:1025–1033
Moshiri F, Callegari E, D’Abundo L, Corrà F, Lupini L, Sabbioni S, Negrini M (2014) Inhibiting the oncogenic mir-221 by microRNA sponge: Toward microRNA-based therapeutics for hepatocellular carcinoma. Gastroenterology and Hepatology From Bed to Bench 7:43–54
Hsu S, Wang B, Kota J, Yu J, Costinean S, Kutay H, Yu L et al (2012) Essential metabolic, anti-inflammatory, and anti-tumorigenic functions of miR-122 in liver. The Journal of Clinical Investigation. 122:2871–2883
Tsai W-C, Hsu S-D, Hsu C-S, Lai T-C, Chen S-J, Shen R, Huang Y et al (2012) MicroRNA-122 plays a critical role in liver homeostasis and hepatocarcinogenesis. The Journal of Clinical Investigation 122:2884–2897
Varnholt H, Drebber U, Schulze F, Wedemeyer I, Schirmacher P, Dienes HP, Odenthal M (2007) MicroRNA gene expression profile of hepatitis C virus–associated hepatocellular carcinoma. Hepatology 47:1223–1232
Spaniel C, Honda M, Selitsky SR, Yamane D, Shimakami T, Kaneko S, Lanford RE et al (2013) microRNA-122 abundance in hepatocellular carcinoma and non-tumor liver tissue from japanese patients with persistent HCV versus HBV infection. PLoS ONE 8:e76867
Janssen HLA, Reesink HW, Lawitz EJ, Zeuzem S, Rodriguez-Torres M, Patel K, van der Meer AJ et al (2013) Treatment of HCV infection by targeting MicroRNA. New England Journal of Medicine 368:1685–1694
Lanford RE, Hildebrandt-Eriksen ES, Petri A, Persson R, Lindow M, Munk ME, Kauppinen S et al (2010) Therapeutic silencing of microRNA-122 in primates with chronic hepatitis C virus infection. Science. 327:198–201
van der Ree MH, van der Meer AJ, de Bruijne J, Maan R, van Vliet A, Welzel TM, Zeuzem S et al (2014) Long-term safety and efficacy of microRNA-targeted therapy in chronic hepatitis C patients. Antiviral Research 111:53–59
Ree MH, Meer AJ, Nuenen AC, Bruijne J, Ottosen S, Janssen HL, Kootstra NA et al (2016) Miravirsen dosing in chronic hepatitis C patients results in decreased microRNA-122 levels without affecting other microRNAs in plasma. Alimentary Pharmacology & Therapeutics 43:102–113
Qadir XV, Han C, Lu D, Zhang J, Wu T (2014) miR-185 inhibits hepatocellular carcinoma growth by targeting the DNMT1/PTEN/Akt pathway. The American Journal of Pathology 184:2355–2364
Authors’ contributions
TBT and JJL compiled the references and wrote the manuscript. EKHC edited the manuscript. All authors read and approved the final manuscript.
Acknowledgements
E.K-H. Chow would like to acknowledge funding from the National Research Foundation Cancer Science Institute of Singapore RCE Main Grant and Ministry of Education Academic Research Fund (MOE AcRF Tier 2, MOE2015-T2-2-126, Seed Fund Grant T1-BSRG 2014–05) and and NMRC Translational and Clinical Research (TCR) Flagship Programme (NMRC/TCR/015-NCC/2016).
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
Not applicable.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Funding
National Research Foundation Cancer Science Institute of Singapore RCE Main Grant and Ministry of Education Academic Research Fund (MOE AcRF Tier 2, MOE2015-T2-2-126, Seed Fund Grant T1-BSRG 2014–05) and and NMRC Translational and Clinical Research (TCR) Flagship Programme (NMRC/TCR/015-NCC/2016).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Toh, T.B., Lim, J.J. & Chow, E.KH. Epigenetics of hepatocellular carcinoma. Clin Trans Med 8, 13 (2019). https://doi.org/10.1186/s40169-019-0230-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40169-019-0230-0