
Abstract
This study compared the effects of a brief repeated sprint training (RST) intervention performed with bilateral blood flow restriction (BFR) conditions in normoxia or conducted at high levels of hypoxia on response to exercise. Thirty-nine endurance-trained athletes completed six repeated sprints cycling sessions spread over 2 weeks consisting of four sets of five sprints (10-s maximal sprints with 20-s active recovery). Athletes were assigned to one of the four groups and subjected to a bilateral partial blood flow restriction (45% of arterial occlusion pressure) of the lower limbs during exercise (BFRG), during the recovery (BFRrG), exercised in a hypoxic room simulating hypoxia at FiO2 ≈ 13% (HG) or were not subjected to additional stress (CG). Peak aerobic power during an incremental test, exercise duration, maximal accumulated oxygen deficit and accumulated oxygen uptake (VO2) during a supramaximal constant-intensity test were improved thanks to RST (p < 0.05). No significant differences were observed between the groups (p > 0.05). No further effect was found on other variables including time-trial performance and parameters of the force-velocity relationship (p > 0.05). Thus, peak aerobic power, exercise duration, maximal accumulated oxygen deficit, and VO2 were improved during a supramaximal constant-intensity exercise after six RST sessions. However, combined hypoxic stress or partial BFR did not further increase peak aerobic power.
Similar content being viewed by others
Introduction
In the last two decades, high-intensity interval training (HIT) has gained remarkable popularity in the sports sphere. Similar or higher gains in several variables, including maximal oxygen uptake (\(\dot{V}{O}_2\mathit{\max}\)), muscle oxidative capacity and time trial performance were shown compared to endurance training protocols achieved with higher training volume [1,2,3]. The addition of hypoxic stimulus to HIT has been increasingly acknowledged to favor training adaptations [4,5,6,7,8,9]. Performing exercise bouts under systemic hypoxia reduces arterial oxygen partial pressure and thus increases energy production through substrate-level phosphorylation [10] and adaptations such as enhanced mitochondrial density, oxidative enzyme activity, and capillary density [11,12,13]. However, it is well recognized that the use of systemic hypoxia induces several adaptive responses and may improve both aerobic and anaerobic performance, as well as repeated sprint ability depending on the nature of the training protocol administered [14, 15]. In the last decade, it was found that repeated sprint training (RST) in hypoxic conditions (called “RSH”) may promote several additional effects on adaptations to exercise [16]. Thus, improvements in repeated sprint ability and several sport-specific physical and technical parameters have been recently reported, notably in swimmers and tennis players [17, 18].
Importantly, it was observed that RSH can significantly enhance performance in a very short window period. In the study from Beard et al., the authors found that four sessions of RSH spread over 2 weeks enhanced repeated sprint ability (i.e., both maximal and mean power) in world-level male rugby union players [19]. Other studies also highlighted that intensified training over 2 weeks or RSH over 10 days can improve physical performance in soccer players and a professional cyclist, respectively [20, 21]. Finally, another investigation demonstrated that six sessions of RSH spread over 2 weeks improved repeated sprint ability of upper body muscles in cross-country skiers [22]. Thus, these findings make RSH of practical relevance in several sports disciplines, especially those where only a short window period is available prior to competition (i.e., “in-season”).
On the other hand, some studies found no impact of RSH on field performance in swimmers [23] or endurance performance in rugby players [24]. Another point of concern is the loss of exercise performance observed in some HIT acute studies in hypoxia, which could lead to relative undertraining compared to training in normoxia in chronic studies [25, 26]. However, those studies used longer sprint exercises than RST. Thus, as glycogenolysis rates decline during long sprints, performance could be more impaired in these protocols [27]. Altogether, RSH potentially improves training adaptations during training protocols.
In addition to training under systemic hypoxia, other strategies have been proposed to enhance training adaptations with local hypoxia in muscles such as training with blood flow restriction (BFR) [28, 29]. BFR training is becoming increasingly popular and represents another way to generate local hypoxia in skeletal muscles and/or to limit venous return depending on occlusion pressure. In recent years, the impact of BFR on performance has been increasingly studied and several investigations have suggested that using BFR may be suitable to provide additional physiological stress and to improve performance.
A study showed that a short-term low-intensity interval BFR (140 to 200 mmHg) training simultaneously increases maximum oxygen uptake (\(\dot{V}{O}_2\mathit{\max}\Big)\) and muscle strength, but no effect was found with HIT even if combined with BFR [30]. Importantly, BFR is enjoying a resurgence in popularity especially since it was combined with HIT protocols [31,32,33]. Thus, Mitchell et al. [34] recently highlighted that adding partial BFR to a 4-week sprint interval training program enhanced \(\dot{V}{O}_2\mathit{\max}\). In this study, HIT without BFR did not show these benefits [34]. Nonetheless, effects on critical power were the same with or without BFR and no impact was found on skeletal muscle mitochondrial and capillarity protein content in either group [34]. Of note, Taylor and coworkers have previously reported that sprint interval training with post-exercise BFR was an effective stimulus to augment \(\dot{V}{O}_2\mathit{\max}\) but the authors did not find improvement in exercise performance (i.e. 15-km time trial) [33]. Furthermore, little is known about the use of BFR during RST protocols except for acute physiological responses. It was suggested that the intermittent application of BFR during RST promotes greater changes in skeletal muscle blood volume (as observed by an increase of total hemoglobin concentrations) [31]. Given this fact, RST with BFR could be considered as an alternative to RSH to induce similar or complementary adaptations and potentially enhance performance.
Hence, even if progress has been made on the impact of training with BFR on performance, there is a lack of data regarding the effects of RST with BFR. Even though continuous BFR has already been compared to intermittent BFR [35], to the best of our knowledge, no study has tested the effects of BFR during exercise versus recovery. Indeed, it has been shown that intermittent BFR can induce similar responses and adaptations compared to continuous BFR, with a reduced pain perception [36, 37]. In addition, no study has compared the benefits of training with BFR to those of training in systemic hypoxia in a single study, especially during a short window period. Nonetheless, achieving performance gains quickly is of practical relevance in several sport disciplines where only a brief period is available prior to championship [19]. Therefore, the present study aimed to compare the effects of RST with bilateral partial BFR (45% of femoral artery occlusion pressure measured at rest) with a systemic hypoxic training protocol at 13% FiO2 (4000 m simulated altitude) on both aerobic and anaerobic responses to exercise (i.e., ramp incremental exercise, time trial, torque-velocity test, and supramaximal exercise) in a short window period. It has been chosen to set maximal stress for both hypoxic and BFR protocols that could be tolerated in this cohort in combination with the training sessions proposed based on preliminary work in our laboratory. Moreover, this study also compared two BFR protocols (i.e., BFR during exercise versus BFR during recovery). It was expected that BFR during exercise would induce higher local stress among muscles and would be more beneficial than BFR during recovery.
Materials and methods
Participants
A priori power analyses were performed with alpha and beta errors of 0.05 and 0.20, respectively, and a medium effect size (f = 0.25) as it has been observed during these training protocols [4,5,6,7,8,9]. The required sample size was 36 split into four groups. Hence, forty male endurance-trained participants initially volunteered to be enrolled in the study and 39 were included in the analysis (mean ± SD; age 25.6 ± 5.7 years; height 176.0 ± 4.4 cm; weight 79.1 ± 15.3 kg; body mass index 23.8 ± 2.5 kg m−2) (Table 1). Participants were involved in endurance activities, including running and/or cycling. The participants were not acclimated to altitude and did not sojourn for more than 2 days at altitude during the 2 months preceding the experiment. Participants were instructed to maintain regular dietary habits throughout the period of the protocol and to abstain from alcohol and dietary supplements or ergogenic aids during the studied period. The study procedures complied with the last Declaration of Helsinki on human experimentation and were approved by the “Commission cantonale d’éthique de la recherche sur l’être humain, Canton de Vaud, CER-VD” (number 2016-02068). The participants provided written informed consent and were informed about possible inconveniences associated with the experiment. All experiments were performed in accordance with relevant guidelines and regulations.
Study design
The study was conducted over 4 weeks (Fig. 1) including 1 week of pre-tests (W1), 2 weeks of training (W2 and W3) counting six training sessions (three times per week), and 1 week of post-tests (W4). On W1 and W4, the participants performed a battery of tests in normoxia over 2 days separated by 48 h, including a ramp incremental exercise (day 1), a time trial performance (day 1), a torque-velocity relationship test (day 2), and an anaerobic capacity exercise (day 2). All testing was carried out at the laboratory with the same environmental condition at the same hour of the day to minimize the effects of circadian cycles. The post-tests on W4 were assessed 3 days after the last training session. In addition, all participants were instructed not to perform high-intensity exercises in their personal training to limit interference with the present protocol.

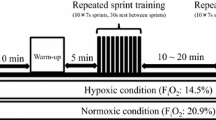
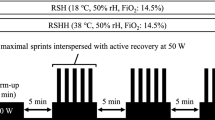
Sequence of the experimental protocol. Participants were randomized into four groups (HG, training in hypoxia; BFRG, training with blood flow restriction during exercise; BFRrG, training with blood flow restriction during recovery; CG, control group without hypoxia or BFR) for a training period of 2 weeks. During warm-up, participants were instructed to exercise at 110 W for 10 min and to finish with a 10-s maximal sprint. On two occasions, participants were asked to perform a battery of tests on two consecutive days
Randomization across the groups was done using \(\dot{V}{O}_2\mathit{\max}\) values relative to body weight according to stratified simple randomization method, and the participants were assigned to one of the four RST groups: HG (hypoxic training group; N = 10, simulated altitude of 4000 m; FiO2 ≈ 13%); BFRG (training with blood flow restriction during sprint exercises in normoxia; N = 10), BFRrG (training with blood flow restriction during recovery between sprint exercises in normoxia; N = 10), and CG in normoxia (control group; training in normoxic group, N = 9).
Randomization was done by an independent researcher blinded to the individuals. BFRG and BFRrG training were subjected to bilateral-leg partial occlusion (45% of femoral artery occlusion pressure measured at rest; 88.2 ± 10.1 mmHg). Of note, the cuff pressure of 45% was fixed following preliminary work performed in the laboratory that highlighted it was the highest level that could be tolerated by the participants in combination with the present RSH protocol. BFR was set up during the 10 s of exercises using automated cuffs. The cuff was released between intervals for this group. For BFRrG, participants were asked to maintain a stationary position on the ergocycle and BFR was applied immediately at the end of each sprint exercise during the 20 s recovery periods. Verbal encouragement was provided during the tests, as well as during the training sessions.
Tests
Anthropometric and femoral artery occlusion pressure measurement
On arrival at the laboratory for the first visit, anthropometric characteristics were assessed using bioelectrical impedance analysis (Tanita, MC-780 MAP, France), and femoral artery occlusion pressure of the lower limbs was measured. For this purpose, automated cuffs (11 × 85 cm cuff size, 10 × 41 cm bladder size, SC10D Rapid Version Cuff, D. E. Hokanson, Inc., Bellevue, WA, USA) were placed on the most proximal region of the lower limbs [38]. Artery pressure was measured at seated rest on a chair by gradually increasing the occlusion pressure until a point when no blood flow was observed in the femoral artery using a linear Doppler ultrasound probe (L12-5L60N) with Echo Wave II 3.4.4 software (Telemed Medical Systems, Lithuania, Telemed Ltd., Milan, Italy). These measurements were performed two or three times to make sure there was no variation and for accuracy, with 2 min between trials. The highest-pressure value obtained was used to determine the 45% of femoral artery occlusion pressure applied for BFRG and BFRrG during the exercise sessions.
Ramp incremental test
Participants performed a ramp test on an electronically-braked cycling ergometer (Lode Excalibur Sport Ergometer, Lode B.V., Netherlands). First, participants completed a warm-up which was composed of 3 steps of 4 min each at 75, 105, and 135 W respectively. Then, after 5 min of rest, the ramp incremental test was initiated at 60 W with an increase of 1 W every 2 s, (30 W/min) until exhaustion. Cardio-respiratory variables were measured breath-by-breath using a metabolic cart (Quark, Cosmed, Italy). Breathing flow was measured by a bi-directional digital turbine that was calibrated at the beginning of each test with a 3-L syringe. O2 and CO2 analyzers were calibrated before each test using ambient air and standard gas (O2: 15%, CO2: 4.99%). The breath-by-breath pulmonary gas exchange data were collected continuously throughout the test. \(\dot{V}{O}_2\mathit{\max}\) and maximum heart rate (HRmax) were determined averaging the last 30 s of exercise. HR was collected with a telemetry-based HR monitor (Garmin, Garmin Ltd., Lathe, Kansas, USA). The end of the ramp test was based on the achievement of three of the following criteria [39]: (i) heart rate greater than 90% of the predicted maximum (220 beats per minute−age) (ii) respiratory exchange ratio (RER) ≥ 1.10 [40], (iii) the athlete’s rating of perceived exertion (i.e., Borg Scale rating ≥ 18), and (iv) the participants stopped the exercise despite strong verbal encouragements. At the end of this test, participants performed an active recovery at a self-adjusted low-intensity pace during 10 min on the ergocycle. Power at the end of the test was considered as the peak aerobic power [41]. The height and configuration of the saddle and handlebars were recorded and reproduced in subsequent tests.
Time trial
To simulate a field cycling performance, participants performed a 250-kJ time trial on the same ergocycle [42]. Participants were instructed to complete the exercise as fast as possible. The resistance and pedal cadence were self-selected in a linear mode load where the linear factor (α) was calculated as follows: α = P/rpm2; where P (W) is 70% of peak aerobic power and revolutions per minute (rpm) is the theoretical optimal cadence (85 rpm). The work progression in kilojoules was given to the participants.
Torque–velocity test
On day 2, participants performed a warm-up consisting of 6 min of submaximal cycling at 100 W, followed by two short submaximal accelerations (5 s) at 80 and 100 rpm, respectively. After 4 min of passive recovery, participants performed a force-velocity test [43] consisting of six repetitive maximal sprints of 5 s in isokinetic mode (i.e., 70, 85, 100, 115, 130, and 145 rpm). The sprints were separated by 4 min of active recovery at 50 W and 80 rpm. Participants had 10 s before the sprint to reach the requested cycling cadence. Torque, rpm, and power were recorded at the frequency of 5 Hz. The torque-velocity relationship was described using a linear relationship. An iterative process was used to minimize the sum of the squared errors between the fitted function and the observed values. Force when contraction velocity is null (T0, x-axis intercept), velocity of unloaded shortening (v0, y-axis intercept), and the slope of the relationship were estimated. The power-velocity relationship was modeled using a second-degree polynomial function where the power of each sprint was the average of the last 3 s of sprinting. In the same way, an iterative process was used to determine the parameter of the quadratic function. The derivative of the polynomial (derivative = zero) was used to calculate the maximum power from this test (Pmax) and to deduce the optimal pedaling velocity (vopt) and torque (Topt) at Pmax.
Assessment of anaerobic capacity
The warm-up consisted of three exercises at different powers (60, 90, 120 W) each lasting 4 min, followed by 5 min of passive recovery. Then, participants performed a supramaximal exercise (105% peak aerobic power) to exhaustion on ergocycle acting in hyperbolic (rpm-independent) mode [44,45,46]. Cardio-respiratory variables were measured breath-by-breath. Anaerobic energy release (i.e., anaerobic capacity) was assessed by quantification of the maximal accumulated oxygen deficit. This consists of calculating the difference over time between the theoretical oxygen consumption at a supra maximum intensity (105% of peak aerobic power) and the effective oxygen uptake. The theoretical consumption was obtained by extrapolating the curve of oxygen consumption as a function of sub-maximum loads. Oxygen consumption of sub-maximum loads was acquired during the warm-up of the ramp incremental test (75 W, 105 W, and 135 W) and during the anaerobic capacity test (60 W, 90 W, and 120 W). Maximal accumulated oxygen deficit was calculated as the area between theoretical and actual oxygen consumption as a function of time. Exercise duration, peak oxygen uptake (\(\dot{V}{O}_2 peak\)), total O2 demand, accumulated oxygen uptake (O2 uptake), the contribution of both aerobic and anaerobic processes (%), % \(\dot{V}{O}_2\mathit{\max}\), and mean \(\dot{V}{O}_2\), were measured. Minute ventilation (\(\dot{V}E\)), \(\dot{V}E\)/\(\dot{V}\mathrm{O}\)2, \(\dot{V}E\)/\(\dot{V}\mathrm{CO}\)2, RER, and heart rate (HR) at the end of the test are also provided. To minimize artifact, values have been filtered (i.e., second order zero-lag Butterworth filter, cutoff frequency 0.05).
Training protocol
Participants followed a 2-week training program with three training sessions per week [22] according to the modality drawn at random. After warming up for 10 min at 110 W, participants performed a first 10-s maximal sprint followed by an active recovery of 5 min at 75 W. Then, the repeated-sprint protocol consisted of four sets of 5 × 10-s maximal (i.e., all-out and sitting) cycling sprints separated by 20 s of active recovery at 75 W between sprints. Five minutes of active recovery (75 W) were performed between sets 1 and 2, and 3 and 4. Recovery between sets 2 and 3 consisted of 10 min of active recovery at 75 W. Sprints were conducted on an ergocycle programmed on constant torque mode (Wingate mode) with a torque factor of 0.8 Nm.kg–1. Shoe clips were used to ensure pedal contact. Exercise bouts were initiated from a rolling start. No progressive overload was applied to training or hypoxic stimulus because the window period was very short, and participants were endurance trained. Mean power, maximal power, and total work were collected throughout the protocol. In addition, a fatigue index was adapted from previous study [47] for each sprint:
where Total sprint mean power corresponds to the sum of sprint mean powers from all sprints and Ideal sprint mean power is the number of sprints x mean power of the most powerful sprint.
Participants were encouraged energetically to complete every repetition maximally and verbal indication of time was provided during each sprint for pacing prevention. Water intake was permitted ad libitum during the exercise sessions.
Statistics
Data from training sessions are presented as mean values ± standard deviation (SD). Data from the tests are presented graphically as box and whisker plots, including the minimum and maximum values, the interquartile region, the median, and the mean. Quartiles are also shown. Statistical analyses were performed using Jamovi (Version 1.1.9.0). One-way ANOVA (analysis of variance) was used to compare anthropometric characteristics before the training program. Linear mixed models were used for all the other variables. Linear mixed models consider both the nested and crossed structure of the data [48, 49]. Thus, Linear mixed models provide precise estimates when data are hierarchized. After inspecting residual plots, no obvious deviations from normality and homoscedasticity were observed. The fixed effect was the group (HG, BFRG, BFRrG, CG), and the time (pre- and post-tests) where participant was the random effect. To obtain contrasts, Holm correction was used. Significance was declared when p < 0.05. Effect sizes (d) are also provided (trivial effect d < 0.10, small effect d = 0.20, medium effect d = 0.50 and large effect d = 0.8) [50].
Results
Training sessions
There were initially 10 participants per group but one of them stopped the experimentation within CG for personal reasons. There were no symptoms of dizziness during all conditions. There was no significant difference on training data (i.e., mean power, maximal power, and total work; Fig. 2) between groups (p = 0.26, 0.09, and 0.26, respectively) and between the different training sessions (p = 0.47, 0.29 and 0.50, respectively). An effect of training session was found for fatigue index (p < 0.001). Post hoc analyses showed that fatigue index was greater during the first session compared to the second (p = 0.011; d = 0.58), third (p < 0.001; d = 0.63), fourth (p = 0.001; d = 0.62), fifth (p < 0.001; d = 0.73), and sixth (p < 0.001; d = 0.71). There was no significant interaction for mean power, total work, and fatigue index (p = 0.39, 0.20 and 0.50, respectively). However, an interaction was found for maximal power (p = 0.004) even if post hoc analyses did not reveal significant effects after Holm correction.

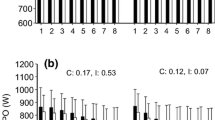
Evolution of mean power (A), maximal power (B), total work (C) and fatigue index (D) during the training protocol. HG, training in hypoxia (N = 10); BFRG, training with blood flow restriction during exercise (N = 10); BFRrG, training with blood flow restriction during recovery (N = 10); CG, training in normal group (N = 9). *: significantly different from the other training sessions (p < 0.05). Of note, for more clarity, standard deviations are displayed unilaterally
Ramp incremental test
There was no time and group effect, or interaction, on \(\dot{V}{O}_2 peak\) relative to body weight during the ramp exercise (p = 0.80, 0.09 and 0.28, respectively). No time and group effect, or interaction, was found for absolute \(\dot{V}{O}_2 peak\) values (p = 0.52, 0.25, and 0.14, respectively). Peak aerobic power increased in all groups after training (d = 0.5, 0.2, 0.2, 0.2 for HG, BFRG, BFRrG, and CG, respectively). This represents an increase with training of 4.4%, 2.8%, 2.2%, and 3.0% for HG, BFRG, BFRrG, and CG, respectively (Fig. 3). Peak aerobic power expressed relative to body weight also increased with time (p = 0.008; d = 0.3, for HG, and 0.2 for BFRG, BFRrG, and CG). However, no interaction and no group differences were found (p = 0.82 and 0.86, respectively) (Fig. 3).

Results of the ramp test. A Relative and B absolute peak oxygen consumption \((\dot{V}{O}_2 peak)\), and C peak aerobic power before and after training in hypoxia (HG, N = 10), training with blood flow restriction during exercise (BFRG, N = 10), training with blood flow restriction during recovery (BFRrG, N = 10), and training in normal group (CG, N = 9). # training effect. The whiskers represent minimum and maximum values, the boxes the interquartile region, the horizontal lines the medians, the crosses are the mean. Quartiles are also shown
Time trial performance
At baseline, time to complete the 250 kJ time trial was not significantly different between the groups (p = 0.75) and remained unchanged (p = 0.14) when repeated after the training program (Fig. 4). There was a significant interaction (p = 0.042) for mean power, however, the adjusted p value (Holm correction) was not significant (p = 0.19).

Time trial performance. A Time to reach 250 kJ before and after training in hypoxia (HG, N = 10), training with blood flow restriction during exercise (BFRG, N = 10), training with blood flow restriction during recovery (BFRrG, N = 10), and training in normal group (CG, N = 9). The whiskers represent minimum and maximum values, the boxes the interquartile region, the horizontal lines the medians, the crosses are the mean. Quartiles are also shown
Torque-velocity exercise
No significant effect of training was found concerning Pmax, T0, v0, Topt, and vopt (Table 2). However, there was an effect of group on Pmax for both absolute and relative to body weight values and for Topt (d = 1.2). Post hoc analyses showed that Pmax and Topt were lower for BFRrG compared to BFRG (p < 0.001; d = 0.9 and p = 0.002; d = 1.2 respectively) and compared to HG (p = 0.007; d = 1.3 and 0.009; d = 1.2 respectively). Relative Pmax was lower for BFRrG compared to BFRG (p = 0.010; d = 0.6).
Anaerobic capacity
An increase of \(\dot{V}{O}_2 peak\) expressed relative to body mass was found in BFRrG (p = 0.030; d = 0.7) but this effect was no longer observed for absolute \(\dot{V}{O}_2 peak\) values. The former represents an increase of 7.5%. Concerning maximal accumulated oxygen deficit, no interaction and no main effect of group were observed. However, a time effect was found with higher values observed after training. \(\dot{V} Epeak\) was higher in HG compared to BFRrG (p = 0.019; d = 1.4). RER was higher in BFRG (p = 0.002; d = 1.4) and in CG (p = 0.007; d = 1.3) compared to HG. However, no difference was found between the groups for the other variables (p > 0.05; Tables 3 and 4). A training effect was observed for all the other variables (p < 0.05), excepting peak \(\dot{V}E\)/\(\dot{V}{O}_2\) and HRpeak.
Discussion
The aim of this study was to compare the effects of RST with BFR or systemic hypoxia on performance in endurance-trained subjects during a very short-time window. The main result of the present study is that there are overall no significant differences among the groups after 2 weeks of RST. However, the data show that a 2-week RST program with three training sessions per week may promote gains of peak aerobic power, as well as maximal accumulated oxygen deficit and accumulated oxygen uptake during a supramaximal constant-intensity test. Nevertheless, time-trial performance was not enhanced by the current protocols.
Training data
In the present study, there was no difference on training data (i.e. mean and peak power, total work) within the protocol between groups and training sessions. However, a decrease of fatigue index was observed following the first session in all the groups, probably through habituation. The present protocol could be too short (six sessions spread over 2 weeks) to observe any evolution of power output and total work. Indeed, in a fairly similar protocol, Montero and Lundby previously observed that 4 weeks of RST with three sessions per week enhanced repeated sprint performance in endurance-trained subjects [51]. However, no additional effect of RSH over training in normoxia was observed in tests performed in both hypoxic and normoxic groups [51]. Other studies observed that RST protocols may enhance resistance to fatigue and thus may increase the number of sprints performed [52]. Nonetheless, no difference between RST and RSH on total work, mean power output, RPE and pain in the legs were observed in a protocol close to ours [7]. Finally, since significant interaction for maximal power during training was found, the commitment to 2 weeks of HIT training between the four groups is not guaranteed. However, post hoc analyses did not reveal differences between groups, suggesting that there was no significant difference.
Ramp test
The present data indicate that peak aerobic power and exercise duration were improved by exercise interventions. These results are in line with previous literature that generated consistent data to confirm that high intensity and sprint exercises promote gains in cardiorespiratory fitness [53]. Nonetheless, the addition of hypoxic and BFR stresses to the current RST protocol did not induce further benefits on anaerobic performance and most physiological variables. However, previous literature has reported some enhancement of molecular actors involved in glycolysis with RSH [7, 52]. RSH with voluntary hypoventilation at low lung volume due to the hypercapnic effect also promotes significant effects on blood lactate concentration and stroke volume [18, 54]. Finally, a significant impact of training was observed concerning minute ventilation and RER suggesting that RST may induce changes in muscle metaboreflex and chemoreflex activation [55, 56]. Importantly, ventilation and RER appeared higher for HG compared to BFRrG and RER was lower for HG compared to BRFG and CG. These data suggest that an impact on the ventilatory response to exercise may exist and potentially affect the perception of effort which could play a role in fatigue development.
The absence of training effects on \(\dot{V}{O}_2 peak\) from the ramp incremental exercise (both relative and absolute values) in all the groups is in line with the previous results of Kasai et al. [57] who found enhanced peak and mean power outputs after RSH (FiO2 = 14.5%) during repeated sprint tests without any effect on \(\dot{V}{O}_2\mathit{\max}\). Similar results on \(\dot{V}{O}_2\mathit{\max}\) were obtained by Wang et al. with a protocol consisting of 3 × 5 × 10 s with 20 s active recovery [58]. Of note, some studies observed a small improvement in \(\dot{V}{O}_2\mathit{\max}\) with RSH, however, RSH appears more related to the enhancement of repeated-sprint ability in team-sport and endurance athletes [6, 8]. In the present study, increases in peak aerobic power were found following RST but without additional effect with both systemic hypoxia and BFR. However, it was previously found that sprint exercise training, with longer sprint durations may improve aerobic fitness [59].
Torque-velocity test
All the force-velocity parameters (i.e., Pmax, T0,Topt, v0, and vopt) remained unaltered after training independently of the group. This suggests that the present RST protocol did not alter the mechanical properties of skeletal muscles leading to increases in maximal power output and muscle efficiency within contraction. Of note, significant differences were observed for longer protocol training duration [60]. Alternatively, it can be hypothesized that three RSH sessions per week could generate fatigue accumulation, thus blunting optimal adaptations.
Time trial
Finally, time trial performance was not improved by the present training protocol. This result can be explained by the fact that, as previously shown by Zinner et al., the latter is largely determined by \(\dot{V}{O}_2\mathit{\max}\) which was unaffected in our study [61]. Indeed, the authors found, with a mechanistic approach, that the principal adaptive mechanism to HIT is the improvement in aerobic energy production, and that the role of \(\dot{V}{O}_2\mathit{\max}\) as a limiting factor for endurance performance becomes even more important after training [61]. However, data indicate that the addition of a systemic hypoxic stress or BFR applied during the exercise bouts does not further improve the training effects on both anaerobic and aerobic performance compared to the control group in such a short period. Consistent with this, RST with additional stress did not elicit larger gains in absolute \(\dot{V}{O}_2 peak\) during the supramaximal constant-intensity exercises.
Anaerobic performance
According to the data, the current protocol leads to increases of both maximal accumulated oxygen deficit and accumulated \(\dot{V}{O}_2\) during the supramaximal constant-intensity exercises in a short time window, as well as contribution of aerobic process. These data suggest that, even if there were few effects on other performance data, training in such a short period should induce metabolic adaptations leading to enhancing some determinants of anaerobic performance. Of note, it cannot be ruled out that peak aerobic power from the time trial exercise should be improved through improvement of both maximal accumulated oxygen deficit and accumulated \(\dot{V}{O}_2\). Importantly, it was also recently observed that repeated sprint performance can be improved after only a 2-week RSH protocol in elite soccer players, international rugby union players and cross-country skiers [19, 20, 22]. Thus, our data are in line with these studies suggesting that 2-week RSH protocols may enhance some parameters of anaerobic performance. Finally, other investigations also observed improved repeated sprint ability with longer duration protocols, such as the study of Pramkratok and coworkers [62] with a protocol consisting of three sets of 6-s × 10 sprints at 140% of velocity at peak oxygen uptake on a treadmill, 3 days per week for 6 weeks.
Limitations
In this study, the four different groups allowed several comparisons, however, the number of groups made it difficult to complete a crossover study. In addition, even if no differences were observed in baseline data, individual trainability may represent a limitation. Therefore, these data must be interpreted regarding these limitations, especially concerning the observed tendencies. Another concern should be that we did not perform repeated sprint ability tests to examine the effectiveness of the present protocol on this field aptitude.
Conclusions and perspectives
In conclusion, no global differences were observed among the groups after 2 weeks of RST. However, the present study indicated that RST can be useful to enhance peak aerobic power or maximal accumulated oxygen deficit and VO2 during a supramaximal constant-intensity exercise in a very short preparation window in endurance-trained participants as it was previously found by other studies concerning repeated sprint ability. Importantly, the addition of hypoxic stress did not add further benefits on performance in this population. The mechanisms that mediate changes in human performance still represent an important challenge for further research. Specifically, additional investigations are needed to compare the effects of different hypoxic protocols (e.g., systemic vs. local hypoxia) on field performance and to examine cellular adaptations occurring in response to these training modalities. Indeed, while systemic hypoxia only reduces the O2 availability to the working muscle, BFR may additionally affect training adaptations by trapping metabolites in the muscle. The mechanisms of action of systemic hypoxia and BFR may be different, making it important to encourage additional studies identifying generic and specific induced adaptations for a better exercise prescription.
References
Burgomaster KA, Heigenhauser GJF, Gibala MJ. Effect of short-term sprint interval training on human skeletal muscle carbohydrate metabolism during exercise and time-trial performance. J Appl Physiol Bethesda Md 1985. 2006;100:2041–7.
Burgomaster KA, Howarth KR, Phillips SM, Rakobowchuk M, Macdonald MJ, McGee SL, et al. Similar metabolic adaptations during exercise after low volume sprint interval and traditional endurance training in humans. J Physiol. 2008;586:151–60.
Gibala MJ, Little JP, van Essen M, Wilkin GP, Burgomaster KA, Safdar A, et al. Short-term sprint interval versus traditional endurance training: similar initial adaptations in human skeletal muscle and exercise performance. J Physiol. 2006;575:901–11.
Brechbuhl C, Brocherie F, Willis SJ, Blokker T, Montalvan B, Girard O, et al. On the use of the repeated-sprint training in hypoxia in tennis. Front Physiol. 2020;11:588821.
James C, Girard O. In-season repeated-sprint training in hypoxia in international field hockey players. Front Sports Act Living. 2020;2:66.
Faiss R, Girard O, Millet GP. Advancing hypoxic training in team sports: from intermittent hypoxic training to repeated sprint training in hypoxia. Br J Sports Med. 2013;47:i45–50.
Faiss R, Léger B, Vesin J-M, Pierre-Etienne F, Eggel Y, Dériaz O, et al. Significant molecular and systemic adaptations after repeated sprint training in hypoxia. PLoS One. 2013;8:e56522.
Brocherie F, Girard O, Faiss R, Millet GP. Effects of repeated-sprint training in hypoxia on sea-level performance: a meta-analysis. Sports Med Auckl NZ. 2017;47:1651–60.
Brocherie F, Girard O, Faiss R, Millet GP. High-intensity intermittent training in hypoxia: a double-blinded, placebo-controlled field study in youth football players. J Strength Cond Res. 2015;29:226–37.
Puype J, Van Proeyen K, Raymackers J-M, Deldicque L, Hespel P. Sprint interval training in hypoxia stimulates glycolytic enzyme activity. Med Sci Sports Exerc. 2013;45:2166–74.
Bailey DM, Davies B. Physiological implications of altitude training for endurance performance at sea level: a review. Br J Sports Med. 1997;31:183–90.
Böning D. Altitude and hypoxia training--a short review. Int J Sports Med. 1997;18:565–70.
Flaherty G, O’Connor R, Johnston N. Altitude training for elite endurance athletes: a review for the travel medicine practitioner. Travel Med Infect Dis. 2016;14:200–11.
Katayama K, Matsuo H, Ishida K, Mori S, Miyamura M. Intermittent hypoxia improves endurance performance and submaximal exercise efficiency. High Alt Med Biol. 2003;4:291–304.
Warnier G, Benoit N, Naslain D, Lambrecht S, Francaux M, Deldicque L. Effects of sprint interval training at different altitudes on cycling performance at sea-level. Sports. 2020;8:148.
Girard O, Goods PSR, Brocherie F. Editorial: elevating sport performance to new heights with innovative ‘live low – train high’ altitude training. Front Sports Act Living. 2020;2:108.
Brechbuhl C, Brocherie F, Millet GP, Schmitt L. Effects of repeated-sprint training in hypoxia on tennis-specific performance in well-trained players. Sports Med Int Open. 2018;2:E123–32.
Trincat L, Woorons X, Millet GP. Repeated sprint training in hypoxia induced by voluntary hypoventilation in swimming. Int J Sports Physiol Perform. 2016;12(3):329-35.
Beard A, Ashby J, Chambers R, Brocherie F, Millet GP. Repeated-sprint training in hypoxia in International Rugby Union players. Int J Sports Physiol Perform. 2019;14:850–4.
Christensen PM, Krustrup P, Gunnarsson TP, Kiilerich K, Nybo L, Bangsbo J. VO2 kinetics and performance in soccer players after intense training and inactivity. Med Sci Sports Exerc. 2011;43:1716–24.
Faiss R, Rapillard A. Repeated sprint training in hypoxia: case report of performance benefits in a professional cyclist. Front Sports Act Living. 2020;2:35.
Faiss R, Willis S, Born D-P, Sperlich B, Vesin J-M, Holmberg H-C, et al. Repeated double-poling sprint training in hypoxia by competitive cross-country skiers. Med Sci Sports Exerc. 2015;47:809–17.
Camacho-Cardenosa M, Camacho-Cardenosa A, González-Custodio A, Zapata V, Olcina G. Effects of swimming-specific repeated-sprint training in hypoxia training in swimmers. Front Sports Act Living. 2020;2:100.
Hamlin MJ, Olsen PD, Marshall HC, Lizamore CA, Elliot CA. Hypoxic repeat sprint training improves rugby player’s repeated sprint but not endurance performance. Front Physiol. 2017;8:24.
Andersen AB, Bejder J, Bonne T, Olsen NV, Nordsborg N. Repeated Wingate sprints is a feasible high-quality training strategy in moderate hypoxia. PLoS One. 2020;15:e0242439 Public Library of Science.
Fallon S, Belcoe A, Shawcross C, May A, Monteverde C, McCann D. Elite female athletes’ ventilatory compensation to decreased inspired O2 during the wingate test. Res Q Exerc Sport. 2015;86:182–9 Routledge.
Parolin ML, Chesley A, Matsos MP, Spriet LL, Jones NL, Heigenhauser GJF. Regulation of skeletal muscle glycogen phosphorylase and PDH during maximal intermittent exercise. Am J Physiol-Endocrinol Metab. 1999;277:E890–900 American Physiological Society.
Willis SJ, Borrani F, Millet GP. High-intensity exercise with blood flow restriction or in hypoxia as valuable spaceflight countermeasures? Front Physiol. 2019;10:1266.
Wortman RJ, Brown SM, Savage-Elliott I, Finley ZJ, Mulcahey MK. Blood flow restriction training for athletes: a systematic review. Am J Sports Med. 2021;49(7):1938-44.
de Oliveira MFM, Caputo F, Corvino RB, Denadai BS. Short-term low-intensity blood flow restricted interval training improves both aerobic fitness and muscle strength. Scand J Med Sci Sports. 2016;26:1017–25.
Willis SJ, Alvarez L, Borrani F, Millet GP. Oxygenation time course and neuromuscular fatigue during repeated cycling sprints with bilateral blood flow restriction. Physiol Rep. 2018;6:e13872.
Solsona R, Berthelot H, Borrani F, Sanchez AMJ. Mechanical, cardiorespiratory, and muscular oxygenation responses to sprint interval exercises under different hypoxic conditions in healthy moderately trained men. Front Physiol. 2021;12:773950.
Taylor CW, Ingham SA, Ferguson RA. Acute and chronic effect of sprint interval training combined with postexercise blood-flow restriction in trained individuals. Exp Physiol. 2016;101:143–54.
Mitchell EA, Martin NRW, Turner MC, Taylor CW, Ferguson RA. The combined effect of sprint interval training and postexercise blood flow restriction on critical power, capillary growth, and mitochondrial proteins in trained cyclists. J Appl Physiol Bethesda Md 1985. 2019;126:51–9.
Brandner CR, Warmington SA. Delayed onset muscle soreness and perceived exertion after blood flow restriction exercise. J Strength Cond Res. 2017;31:3101–8.
Neto GR, Sousa MSC, Costa e Silva GV, Gil ALS, Salles BF, Novaes JS. Acute resistance exercise with blood flow restriction effects on heart rate, double product, oxygen saturation and perceived exertion. Clin Physiol Funct Imaging. 2016;36:53–9.
Silva JCG, Domingos-Gomes JR, Freitas EDS, Neto GR, Aniceto RR, Bemben MG, et al. Physiological and perceptual responses to aerobic exercise with and without blood flow restriction. J Strength Cond Res. 2021;35(9):2479-85.
Loenneke JP, Fahs CA, Rossow LM, Sherk VD, Thiebaud RS, Abe T, et al. Effects of cuff width on arterial occlusion: implications for blood flow restricted exercise. Eur J Appl Physiol. 2012;112:2903–12.
Sanchez AMJ, Borrani F. Effects of intermittent hypoxic training performed at high hypoxia level on exercise performance in highly trained runners. J Sports Sci. 2018;136(18):2045-52.
Edvardsen E, Hem E, Anderssen SA. End criteria for reaching maximal oxygen uptake must be strict and adjusted to sex and age: a cross-sectional study. PLoS One. 2014;9:e85276.
Méline T, Solsona R, Antonietti J-P, Borrani F, Candau R, Sanchez AMJ. Influence of post-exercise hot-water therapy on adaptations to training over 4 weeks in elite short-track speed skaters. J Exerc Sci Fit. 2021;19:134–42.
Brewer CP, Dawson B, Wallman KE, Guelfi KJ. Effect of sodium phosphate supplementation on cycling time trial performance and VO2 1 and 8 days post loading. J Sports Sci Med. 2014;13:529–34.
Sanchez AMJ, Borrani F, Le Fur MA, Le Mieux A, Lecoultre V, Py G, et al. Acute supra-therapeutic oral terbutaline administration has no ergogenic effect in non-asthmatic athletes. Eur J Appl Physiol. 2013;113:411–8.
Medbø JI, Mohn AC, Tabata I, Bahr R, Vaage O, Sejersted OM. Anaerobic capacity determined by maximal accumulated O2 deficit. J Appl Physiol Bethesda Md 1985. 1988;64:50–60.
Hill DW, Poole DC, Smith JC. The relationship between power and the time to achieve .VO(2max). Med Sci Sports Exerc. 2002;34:709–14.
Muniz-Pumares D, Pedlar C, Godfrey RJ, Glaister M. Accumulated oxygen deficit during exercise to exhaustion determined at different supramaximal work rates. Int J Sports Physiol Perform. 2017;12:351–6.
Glaister M, Howatson G, Pattison JR, McInnes G. The reliability and validity of fatigue measures during multiple-sprint work: an issue revisited. J Strength Cond Res. 2008;22:1597–601.
Baayen RH, Davidson DJ, Bates DM. Mixed-effects modeling with crossed random effects for subjects and items. J Mem Lang. 2008;59:390–412.
Boisgontier MP, Cheval B. The anova to mixed model transition. Neurosci Biobehav Rev. 2016;68:1004–5.
Judd CM, Westfall J, Kenny DA. Experiments with more than one random factor: designs, analytic models, and statistical power. Annu Rev Psychol. 2017;68:601–25.
Montero D, Lundby C. No improved performance with repeated-sprint training in hypoxia versus normoxia: a double-blind and crossover study. Int J Sports Physiol Perform. 2017;12:161–7.
Millet G, Girard O, Beard A, Brocherie F. Repeated sprint training in hypoxia – an innovative method. Dtsch Z Für Sportmed. 2019;2019:115–22.
de Oliveira-Nunes SG, Castro A, Sardeli AV, Cavaglieri CR, Chacon-Mikahil MPT. HIIT vs. SIT: what is the better to improve V˙O2max? A systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18:13120.
Woorons X, Lemaitre F, Claessen G, Woorons C, Vandewalle H. Exercise with end-expiratory breath holding induces large increase in stroke volume. Int J Sports Med. 2021;42:56–65.
Mulliri G, Sainas G, Magnani S, Roberto S, Ghiani G, Mannoni M, et al. Effects of exercise in normobaric hypoxia on hemodynamics during muscle metaboreflex activation in normoxia. Eur J Appl Physiol. 2019;119:1137–48.
Lam E, Greenhough E, Nazari P, White MJ, Bruce RM. Muscle metaboreflex activation increases ventilation and heart rate during dynamic exercise in humans. Exp Physiol. 2019;104:1472–81.
Kasai N, Mizuno S, Ishimoto S, Sakamoto E, Maruta M, Goto K. Effect of training in hypoxia on repeated sprint performance in female athletes. SpringerPlus. 2015;4:310.
Wang R, Fukuda DH, Hoffman JR, La Monica MB, Starling TM, Stout JR, et al. Distinct effects of repeated-sprint training in normobaric hypoxia and β-alanine supplementation. J Am Coll Nutr. 2019;38:149–61.
Gist NH, Fedewa MV, Dishman RK, Cureton KJ. Sprint interval training effects on aerobic capacity: a systematic review and meta-analysis. Sports Med Auckl NZ. 2014;44:269–79.
Linossier MT, Denis C, Dormois D, Geyssant A, Lacour JR. Ergometric and metabolic adaptation to a 5-s sprint training programme. Eur J Appl Physiol. 1993;67:408–14.
Zinner C, Morales-Alamo D, Ørtenblad N, Larsen FJ, Schiffer TA, Willis SJ, et al. The physiological mechanisms of performance enhancement with sprint interval training differ between the upper and lower extremities in humans. Front Physiol. 2016;7:426.
Pramkratok W, Songsupap T, Yimlamai T. Repeated sprint training under hypoxia improves aerobic performance and repeated sprint ability by enhancing muscle deoxygenation and markers of angiogenesis in rugby sevens. Eur J Appl Physiol. 2022;122:611–22.
Acknowledgements
The authors thank the participants for their cooperation and time.
Funding
No funding was received for this study.
Author information
Authors and Affiliations
Contributions
FB designed the study. MG and RS performed the experiments. FB, AMJS, RS, and MG analyzed the data. AMJS, FB, and RS wrote the manuscript. All authors read and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
No conflict of interest, financial or otherwise, is declared by the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Giovanna, M., Solsona, R., Sanchez, A.M.J. et al. Effects of short-term repeated sprint training in hypoxia or with blood flow restriction on response to exercise. J Physiol Anthropol 41, 32 (2022). https://doi.org/10.1186/s40101-022-00304-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40101-022-00304-1