
Abstract
Background
He long noncoding RNA small nucleolar host RNA 5 (SNHG5) is highly expressed in many cancers, and there is a notable correlation between the elevated expression of SNHG5 and survival outcome in cancer patients. The objective of this study was to conduct a meta-analysis to evaluate the correlation between SNHG5 expression and the clinical outcome of cancer patients.
Methods
Six relevant electronic databases were exhaustively searched, and, depending on the inclusion and exclusion criteria, appropriate literature was obtained. The Newcastle-Ottawa Scale (NOS) score was utilized to evaluate the quality of the research for every article included, and pertinent data from each study were carefully extracted. Hazard ratios (HRs), odds ratios (ORs) and 95% confidence intervals (CIs) were combined to explore the association of SNHG5 expression levels with cancer prognosis, and sensitivity analyses and assessments of publication bias were also conducted to investigate any possibility in the publication of the studies.
Results
Eleven studies encompassing 721 patients were ultimately collected. When combined, the hazard ratios (HRs) revealed a substantial direct correlation between elevated SNHG5 expression and an unfavourable prognosis for cancer patients (HR = 1.90, 95% CI 0.87–4.15); however, the correlation did not reach statistical significance. Furthermore, high SNHG5 expression was predictive of advanced TNM stage (OR: 1.988, 95% CI 1.205–3.278) and larger tumour size (OR: 1.571, 95% CI 1.090–2.264); moreover, there were nonsignificant relationships between SNHG5 expression and DM (OR: 0.449, 95% CI 0.077–2.630), lymph node metastasis (OR: 1.443, 95% CI 0.709–2.939), histological grade (OR: 2.098, 95% CI 0.910–4.838), depth of invasion (OR: 1.106, 95% CI 0.376–3.248), age (OR: 0.946, 95% CI 0.718–1.247) and sex (OR: 0.762, 95% CI 0.521–1.115).
Conclusion
SNHG5 expression is typically increased in the majority of tumour tissues. Elevated SNHG5 expression may indicate poor prognosis in cancer patients. Therefore, SNHG5 is a promising potential therapeutic target for tumours and a reliable prognostic biomarker.
Similar content being viewed by others


Introduction
Cancer has caused social and public problems that cannot be ignored, with huge economic losses and mental burdens to people all over the world every year [1, 2]. Based on the 2021 Cancer Statistics Report, the numbers of individuals newly diagnosed with cancer and dying from cancer in 2020 will be approximately 19.84 million and 10 million, respectively [3, 4]. Despite the well-being and satisfaction of cancer patients having improved to a certain extent alongside advancements in molecular biology technology and medical care, the 5-year survival rate for cancer patients has remained unsatisfactory [5, 6]. The main reason is that classic treatment methods such as chemotherapy, radiation therapy, hormone therapy and targeted therapeutics are already in their prime, and it is difficult for these methods to improve survival [7,8,9,10]. Therefore, novel therapeutic targets aimed at improving the prognosis of cancer patients are urgently needed [11,12,13].
Over the past few years, the employment of high-throughput sequencing techniques and advancements in molecular biology have gradually revealed an increasing number of genes that are intricately linked to cancer. Additionally, a growing body of evidence has confirmed the involvement of numerous noncoding RNAs in the initiation and progression of cancer [14, 15]. Noncoding RNAs are a class of small molecular compounds that lack the ability to encode proteins [16,17,18]. They are called the "useless product" of genetic material and account for 95–98% of human genetic material [19]. Although noncoding RNAs do not perform the biological function of encoding proteins, there is substantially more evidence that noncoding RNAs can exert their control over the biological behaviour of cells by influencing the expression of cell-coding genes at various levels, encompassing gene transcription, post-transcriptional translation, and epigenetic regulation [20,21,22]. Noncoding RNAs can affect the proliferation, invasion and apoptosis of tumour cells, thereby affecting the progression of tumours. For example, Professor Yang showed that low expression of lncRNA-BANCR can significantly stimulate the growth and motility of lung cancer cells and suppress programmed cell death, thereby contributing to the initiation and progression of lung cancer [23]. Professor Yan stated that high expression of lnc-SNHG6 can significantly suppress the programmed cell death (apoptosis) of gastric cancer cells, stimulate their proliferation, migration, and invasion, and exhibit a strong correlation with an unfavourable prognosis [24]. Noncoding RNA are being considered by more and more researchers as promising targets and prognostic indicators for future cancer therapies.
Lnc-SNHG5 is a category of low-molecular-weight compounds characterized by more than 200 nucleotide units that lack protein coding ability [25]. An increasing number of studies have shown that SNHG5 is differentially expressed across various tumour cell types and is implicated in the aetiology and progression of diverse cancers [26, 27]. For example, Professor Wei showed that SNHG5 is abundantly expressed in oesophageal cancer tissues and that elevated SNHG5 levels can enhance the proliferative and migratory potential of oesophageal squamous cell carcinoma (ESCC) cells, suppress cellular apoptosis, and consequently promote the progression of ESCC [28]. Professor Kang reported that SNHG5 is overexpressed in lung cancer, where its high expression facilitates the movement and infiltration of lung cancer cells while suppressing their apoptosis. Furthermore, numerous studies have increasingly indicated a significant association between elevated SNHG5 expression and poor lung cancer prognosis [29]. Inconsistencies across different studies involving relatively small numbers of patients have made conclusions questionable; even though some outcome indicators have suggested that SNHG5 is a poor prognostic marker, the differences did not reach statistical significance. Hence, the objective of this investigation was to conduct a meta-analysis to investigate the potential correlation between the expression level of SNHG5 and cancer prognosis.
Materials and methods
Inclusion of appropriate literature
Utilizing the reporting guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) as the foundation for our reporting format, a comprehensive search was performed by browsing relative databases such as PubMed, Embase, the Web of Science, the Cochrane Library, Google Scholar, the China National Knowledge Infrastructure (CNKI) and the Wanfang Database from the establishment of the database to January 1, 2023. The retrieval strategies used in this study were as follows: “Small nucleolar RNA host gene 5” OR “lncRNA Small nucleolar RNA host gene 5” OR “lncRNA SNHG5” OR “SNHG5” OR “lncSNHG5”) AND “cancer” OR “carcinoma” OR “prognosis” OR “survival” OR “survival prognosis.” We also consulted the references of the included publications in detail to obtain useful and appropriate publications.
Inclusion and exclusion criteria
Publications that fulfilled the following criteria were deemed appropriate for inclusion in this meta-analysis: (1) the fundamental purpose of the literature review was to evaluate the relationship between SNHG5 expression levels and cancer prognosis; (2) patients were divided into two distinct groups based on their expression level (high or low); (3) the research subjects were limited to human patients; (4) provided enough raw data to be extracted. Studies with the following characteristics were considered unsuitable for inclusion in this meta-analysis: (1) lacked sufficient data; (2) the participants were animals; (3) literature reviews, meta-analyses, case reports, conference summaries, and research not officially published; (4) non-English language publications.
NOS score of included studies
The Newcastle-Ottawa Scale (NOS) score, which includes eight items, was utilized for evaluating the overall quality of the studies included [30]. Two researchers meticulously and independently assessed the quality of every included article, taking into consideration the aforementioned NOS score. If the evaluation results were not consistent, an agreement was reached through discussion or a third researcher was consulted for discussion and confirmation. The total NOS score ranged from 0 to 9. Articles with a score of 6 or more were considered high-quality documents and suitable for inclusion in this study. Articles with a score less than 6 points were considered low-quality studies and were excluded from this investigation.
Data extraction
The useful raw data were obtained by two researchers independently, and the detailed information included the name of the primary author, the year the article was published, the total number of patients involved, the reference gene, the cutoff value, and the country to which the patient belonged. We also extracted the main outcome indicators, including overall survival (OS) and relapse-free survival (RFS). Furthermore, secondary outcome indicators, including TNM stage, lymph node metastasis (LNM) status, distant metastasis(DM) status, tumour dimensions, histological grade, depth of infiltration, chronological age and sex, were obtained. If the survival data provided in the publication included multivariate analysis and univariate analysis, only multivariate analysis was obtained; for example, if the study only included the survival curve, then the detailed survival data were obtained utilizing Engauge Digitizer V 4.1 software, and the study included the time-dependent survival rates of both the high- and low-expression groups of SNHG5 [31].
Statistics and analysis
RevMan V 5.4 software and STATA V 12.0 software were used to perform the statistical analysis of this meta-analysis. Patients were categorized into either a high-expression group or a low-expression group according to the original literature reports. The combination of the odds ratio (OR) with 95% confidence interval (CI) was used to evaluate the associations between SNHG5 expression and TNM stage, LNM, DM, tumour size, etc. The combination of the hazard ratio (HR) and 95% confidence interval (CI) was used to evaluate the relationship between SNHG5 expression and cancer prognosis, including OS and RFS. If I2 (I-square) < 50% and P > 0.05, the result was considered to indicate insignificant heterogeneity, and a fixed effects model was used. If I2 > 50% and P < 0.05 were significant, significant heterogeneity was considered. A random effects model was used, and subgroup analysis was conducted based on cancer type (digestive system and nondigestive tract), number of patients (fewer than 60 patients and no less than 60 patients), follow-up month (fewer than 60 and no less than 60), cutoff value (mean and median), and data analysis method (multivariate analysis and univariate analysis). Sensitivity analysis was conducted using STATA software to assess whether the results of individual studies had a significant impact on the overall findings. Additionally, Begg's analysis was employed to detect any significant publication bias in the original study.
Results
Characteristics of the enrolled publications
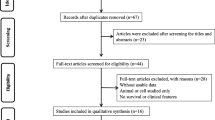
After the systematic and detailed searches, 127 publications were initially obtained, 32 duplicate documents were found, 68 articles were excluded for not exploring the relationship between SNHG5 expression and cancer prognosis, 6 publications were excluded for involving animal experimentation, 8 articles lacked sufficient data, and 2 non-English papers were also excluded. Finally, 11 suitable investigations involving 721 patients were included in this meta-analysis (Fig. 1). The cancer types included bladder cancer [32], hepatocellular carcinoma [33], cervical cancer [34], osteosarcoma [35], nasopharyngeal carcinoma [36], non-small cell lung cancer [29], oesophageal cancer [28], diffuse large B-cell lymphoma [37], and gastric cancer [38, 39]. All the patients were Chinese, and the number of patients in each study varied between 32 and 90; seven [7] papers provided survival data (Table 1). According to the NOS score, the enrolled studies ranged from 7 to 8, indicating that all the papers were suitable for enrolment and analysis (Table 2).

Literature search and inclusion process
The correlation between SNHG5 expression and survival outcome
Seven studies involving a total of 425 patients were obtained to evaluate the correlation between SNHG5 expression and cancer prognosis. A positive correlation was revealed between elevated SNHG5 expression and poor survival outcome (HR = 1.90, 95% CI 0.87–4.15) (Fig. 2), but the correlation was not statistically significant. Considering the inconsistent results of SNHG5 expression in patients with different tumour types, a subgroup analysis was conducted, taking into account cancer type, sample size, cutoff value, follow-up duration, hazard ratio (HR) statistics, and analysis method. The findings indicated that elevated SNHG5 expression was associated with a poorer cancer prognosis, specifically in patients with nondigestive system cancers (HR = 2.54, 95% CI 1.18–5.48); multivariate analysis was also performed (HR = 4.84, 95% CI 2.42–9.70), and the mean cutoff value was 2.82, 95% CI 1.13–7.04. Moreover, there was an insignificant relationship between SNHG5 expression and OS in the digestive system subgroup according to cancer type (HR = 1.45, 95% CI 0.42–4.96); univariate analysis was also performed (HR = 1.31, 95% CI 0.58–2.99), and the median cutoff value was 1.79, 95% CI 0.74–4.30 (Table 3). In addition, the results of one original study demonstrated that increasing SNHG5 expression might contribute to poor DFS (hazard ratio (HR): 3.690, 95% CI 1.229–11.082) (Table 3).

Forest plot of SNHG5 expression and survival outcome in cancers. A OS; B DFS
The correlation between SNHG5 expression and TNM stage
Eight original studies comprising 527 patients were included in this study to explore the correlation between SNHG5 expression and TNM stage. A pooled OR with 95% CI was used to determine the strong positive correlation between high SNHG5 expression and advanced TNM stage (OR = 1.988, 95% CI 1.205–3.278) (Fig. 3). Due to inconsistencies in cancer types between different primary studies, subgroup analyses were also performed. The results of subgroup analysis demonstrated that increasing SNHG5 expression predicted advanced TNM stage in the nondigestive system subgroup (OR = 2.617, 95% CI 1.686–4.061), and an insignificant correlation was observed in the digestive system subgroup (OR = 1.237, 95% CI 0.560–2.733) (Table 4).

Forest plot of SNHG5 expression and TNM stage in cancers
The correlation between SNHG5 expression and LNM
Four papers with 270 cases were obtained in this analysis to assess the correlation between SNHG5 expression and LNM. Combining the odds ratio (OR) with the 95% confidence interval (CI) indicated that SNHG5 expression was positively related to LNM (OR: 1.443, 95% CI 0.709–2.939) (Fig. 4); however, the correlation was nonsignificant. The results of the subgroup analysis revealed a noteworthy correlation between SNHG5 expression and easier-to-lymph node metastasis in the subgroup of patients with a nondigestive system invasion (OR = 1.992, 95% CI 1.204–3.295) and a nonsignificant correlation in the subgroup of patients with a digestive system invasion (OR = 0.467, 95% CI 0.175–1.245) (Table 4).

Forest plot of SNHG5 expression and LNM in cancers
Correlations between SNHG5 expression and various other clinicopathological factors
Analysis of the pooled ORs with 95% CIs revealed that elevated SNHG5 expression was associated with increased tumour size (OR: 1.571, 95% CI 1.090–2.264) (Fig. 5); moreover, there were no significant associations between SNHG5 expression and DM (OR: 0.449, 95% CI 0.077–2.630) (Fig. 6A), histological grade (OR: 2.098, 95% CI 0.910–4.838) (Fig. 6B), depth of invasion (OR: 1.106, 95% CI 0.376–3.248) (Fig. 6C), age (OR: 0.946, 95% CI 0.718–1.247) or sex (OR: 0.762, 95% CI 0.521–1.115) (Table 4).

Forest plot of SNHG5 expression and tumor size in cancers

Forest plot of SNHG5 expression and DM, histological grade and depth of invasion in cancers. A DM; B histological grade; C depth of invasion
Sensitivity analysis and publication bias
The results of the sensitivity analysis of the overall survival rate showed that after removing the results of any one study, the overall survival was not affected at any time, suggesting that the overall survival rate was reliable and robust (Fig. 7). The results of Beeg's test of OS were as follows: Pr >|z|= 0.368, TNM stage = Pr >|z|= 0.108, LNM >|z|= 0.734, tumour size >|z|= 0.452, histological grade >|z|= 0.308, and DM >|z|= 1.000. These findings indicate that publication bias or other bias was not present in the original study (Fig. 8).

Sensitivity analysis for SNHG5 expression with overall survival (OS) in various cancers. HR: hazard ratio, CI confidence interval

Beeg’s test about the relationship between SNHG5 expression and survival outcome in various cancers. A OS; B TNM stage; C LNM; D DM; E Tumor size; F Histological grade
Discussion
Cancer has consistently posed a profound threat to the wellbeing of humanity [1, 3]. Over the years, diverse treatment modalities have been incrementally employed to address this menace, leading to important advancements [5, 40]. Nevertheless, the survival outcomes in numerous cancers have reached a plateau, rendering further progress challenging. Consequently, there is an urgent need to explore innovative therapeutic strategies. Long noncoding RNAs have been confirmed to play a role in the emergence and progression of diverse ailments, including cardiovascular disease [41], metabolic disease [42], nervous system disease [43], rheumatic immune system disease and cancer [44]. Because cancer is the number one killer in human health, an increasing number of researchers have begun to uncover the underlying pathogenic mechanisms by which long noncoding RNAs (lncRNAs) contribute to cancer progression. Mounting evidence suggests that these RNAs can modulate key processes in tumour cells, including proliferation, migration, invasion, and apoptosis, and influence the response of these cells to chemotherapy and radiotherapy [45]. Long noncoding RNAs (lncRNAs) regulate stem cell transformation and epithelial-to-mesenchymal transition (EMT), and numerous such RNAs have been identified as potential targets for cancer therapeutics; these RNAs notably affect tumour progression and markedly predict tumour prognosis. Therefore, long noncoding RNAs are promising potential tumour therapeutic targets and prognostic markers.
This analysis included 11 original studies, and the scores assigned based on the NOS indicated a high level of research quality across all 11 documents. When the hazard ratio (HR) was combined, it was revealed that elevated expression of SNHG5 could predict poor cancer prognosis, but the results were not statistically significant, and additional relevant high-quality original studies are needed to further support the results and conclusions of this investigation. Furthermore, combined OR data indicated that elevated SNHG5 expression was a predictor of advanced TNM staging, larger tumour size, easier distant metastasis, and poor histological grade. However, the correlations of SNHG5 expression with cancer LNM, invasion depth, age and sex were not statistically significant. In summary, the number of studies included in this meta-analysis was small, and the insufficient sample size may explain the reason for the effect of some prognostic indicators not reaching statistical significance. The results of the sensitivity analysis suggested that the overall survival results were reliable and robust. Furthermore, Begg's test results indicated the absence of any significant publication bias or other biases in the original studies.
SNHG5 was first revealed to be highly expressed as an oncogene in gastric cancer, and successive researchers subsequently reported that SNHG5 was differentially expressed in bladder cancer, lung cancer, liver cancer, cervical cancer, osteosarcoma, laryngeal cancer, oral cancer, and lymphoma. An increasing number of researchers have explored the oncogenic mechanism of SNHG5 (Fig. 9 and Table 5). Ma et al. reported that SNHG5 contributes to proliferation and inhibits the apoptosis of bladder cancer cells by downregulating p27 and caspase-3 and caspase-9 and upregulating CDK2 expression [32]. Wang et al. reported that SNHG5 induces gefitinib resistance by upregulating its expression via the competitive sponging of miR-377 [46]. Li et al. discovered that SNHG5 contributed to the proliferation and migration of hepatocellular carcinoma (HCC) cells through regulating GSK3β and the Wnt/β-catenin signalling pathway by competitively binding miR-26a-5p [33]. Yan et al. suggested that SNHG5 could promote the proliferation and migration of HCC cells by upregulating spermatogenesis-associated serine-rich 2 (SPATS2) expression (47). Zhang et al. indicated that SNHG5 accelerates the proliferation, migration and invasion of cervical cancer cells through upregulating sex-determining region Y-Box 4 (SOX4) expression via competitive sponging of miR-132 [34]. Wang et al. demonstrated that SNHG5 could accelerate the migration, invasion and proliferation and inhibit the apoptosis of osteosarcoma cells through targeting and positively regulating Rho-associated coiled coil-containing protein kinase 1 (ROCK1) expression by sponging and negatively regulating miR-26a [35]. Liu et al. reported that SNHG5 accelerated the proliferation, migration and invasion of nasopharyngeal carcinoma (NCC) cells by positively regulating high mobility group Box 3 (HMGB3) expression by downregulating miR-1179 expression [36]. Zhang et al. showed that SNHG5 contributed to the proliferation—and inhibited apoptosis—of AML cells through accelerating sex-determining region Y-Box 4 (SOX4) expression by competitively binding to miR-489-3p [34]. Wei et al. discovered that SNHG5 could inhibit the epithelial–mesenchymal transition (EMT) process in oesophageal cancer cells by downregulating the expression of metastasis-associated protein 2 (MTA2) [28]. Xing et al. revealed that SNHG5 could promote proliferation, invasion, migration, and inhibited apoptosis of diffuse large B-cell lymphoma (DLBC) cells through the positive regulation of X-linked inhibitor of apoptosis protein (XIAP) expression via the competitive sponging of miR-181-5p [37]. Li et al. reported that high SNHG5 expression indicated poor GC prognosis, but the detailed biological mechanism was not revealed [38]. Zhao et al. reported that SNHG5 suppressed the proliferation, migration and invasion of gastric cancer cells by upregulating MAT2 expression [39].

SNHG5 regulates some molecular biological mechanisms of tumor cells
This study has several limitations. First, all patients in this meta-analysis were from China, and thus, the conclusions of this study are representative of only Asians. Second, the number of patients included in this study was insufficient, preventing some positive conclusions from reaching statistical significance. Third, some of the included studies did not provide hazard ratios (HRs) or 95% confidence intervals (95% CIs); therefore, we had to use the Engage software to analyze the survival data. This result is inconsistent with the data from the original SPSS. In addition, this study collected and explored only the relationship between SNHG5 and the prognosis of some cancers, which may bias the results. However, additional high-quality studies with larger sample sizes are needed to support the conclusions of this study. Finally, several studies revealed that SNHG5 is highly expressed in tumour cells, while others revealed that SNHG5 is expressed at low levels in tumour cells, leading to inconsistent experimental conclusions.
Conclusion
SNHG5 is abundantly expressed across numerous tumour tissues, and elevated SNHG5 levels are significantly positively associated with poorer tumour prognosis. Additionally, high SNHG5 expression predicts advanced TNM staging, increased susceptibility to distant metastasis, increased tumour diameter, and decreased histological grade. These findings suggest that SNHG5 could emerge as a potential therapeutic target and a promising prognostic marker for tumour management. However, the conclusions drawn from this study require further validation through high-quality original research.
Availability of data and materials
All the data generated or analyzed throughout the course of this study have been included in the present publication. Additionally, any further data requests can be made to the corresponding author and will be provided upon reasonable request.
References
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA. 2023;73(1):17–48. https://doi.org/10.3322/caac.21763.
Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, Rosso S, Coebergh JW, Comber H, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49(6):1374–403. https://doi.org/10.1016/j.ejca.2012.12.027.
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. 2021;71(3):209–49. https://doi.org/10.3322/caac.21660.
Miller BA, Chu KC, Hankey BF, Ries LA. Cancer incidence and mortality patterns among specific Asian and Pacific Islander populations in the U.S. Cancer Causes Control. 2008;19(3):227–56. https://doi.org/10.1007/s10552-007-9088-3.
Kratzer TB, Jemal A, Miller KD, Nash S, Wiggins C, Redwood D, et al. Cancer statistics for American Indian and Alaska Native individuals, 2022 including increasing disparities in early onset colorectal cancer. CA. 2023;73(2):120–46. https://doi.org/10.3322/caac.21757.
Schafer EJ, Jemal A, Wiese D, Sung H, Kratzer TB, Islami F, et al. Disparities and trends in genitourinary cancer incidence and mortality in the USA. Eur Urol. 2023;84(1):117–26. https://doi.org/10.1016/j.eururo.2022.11.023.
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA. 2011;61(2):69–90. https://doi.org/10.3322/caac.20107.
de Martel C, Ferlay J, Franceschi S, Vignat J, Bray F, Forman D, et al. Global burden of cancers attributable to infections in 2008: a review and synthetic analysis. Lancet Oncol. 2012;13(6):607–15. https://doi.org/10.1016/s1470-2045(12)70137-7.
Fidler MM, Bray F, Soerjomataram I. The global cancer burden and human development: a review. Scandinavian J Public Health. 2018;46(1):27–36. https://doi.org/10.1177/1403494817715400.
Miro C, Di Giovanni A, Murolo M, Cicatiello AG, Nappi A, Sagliocchi S, et al. Thyroid hormone and androgen signals mutually interplay and enhance inflammation and tumorigenic activation of tumor microenvironment in prostate cancer. Cancer Lett. 2022;532: 215581. https://doi.org/10.1016/j.canlet.2022.215581.
Rupaimoole R, Slack FJ. Microrna therapeutics: towards a new era for the management of cancer and other diseases. Nat Rev Drug Discovery. 2017;16(3):203–22. https://doi.org/10.1038/nrd.2016.246.
Pérez-Herrero E, Fernández-Medarde A. Advanced targeted therapies in cancer: drug nanocarriers, the future of chemotherapy. Eur J Pharm Biopharm. 2015;93:52–79. https://doi.org/10.1016/j.ejpb.2015.03.018.
Qiu X, Li Y, Zhang Z. Crosstalk between oxidative phosphorylation and immune escape in cancer: a new concept of therapeutic targets selection. Cell Oncol. 2023;46(4):847–65. https://doi.org/10.1007/s13402-023-00801-0.
Anastasiadou E, Jacob LS, Slack FJ. Non-coding Rna networks in cancer. Nat Rev Cancer. 2018;18(1):5–18. https://doi.org/10.1038/nrc.2017.99.
Toden S, Zumwalt TJ, Goel A. Non-coding Rnas and potential therapeutic targeting in cancer. Biochim Biophys Acta. 2021;1875(1): 188491. https://doi.org/10.1016/j.bbcan.2020.188491.
Mattick JS, Makunin IV. Non-Coding Rna. Hum Mol Gene. 2006;15(1):17–29. https://doi.org/10.1093/hmg/ddl046.
Hombach S, Kretz M. Non-Coding Rnas: classification, biology and functioning. Adv Exp Med Biol. 2016;937:3–17. https://doi.org/10.1007/978-3-319-42059-2_1.
Panni S, Lovering RC, Porras P, Orchard S. Non-coding Rna regulatory networks. Biochim Biophys Acta. 2020;1863(6): 194417. https://doi.org/10.1016/j.bbagrm.2019.194417.
Mercer TR, Dinger ME, Mattick JS. Long non-coding Rnas: insights into functions. Nat Rev Genet. 2009;10(3):155–9. https://doi.org/10.1038/nrg2521.
McCabe EM, Rasmussen TP. Lncrna involvement in cancer stem cell function and epithelial-mesenchymal transitions. Semin Cancer Biol. 2021;75:38–48. https://doi.org/10.1016/j.semcancer.2020.12.012.
Li J, Meng H, Bai Y, Wang K. Regulation of Lncrna and its role in cancer metastasis. Oncol Res. 2016;23(5):205–17. https://doi.org/10.3727/096504016x14549667334007.
Rajagopal T, Talluri S, Akshaya RL, Dunna NR. Hotair Lncrna: a novel oncogenic propellant in human cancer. Clin Chimica Acta. 2020;503:1–18. https://doi.org/10.1016/j.cca.2019.12.028.
Yang L, Liu G. Lncrna Bancr suppresses cell viability and invasion and promotes apoptosis in non-small-cell lung cancer cells in vitro and in vivo. Cancer Manage Res. 2019;11:3565–74. https://doi.org/10.2147/cmar.S194848.
Yan K, Tian J, Shi W, Xia H, Zhu Y. Lncrna Snhg6 Is associated with poor prognosis of gastric cancer and promotes cell proliferation and Emt through epigenetically silencing P27 and sponging Mir-101-3p. Cell Phys Biochem. 2017;42(3):999–1012. https://doi.org/10.1159/000478682.
Li YH, Hu YQ, Wang SC, Li Y, Chen DM. Lncrna Snhg5: a new budding star in human cancers. Gene. 2020;749: 144724. https://doi.org/10.1016/j.gene.2020.144724.
Li Y, Hu J, Guo D, Ma W, Zhang X, Zhang Z, et al. Lncrna Snhg5 promotes the proliferation and cancer stem cell-like properties of Hcc by regulating Upf1 and Wnt-signaling pathway. Cancer Gene Ther. 2022;29(10):1373–83. https://doi.org/10.1038/s41417-022-00456-3.
Qin Y, Sun W, Wang Z, Dong W, He L, Zhang T, et al. Rbm47/Snhg5/Foxo3 axis activates autophagy and inhibits cell proliferation in papillary thyroid carcinoma. Cell Death Dis. 2022;13(3):270. https://doi.org/10.1038/s41419-022-04728-6.
Wei S, Sun S, Zhou X, Zhang C, Li X, Dai S, et al. Snhg5 inhibits the progression of Emt through the Ubiquitin-Degradation of Mta2 in Oesophageal Cancer. Carcinogenesis. 2021;42(2):315–26. https://doi.org/10.1093/carcin/bgaa110.
Kang S, Ou C, Yan A, Zhu K, Xue R, Zhang Y, et al. Long Noncoding Rna Snhg5 Induces the Nf-Κb pathway by regulating Mir-181c-5p/Cbx4 axis to promote the progression of non-small cell lung cancer. Arch Bronconeumol. 2023;59(1):10–8. https://doi.org/10.1016/j.arbres.2022.07.001.
Stang A. Critical evaluation of the newcastle-ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–5. https://doi.org/10.1007/s10654-010-9491-z.
Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8:16. https://doi.org/10.1186/1745-6215-8-16.
Ma Z, Xue S, Zeng B, Qiu D. Lncrna Snhg5 is associated with poor prognosis of bladder cancer and promotes bladder cancer cell proliferation through targeting P27. Oncol Lett. 2018;15(2):1924–30. https://doi.org/10.3892/ol.2017.7527.
Li Y, Guo D, Zhao Y, Ren M, Lu G, Wang Y, et al. Long Non-Coding Rna Snhg5 promotes human hepatocellular carcinoma progression by regulating Mir-26a-5p/Gsk3β signal pathway. Cell Death Dis. 2018;9(9):888. https://doi.org/10.1038/s41419-018-0882-5.
Zhang L, Wu X, Li Y, Teng X, Zou L, Yu B. Lncrna Snhg5 promotes cervical cancer progression by regulating the Mir-132/Sox4 pathway. Autoimmunity. 2021;54(2):88–96. https://doi.org/10.1080/08916934.2020.1864731.
Wang Z, Wang Z, Liu J, Yang H. Long non-coding Rna Snhg5 sponges Mir-26a to promote the tumorigenesis of osteosarcoma by targeting rock1. Biomedicine. 2018;107:598–605. https://doi.org/10.1016/j.biopha.2018.08.025.
Liu D, Wang Y, Zhao Y, Gu X. Lncrna Snhg5 promotes nasopharyngeal carcinoma progression by regulating Mir-1179/Hmgb3 Axis. BMC Cancer. 2020;20(1):178. https://doi.org/10.1186/s12885-020-6662-5.
Xing X, Xu T, Liu B, Guo Q. Lncrna Snhg5 can regulate the proliferation and migration of diffuse large B cell lymphoma progression via targeting Mir-181-5p/Xiap. J Cancer. 2022;13(3):784–92. https://doi.org/10.7150/jca.60521.
Li X, Du Y, Wang Y. The value of Lncrna Snhg5 as a marker for the diagnosis and prognosis of gastric cancer. Am J Translat Res. 2021;13(5):5420–7.
Zhao L, Guo H, Zhou B, Feng J, Li Y, Han T, et al. Long Non-Coding Rna Snhg5 Suppresses Gastric Cancer Progression by Trapping Mta2 in the Cytosol. Oncogene. 2016;35(44):5770–80. https://doi.org/10.1038/onc.2016.110.
Crocetto F, Buonerba C, Caputo V, Ferro M, Persico F, Trama F, et al. Urologic malignancies: advances in the analysis and interpretation of clinical findings. Future Sci OA. 2021;7(4):674. https://doi.org/10.2144/fsoa-2020-0210.
Uchida S, Dimmeler S. Long noncoding Rnas in cardiovascular diseases. Circ Res. 2015;116(4):737–50. https://doi.org/10.1161/circresaha.116.302521.
Li SY, Susztak K. The long noncoding Rna Tug1 connects metabolic changes with kidney disease in podocytes. J Clin Investig. 2016;126(11):4072–5. https://doi.org/10.1172/jci90828.
Bai Y, Ren H, Bian L, Zhou Y, Wang X, Xiong Z, et al. Regulation of Glial function by noncoding Rna in central nervous system disease. Neurosci Bull. 2023;39(3):440–52. https://doi.org/10.1007/s12264-022-00950-6.
Lorenzi L, Avila Cobos F, Decock A, Everaert C, Helsmoortel H, Lefever S, et al. Long Noncoding Rna expression profiling in cancer: challenges and opportunities. Genes Chromosom Cancer. 2019;58(4):191–9. https://doi.org/10.1002/gcc.22709.
Gugnoni M, Ciarrocchi A. Long noncoding Rna and epithelial mesenchymal transition in cancer. Int J Mol Sci. 2019. https://doi.org/10.3390/ijms20081924.
Wang Z, Pan L, Yu H, Wang Y. The long non-coding Rna Snhg5 regulates gefitinib resistance in lung adenocarcinoma cells by targetting Mir-377/Casp1 Axis. 2018. Biosci Reports. https://doi.org/10.1042/bsr20180400.
Yan J, Huang QY, Huang YJ, Wang CS, Liu PX. Spats2 Is positively activated by long noncoding Rna Snhg5 via regulating Dnmt3a expression to promote hepatocellular carcinoma progression. PLoS ONE. 2022;17(1): e0262262. https://doi.org/10.1371/journal.pone.0262262.
Acknowledgements
Not applicable.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
YL conceived and designed the project. QH, YX, YH, and HQ conducted a comprehensive literature search and screening of the databases. QZ and CW were responsible for the data extraction and analysis. WT and YL assessed the quality of the included literature. YL, QH, YH, and WT actively contributed to the manuscript preparation. The final manuscript was reviewed and approved by all the authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This article does not include any clinical patient studies, thus eliminating the need for an ethical statement. The responsibility of guaranteeing that any inquiries pertaining to the precision or integrity of the work are thoroughly examined and addressed rests solely with the authors.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Huang, Q., Xia, Yg., Huang, Yj. et al. An increase in SNHG5 expression is associated with poor cancer prognosis, according to a meta-analysis. Eur J Med Res 29, 160 (2024). https://doi.org/10.1186/s40001-024-01745-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-024-01745-3