
Abstract
Background
Actigraphy is a method used for determining sleep (S)/wakefulness (W) by actigraph, a device equipped with a built-in accelerometer and an algorithm validated for each device. The S/W determination algorithm for the waist-worn actigraph FS-760 has been formulated for adults. However, the algorithm for children has not been established. The purpose of this study was to formulate an algorithm for discriminating S/W in school-aged children using FS-760 and to evaluate its validity. We further tested the generalizability of existing algorithm for adults by applying it to the children’s activity data and then examined factors associated with adult algorithm agreement rates by multiple regression analysis using combined adult and children data.
Methods
Sixty-five, healthy, school-aged children (aged 6 to 15 years) were recruited and randomly assigned to two groups: A (n = 33) and B (n = 32). They underwent 8-h polysomnography (PSG) and wore FS-760 simultaneously to obtain activity data. To determine the central epoch of the sleep/wake states (𝑥), a five-order linear discriminant analysis was conducted using the activity intensity of group A for five epochs (𝑥−2, 𝑥−1, 𝑥, 𝑥+1, 𝑥+2; 10 min) and evaluate its accuracy with the activity of group B. To reveal the factors associated with adult algorithm agreement rate, we integrated the activity, age, sleep efficiency of 15 adults (aged 20 to 39 years) and those of 65 children for multiple regression analysis.
Results
The mean agreement rate of the developed algorithm was 91.0%, with a mean sensitivity (true sleep detection rate) of 93.0% and a mean specificity (true wakefulness detection rate) of 63.9%. The agreement rate of the adult algorithm applied to children’s activity was significantly lower (81.8%) than that of the children algorithm. Multiple regression analysis showed that the agreement rates calculated by the adult algorithm were significantly related to mean activity of the 𝑥 epoch in NREM and REM sleep as well as age and sleep efficiency.
Conclusions
The S/W states in school-aged children can be reliably assessed using the developed algorithm for waist-worn actigraph FS-760. Since the accuracy of the adult algorithms decreased when applied it to children which have different activity levels during sleep, the establishment and validation of population-specific S/W algorithms should be required.
Similar content being viewed by others

Background
Polysomnography (PSG) is the gold-standard diagnostic method for evaluating sleep stages; it uses electroencephalography (EEG), electrooculography (EOG), and electromyography (EMG). While PSG can provide a detailed assessment of sleep status, it requires special equipment as well as skilled technicians, and it is hard to examine the long-term and continuous sleep status assessments. The primary sleep assessment method as an alternative to PSG is actigraphy. Actigraphy is a method using an actigraph, a small device equipped with a built-in accelerometer. By applying an activity intensity measured by actigraphs to the algorithm validated for each device [1,2,3,4], it is possible to determine sleep (S)/wakefulness (W). Although actigraphy cannot be used to assess detailed sleep stages, they are less invasive and do not interfere with the one’s living environment, thus making them suitable for screening and long-term sleep/wake recording under real-world situation objectively. In recent years, the use of actigraphy has expanded into various fields in public health studies [5,6,7].
As described, S/W algorithms of actigraphy were validated among various disorders and age groups including children [8,9,10], thus leading to the development of guidelines for diagnosing pediatric sleep disorders [11, 12].
The presence of these guidelines would cause the application of the algorithm only being validated with adults to children’s activity; however, the extrapolation is generally not recommended because of the lack of reliability. In fact, children tend to move a lot during sleep, which may underestimate the total sleep time measured by actigraphs [13]. Considering that children have different activity characteristics during sleep, it would be necessary to formulate a pediatric S/W scoring algorithm.
In addition to differences in overall nocturnal activity, children differ from adults in many aspects, so a multifactorial contribution is assumed if the accuracy of the algorithm is affected. Since children are characterized by weaker motor inhibition in REM sleep [14] and greater sleep need [15, 16], sleep stage-dependent activity, sleep efficiency, and other age-dependent factors may also be involved. It would also lead to accuracy issues in non-pediatric populations where such factors are common (e.g., patients with sleep-related breathing diseases with high activity during nighttime sleep). Therefore, clarifying what characteristics of children are relevant to sleep-wake determination algorithms will provide useful information for understanding methods for estimating sleep-wake from activity levels, as well as for applying the methods to various populations.
In this study, we evaluated the validity of waist-worn actigraph FS-760 (ACOS Co., LTD), which has only been validated with an adult, by formulating an S/W scoring algorithm for healthy, school-aged children. Among the sleep parameters to be estimated, we optimized sleep latency and wake after sleep onset time, as reported by Nakazaki et al. [4]. We also tested the generalizability of the existing algorithm for adults by applying it to the children’s activity data and then examined factors associated with adult algorithm agreement rates by multiple regression analysis using combined adult and children data.
Results
School-aged children S/W scoring algorithm
The S/W scoring algorithm was obtained by performing discriminant analysis using the activity intensity and PSG data (total 6900 epochs) obtained from the 33 participants in group A.
Here, z ≥ 1 denotes wake (WACT) and z < 1 denotes sleep (SACT). 𝑥−2, 𝑥−1, 𝑥, 𝑥+1, and 𝑥+2 indicate the activity intensity at 4 min before the evaluation epoch, at 2 min before the evaluation epoch, at 2 min after the evaluation epoch, and 4 min after, respectively.
Validity of the school-aged children S/W scoring algorithm
The children algorithm formulated in this study was adapted to the activity data of group B, an independent group. The agreement rate, sensitivity, and specificity for each sleep stage were calculated (Table 1). The agreement rate for the entire recording period was 91.04 ± 4.94%, sensitivity 92.95 ± 6.32%, and specificity 63.88 ± 35.82%. In group A, the agreement rate was calculated in the same way. As the results showed no statistically significant differences between the two groups for any of the items, the following analyses were performed with the data by merging both groups.
Optimizing the calculation of sleep parameters with the FS-760
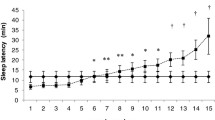
The number of consecutive SACT epochs in the definition of SLACT (see the “Methods” section) ranged 1–10 epochs showed no statistically significant difference between SLACT and SLPSG. When the number of epochs was 4 epochs, ICC was > 0.6 [17] and delta was minimum (Fig. 1). Therefore, the 4 consecutive SACT epoch sequences were adopted as the optimal condition for SLACT. As in SLACT, the ICC was > 0.6 and delta was minimal when the number of consecutive WACT epochs set at 5 for WASOACT (Fig. 2), we adopted it as the optimal condition for WASOACT. The sleep parameters calculated by PSG and activity when optimal conditions (SLACT: n = 4; WASOACT: n = 5) were applied are shown in Table 2. There were no statistically significant difference between the sleep parameters calculated from the PSG data and those from the activity for any of the items; there was a significantly positive ICCs between the two parameters and improved after optimization for all the variables.

Optimization of sleep latency determined by the FS-760 (SLACT). SLACT is the interval between the time lights were turned off and the time of the first SACT (sleep-onset time) among the sleep states that appeared continuously for more than n epoch for the first time after the lights were turned off. The horizontal axis shows the n defined above. The vertical axis shows sleep latency (min) defined for each n. *P < .01 and **P < .001, significant intraclass correlation between sleep latency determined by polysomnography (SLPSG) and SLACT

Optimization of wake after sleep onset determined by the FS-760 (WASOACT). WASOACT is the total time that wake epochs determined by the FS-750 (WACT) appeared continuously for more than n epochs after sleep onset. The horizontal axis shows the n defined above. The vertical axis shows wake after sleep onset (min) defined for each n. †P < .01 and ‡P < .001, significant difference between WASOPSG and WASOACT (paired t-test). Values are expressed as mean ± SE
Accuracy of adult S/W algorithms in school-aged children
Table 3 shows the agreement rate, sensitivity, and specificity for each sleep stage of the S/W scoring, as calculated by adapting adult S/W scoring algorithms to the activity data of 65 children. The accuracy of the adult S/W scoring algorithm was significantly lower than that of the developed algorithm with children, except for the rate of agreement and specificity for Stage W (agreement rate, sensitivity, and specificity are 81.84 ± 8.83%, 81.64 ± 10.62%, and 79.17 ± 28.47%, respectively). On the other hand, the result of adapting the adult scoring algorithm to the activity data of the 15 adults showed that the accuracy was almost the same as that of existing reports [4, 18]: agreement rate 84.41 ± 1.88%, sensitivity 91.15 ± 1.91%, and specificity 53.19 ± 3.96%.
Differences in activity intensity between adults and children
Two-way analysis of variance showed no significant interaction between the group and epochs. However, there was a significant main effect of the group; activity intensity was significantly higher in children than in adults during all sleep stages (W, NREM, and REM) (see Supplemental Fig.).
Searching for factors contributing to the accuracy of the adult S/W algorithm
To clarify the factors related to the agreement rate, we conducted a multiple regression analysis using the agreement rate of the adult algorithm as the objective variable (Table 4). Since the multicollinearity was not violated, all five explanatory variables (age, sleep efficiency, and the average activity of each 𝑥 during Wake, NREM sleep, and REM sleep) were included. Adjusted-R2 (0.720) indicated that the model was judged to be a good fit (F (5,70) = 39.602, P < 0.0001). Agreement rates calculated by the adult algorithm were significantly associated with the mean activity in NREM and REM sleep of 𝑥 epoch as well as age and sleep efficiency. On the other hand, the average activity of 𝑥 epochs of W showed no significant association.
Discussion
In this study, we developed an S/W scoring algorithm for the FS-760 in healthy school-aged children.
First, we established the five-order linear discriminant equation as the S/W scoring algorithm using a total of five epochs of activity, including two epochs before and after, following previous studies using group A’s activity data and PSG’s sleep scoring data. The formulated S/W scoring algorithm was applied to the activity data of group B, which was an independent population with no difference in age, sex, or body size, to determine S/W. The results showed that the agreement with PSG data was 90.92 %. Out result was comparable to the agreement rates which have been reported in the range of 85 to 96% [1,2,3,4, 19,20,21,22]. The sensitivity and specificity also showed a trend of high sensitivity and low specificity, as in many previous reports [1,2,3,4, 20, 21].
One of the problems with the use of actigraphs has been pointed out the difficulty in detecting wake [23, 24]. In particular, it was difficult for actigraphy to distinguish silent awakeness from sleep based on the activity [1, 21, 25, 26]. When using the algorithm developed in this study, the specificity with PSG data was approximately 63%, which is a little lower than that reported for the FS-760 adult algorithm (65%) [4] but approximately the similar or higher than in the other previous reports (34–58%) [3, 21, 27]. In this study, optimization of the definition of sleep parameters was conducted following previous studies; the optimal settings were four consecutive epochs for sleep onset latency and five consecutive epochs for wake after sleep onset. When the sleep variables were recalculated by adapting this optimization, there was no longer a significant difference in those calculated by PSG in all sleep variables (SL, WASO, TST, and SE). Thus, the sleep variables calculated using this algorithm were reasonable. Note that the data used in this study were obtained from the first night PSG, so it is likely that the first night effect [28] is occurring in WASO.
To examine the generalizability of the adult S/W scoring algorithm, we applied it to the activity data of 65 school-aged children in the present study; then, S/W scoring was conducted. The overall agreement rate of the adult S/W algorithm was significantly lower than that of the school-aged children. Although the accuracy of specificity increased by approximately 12 points, the accuracy of the other parameters decreased by approximately 10 points.
To clarify the factors associated with this decreased inaccuracy, multiple regression analysis was conducted using the agreement rate of adult algorithm as the objective variable with integrated the 80 data of adults and children. Results showed that the average amount of activity during sleep, sleep efficiency, and age were significantly associated. Since children were more active during sleep, their S/W determination algorithm must use a high threshold to determine W. In fact, the coefficients of their S/W scoring algorithm was smaller than those of the adult algorithm. When the adult S/W scoring algorithm with the lower threshold was applied to the children’s activity data, the probability of being scored as W, with a discrimination score z ≥ 1, further increases. It has been reported that children shifted their body position during sleep more frequently than adults [13], and that the accuracy of S/W scored by the actigraph was lower [8, 10]. Considering that there are differences in the amount of activity during sleep between children and adults, and that the activity during sleep was also a major determinant of accuracy during the multiple regression analysis, the population with higher activity levels during sleep due to concomitant sleep disorders including sleep apnea, and inappropriate sleep environment (noise, inappropriate temperature/humidity/bedding, etc.) were highly likely to show the similar inaccuracy. For the population, it was necessary to validate a unique S/W determination algorithm that considers population activity characteristics. A low accuracy has been reported in such populations [24, 29]. As revealed by the multiple regression analysis in this study, age and sleep efficiency may have contributed to the accuracy, which were independent of activity. These results were consistent with existing studies [30].
Although the results of this study indicated the need to validate a unique S/W determination algorithm for children, there were reports showing that the accuracy of the adult algorithm may be maintained even when adapted to children. In these reports, the agreement rate with PSG were 87–90% [9, 29, 31, 32]. One possible factor causing difference between these reports and the present study is the site of attachment of the actigraph. The previous reports attached actigraphs to the non-dominant wrist (extremity region) while we attached it the waist (lumbar region) in the present study. Differences in the activity intensity depending on the attached site have also been reported. Previous reports have shown lower activity in the trunk than in the wrist [33]. Position shifts during sleep were more common in children than in adults [13]; since the actigraph FS-760 measured the activity of the trunk, the amount of body movements during sleep, which is usually small in adults compared to the peripheral, is relatively large in children. This may account for the discrepancy with the results of the previous studies. On the contrary, Paavonen et al. reported that in children aged 7–12 years, the actigraph is equally accurate at the wrist and the waist [34], suggesting the discrepancy may depend on the device characteristics.
As mentioned above, the amount of activity may differ between the wrist and trunk, and the accuracy of the actigraph may vary. However, the results of this study indicate that a waist-worn actigraph has sufficient accuracy to determine the S/W as well as a wrist-worn actigraph. Wearing the actigraph on the waist is less burdensome and less conspicuous compared to the wrist. Therefore, waist-worn actigraph is considered more applicable to children who are not accustomed to wearing wristwatches.
This study has several limitations: the children included in this study were 6–15 years old; only elementary to middle-school students were included in the study. Therefore, preschoolers, including newborns, should also be considered in future studies. In addition to age, only healthy subjects without sleep disturbances were included in this study. Because the actigraph used in this study was worn on the trunk, it may be necessary to examine the differences in the wearing site in future studies. FS-760 is a simple wearable device that can measure only activity intensity. In the future, it is one of the possibilities to consider further enhancing its accuracy as a multi-wearable device by combining it with a heart rate monitor and other devices [35]. The time epoch for the FS-760 used in this study is 2 min; 4 consecutively scored sleep stages (1 epoch = 30 s) were re-classified as either sleep (sleep epochs determined by PSG, SPSG) or wake (wake epochs determined by PSG, WPSG) every 2 min. So it is possible that Wpsg is more likely to contain obvious wakes rather than W in PSG, and that this procedure may lead the high specificity.
Conclusion
In this study, we developed an algorithm for the S/W scoring of a waist-worn actigraph FS-760 in school-aged children. The resultant algorithm was then validated using PSG data to determine whether its accuracy in children was similar to that in the adults. We also examined the differences between the resultant and established adult algorithms and clarified the importance of validating the scoring algorithm for specific population. Our results may be applied in the fields of sleep re-exploration and sleep medicine in the future, particularly in interventions targeted for school-aged children.
Methods
Formulation of the algorithm for school-aged S/W scoring
Subjects
Sixty-seven school-aged children participated in this study. Screening PSG, questionnaires and medical examination of children and their caregivers confirmed that the participants had no severe mental, physical, or sleep disorders. Two children who were unable to complete the protocol were excluded from the analyses. Finally, we recruited 65 children (41 boys, 24 girls; mean age 10.5 ± 2.6 years, aged 6 to 15 years) for this study. Following the split-sample method [36], they were randomly assigned to two groups: group A (33 participants) and group B (32 participants). There were no significant differences in %male, age, height, weight, and BMI between groups (Table 5).
Procedure
This study was conducted in the sleep laboratory unit of the National Institute of Mental Health, National Center of Neurology and Psychiatry. We simultaneously recorded the sleep state and activity intensities during sleep using PSG and actigraphy.
PSG recording
The lights-out time in the laboratory was determined according to the participants’ habitual bedtime in their home records (sleep diary) preceding the experiments. In principle, the time in bed was set at 7 h; subjects were instructed to not get up if they woke up in the middle of the night and to get as much sleep as possible until lights-on. For those whose bedtime exceeded 7 h, data from the first 7 h were used for analysis; for those whose bedtime was less than 7 h, all data were used for analysis. The unit was maintained at 25°C and 50% relative humidity (RH). PSG recordings were made using Neurofax digital EEG system (EEG-1200, Nihon Kohden, Tokyo, Japan), which included an EEG with a conventional montage (F3, F4, C3, C4, O1, O2) based on the contralateral mastoid (M1, M2), an EOG at the outer canthus of each eye, a submental EMG, and an electrocardiogram (ECG). Upon recording, the EEG, EOG, EMG, and ECG signals were digitized at 200 Hz; the signal was filtered using a high-pass filter with the following time constants: EEG 0.3 s, EOG 0.03 s, submental EMG 0.03 s, and ECG 1.0 s. The signal was filtered using a low-pass filter as following: EEG 60 Hz, EOG 60 Hz, submental EMG 60 Hz, and ECG 60 Hz. The sleep stage (Stage N1, Stage N2, Stage N3, Stage R, or Stage W) was determined every 30 s according to the American Academy of Sleep Medicine (AASM) Manual for the scoring of sleep and associated events [37]. Four consecutively scored sleep stages (1 epoch = 30 s) were re-classified as either sleep (sleep epochs determined by PSG, SPSG) or wake (wake epochs determined by PSG, WPSG) every 2 min; they corresponded with the activity intensity data measured by the FS-760 (1 epoch = 2 min). When four consecutive data contained two or more Stage W parameters, the dataset was classified as wake (WPSG) according to the definition adopted by previous studies [2,3,4, 38]. On the other hand, all other datasets were classified as sleep datasets (SPSG). Furthermore, SPSG was sub-classified as Stage R, Stage N1, Stage N2, or Stage N3, according to the most frequent sleep stage in the epoch (e.g., when SPSG contained three or more Stage N1 data, it was classified as Stage N1). However, when SPSG contained two different stages, the priority order (Stage R → Stage N1 → Stage N2 → Stage N3) was used (e.g., when SPSG contained two stages N1 and R, it was classified as Stage R).
Activity recording with the FS-760
Activity during the night was recorded using the waist-worn FS-760 (ACOS CO., LTD, Nagano, Japan). This small, rectangular device had the same accelerometer as that in the FS-750, which was validated by Nakazaki et al. for adults [4].
Briefly, the FS-760 is equipped with a three-axis accelerometer, which count the number of times the acceleration exceeds a reference value every 0.125 s and sums it at 2-min intervals. From this record, 32 levels of activity intensity are calculated and stored.
Formulation of the algorithm for S/W scoring
To develop an algorithm for the FS-760 that determines the S/W states, a five-dimensional linear model was adopted according to previous studies [3, 4]. We hypothesized that this model utilizes activity intensity at an evaluation epoch as well as two epochs before and two epochs after (total of 10 min). Using the activity intensity at 4 and 2 min before the evaluation epoch, at the evaluation epoch, and at 2 and 4 min after the epoch (𝑥−2, 𝑥−1, 𝑥, 𝑥+1, 𝑥+2), each with a weighting coefficient (𝑎−2, 𝑎−1, 𝑎, 𝑎+1, 𝑎+2), the following equation gives composite variable z, which is the discriminant score:
The criteria for the linear discriminant equation were SPSG (= 0) and WPSG (= 1) obtained with PSG (1 epoch = 2 min). The coefficients for classifying the activity intensity obtained from the FS-760 into sleep (SACT) and wakefulness (WACT) according to the above formula were obtained by linear discriminant analysis using a data set containing activity intensity and PSG data from 33 subjects in Group A. We adopt the split-sample method for this study [36].
Validity of the school-aged children S/W scoring algorithm
Using the newly developed S/W scoring algorithm, the overall agreement rate, sensitivity, and specificity were calculated for the entire recording period as well as for each sleep stage (Stage N1, Stage N2, Stage N3, Stage R, or Stage W) for each participant in group B. These parameters indicated how sleep scores by PSG (SPSG, WPSG) closely match the estimates by activity intensity (SACT, WACT) for each corresponding epoch. Sensitivity was defined as the ratio of SACT to SPSG during the entire recording period. Specificity was defined as the ratio of WACT to WPSG during the entire recording period. The agreement rate for each sleep stage determined by PSG (Stage N1, Stage N2, Stage N3, Stage R, or Stage W) was defined as the percentage of activity intensity scores (SACT or WACT) that closely match those calculated for each sleep stage. Similarly, the agreement rate in group A was calculated; it was considered whether there was any difference from the agreement rate in group B.
Optimization of the definition of sleep parameters
Sleep latency (SL), total sleep time (TST), wake after sleep onset (WASO), and sleep efficiency (SE) were calculated using the S/W data obtained from the PSG and activity intensity data for each 2-min epoch [37].
The definitions of sleep parameters calculated from the PSG data are as follows: (1) SLPSG: the interval between the time of lights-off and the time of the first epoch when any of the sleep stages appeared (sleep-onset time); (2) TSTPSG: the total time period when sleep (SPSG) appeared from the time of sleep onset to the time of lights-on; (3) WASOPSG: time of (Time in bed (TIB) – (SLPSG + TSTPSG); and (4) SEPSG: the ratio of TSTPSG to TIB.
The definitions of sleep parameters calculated from the activity intensity data are as follows: (1) SLACT: the interval between the time of lights-off and the time of the first SACT (sleep-onset time) among the sleep states that appeared continuously for more than n epochs for the first time after the time of lights-off, where n ranged from 1 to 10 (2 to 20 min) and the SLACT was calculated for each occurrence; (2) WASOACT: the total time of WACT that appeared continuously for more than n epochs after (optimized) sleep onset, where n ranged from 1 to 10 (2 to 20 min) and the WASOACT was calculated for each occurrence. When WACT appeared continuously for more than n epochs, the epochs were defined as WACT; (3) TSTACT: TIB from which SLACT and WASOACT were subtracted; and (4) SEACT: the ratio of TST to TIB.
For the calculation of SLACT and WASOACT, the values obtained from the criteria applied above to the values of SLPSG and WASOPSG were compared; the epoch numbers that would optimize the calculated results were sought. The optimization rules were to minimize the difference between the average parameter values obtained by PSG for the 65 participants and the average parameter values obtained from the S/W algorithm, such that the difference was not significant. The intraclass correlation coefficient (ICC) was considered sufficient when the ICC was ≥ 0.6 [17].
Accuracy of adult S/W algorithms in children
To confirm whether the accuracy of the existing algorithm for FS760, which was established with adults, can be used for children, the algorithm of Nakazaki et al. [4] was adapted to the activity data of our subjects (65 children). After adaptation, we calculated the agreement rate, sensitivity, and specificity of PSG S/W scoring for the entire recording period and each sleep stage (Stage W, Stage N1, Stage N2, Stage N3, and Stage R).
Differences in activity intensity between adults and children
As a background factor for using different algorithms for children and adults, we compared differences in the amount of activity during sleep between children and adults. Differences in activity intensity between adults and children according to sleep stage (Wake, NREM, and REM) were compared.
Searching for factors contributing to the accuracy of the adult S/W algorithm
To identify the factors associated with adult S/W scoring agreement rates in the activity data, we used concurrently recorded PSG and activity data from 17 adults who participated in the other studies as well as those from 65 children of this study. Of the 17 adults, one with an apnea hypopnea index (AHI) > 5 and another with periodic limb movement index (PLMI) > 15 were excluded; finally, 15 adults (14 males and 1 female, mean age 26.8 ± 6.0 years, aged 20 to 39 years) were included in the analysis. Activity data of adults were acquired using FS-760 or compatible actigraph MTN-220 (ACOS CO., LTD) [39] and processed in the same way as for the children. The adult S/W scoring algorithm was applied to the activity data of 80 people; the agreement rate was then calculated. Multiple linear regression was conducted to reveal the factors associated with the agreement rates using the adult S/W scoring algorithm with age, sleep efficiency, and the average activity of each 𝑥 when 𝑥 was Wake, NREM sleep, and REM sleep.
Statistics
Unpaired t-tests were used to compare the sensitivity, specificity, and agreement rates between groups A and B for both the entire recording period and each sleep stage. Paired t-tests and ICC were performed to compare sleep parameters determined from PSG and activity intensity data obtained before and after the application of the optimization rules. Two-way analysis of variance with group (adult/ children)✕ epoch (𝑥−2, 𝑥−1, 𝑥, 𝑥+1, 𝑥+2) was used for the comparison of differences in activity intensity between adults and children. Multiple linear regression analysis was performed using the forced entry method. All data are expressed as the mean ± SD. All statistical analyses were performed using R (version 3.6.1; R Foundation) and IBM SPSS Statistics (version 26.0; IBM). Statistical significance was set at P < 0.05.
Availability of data and materials
The datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- AHI:
-
Apnea and hypopnea index
- ECG:
-
Electrocardiogram
- EEG:
-
Electroencephalogram
- EMG:
-
Electromyogram
- EOG:
-
Electrooculogram
- ICC:
-
Intraclass correlation coefficient
- PLMI:
-
Periodic limb movement index
- PSG:
-
Polysomnography
- RH:
-
Relative humidity
- SACT :
-
Sleep epochs determined by the FS-760
- SE:
-
Sleep efficiency
- SL:
-
Sleep latency
- SLACT :
-
Sleep latency determined by the FS-760
- SLPSG :
-
Sleep latency determined by PSG
- SPSG :
-
Sleep epochs determined by PSG
- S/W:
-
Sleep/wake
- TIB:
-
Time in bed
- TST:
-
Total sleep time
- WACT :
-
Wake epochs determined by the FS-760
- WASO:
-
Wake after sleep onset
- WASOACT :
-
Wake after sleep onset determined by the FS-760
- WASOPSG :
-
Wake after sleep onset determined by PSG
- WPSG :
-
Wake epochs determined by PSG
References
Cole RJ, Kripke DF, Gruen W, Mullaney DJ, Gillin JC. Automatic sleep/wake identification from wrist activity. Sleep. 1992;15(5):461–9.
Sadeh A, Sharkey KM, Carskadon MA. Activity-based sleep-wake identification: an empirical test of methodological issues. Sleep. 1994;17(3):201–7.
Enomoto M, Endo T, Suenaga K, Miura N, Nakano Y, Kohtoh S, et al. Newly developed waist actigraphy and its sleep/wake scoring algorithm. Sleep Biol Rhythms. 2009;7:17–22.
Nakazaki K, Kitamura S, Motomura Y, Hida A, Kamei Y, Miura N, et al. Validity of an algorithm for determining sleep/wake states using a new actigraph. J Physiol Anthropol. 2014;33:31.
Enomoto M, Tsutsui T, Higashino S, Otaga M, Higuchi S, Aritake S, et al. Sleep-related problems and use of hypnotics in inpatients of acute hospital wards. Gen Hosp Psychiatry. 2010;32(3):276–83.
Sadeh A, Dan O, Bar-Haim Y. Online assessment of sustained attention following sleep restriction. Sleep Med. 2011;12(3):257–61.
Meltzer LJ, Montgomery-Downs HE, Insana SP, Walsh CM. Use of actigraphy for assessment in pediatric sleep research. Sleep Med Rev. 2012;16(5):463–75.
Bélanger MÈ, Bernier A, Paquet J, Simard V, Carrier J. Validating actigraphy as a measure of sleep for preschool children. J Clin Sleep Med. 2013;9(7):701–6.
Meltzer LJ, Wong P, Biggs SN, Traylor J, Kim JY, Bhattacharjee R, et al. Validation of actigraphy in middle childhood. Sleep. 2016;39(6):1219–24.
Sitnick SL, Goodlin-Jones BL, Anders TF. The use of actigraphy to study sleep disorders in preschoolers: Some concerns about detection of nighttime awakenings. Sleep. 2008;31(3):395–401.
Morgenthaler T, Alessi C, Friedman L, Owens J, Kapur V, Boehlecke B, et al. Practice parameters for the use of actigraphy in the assessment of sleep and sleep disorders: an update for 2007. Sleep. 2007;30(4):519–29.
Smith MT, McCrae CS, Cheung J, Martin JL, Harrod CG, Heald JL, et al. Use of actigraphy for the evaluation of sleep disorders and circadian rhythm sleep-wake disorders: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2018;14(7):1231–7.
De Koninck J, Lorrain D, Gagnon P. Sleep positions and position shifts in five age groups: an ontogenetic picture. Sleep. 1992;15(2):143–9.
Kohyama J, Shimohira M, Iwakawa Y. Maturation inhibition in of motility and motor rapid-eye-movement sleep. Neurobiol Resemch. 1997;130(1):117–22.
Ohayon MM, Carskadon MA, Guilleminault C, Vitiello MV. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals: developing normative sleep values across the human lifespan. Sleep. 2004;27(7):1255–73.
Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National sleep foundation's sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40–3.
Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropractic Med. 2016;15(2):155–63.
Nattala P, Leung KS, Abdallah AB, Cottler LB. Heavy use versus less heavy use of sedatives among non-medical sedative users: characteristics and correlates. Addict Behav. 2011;36(1-2):103–9.
Webster JB, Kripke DF, Messin S, Mullaney DJ, Wyborney G. An activity-based sleep monitor system for ambulatory use. Sleep. 1982;5(4):389–99.
Jean-Louis G, Kripke DF, Cole RJ, Assmus JD, Langer RD. Sleep detection with an accelerometer actigraph: comparisons with polysomnography. Physiol Behav. 2001;72(1-2):21–8.
de Souza L, Benedito-Silva AA, Pires ML, Poyares D, Tufik S, Calil HM. Further validation of actigraphy for sleep studies. Sleep. 2003;26(1):81–5.
Acebo C, MK LB. Actigraphy. Respir Care Clin N Am. 2006;12(1):23–30 viii.
Lichstein KL, Stone KC, Donaldson J, Nau SD, Soeffing JP, Murray D, et al. Actigraphy validation with insomnia. Sleep. 2006;29(2):232–9.
Marino M, Li Y, Rueschman MN, Winkelman JW, Ellenbogen JM, Solet JM, et al. Measuring sleep: Accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36(11):1747–55.
Paquet J, Kawinska A, Carrier J. Wake detection capacity of actigraphy during sleep. Sleep. 2007;30(10):1362–9.
Van De Water ATM, Holmes A, Hurley DA. Objective measurements of sleep for non-laboratory settings as alternatives to polysomnography - a systematic review. J Sleep Res. 2011;20(1 PART II):183–200.
Tryon WW. Issues of validity in actigraphic sleep assessment. Sleep. 2004;27(1):158–65.
Jr AH, WB W, RL W. The first night effect: an EEG study of sleep. Psychophysiology. 1966;2(3):263–6.
Hyde M, O'Driscoll DM, Nette SBI, Galang C, Tan SK, Verginis N, et al. Validation of actigraphy for determining sleep and wake in preterm infants. J Sleep Res. 2007;16(1):213–6.
Blackwell T, Redline S, Ancoli-Israel S, Schneider JL, Surovec S, Johnson NL, et al. Comparison of sleep parameters from actigraphy and polysomnography in older women: The SOF study. Sleep. 2008;31(2):283–91.
Galland BC, Kennedy GJ, Mitchell EA, Taylor BJ. Algorithms for using an activity-based accelerometer for identification of infant sleep-wake states during nap studies. Sleep Med. 2012;13(6):743–51.
Meltzer LJ, Walsh CM, Traylor J, Westin AML. Direct comparison of two new actigraphs and polysomnography in children and adolescents. Sleep. 2012;35(1):159–66.
Middelkoop HA, van Dam EM, Smilde-van den Doel DA, Van Dijk G. 45-hour continuous quintuple-site actimetry relations between trunk N Limb. Psychophysiology. 1997;34:199–203.
Paavonen EJ, Fjällberg M, Steenari MR, Aronen ET. Actigraph placement and sleep estimation in children. Sleep. 2002;25(2):235–7.
Burkart S, Beets MW, Armstrong B, Hunt ET, Dugger R, von Klinggraeff L, et al. Comparison of multichannel and single-channel wrist-based devices with polysomnography to measure sleep in children and adolescents. J Clin Sleep Med. 2021;17(4):645–52.
Picard RR, Berk KN. Data splitting. Am Stat. 1990;44(2):140–7.
Berry RB, Albertario C, Harding S, et al; For the American Academy of Sleep Medicine. The AASM manual for the scoring of sleep and associated events: rules, terminology and technical specifications, Version 2.5. Darien: American Academy of Sleep Medicine; 2018.
Lotjonen J, Korhonen I, Hirvonen K, Eskelinen S, Myllymaki M, Partinen M. Automatic sleep-wake and nap analysis with a new wrist worn online activity monitoring device vivago WristCare. Sleep. 2003;26(1):86–90.
Marzano C, Ferrara M, Sforza E, De Gennaro L. Quantitative electroencephalogram (EEG) in insomnia: a new window on pathophysiological mechanisms. Curr Pharm Des. 2008;14(32):3446–55.
Acknowledgements
The authors would like to thank N. Takano and Y. Sema for their assistance in conducting the experiments.
Funding
This work was supported by JSPS KAKENHI Grant Number 15H02426,17K07597, and 21K06368.
Author information
Authors and Affiliations
Contributions
SK conceived and designed the study. KN and SK conducted the study. ME and SK performed the statistical analysis. ME drafted the manuscript. SK contributed to drafting the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the National Center of Neurology and Psychiatry (#A2020-112), and written consent was obtained from all children’s caregivers.
Consent for publication
“Not applicable”
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
A description of this figure is provided in the text.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Enomoto, M., Kitamura, S. & Nakazaki, K. Validity of an algorithm for determining sleep/wake states using FS-760 in school-aged children. J Physiol Anthropol 41, 29 (2022). https://doi.org/10.1186/s40101-022-00303-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40101-022-00303-2